
Abstract
Given the severity of the consequences of operating room fires, it is recommended that every anaesthesiologist master fire safety protocols and periodically participate in operating room fire drills. The aim of the present study was to evaluate skill retention one year after an airway fire training programme. Anaesthesiology residents were evaluated using an airway fire simulation-based scenario one year after an educational programme that included a one-h long problem-based learning session, a simulation-based airway fire drill with debriefing, and a formal group discussion. The same simulation scenario was used for both the initial training and the one-year assessment. Thirty-eight anaesthesiology residents participated as pairs in the initial training programme. Of these, 36 participated in the evaluation a year later. Performance after one year was better than performance during the initial simulation. Time to removal of tracheal tube was 7.0 (4.0–12.8) s (median (interquartile range)) at the one-year assessment compared with 22.0 (18.5–52.5) s at the time of initial training (P < 0.001). Performance improvement was also demonstrated by a higher incidence of performance of crucial action items (cessation of airway gases, removal of sponges and pouring of saline), as well as shorter duration of time necessary to perform these tasks. After controlling the fire, the time to re-establish ventilation by bag-mask ventilation or intubation was shorter at one year: 18.0 (11.0–29.0 ) s, compared with initial training 54.0 s (36.2–69.8) s (P = 0.001). We conclude that skills are effectively retained for a year after an airway fire management training session.
Keywords
Introduction
According to the emergency care research institute, between 550 and 650 operating room fires occur annually in the USA. 1 The risk of operating room fire stems from the routine use of potential sources of ignition in an environment rich in fuel sources and oxidisers. Operating room fires can be divided into two different types: on or in the patient and remote from the patient. The most common sites of operating room fires are on the patient and involve the head, face, neck and upper chest due to the presence of an ignition source in an oxidiser rich environment. 2
Airway fires are one of the most feared complications of airway surgery, posing a grave risk to patient safety. 3 According to a recent review, airway fire occurs mainly during tracheostomies, endoscopic procedures and monitored anaesthesia care or local procedures. 4 Of 87 fire cases identified, 76 (86%) patients experienced acute complications, including one intraoperative death. A major contributing factor to airway fires is the flammability of drapes, towels and sponges used to create the surgical field; this is increased in oxygen-enriched environments. 5 Similar data come from the American Society of Anesthesiologists Closed Claims Study analysis. 6
Given the severity of the consequences of operating room fire, the American Society of Anesthesiologists Task Force on Operating Room Fires recommended that every anaesthesiologist should possess knowledge of fire safety protocols and periodically participate in operating room fire drills. 7
Following an airway fire event in our institution, we launched airway fire training for our residents. The training included problem-based learning (PBL), simulation-based training of an airway fire event, and debriefing. Simulation-based training was incorporated based on previous operating room fire training studies which demonstrated the face validity, 8 effectiveness, 9 and superiority of simulation compared with other training modalities. 10
Given the concern regarding skill retention after high-fidelity simulation-based training,11,12 the aim of the present study was to evaluate participants’ performance one year after initial training. Our hypothesis was that participants would effectively retain knowledge regarding the management of an airway fire scenario one year after initial training.
Methods
The study
Ethical approval for this study was provided by the Ethical Committee of Sheba Medical Center (N° 7198-20-SMC), Tel Aviv, Israel on 25 May 2020. Anaesthesia junior (postgraduate year 1–2) and senior (postgraduate year 3–5) residents participated in an educational programme targeting airway fire safety. Our learning objectives included understanding the elements of the fire triad, recognising how standard operating room equipment can initiate a fire, demonstrating the proper management of an operating room fire involving a patient with an emphasis on airway fire, demonstrating appropriate teamwork and communication, discussing the mechanisms of injury from fire and discussing control of oxygen during head, neck and upper chest surgery.
