
Abstract
Anaesthetic agents have various financial and environmental impacts. Climate change is one of the biggest threats to human health, and anaesthetic gases contribute to global heating by acting as greenhouse gases. The primary aim of this study was to quantify the financial and environmental impacts of anaesthesia maintenance agents used during surgery in an Australian university teaching hospital. The volume of desflurane, sevoflurane, isoflurane and propofol purchased by a university teaching hospital between 2010 and 2020 was analysed and described in terms of financial and environmental impact. Estimated carbon emissions and financial costs of each agent per annum were calculated using the volumes purchased for each agent. A model of ideal anaesthetic agent usage was used to hypothesise the financial and environmental impact of replacing desflurane (the most environmentally damaging and expensive agent) with alternative agents. Using 2019 as an example year at our health service, replacing desflurane with low flow sevoflurane would save greenhouse gas emissions equivalent to driving over 1.4 million kilometres in an average petrol car. Removing desflurane from machines at our institution could save an estimated A$14,630 per annum through reduced machine testing alone. Our findings and calculations indicate that reducing the use of desflurane would have both financial and environmental benefits for healthcare.
Keywords
Introduction
Patient-centred care is at the heart of clinical decision-making in modern medicine. However, with humanity facing a climate crisis that will directly impact the health of current and future patients and the increasing financial burden of healthcare, the choices that healthcare providers make today impact the health that patients experience in the future.1,2 This necessitates a triple-bottom-line approach to healthcare. 3 Such an approach mandates the inclusion of patient safety, and financial and environmental impacts in clinical decision-making at all stages of healthcare delivery. 3
With growing appeals to limit the significant contribution of healthcare to climate change, volatile anaesthetic agents are of increasing interest because they are potent greenhouse gases (GHGs) that exert radiative forces and contribute to global heating.4,5 A carbon footprint study of healthcare services in Australia found that healthcare contributes about 7% of Australia’s national carbon footprint; however, this did not include volatile anaesthetic agents.6 In the UK’s National Health Service, around 5% of healthcare’s carbon footprint is estimated to be directly attributed to anaesthetic gases. 7 A health economic evaluation of volatile anaesthetic purchasing in hospitals in Victoria between 2005 and 2011 found that desflurane use was increasing despite a 9% inflation-adjusted increase in its cost. 8 This study also reported the reduction in isoflurane and reflected on ‘trends’ in volatile anaesthetic use, which are influenced by clinicians’ familiarity with different practices and the introduction of newer anaesthetic machines. 8
Trends in the use of desflurane are of particular relevance because it is more expensive and environmentally damaging than other safe volatile alternatives. 9 In evaluations of the carbon footprint of surgery in three operating suites in the USA, Canada and the UK, hospitals that used desflurane had a carbon footprint that was 13 times (USA) and 16 times (Canada) greater than the UK hospital that did not use desflurane, despite the UK hospital performing almost double the number of cases annually. 10
The primary aim of this study was to quantify the financial and environmental impacts of anaesthesia maintenance agents used during surgery in an Australian university teaching hospital.
Methods
The study was conducted at Austin Health, a tertiary teaching hospital affiliated with the University of Melbourne in Melbourne, VIC, Australia. Austin Health performs approximately 38,000 adult surgical procedures annually across two campuses with a diverse admixture of complex cardiothoracic, hepatobiliary-pancreatic and subspecialty surgeries (e.g. bariatrics, neurosurgery, liver and renal transplantation, orthopaedics), endoscopic, radiological and cardiac interventional procedures.
After institutional ethics approval (approval number: Audit/22/Austin/13), the annual purchasing volume and cost data were retrieved for isoflurane, sevoflurane, desflurane and propofol (200 mg and 500 mg vials) for all Austin Health operating theatres, endoscopy and radiology procedure rooms and cardiac catheterisation rooms (N = 24) between 1 January 2010 and 31 December 2020. Annual surgical encounters for the same period were also retrieved. Propofol vials used in the intensive care unit and emergency department were excluded.
GHG emissions were calculated in kilograms of carbon dioxide equivalents (CO2e) and minutes of anaesthesia provided using accepted formulae. 11 The calculations of Sulbaek Anderson et al. were used to evaluate the volatile agent’s global warming potentials (GWP100), as they are widely accepted. 5 The calculations and reference agent data used are contained within Table S1 and Table S2 in supplementary material. The CO2e of propofol was calculated using 0.45 kg CO2e/h, based on an estimate from Allen and Baxter which included seven h of anaesthesia, ten syringes, an extension line, an electroencephalogram (EEG) monitor, 21 g CO2e per gram of propofol, and assumed a dose of 100 µg/kg per h for a 70 kg adult.12,13 We assumed all 500 mg vials of propofol were used for maintenance anaesthesia and assumed all 200 mg vials of propofol were not used for maintenance. Purchasing of propofol 200 mg vials mirrored annual surgical encounters while propofol 500 mg vials increased in use over the study period, reflecting the observed propofol total intravenous anaesthesia (TIVA) practice in our institution (Figure 1).
