
Abstract
The most appropriate method to predict postoperative outcomes in patients with severe obesity undergoing elective non-bariatric surgery is not known. We conducted a single-centre prospective cohort study in patients with a body mass index of at least 35 kg/m2 undergoing non-bariatric, non-cardiac surgery. Patients completed the six-minute walk test prior to surgery. Disability was measured before and six months after surgery using the World Health Organization disability assessment schedule. Primary outcome measures included quality of recovery at one month and significantly increased disability at six months after surgery. A total of 293 patients participated. The median body mass index was 41 kg/m2. Patients generally recovered well. Following surgery, 9% of patients experienced a poor quality of recovery and 7% developed a significant increase in disability. The proportion of patients free from clinically significant disability increased from 66% prior to surgery to 90% at six months after surgery. The distance walked in six minutes was weakly predictive of poor recovery at one month and significantly increased disability at six months; weight and body mass index were not. The area under the receiver operating characteristic curve was 0.65 (95% confidence intervals 0.51 to 0.78) for poor recovery and 0.64 (95% confidence intervals 0.51 to 0.77) for increased disability. A preoperative six-minute walk test distance of 308 m was the best cut-off value for predicting increased postoperative disability (sensitivity 0.68, specificity 0.63). The six-minute walk test was most discriminatory at shorter distances. This population of patients with severe obesity appeared to recover well and had few adverse outcomes. The degree of functional capacity was more important than the degree of obesity in predicting postoperative outcomes.
Introduction
The prevalence of severe obesity defined as a body mass index (BMI) greater than or equal to 35 kg/m2 has doubled in the past two decades. 1 Most of the literature suggests that patients with severe obesity have higher rates of clinical complications in the postoperative period than the non-obese,2,3 although this has not been universally reported.4–7
The optimal method of preoperative assessment to predict risk in patients with severe obesity has not been determined. Functional capacity is an important concept and can be evaluated in several ways. Recent work has shown that patient self-reported metabolic equivalents (METs) are not associated with objective measures of fitness or with death or poor cardiac outcomes.8–10 Direct measures of exercise capacity such as cardiopulmonary exercise testing (CPET) are more useful yet require significant resources. 8
The six-minute walk test (6MWT) has been used to estimate functional capacity and correlates well with CPET in healthy adults. 11 It is reliable in individuals with obesity and a reference equation for normal values in obesity has been published.12–14 Although it has been used in the setting of bariatric surgery and some specific high-risk surgeries, its value in patients with severe obesity undergoing a wide range of non-bariatric surgery has not previously been investigated.15–18 We have previously published data on 6MWT distances achieved by surgical patients with severe obesity. 19 The 6MWT distances were lower than expected, with the mean being 150 m lower than predicted, and 22% of patients were unable to walk for a total of six minutes. 19 That paper also provided detailed information on other aspects of this population of patients, with high levels of comorbidity and disability that were not apparent on routine clinical assessment. This current publication reports the association between preoperative 6MWT distances and postoperative recovery measures in the same group of patients.
Patient-centred outcomes after surgery are increasingly recognised as important. 20 Short-term postoperative recovery can be measured using the 15-item Quality of Recovery score (QoR-15). 21 The World Health Organization Disability Assessment Schedule 2.0 (WHODAS) was developed for use in the general population, and has since been validated in varied patient groups including obese populations.22–25 It is an acceptable, valid and reliable measure of new disability and disability-free survival after a range of types of major surgery.23,26
We investigated the ability of a preoperative 6MWT to predict postoperative functional recovery and adverse outcomes in patients with severe obesity undergoing non-bariatric surgery. The primary aim was to determine if the distance walked in a preoperative 6MWT would predict postoperative quality of recovery measured by the QoR-15 at one month and a significant increase in disability between baseline and six months as measured by the WHODAS. The secondary aim was to investigate whether a preoperative 6MWT would predict the incidence of postoperative adverse medical events at one month in these patients.
Methods
Design
We performed a prospective single-centre cohort study in Wollongong Hospital, NSW, Australia, in 2016–2018. Ethics approval was granted by the local regulatory body (HE15/379) in February 2016 and the trial was registered with the Australian and New Zealand Clinical Trial Registry (ACTRN12615001264572). Wollongong Hospital is an outer metropolitan general tertiary hospital with 350 beds and 15 operating theatres, and performs approximately 13,000 operations per year of all types excluding cardiothoracic and complex paediatric procedures. The methods for recruitment of participants and collection of preoperative data were described in our previous paper on 6MWT distances achieved by this cohort of surgical patients with severe obesity. 19 The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement guidelines were followed in reporting this study.
