
Abstract
Despite the self-evident importance of hospital funding, many anaesthetists remain unsure of exactly how their daily work relates to hospital reimbursement. A lack of awareness of the nuances of the Australian hospital activity–based funding system has the potential to affect anaesthetic department reimbursement and thus resourcing. Activity-based funding relies on clinical coders reviewing clinical documentation and quantifying the care given to a patient during an admission. Errors in funding allocation may arise when there is a disconnect between the work performed and the information coded. In anaesthesia, there are several factors impeding this process, including clinical understanding of coding, system setup and coders’ understanding of anaesthesia. This article explores these factors from the clinical anaesthetist’s point of view and suggests solutions, such as awareness and education, clinician–coder cooperation and redesign of documentation systems at a systems level that anaesthetic departments can incorporate.
Introduction
Healthcare system funding is complex, challenging and often poorly understood by clinicians. 1 To provide equitable access to healthcare, funding systems must balance sustainability, efficiency and innovation with the ever-expanding need to improve quality, volume and breadth of health services.1–4 In many countries healthcare funding equals over 10% of gross domestic product and costs are predicted to increase with the ageing population. 5 To mitigate rising costs worldwide, most healthcare systems have moved to an activity-based funding (ABF) model. 1 Implemented in Australia in 2012, ABF awards funding based on services (activity) provided to patients, and the complexity of the activity. 6 In this way hospitals are more appropriately compensated, tailoring funding to case volume and complexity, encouraging efficiency to accommodate increased service provision.1,2,6,7
ABF and the wider healthcare system rely on accurate clinical documentation of activity, which is then coded for billing. A lack of detailed documentation leaves hospitals at risk of underfunding. 1 One of the most at-risk areas for hospital revenue loss is procedural and peri-procedural care. 4 Surgical and anaesthetic costs are some of the largest drivers of hospital funding, accounting for nearly one-third of US healthcare spending. 4 As a result of the high volume of cases, rapid-paced nature of treatment, barriers to documentation, and lack of healthcare funding education, anaesthesia represents an area at high risk of potential revenue loss. A UK study revealed that 93% of surgical cases had at least one clinical coding error, with up to 20% of cases incorrectly coding the primary procedure performed. 8 Each coding error results in potential hospital revenue loss, and inaccurate patient records, creating subsequent issues in quality control, research and policy development.
Anaesthetists’ understanding of clinical coding (the process of assigning standardised codes to specific clinical events for billing) and ABF in its entirety is essential to motivate practice change and provide value-based healthcare. Practice change, at an individual and systems level, could be levied into funding that could purchase clinical equipment, provide more clinical staff and improve patient care. This article aims to: (a) describe the process of clinical coding and ABF relevant to anaesthetists; (b) provide examples of missed clinical coding opportunities relevant to anaesthetists; and (c) outline potential individual and systems-based approaches to improve compensation for patient management in public hospital anaesthetic departments.
How are hospitals funded?
With changing times and needs, governments internationally have moved away from block grants towards models allocating funding based on patient volume and complexity and in-hospital interventions, so-called ‘activity-based funding’ (ABF).1,2,6,7 ABF was developed in the USA to reduce healthcare costs while promoting efficiency and penalising poor patient outcomes, and is now used internationally under various names, including the UK, Canada, Australia, New Zealand, and much of Europe.1,9–11
An outline of the process used in Australia, broadly similar to many other countries, can be seen in Figure 1.11,12 Clinical coders (professionals qualified in health information systems often with clinical backgrounds) use clinical documentation to categorise admissions by principal and additional diagnoses, interventions that occurred (from surgery to electrolyte replacement) and complications, closely examining each patient’s chart from their admission. International Classification of Diseases (ICD) diagnoses are mapped to a larger major disease category (e.g. gastrointestinal), and then subcategorised to more specific diagnosis-related groups (DRGs; e.g. gastrointestinal haemorrhage). To account for the complexities of each individual patient’s admission, each DRG is assigned a complexity specifier from A (most complex) to D (least complex). The combination of DRG and complexity code are then quantified in national weighted activity units (NWAUs). One NWAU is equivalent to an ‘average’ hospital admission, with an admission’s NWAU increasing or decreasing based on principal diagnosis, complexity and various other factors. The NWAU for each admission is then multiplied by the national efficiency price (NEP) to determine the financial reimbursement for that admission, determined annually in Australia by the Independent Hospital Pricing Authority (IHPA). 11 Thus, principal diagnosis, complexity and interventions all directly contribute to the reimbursement towards each admission period, as well as taking into account external financial system considerations.