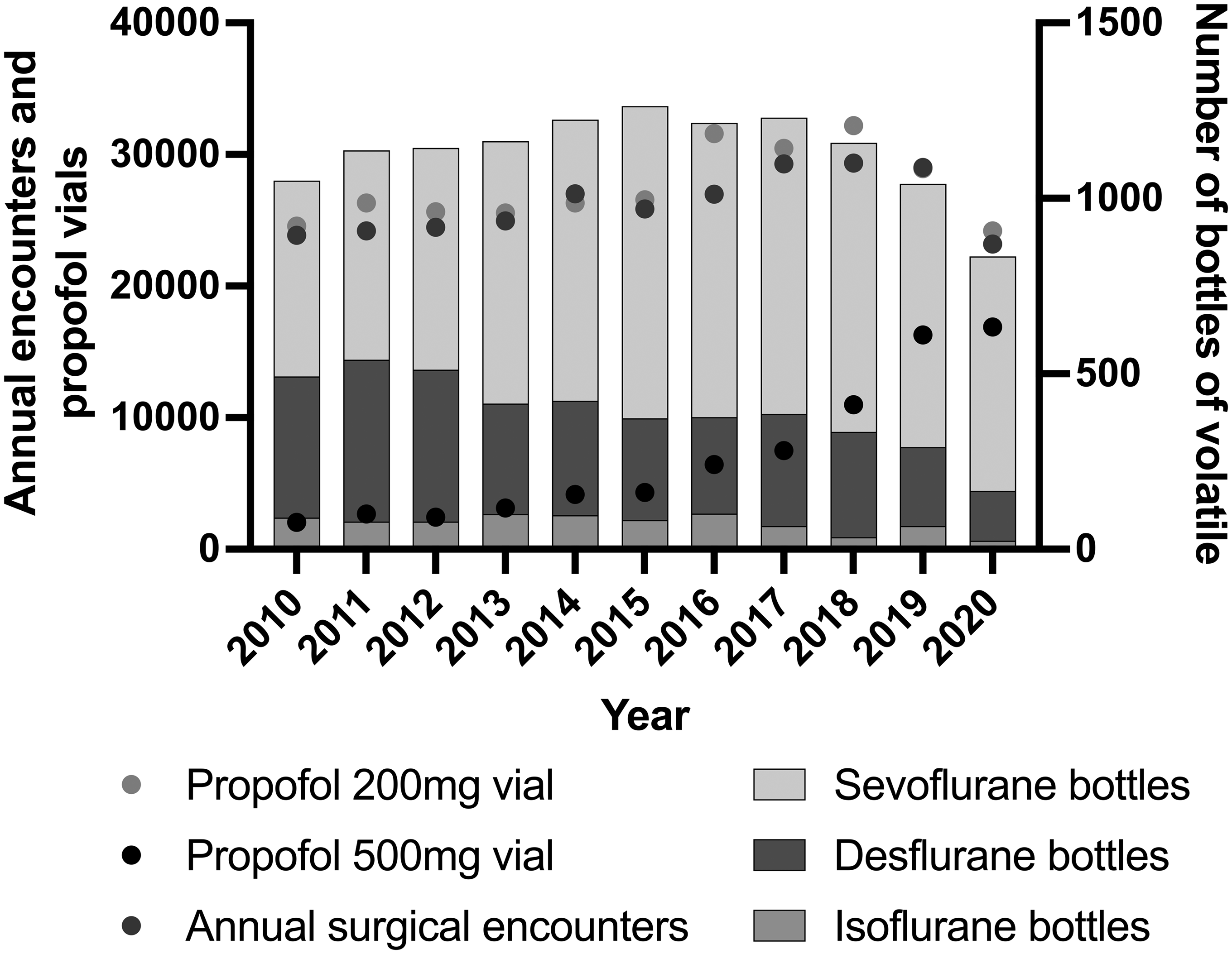
Annual anaesthetic agent purchasing and surgical activity. Bottles of volatile anaesthetic agent purchased, propofol 200 mg and 500 mg vials purchased, surgical encounters at Austin Health per annum.