Study outcomes
The primary outcomes were quality of recovery measured by the QoR-15 at one month after surgery, and a significant increase in disability between baseline and six months after surgery as measured by the WHODAS. The secondary outcome was the incidence of adverse medical outcomes at one month.
The QoR-15 score ranges from 0 to 150, with less than 112 considered to represent poor recovery. 27 This was measured at three and 30 days. Patients completed the WHODAS in the pre-admission clinic at baseline, and at one month and six months after surgery. Scores were converted to percentages as previously described, ranging from 0% (no disability) to 100% (complete disability). 23 A significant increase in disability was defined as an increase of 8% or more from the baseline score. 23 At the time of the study design, this was defined as ‘new’ disability. As the definition of ‘new’ disability has since been modified (increase in WHODAS score of >8% to a final score of >25%), 26 we used the original definition according to our protocol but re-defined this to represent a significant increase rather than new onset. A WHODAS score of greater than or equal to 25% was defined as clinically significant disability at the time of study design, although this has also recently been updated. 28 Disability-free survival was defined as a patient who is both alive and disability free (WHODAS < 25%). Anaesthesia charts were accessed through the electronic medical record system and interrogated for information on airway, intraoperative and immediate postoperative management. The electronic medical record was searched at 30 days for evidence of postoperative medical adverse events using definitions from the REASON study. 29
Statistics
Statistical analysis was completed using SPSS (V 23; IBM Corp., Armonk, NY, USA). All patients who consented to the study and attempted the 6MWT were included. For the primary outcome analysis we anticipated the correlation coefficient to be 0.5 as the outcomes are somewhat but not completely associated, and chose the confidence intervals to be no wider than ±0.1. A sample size of 219 participants was necessary to satisfy these requirements. We aimed to recruit approximately 250 patients to allow for losses in recruitment and follow-up of approximately 10%.
For the primary outcome of correlation between 6MWT distance and one month QoR scores, data were assessed for a linear association both graphically using scatter plots and analysed in a correlation matrix to determine Pearson’s correlation coefficient. If a linear relationship was found to exist, simple linear regression was used to calculate R2. The association between 6MWT distances and increased disability was assessed by Student’s t-test. The ability of the 6MWT to differentiate between good and poor QoR-15 scores and to predict significant disability was analysed with the receiver operating characteristic method. Sensitivity and specificity analyses were conducted to look for cut-off values for the 6MWT distances. Data for the secondary hypothesis were handled in the same manner. A multivariate analysis was also performed to investigate which of the preoperative variables was most predictive of outcomes. The 6MWT distance, BMI, waist circumference, age, American Society of Anesthesiologists (ASA) physical status class, baseline WHODAS, forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC), serum bicarbonate, and N-terminal pro B-type natriuretic peptide (NT-proBNP) levels were included in the model.
Results
Patient characteristics
We approached 406 eligible individuals for recruitment. Approximately 25% (n = 111) declined, with the most common reasons being not interested, having pain in legs or body, and physical limitations such as being in a wheelchair (see Supplementary Table 1). Two patients were excluded after erroneous enrolment. The range of patient BMIs in the study group was 35–63, with a range of 35–73 in the group that did not consent. The median BMI in both groups was the same (41 kg/m2) (see Supplementary Table 2). No further information was collected for patients who declined or were excluded.
A total of 293 patients participated in the study over 18 months (Figure 1). Their morphology characteristics have previously been reported. 19 Perioperative data are shown in Table 1. Just over half of the patients were female. Twenty-two percent were aged 70 years or over. The mean weight was 115 kg and the mean waist circumference was 127 cm. Ninety-six percent of patients were classified as having an ASA physical status class of 2 or 3 and 79% underwent either moderate or major surgery of varying types. Twelve patients (4%) were admitted to critical care beds postoperatively. More patients had unplanned destinations that were downgraded (high dependency unit (HDU) to ward) than were upgraded (ward to HDU). Two anaesthesia charts were missing from the electronic medical record system so could not be analysed.