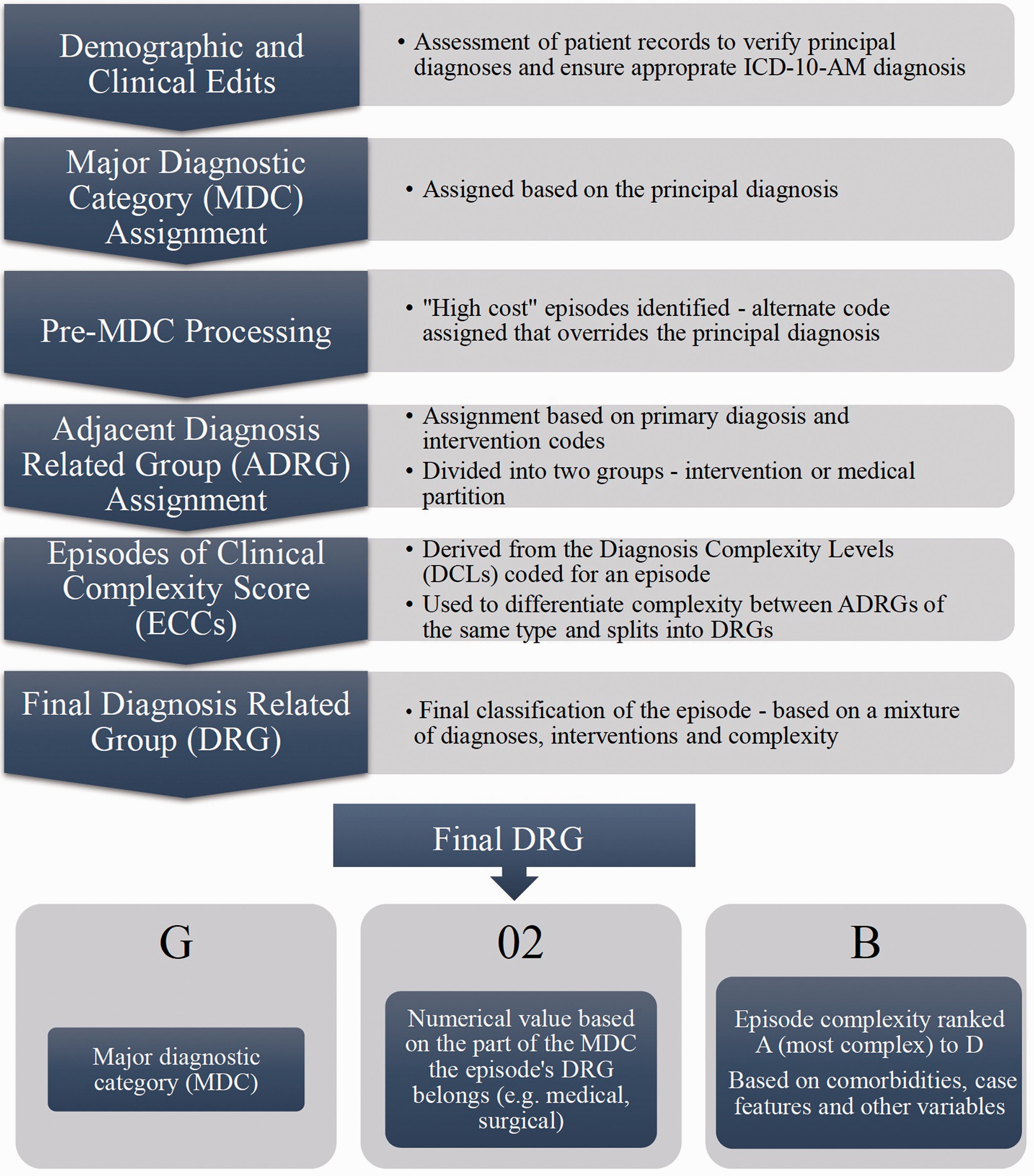
The reality of coding and reimbursement is somewhat more complex than Figure 1 suggests. Many factors other than complexity contribute to the NWAU and final payment in Australia, including patient age, Aboriginal, Torres Strait Islander or rural origin, and the presence of avoidable hospital complications as given by the formula:11,12




Furthermore, up to 20% of hospital funding comes from other sources, including block grants for teaching and research and rural hospital funding schemes. 11 Nevertheless, ABF remains the major funding source in Australia. There are several potential benefits to ABF as a hospital funding system; increased efficiency, volume, shorter length of stay (LOS), and funding transparency.1,2,6,7,13 The NEP attempts to ensure