The educational programme began with a one-h PBL session. A month later, residents performed a simulation-based airway fire drill in pairs consisting of one junior and one senior resident. In the briefing preceding the drill, residents were told they were going to participate in an airway training scenario, but the actual purpose of the scenario was not disclosed. Participants were also instructed not to share their experience with the other subjects. Immediately following the simulation scenario, the residents participated in a debriefing session. One month after the simulation/debriefing, a group discussion involving all of the participants was conducted. During this concluding session, results of the training and simulation were presented and further discussion related to airway fire management was conducted. One year after completion of the initial training (PBL, simulation/debriefing/group discussion), the residents participated in a simulation-based reassessment of airway fire management skills. The identical simulation-based scenario used for training was re-utilised but for assessment only, without a PBL session before the simulation assessment. Residents were unprepared regarding the aim and specific subject of the assessment simulation and were asked not to share information with the other participants. The scenario involved an unexpected airway fire that occurs during a tracheostomy in a ventilated patient with an FiO2 = 0.6. (More details of the scenario can be found in Appendix 1.)
Performance assessment
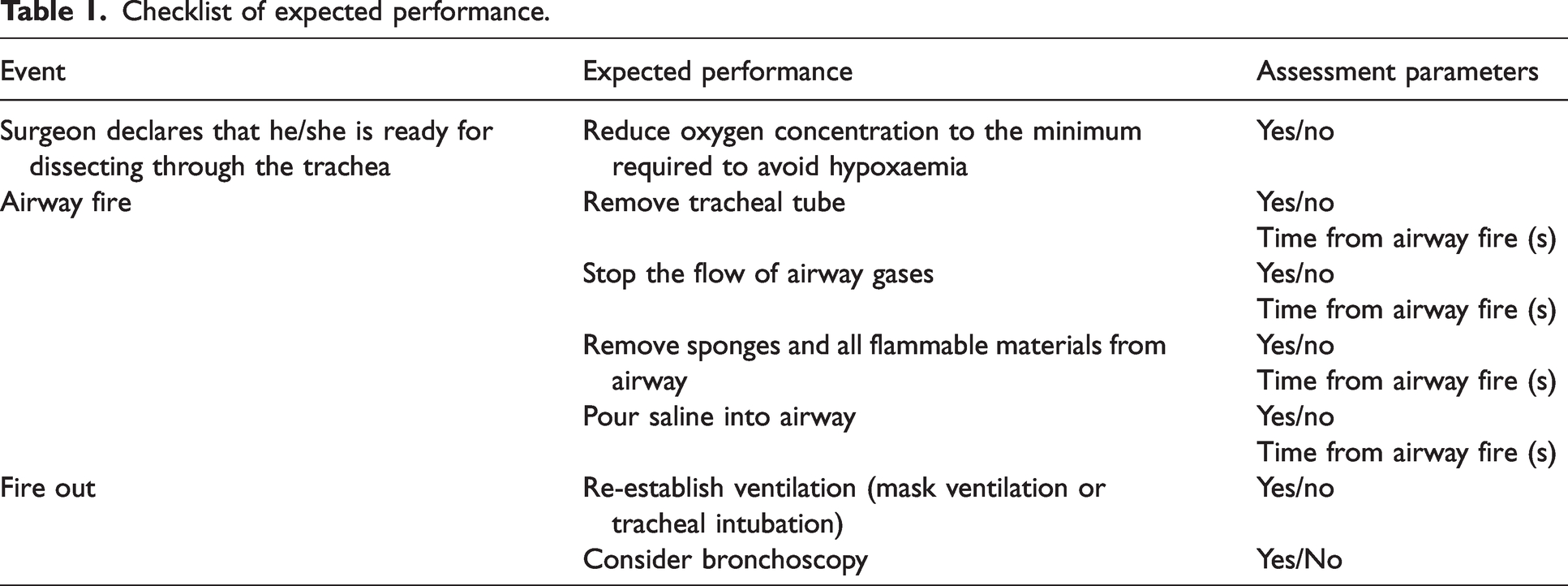
Performance both during the simulation training session and during the assessment session a year later was assessed in real time by a single observer (AZ, IEP or MI) using a checklist based on the recommendation of the American Society of Anesthesiologists Task Force on Operating Room Fires. 5 Parameters of yes/no and time for task performance were obtained (Table 1). The expected performance tasks were as follows: reduce oxygen concentration during procedure, remove tracheal tube, stop flow of airway gases, remove flammable materials, pour saline into airway, re-establish ventilation, consider bronchoscopy.
Checklist of expected performance.