We created an ‘ideal’ volatile usage model to calculate the maximum minutes of anaesthesia possible per anaesthetic agent, which used one litre per minute fresh gas flows for sevoflurane and isoflurane and 0.5 l/min for desflurane. This assumed a best-case scenario for desflurane and recognised that most clinicians use low flows with volatile anaesthetic agents. 14 We calculated the GHG emissions and financial impacts of replacing the minutes of desflurane and isoflurane anaesthesia with sevoflurane anaesthesia or propofol TIVA anaesthesia using only 500 mg vials. The data were analysed using descriptive statistics, and graphs were created in Prism (version 9, 2021, GraphPad, USA).
Results
Surgical activity
Between 1 January 2010 and 31 December 2020, 288,169 adult surgical encounters were undertaken across Austin Health, with a total of 29,014 encounters in 2019. In 2019, an issue with operating theatre sterilising equipment created the potential for a reduction in elective surgery. However, the number of surgical encounters for the year was not different from 2018. In 2020, the SARS-CoV2 pandemic led to a reduction in elective surgery by 21% compared with 2019.
The annual purchase of volatile anaesthetic agents between 2010 and 2020 is shown in Figure 1.
The number of bottles of desflurane purchased in 2019 was 41% less than the volume purchased in 2010 but peaked in 2011. In 2010, desflurane bottle purchases were 30% of all bottles purchased, but by 2020 this had dropped to 16%.
Despite the fall in surgical encounters during the response to the SARS-CoV2 pandemic, propofol volume and spending continued to rise annually. By 2020, this had increased eightfold over the volume purchased in 2010 (Figure 1). Austin Health operating theatres did not deliver intensive care services during the pandemic in 2020.
Annual cost of purchased anaesthesia maintenance agents