admissions are reimbursed at an ‘efficient’ price, within the bounds of an ‘average’ LOS (Figure 2). Conversely, there are numerous limitations to ABF. These include increasingly early discharges, a one-size-fits-all standard of efficiency, administrative costs and complexity, and potential inappropriate upcoding.1,14–18 These have all been seen in studies examining the implementation of ABF into new health systems internationally.1,15–17 Finally, the question of whether ABF truly improves outcomes remains unanswered, with a systematic review of over 50 studies showing increases in post–acute care, but little change in re-admissions, or patient-centred outcomes. 1
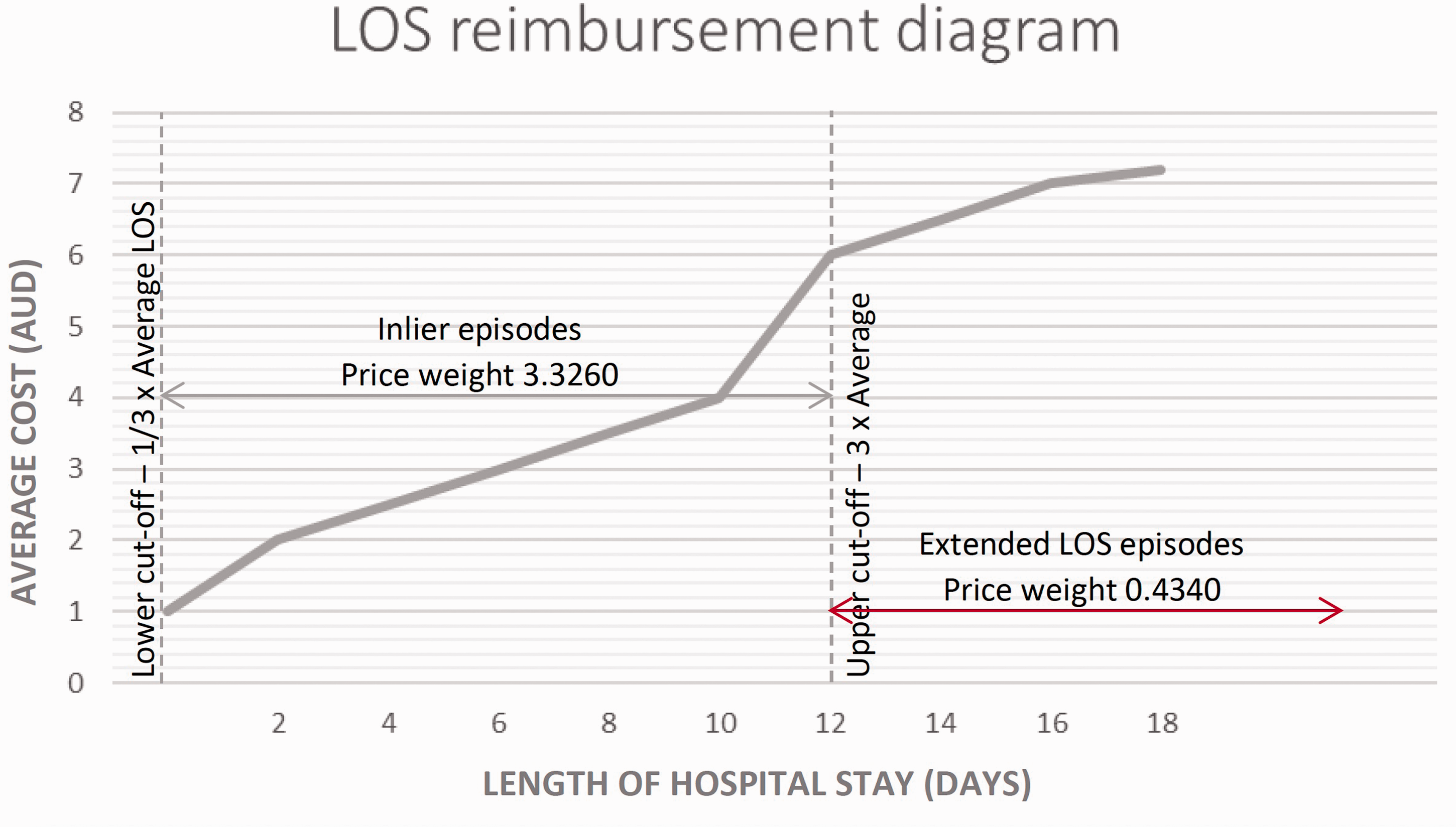
Graph demonstrating the effect of extended length of stay (LOS) on hospital reimbursement.