Statistics
Wilcoxon rank-sum test and Fisher’s exact test were used for statistical comparisons for numerical and categorical variable, respectively. The statistical analysis was done with R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Thirty-eight anaesthesiology residents (19 junior and 19 senior residents) participated as pairs in the initial training programme. Of these residents, 36 participated in the second evaluation a year later (data from these participants were used for further evaluation). Data are presented as n/N (%) for ‘yes’ or ‘no’ parameters or median (interquartile range) for task completion time (results presented in Table 2).
Performance during airway fire simulation at the initial training and one year after the initial training.
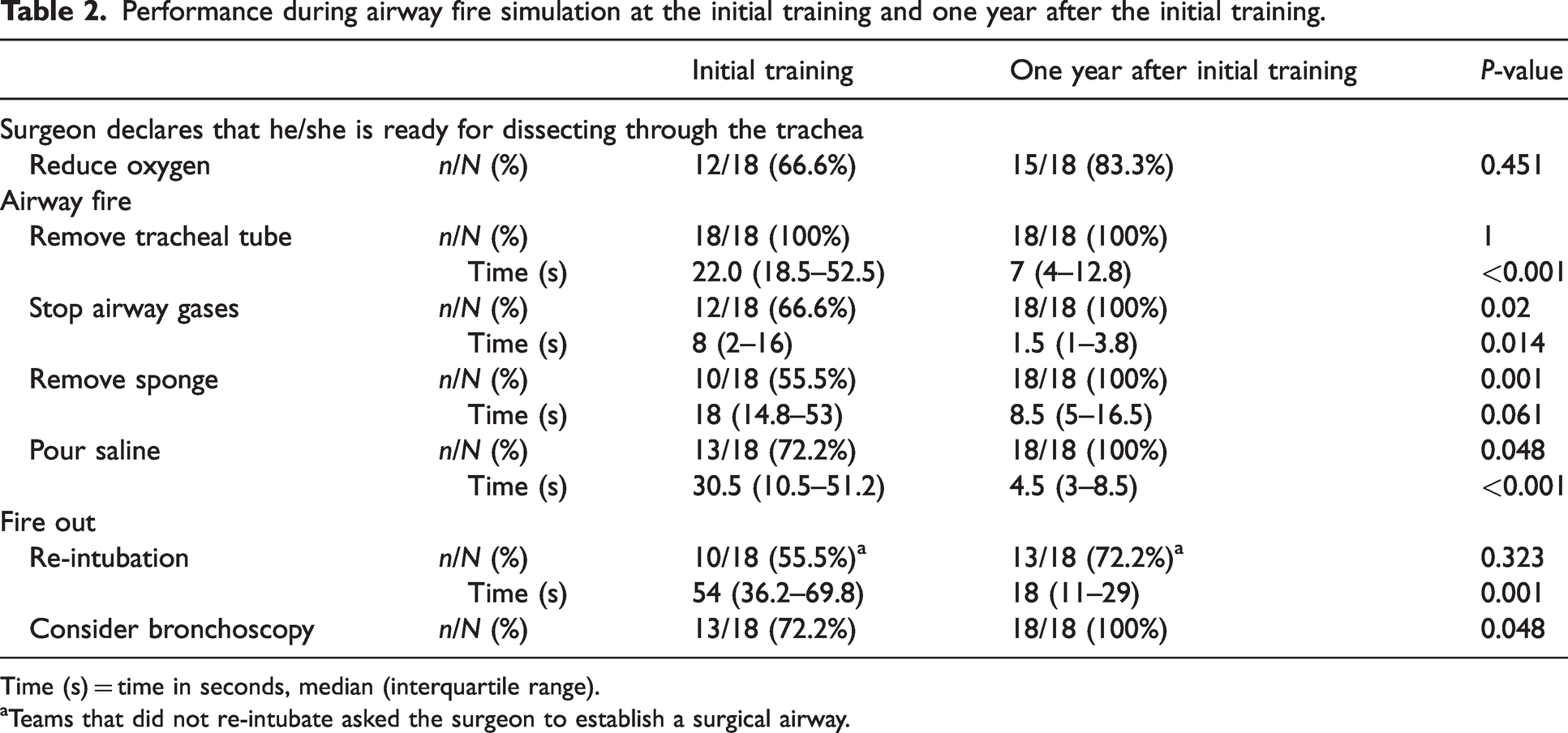
Time (s) = time in seconds, median (interquartile range).
aTeams that did not re-intubate asked the surgeon to establish a surgical airway.