Desflurane was the most expensive anaesthetic agent; it was four times the cost of sevoflurane per millilitre. The proportional volumes of all volatiles purchased were 72% (sevoflurane) and 24% (desflurane). However, desflurane accounted for 40% of the total cost of volatile anaesthetic agents. By contrast, propofol 500 mg vials were 1% of total anaesthetic agent costs.
Greenhouse gas emissions from anaesthesia maintenance agents
Although the volume of desflurane was only 24% of the total volume of volatile agents purchased, the GHG emissions from desflurane accounted for 83% of all volatile carbon emissions over the study period (Figure 2). For every year between 2010 and 2020, the GHG emissions from desflurane contributed over 80% of all volatile GHG emissions. Desflurane purchasing fell overall between 2011 and 2020; in 2019, desflurane constituted 13% of all volatiles purchased, yet still contributed 80% of all volatile anaesthetic GHG emissions. In 2019, desflurane alone contributed 261,664 kg CO2e, the equivalent of driving over 1.4 million km in an average non-electric car in Australia. 15 Even with a steady increase in propofol 500 mg vial purchasing, the CO2e from propofol maintenance anaesthesia amounted to only 0.017% of all agent GHG emissions.
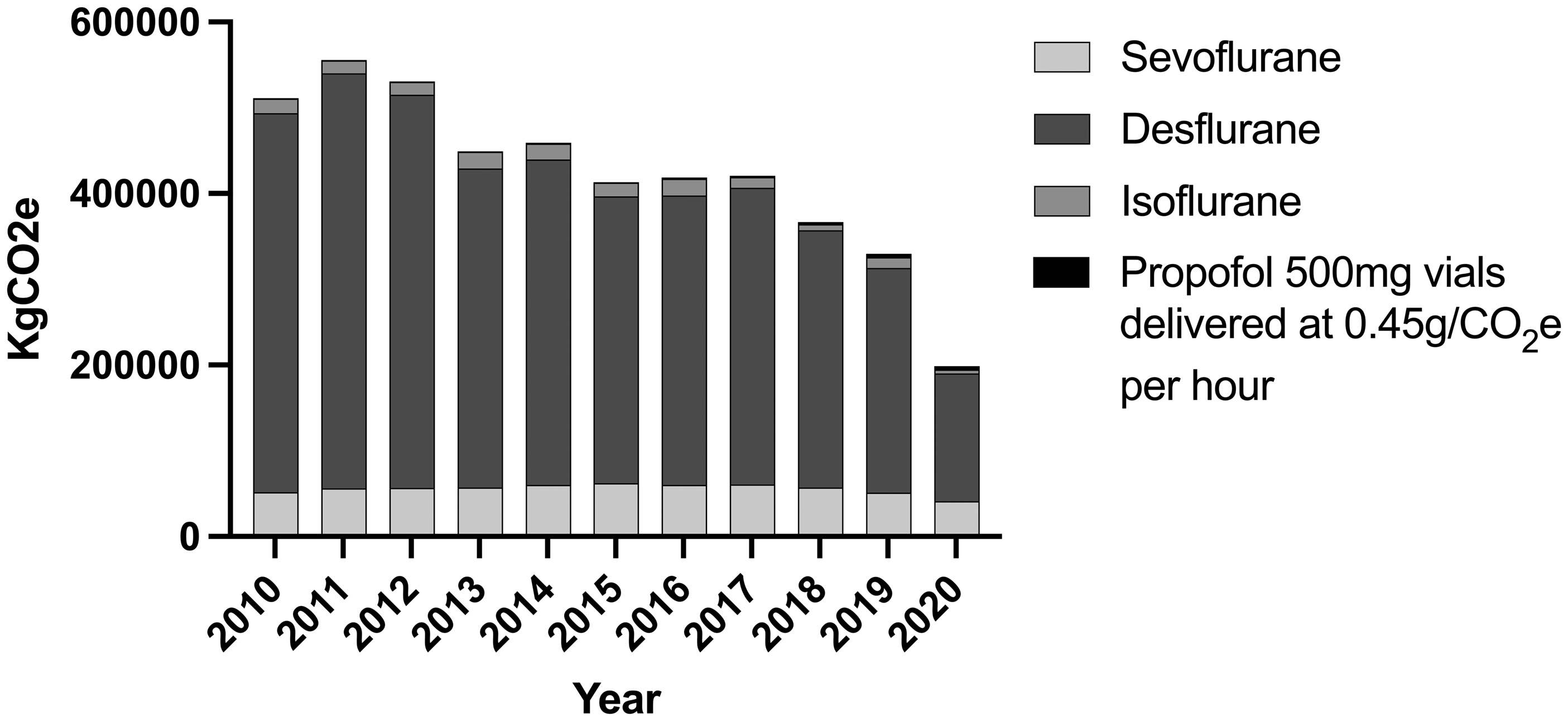
Annual calculated emissions of anaesthetic maintenance agents. Emissions were calculated using kgCO2e = (GWP100 × density × volume in millilitres) ÷ 1000.
Using our ‘ideal’ model for anaesthesia agent delivery, the kilograms of CO2e per ideal anaesthesia hour was 32 kg CO2e for a desflurane anaesthetic compared with 1.3 kg CO2e for sevoflurane and 0.3 kg CO2e for a propofol anaesthetic (Figure 3).
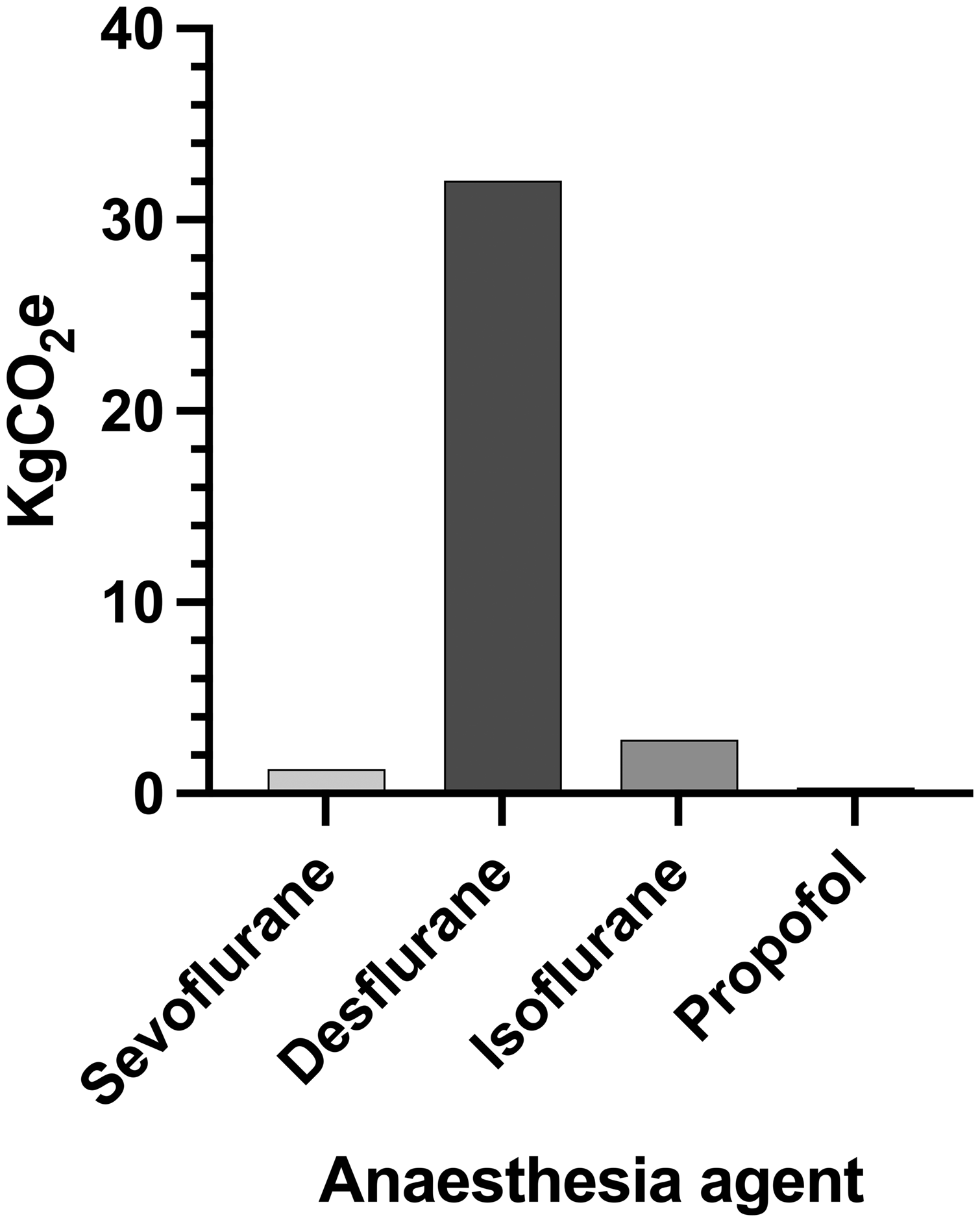