Anaesthesia-specific challenges in attracting hospital funding
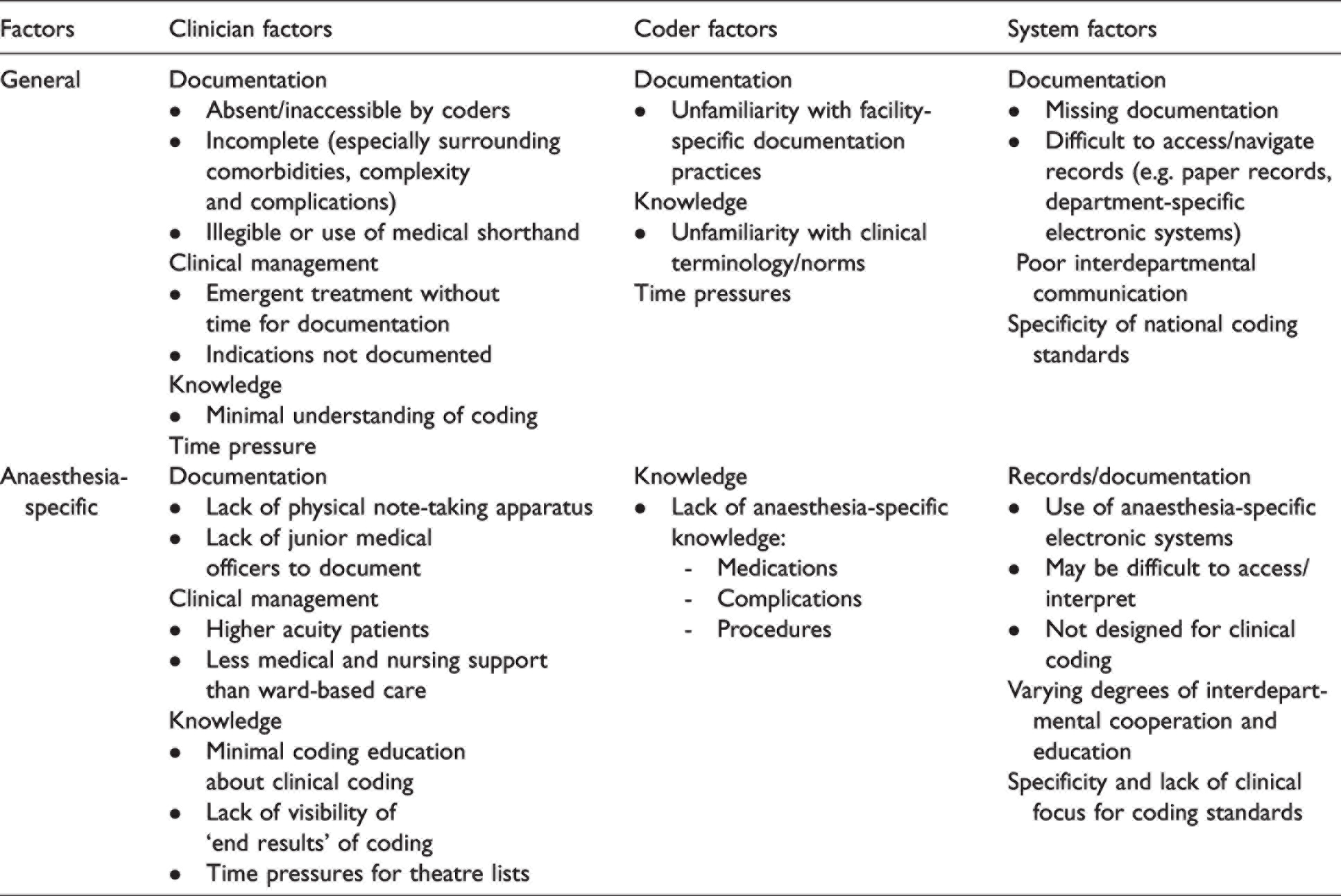
In anaesthesia, there are many challenges related to clinical coding (Table 1). These include documentation challenges, the turnover and nature of anaesthesia, understandable discrepancies in knowledge of coding by anaesthetists and anaesthesia by coders.18,19 First, rather than the typical written or typed clinical notes seen on the wards, anaesthetic peri- and intraoperative notes are stored either on anaesthesia-specific health information management programmes or specialised paper charts. These systems are structured to provide ease of documentation for a typical theatre case. This has two impacts for clinical coding and ABF. First, unusual deviations from a typical case that may have an impact on funding can be more difficult to record and thus may be omitted. Second, it may be difficult for clinical coders to access and interpret specialised anaesthetic charts or outputs of such specific software, which can subsequently lead to incorrect or incomplete coding.
Anaesthesia is unique among non-surgical specialties in the number of procedures performed in a single episode of care. Skilled, essential interventions such as invasive monitoring using arterial or central lines, or transoesophageal echocardiography, are often missed during coding. 20 Without formal documentation by anaesthetists, the time and expertise involved will not attract funding, leaving anaesthetic departments to cover the expenses for equipment and training.