From the onset of the airway fire, time to removal of the tracheal tube was shorter at one-year assessment compared with initial training, 7.0 (4.0–12.8) s versus 22.0 (18.5–52.5) s, P < 0.001). In other measured action items, the number of participants completing the task was greater, and the time from airway fire event to action performance was shorter during the assessment simulation than during the training simulation (Table 2).
After controlling the fire, the time to re-establish ventilation by bag–mask ventilation or intubation was shorter at one-year assessment than at initial simulation training, 18.0 (11.0–29.0) s versus 54.0 (36.2–69.8) s, (P = 0.001). At both simulations, the teams that did not attempt to re-establish ventilation by intubation asked the surgeon to establish a surgical airway. All teams considered bronchoscopy at the one-year assessment compared with 13/18 teams considering bronchoscopy during the initial training simulation (P = 0.048).
Discussion
In this study, the performance of anaesthesiology residents in a simulation-based airway fire drill was assessed one year after airway fire training. The initial training programme included a PBL session, followed by a simulation/debriefing session one month later, and a group discussion a month after the simulation/debriefing session. As the relative effectiveness of different learning modalities (high-fidelity simulation-based training, PBL, lectures and more)13–17 is controversial, we elected to perform integrative training by combining several modalities.
The main result of the study was that performance during the assessment drill performed one year after the training programme was better than performance during the initial simulation training module. This improvement was demonstrated by a higher incidence of performance of crucial action items as well as a reduction in time to perform these actions. Previous studies have demonstrated retention of knowledge and skills up to one year after simulation-based training for cricothyroidotomy skills, 18 ‘can't intubate, can't oxygenate’ scenario, 19 postpartum haemorrhage, 20 general anaesthesia for emergency caesarean section 21 and difficult airway management. 22
One hypothesis, raised to explain the retention of knowledge and skills after a single simulation-based training, was that the realism of the simulation scenario used to teach and assess performance aids retention. 16 The high realism may improve performance if the subjects experienced stress and were able to appraise the situation as a challenging one. While one study supported the hypothesis that stress improves participant performance and retention after simulation-based training; 23 others24,25 have questioned the additional educational value of a stressful simulation environment as it might impair memory retrieval. In our study we did not assess the level of stress that participants experienced during simulation; however, presumed stress during a realistic simulation with special effects including actual fire may explain the retention of memory one year later.
Another explanation for skills retention may be the routine use of simulation-based training at our institution. During the one-year period between airway fire training and reassessment, each resident participated in ten or eleven different small group simulation-based training sessions followed by debriefing. These sessions included training in the management of difficult intubation, local anaesthetic toxicity and anaphylaxis during anaesthesia among others. To the best of our knowledge, the transference of skills between different simulation-based scenarios has not been tested. However, from studies on the transfer of skills from simulation-based training to the clinical setting we can learn that the process is complex and dynamic. Factors affecting transfer of learning include learner characteristics, training design and work environment.26,27 We speculate that repeated training in a simulation environment may contribute to skill retention in the present study.
One limitation of the present study is that the same scenario was used for both the initial training and for the assessment one year later. Other limitations are that multiple modalities were used during training, including problem-based case discussion, simulation-based training and debriefing, and we cannot draw conclusions on the relative value of each of these components of the training process. The same residents participated in both training and assessment one year later, and the experience gained during the intervening year of residency training may have influenced performance. Although no events of airway fire were recorded in the department during the study year, most residents participated in anaesthesia for tracheostomy or other airway procedures and the experience gained during these cases may be relevant to airway fire event management.
In conclusion, our study demonstrates that a short training scheme can be maintained on a yearly basis after a high fidelity simulation practice and feedback. Future research should focus on the optimal repetition interval between simulation training sessions. In addition, frequent errors and missed tasks offer opportunities to improve training and design an improved educational modality.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.