kgCO2e per hour of anaesthesia delivered in an ‘ideal conditions’ model for 2019. The hypothetical model was based on 2% sevoflurane at 1 l/min fresh gas flows, 6% desflurane at 0.5 l/min fresh gas flows, 1.2% isoflurane at 1 l/min fresh gas flows, propofol at 100 µg/kg per min for 70 kg adult using a model of 0.45 g/CO2e per hour.
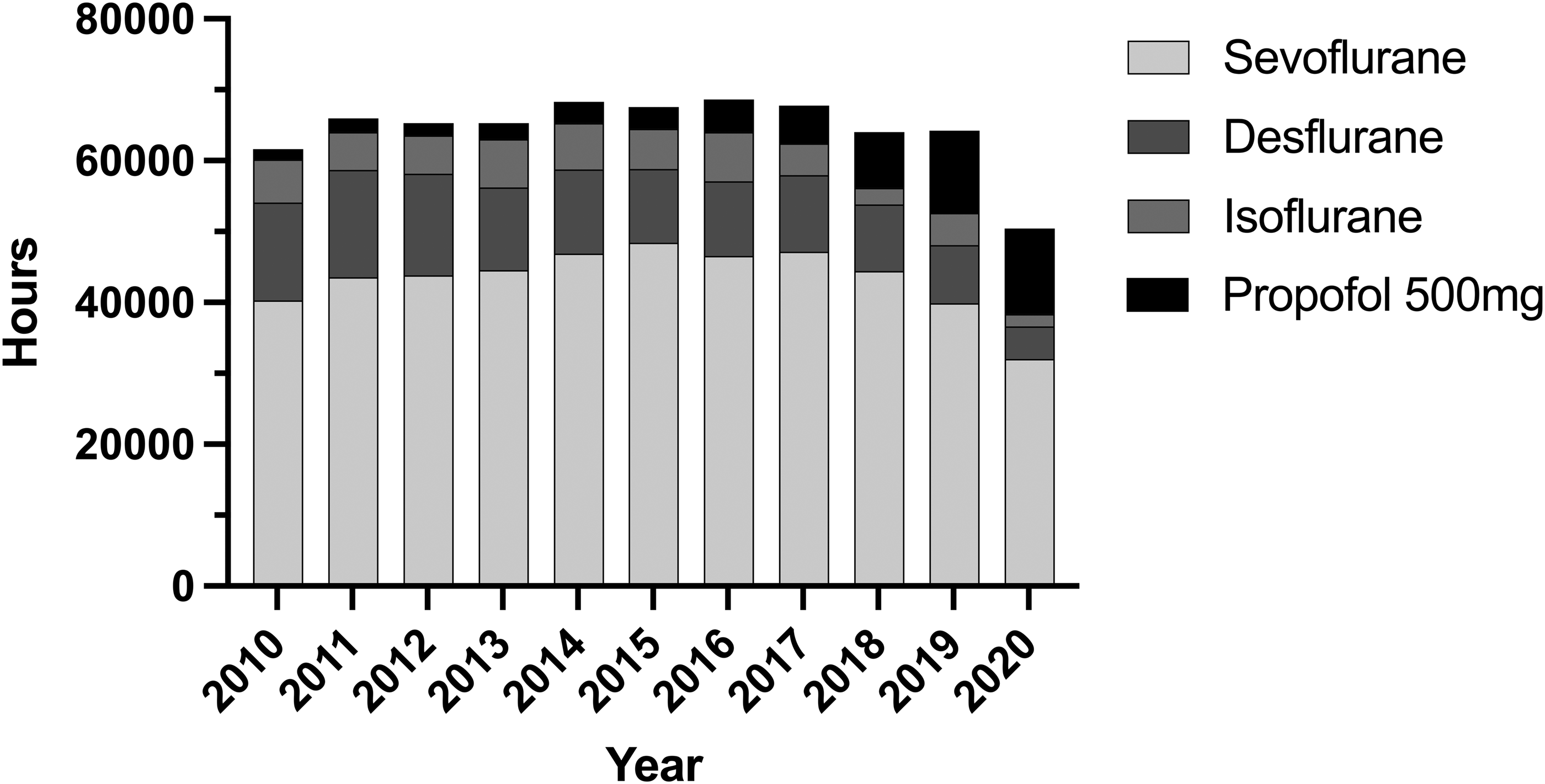
Calculated maximum hours of anaesthesia by volume purchased. Maximum hours were calculated using a hypothetical model of 2% sevoflurane at 1 l/min fresh gas flows, 6% desflurane at 0.5 l/min fresh gas flows, 1.2% isoflurane at 1 l/min fresh gas flows, propofol at 100 µg/kg per min for a 70 kg adult using a model of 0.45 g/CO2e per hour. The model assumes steady state of volatile anaesthesia and no losses.
Financial savings by removing desflurane and isoflurane
Using 2019 as the test year, if the anaesthesia minutes of desflurane and isoflurane were delivered by sevoflurane instead, the cost savings for 2019 alone would be A$89,383 across all operating theatres combined. This translates to a saving of A$4470 per operating theatre per year in our institution. However, if propofol delivered these same desflurane and isoflurane minutes, the cost savings would be A$84,464 per year.
Environmental savings by replacing desflurane and isoflurane
Using 2019 as our test year, if the anaesthesia minutes of desflurane and isoflurane were delivered by sevoflurane using ideal conditions of one litre per minute at 2% sevoflurane, the replacement sevoflurane would generate 16,706 kg CO2e. This would save approximately 257,773 kg of CO2 equivalent emissions for the year. This is equivalent to the carbon sequestration of 4262 tree seedlings grown for ten years or driving 1.4 million km in an average non-electric car in Australia 15,16