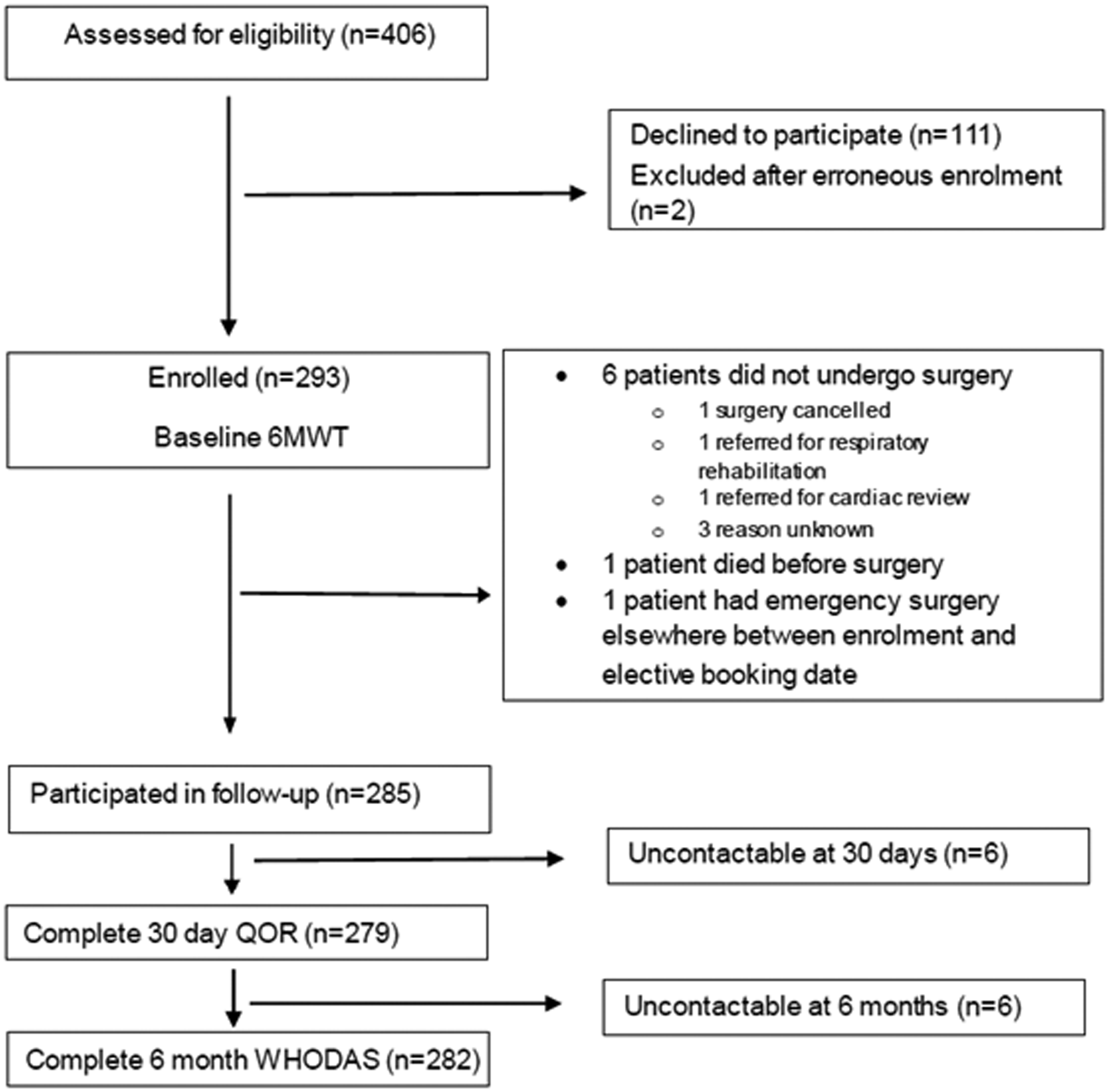
CONSORT diagram of patient flow. 6MWT: six-minute walk test; QOR-15: 15-point Quality of Recovery score; WHODAS: World Health Organization disability assessment schedule.
Perioperative patient characteristics.