Expecting universal pristine documentation using current systems is impractical given the time pressures and current lack of motivation faced routinely by anaesthetists. Between minimal time and competing clinical and safety priorities, the seemingly trivial task of documentation is often the first to be sacrificed for the time-poor physician, unaware of its downstream importance. Despite the enormous impact of documentation quality on hospital revenue, clinical coding receives minimal attention in most medical curricula, and is not taught in most anaesthesia training programmes. As a result, many clinicians are unaware of strategies, or even the need, to improve their documentation from a coding perspective. Clinicians such as anaesthetists are far removed from the funding process and are indirectly impacted by poor coding practices. As a result, there is minimal incentive to encourage a change in practice. Indirectly, however, such changes could drastically improve an anaesthetist’s daily working life, from increased staffing levels, state-of-the-art equipment, and increased training and education opportunities.
Anaesthesia poses coding challenges not only for clinicians, but for clinical hospital coders themselves. Anaesthesia is a highly specialised field, with procedures, treatments, and specialty-specific terminology. As a result, it may be difficult to ensure accurate coding even with adequate documentation, if it cannot be understood.19,21,22 The implications of imperfect coding practices extend further than hospital funding, towards research capacity and the quality of audit results. 21 Thus, there are multiple incentives to improve this aspect of our practice.
Examples of the impact of anaesthesia documentation
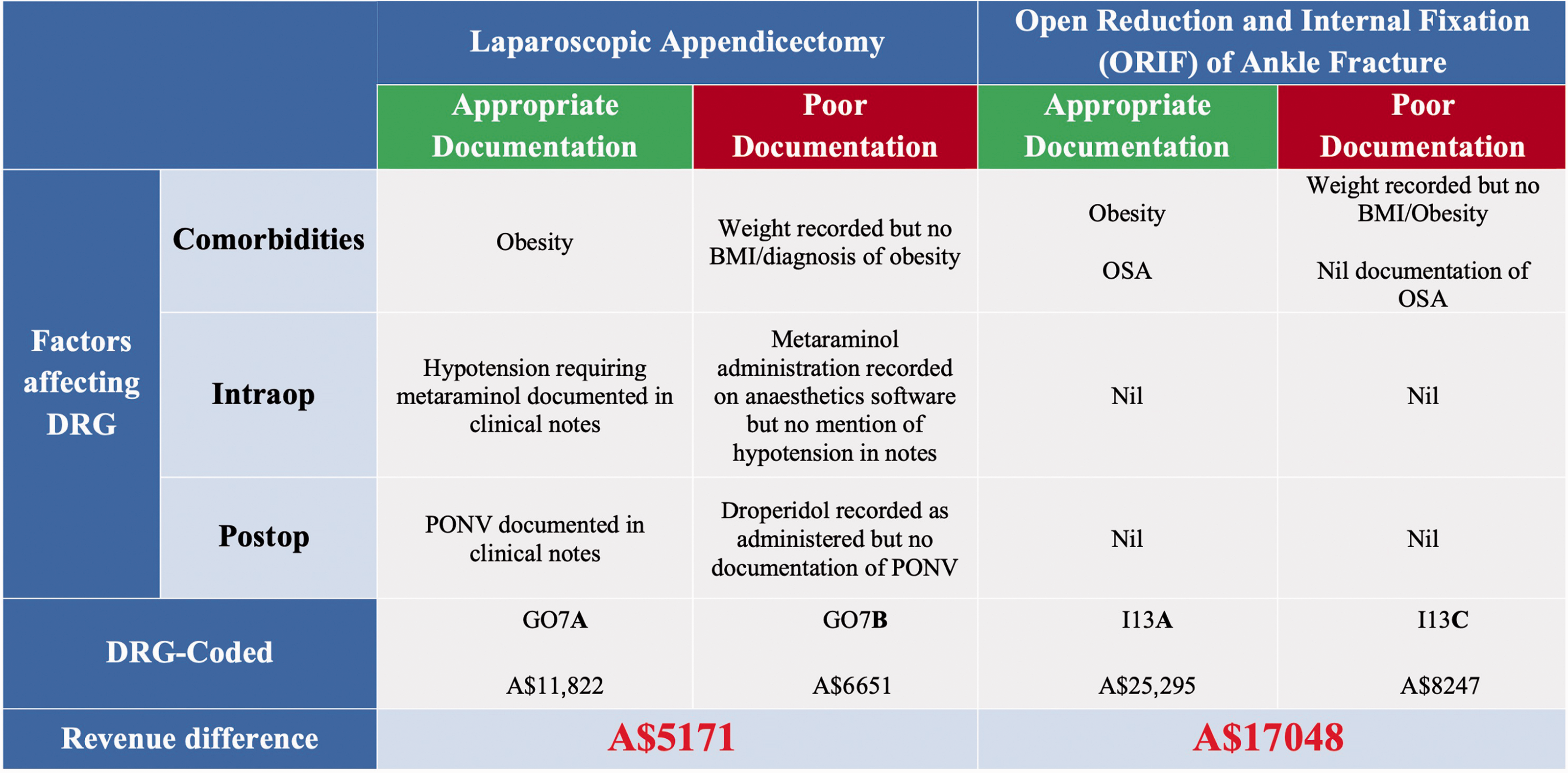
Below are two examples of common anaesthetic clinical scenarios, laparoscopic appendicectomy and ankle reduction and internal fixation, with and without optimal documentation and clinical coding (Figure 3). 27 The reimbursement for these cases differs by A$5000 to A$17,000 based solely on factors commonly missed in clinical coding, such as obesity, obstructive sleep apnoea, intraoperative hypotension and postoperative nausea and vomiting.11,28 By documenting comorbidities and complications, as well as how these impact the anaesthetic (e.g. choice of tracheal tube for airway, increased anaesthesia dosage requirement, ventilation strategies for obese patients, etc.) funding is significantly increased. An anaesthetist may only be motivated to record these details accurately, however, if aware of their importance in clinical coding and reimbursement.