If the anaesthesia minutes of desflurane and isoflurane were delivered by propofol rather than sevoflurane, the CO2e generated would be 187 kg CO2e from the drug alone. However, using an estimate of 0.45 kg CO2e per hour of the TIVA model, the CO2e generated from the propofol TIVA replacing those anaesthetic hours would be only 4004 kg CO2e, amounting to a saving of 270,474 kg CO2e in 2019. This saving is equivalent to 331 acres of forest sequestering CO2 in one year or driving 1.48million km in an average petrol car in Australia.15,16
Machine testing costs and environmental impact
Using the volumes of agents used per machine test as determined by Dehouwer et al. for Dräger Zeus® (Drägerwerk AG & Co. Lübeck, Germany) (n = 11), GE Aisys™ (General Electric healthcare, Chicago, USA) (n = 5) and Getinge Flow-I (Getinge, Gottenburg, Sweden) (n = 2) machines, the costs and GHG emissions from the testing of these machines at Austin Health are displayed in Table 1. 17 Removing desflurane from these machines to avoid unnecessary testing (i.e. when desflurane is not planned to be used) would save A$14,630 per year and 36,909 kgCO2e. This assumed 260 checks per year (daily check, five days per week over 52 weeks). Importantly, this result does not include all machines in use as no ‘agent volume used per check’ data was available for the other machines in use. The annual cost of testing on these three machines alone with desflurane vaporisers in situ was eight times the cost of testing with sevoflurane vaporisers. Removing desflurane from storage on anaesthetic machines avoids unnecessary volatile atmospheric release and constitutes a small but potentially valuable financial benefit over time.
Cost and greenhouse gas emissions due to volatile anaesthetic agents using Austin Health data and volumes of agent per machine check derived from Dehouwer A et al.:17 Dräger Zeus® (Drägerwerk AG & Co. Lübeck, Germany), GE Aisys™ (General Electric healthcare, Chicago, USA), Getinge Flow-I (Getinge, Gottenburg, Sweden).