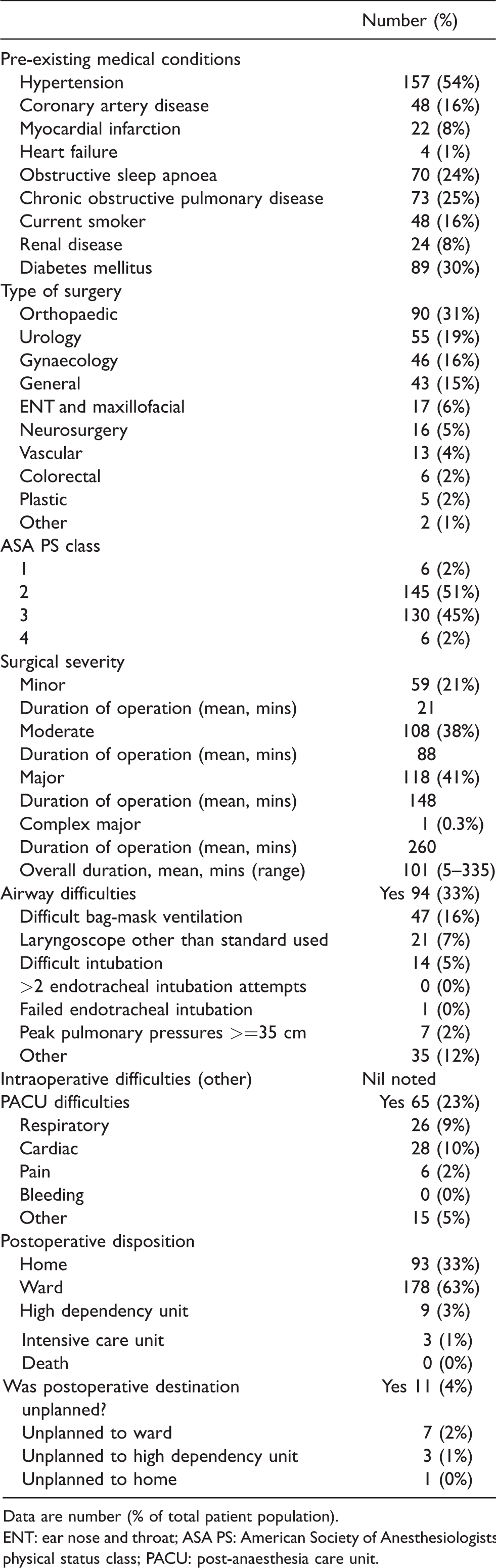
Data are number (% of total patient population).
ENT: ear nose and throat; ASA PS: American Society of Anesthesiologists physical status class; PACU: post-anaesthesia care unit.
Preoperative six-minute walk test
As previously reported, the mean distance walked in the 6MWT was 322 m (standard deviation 137m). Sixty-four patients (22%) were not able to walk for six minutes, with the most common reasons being pain in joints, limbs or back in 74% and shortness of breath in 25%. Those who stopped early were significantly older than those who did not (mean age 66 years versus 56 years, P < 0.001) but had similar mean BMIs (43 kg/m2 versus 42 kg/m2, P = 0.5). No adverse events occurred.
Disability
Prior to surgery, 99 patients (34%) met the criteria for clinically significant disability. Thirteen of the 14 patients with moderate or severe disability were booked for moderate or major surgery. Near complete follow-up was achieved, with 279 patients completing a WHODAS at one month and 282 at six months. Patients tended to have less disability after surgery, with 16% meeting the criteria for clinically significant disability at one month and 10% at six months. Nineteen patients (7%) had developed significantly increased disability at six months after surgery. Patients who developed increased disability had a lower mean 6MWT distance than those who did not (256 m versus 327 m, P = 0.03) but had similar baseline WHODAS scores (both mean 19%) and BMIs (43 and 42 kg/m2). Disability-free survival occurred in 253 patients (90%) at six months after surgery.
Linear regression analysis showed a weak but statistically significant association between the 6MWT distance and increased disability at six months (Figure 2(a)). The difference in distance walked between those who did and those who did not develop increased disability was 70.4 m (95% confidence intervals (CI) 6.8 to 134, P = 0.03). The distance walked accounted for 12.2% of the variation in the WHODAS score at six months. BMI did not correlate with significantly increased disability (r = 0.039, P = 0.52).