Opportunities for improvement
Individual level
Training and education of clinicians
Hospital clinical coders rely on clinician notes to assign DRGs and complexity weightings, which determine the final reimbursement. Improving clinician documentation is key to improving coding accuracy and ensuring appropriate funding allocation. Clinicians can be supported and educated at all stages of their medical training to be aware of the coding nuances relevant to medical notes. For instance, coders in Australia may not extrapolate diagnoses from laboratory values or vague phrasing, and educating around the need for clear diagnoses (e.g. hypokalaemia and not K=3.0 mmol/l) may be useful. Such curricula have already been developed in the US for surgical residents, with encouraging results. 18 This training needs to carry on through to specialty training; in each specialty there are specific diagnoses or complications that are frequently missed. For example, in anaesthesia, a difficult airway is a commonly missed complexity code with real financial value. Examples of such diagnoses are seen in Table 2. Encouraging specificity in note-taking improves both clinical communication and coding.
Commonly missed anaesthetic-related additional diagnoses. 28
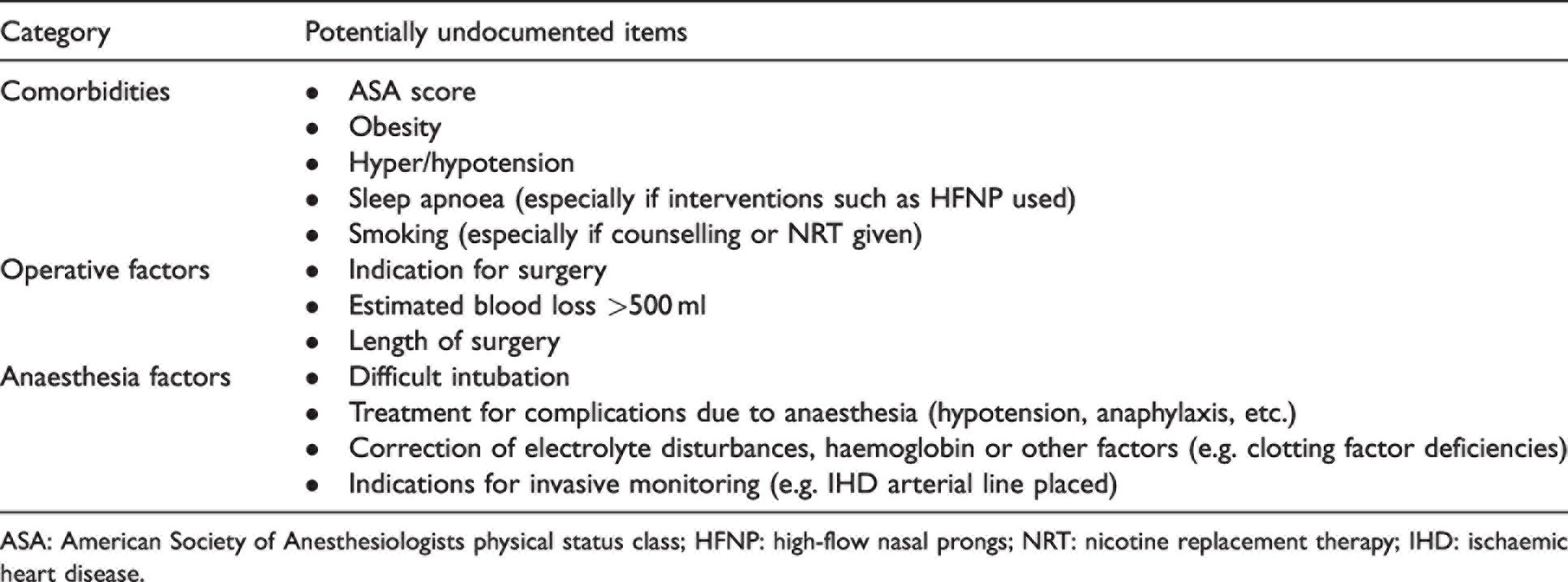
ASA: American Society of Anesthesiologists physical status class; HFNP: high-flow nasal prongs; NRT: nicotine replacement therapy; IHD: ischaemic heart disease.