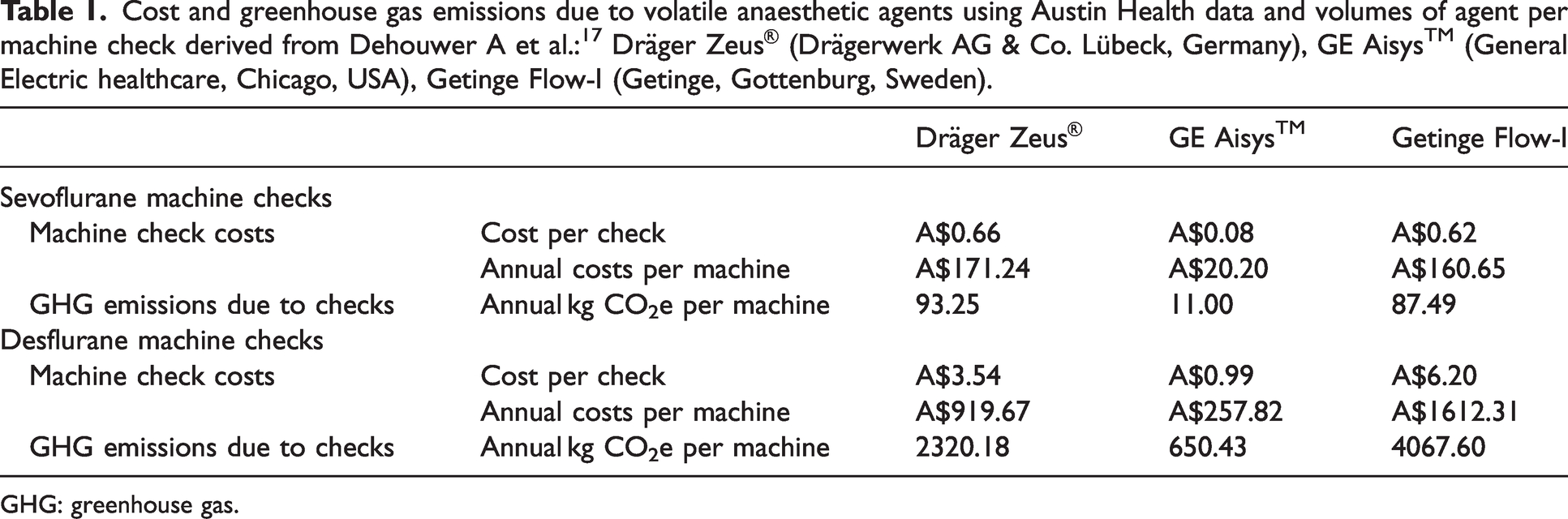
GHG: greenhouse gas.
Discussion
We performed an observational study in a single centre Australian university teaching hospital to quantify the financial and environmental impacts of anaesthesia maintenance agents used during surgery. Whilst sevoflurane use was almost fourfold greater than desflurane, desflurane accounted for 40% of the total cost of volatile anaesthetic agents. Moreover, by volume alone, desflurane was four times the cost of sevoflurane and had a 20 times greater contribution to global warming than sevoflurane. By contrast, propofol 500 mg vials were 1% of total anaesthetic agent costs.
We used ideal circumstances to generate estimates of CO2 emissions for volatile anaesthetic maintenance agents, using air as a carrier gas, and assumed that the agents would deliver the maximum number of anaesthetic hours in ideal conditions (Figure 4). Even taking a more basic comparison of potency where desflurane is three times less potent than sevoflurane, desflurane still has a disproportionately high financial and environmental cost. Sherman et al. showed that using nitrous oxide as a carrier gas increases the GHG emissions of sevoflurane by 900% when using two litres per minute fresh gas flows. 18 Our calculation did not consider some of the real-world aspects of delivering volatile-based general anaesthesia, such as higher fresh gas flows at the start of anaesthesia and over-pressurising a vaporiser to establish a suitable end-tidal agent concentration. Both factors would increase the GHG emissions, as the majority of volatile environmental impact comes from direct atmospheric release rather than agent manufacture. 18 This model also assumes steady-state anaesthesia maintenance and ignores the fractional inspired concentration gradient required to deliver an expired concentration of, for example, 2% sevoflurane. This, therefore, underestimates the CO2 emissions from volatiles. Some arguments against reducing GHG emissions attributable to anaesthesia include an assumption that using low flow anaesthesia results in more acceptable levels of GHG emissions. Our conservative model demonstrates that the contribution from desflurane would remain far greater than sevoflurane, even when used at very low flows.