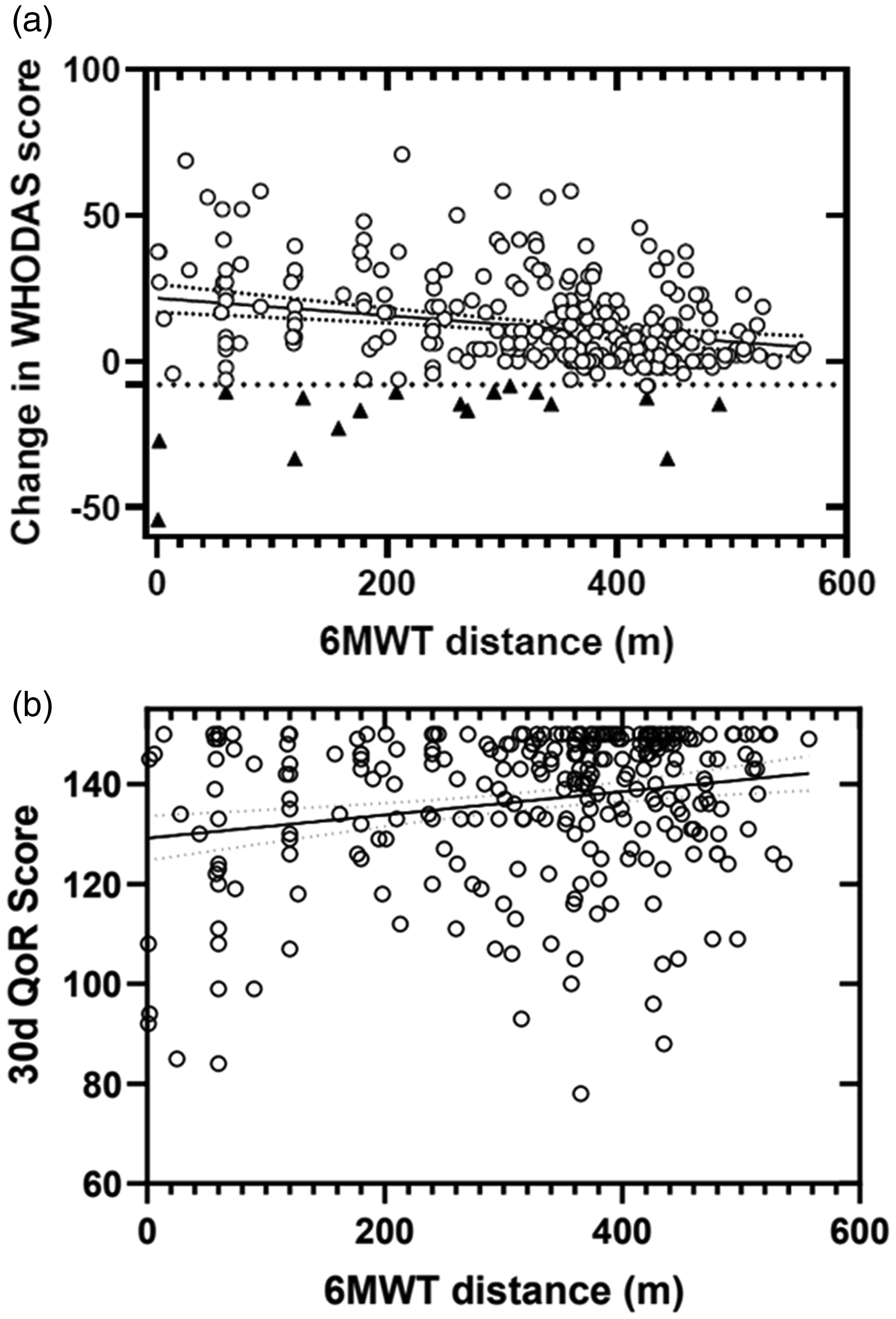
Correlation between the six-minute walk test (6MWT) distance and the primary outcomes. (a) Correlation between the 6MWT distances and change in the World Health Organization Disability Assessment Schedule 2.0 (WHODAS) (%) from baseline to six months. Black triangles represent patients with 8% or greater increase in disability (n=19); black circles represent all other patients (n = 263). (b) Correlation between the 6MWT distances and the quality of recovery (QoR-15) score at 30 days. Black circles represent all patients (n = 279).
We also analysed the WHODAS as a continuous variable. Those with the furthest baseline 6MWT distances had a greater improvement in disability score at six months. For every 10 m increase in 6MWT distance, the WHODAS score decreased by 0.16 units (P = 0.001) and the odds of developing increased disability reduced by 0.3% (95% CI –0.4 to –1, P = 0.034).