Incorporation into routine practice and departmental support
While education is an essential part of any implementation programme, it is unlikely to succeed unless supported at the departmental level. Departments could ensure improved documentation by supporting adequate time allocation for improved note-taking or reviewing previous days’ notes from a coding perspective, audits of coding to ensure accuracy from the coder’s side and ensuring anaesthetic health information systems integrate with the hospital’s clinical coding team. 25 As patient care is the primary focus of all anaesthetists it is essential that such programmes are not overly time-consuming and can integrate into clinical practice without detracting from time dedicated to patient care. There must be increased anaesthetist awareness of coding importance, potential department improvements, built-in mechanisms to improve coding or reduce the technological time burden on anaesthetists, and feedback to clinical coding teams to ensure accuracy in a highly specialised field of medicine.
Dedicated DRG forms
Another solution in use is dedicated DRG forms. By consolidating commonly encountered conditions onto a single, standardised form many of the potentially missed complexity-adding diagnoses or procedures can be captured. A system whereby doctors can confirm conditions on a single page, rather than rely on coders searching through an entire admission’s documentation is already in use at some hospitals. The authors have developed an example of such a form, seen in Table 3. These forms could be physically available in operating theatres, or be integrated in a ‘smart form’ into a department’s anaesthesia health information system, speeding up as well as improving the accuracy of data collection. Successful implementation of such a form will require close collaboration with the local health information systems department to ensure it follows local coding legislation; often such forms can act as guidance for coders, but contemporaneous documentation in the chart may still be necessary.
Anaesthetic diagnosis-related group template.
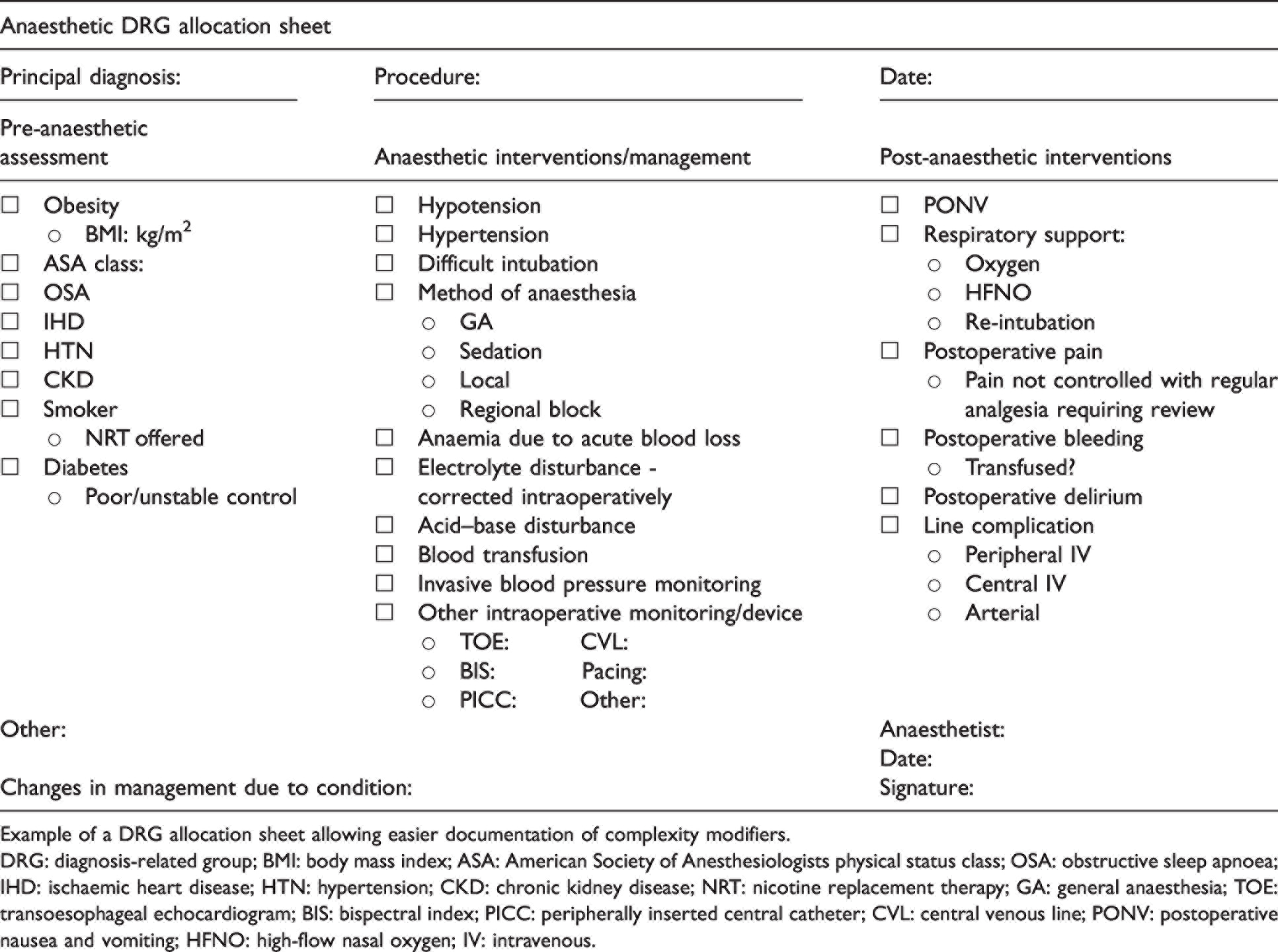
Example of a DRG allocation sheet allowing easier documentation of complexity modifiers.