We also chose a fresh gas flow rate of only 500 ml/min for desflurane because most anaesthetists understand the cost and environmental implications of anaesthetic gases, and we wanted to assume a ‘best-case’ scenario based on observed practices in our institution. Even at low flows, the carbon footprint of desflurane was around 80% of total volatile-related GHG emissions despite only contributing a maximum of 17% of all anaesthetic hours in the model. If desflurane were used at a fresh gas flow rate of over 500 ml/min, the implications for CO2e and cost are considerably greater. A survey of anaesthetist practices in 2019 demonstrated that most Australian and New Zealand College of Anaesthetists respondents already use low flow volatile anaesthesia. However, this is sometimes contextualised as a justification for continued use of desflurane, despite representing low-value care, which is where healthcare comes at a higher cost for little benefit. 19 Some argue that desflurane is insignificant compared with other GHGs, yet desflurane has been detected in the atmosphere. Although its use may be declining, use in 2022 will continue to exert a GHG effect until 2036 owing to its long atmospheric life. 20
Several assumptions were made for estimating our GHG emissions from propofol TIVA, which likely overestimate its environmental impact. This is because it assumes that one EEG monitor is used per hour of TIVA, which may overestimate the CO2e for longer cases and in cases where EEG monitoring may not be routinely used. We also assumed that no EEG monitors were used for volatile anaesthetic cases, underestimating the GHG emissions for volatile anaesthetics. This model also assumed that two 100 ml saline bags and remifentanil were used per hour of TIVA, which is not always the case in our institution. Regardless, overestimating the impact of TIVA still resulted in carbon emissions that were lower than for all volatiles and responds to a commonly encountered misperception regarding the environmental impact of plastic disposables associated with TIVA, although longer cases will require more plastic disposables. Propofol is not without environmental harm, though, as it is toxic to some aquatic species and can enter waterways if not appropriately destroyed by incineration.21,22 In Australia pharmaceutical waste is required to be high-temperature incinerated. 23 Additionally, our study assessed only financial and environmental impacts and did not assess any patient outcomes.
Our data highlight the need to make objective, evidence-based decisions when minimising environmental impact, and to avoid biased and subjective perspectives. For example, it is easier to ‘see’ an environmental impact due to plastic waste and more difficult to ‘see’ the invisible yet greater environmental impact of volatile anaesthetic agents that are scavenged and released from hospital roofs. The lifecycle analysis of Sherman et al. showed that the carbon footprint of one hour of dose-equivalent propofol TIVA, including two syringes, extension line, 50% drug wastage, incineration of wasted drugs and disposable equipment and the energy to power the syringe driver has an environmental impact that was 10,000 times less than an equivalent anaesthetic delivered by desflurane at one litre per minute. 18 In Sherman and colleagues’ research, the environmental impact of propofol was largely derived from the energy used to power the syringe driver. Allen and Baxter’s estimate for TIVA used a UK energy estimate, which has a greater renewable energy mix than VIC, Australia. 12,24 However, the Victorian Government has pledged to power all hospitals with renewable energy by 2025, suggesting that the CO2e of propofol TIVA in VIC is likely to fall over time. 25
We also assumed that all maintenance anaesthesia from propofol was delivered by 500 mg vials only; however, this does not account for the 200 mg vials used to replenish propofol syringes during maintenance anaesthesia. The propofol volume required will vary with patient characteristics; however, we aimed to estimate the implications of agent choice using ideal conditions and in general terms.
Our findings have several clinical implications. Additional to the significant environmental benefits that accompany the reduction and removal of desflurane from routine anaesthetic practice are the financial gains for departments that opt to limit desflurane use. Removing desflurane from immediate availability on anaesthetic machines has several benefits. First, it creates a small access barrier to an anaesthetist selecting desflurane and, therefore, encourages the department’s inherent cost-saving and environmental benefit. Second, it prevents desflurane from being wasted in routine daily machine checks where it is not intended to be used. Although data for other machines in use at our institution were not available, a small but cumulatively important financial saving can be realised by simply removing desflurane from storage on the machine. Third, it allows for the enculturation of a new normal clinical practice for those who routinely use desflurane, which may pave the way to its eventual removal from standard anaesthetic practice.
In conclusion, our study provides insights into the impacts of anaesthetic agent procurement in a university teaching hospital. Further, these findings can inform health economic decisions to determine the most appropriate financial resource allocation approach in delivering care to patients. The economic implications of anaesthetic agent choice may appear individually insignificant but, on a larger scale, they can lead to cumulatively substantial financial gains. In addition, this health economic and environmental evaluation indicates that anaesthesia agent choices may reduce the cost and environmental harm of anaesthesia.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221129291 - Supplemental material for The financial and environmental impact of purchased anaesthetic agents in an Australian tertiary hospital
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221129291 for The financial and environmental impact of purchased anaesthetic agents in an Australian tertiary hospital by Jessica F Davies, Ljubiana Trajceska, Laurence Weinberg in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no conflicting interests for the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.