The 6MWT distance could be used to predict a WHODAS score at six months using the following equation:

Quality of recovery
At three days after surgery, 281 patients completed the QoR-15, with a median score of 130 (interquartile range (IQR) 113–141, total range 31–150), and 61 patients (22%) met the criterion for poor recovery. The QoR-15 was completed by 279 patients at one month. Most had recovered well, with a median QoR-15 score of 142/150 (IQR 130–148, total range 78–150). Poor postoperative recovery occurred in 24 patients (9%).
Both linear and non-linear tests of association were attempted, with little difference in goodness of fit, so a linear model was used for further analysis. Linear regression found a weak but statistically significant association between 6MWT distances and one month QoR-15 (Figure 2(b)). For every 10 m increase in 6MWT distances, the QoR-15 score increased by 0.23 units (95% CI 0.007 to 0.039, P = 0.005). The distance walked accounted for 4.1% of the variation in QoR-15 at one month. Most one-month QoR-15 scores were good, which gave a ceiling effect to the analysis. BMI did not correlate with QoR-15 (r = 0.041, P = 0.5).
Predictive ability of the six-minute walk test
The area under the receiver operating characteristic curve for the 6MWT to predict significantly increased disability was 0.641 (95% CI 0.507 to 0.774). For the prediction of poor QoR-15 at 30 days, the area under the curve was 0.646 (95% CI 0.513 to 0.778). The optimal cut-off value for predicting increased disability at six months was 308 m (sensitivity 0.68, specificity 0.63, index 1.31). Analysis using this value revealed a low positive predictive value (18%) but high negative predictive value (96%) for the test (Table 2).
Predictive analysis using a six-minute walk distance cut-point of 308 m.

Figures are % (95% confidence intervals).
Other analyses
In the multivariate analysis, baseline WHODAS was the only variable that was predictive of a poor QoR-15 at one month (P = 0.000) and none of the variables significantly predicted increased disability at six months.
We also compared day stay patients to those who stayed at least one postoperative night. The 93 (33%) day stay patients had lower preoperative WHODAS scores than the overnight patients (mean 15.4 versus 20.1, P = 0.008). Their level of disability improved on average at six months postoperatively but the overnight stay patients improved more (mean improvment in WHODAS +8.0 versus +13.8, P = 0.002). Day stay patients had a higher QoR-15 score at one month than patients who stayed at least one night, but the difference was not significant (mean 139 versus 135, P = 0.067).
Due to the unexpectedly high number of patients who could not walk for six minutes, we compared data between this group and all others who completed the test. Patients who could not walk for six minutes had significantly higher mean disability scores both at baseline (P < 0.001) and at six months (P = 0.004) and a lower QoR-15 score at one month (P = 0.011) (Table 3).
Patient outcomes by six-minute walk test completion group.
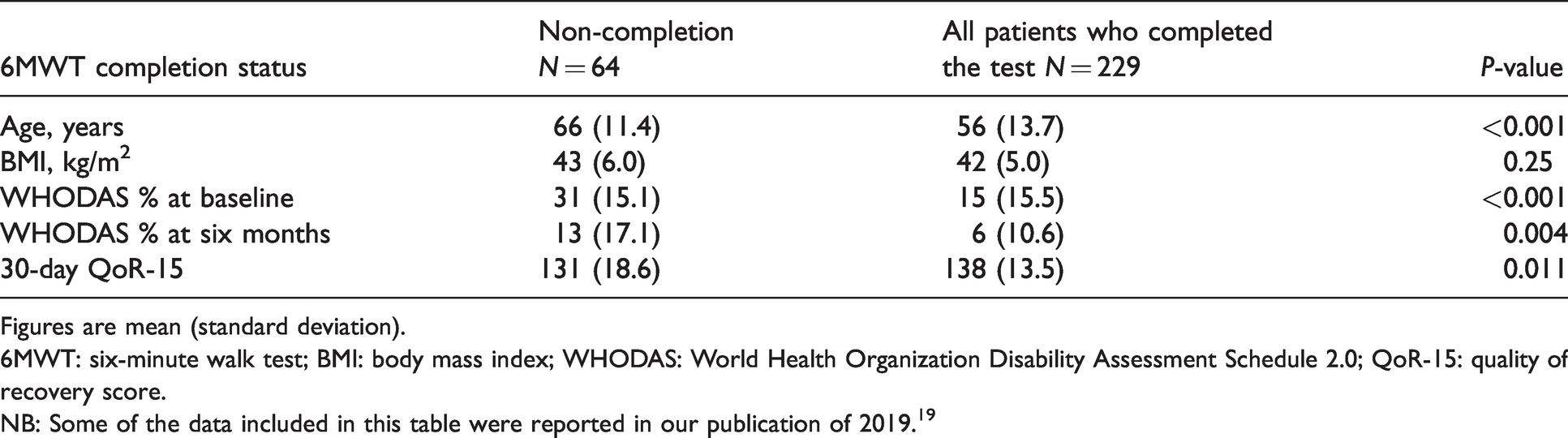
Figures are mean (standard deviation).