DRG: diagnosis-related group; BMI: body mass index; ASA: American Society of Anesthesiologists physical status class; OSA: obstructive sleep apnoea; IHD: ischaemic heart disease; HTN: hypertension; CKD: chronic kidney disease; NRT: nicotine replacement therapy; GA: general anaesthesia; TOE: transoesophageal echocardiogram; BIS: bispectral index; PICC: peripherally inserted central catheter; CVL: central venous line; PONV: postoperative nausea and vomiting; HFNO: high-flow nasal oxygen; IV: intravenous.
Systems level
Forcing functions
A systems-thinking approach is required in any large anaesthetic department to implement sustainable change, and in this case, improve clinical documentation and thus coding and finance. While the use of anaesthetic management systems in anaesthesia is commonly cited as one of the limitations to clinical coding, it could potentially also be a solution. Software developers of such electronic systems could add forcing functions or pop-up windows for certain common and clinically important variables that affect funding. These could take the form of checklists for common DRGs or procedures when imputing patient details, or a pop-up window prompting anaesthetists to consider documentation of comorbidities, for instance, obesity. Obesity is an important, commonly non-coded variable in anaesthesia, that is highly prevalent (up to 31% of the population) and adds complexity to a DRG if affecting patient management. 29 If 31% of cases had this comorbidity added through a pop-up reminder or checklist when inputting data into the anaesthesia software system, the additional funding could be significant for anaesthetic departments.
Interdisciplinary teamwork and cooperation
Improving clinical documentation is only one piece of the puzzle. Documentation then needs to be reliably understood and translated by clinical coders. Although coders are experts in their field, an inability to translate anaesthesia events accurately may render other improvements moot. This can arise both from lack of clinical knowledge but also difficulty interpreting information from anaesthetic software. 25 Collaborative interdepartmental educational sessions to improve the flow of information, understanding between the clinicians and coders, and redesign of hindering systems could also help reduce confusion and increase accuracy.23–26 A collaborative approach such as clinicians teaching coders how to interpret anaesthetic reports accurately so that they can directly code from them will lead not only to a greater amount of reimbursement for activities performed by the department but a more seamless coding system that will be time efficient for both clinicians and coders. 18
Clinician advocacy
ABF is by no means a perfect system. However, limited clinician engagement means many potential solutions are not pursued. Improving education on this topic could induce anaesthetists to become change advocates. Anaesthetists know best the practice of anaesthesia and where funding could be better spent, and with better knowledge of ABF, they could be powerful agents of change. 26 One further way this could be encouraged is advocating for departmental improvements to be reflected in department budgets. This would better link clinical coding to hospital funding in clinicians' minds and encourage sustainable changes.
Conclusion
Funding for a healthcare system is undoubtedly a complex business. Although ABF is one of the most commonly used systems worldwide, there remain a number of limitations for its use in anaesthesia. There are numerous considerations anaesthetic providers need to make when documenting their cases to ensure all their activities attract funding. This is important not just at a departmental level, but from the perspective of patient care. Solutions are required at the individual and systems level to improve clinical coding, informed by an understanding of the entire system at work. Unless anaesthetists, anaesthetic departments, clinical coders and medical administrators engage and work together to improve the hospital system they work in, we are engaged in a cycle of ongoing poor documentation, inaccurate clinical coding and loss of healthcare funding that could otherwise be spent to maximise safe and best practice anaesthetic care.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank Surya Harijatna for his invaluable contributions in reviewing this manuscript from a clinical coder’s perspective, as well as Stephen Gatt, Michelle Roets and Edu van Zyl for their thorough reviews of the manuscript.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.