6MWT: six-minute walk test; BMI: body mass index; WHODAS: World Health Organization Disability Assessment Schedule 2.0; QoR-15: quality of recovery score.
NB: Some of the data included in this table were reported in our publication of 2019. 19
Secondary outcome: medical complications
Twenty-three (8%) patients had one or more documented medical complication at 30 days postoperatively (Table 4). Their median age was 62 years (IQR 57–73, total range 47–82). Seventy percent of the patients who experienced complications had a preoperative ASA physical status class of 3, and 83% underwent major or complex major surgery. Only four patients (1%) had three or more complications: these patients were aged between 53 and 82 years, had a range of BMIs from 36 to 46 kg/m2 and a range of 6MWT distances from 1 to 436 m. All four of these patients developed acute renal impairment and wound infection, with other complications including systemic sepsis, acute angina, acute pulmonary oedema and reintubation. There were no deaths by six months postoperatively. There was no association between either the preoperative 6MWT distances or BMI with the number of medical complications at six months. Due to the small number of patients with more than one complication, further analysis was not pursued.
Incidence of complications by postoperative day 30.
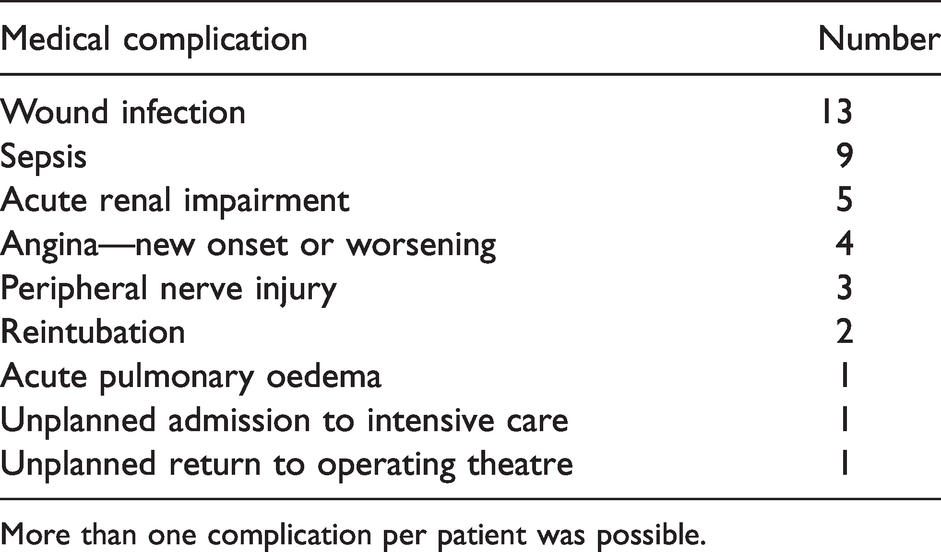
More than one complication per patient was possible.
Waist circumference, waist-to-hip ratios, spirometry values, serum bicarbonate values and NT-proBNP levels were not significantly associated with the QoR-15 at one month, increased disability at six months, or the frequency of medical complications (P values for all calculations >0.5).
Discussion
In this cohort of almost 300 patients with severe obesity undergoing a wide range of operations, the distance achieved during a 6MWT prior to surgery was weakly associated with the quality of recovery at one month and the development of significantly increased disability at six months after surgery. Most patients were functionally better after their operation than they were before: only 7% developed significantly increased disability and only 9% scored their recovery as poor. The small number of patients with poor outcomes limited the ability of the study to investigate the predictive ability of the 6MWT more definitively.
This cohort of patients had severe obesity. By definition, all had a BMI of 35 kg/m2 or over. Every patient had a waist circumference measurement above the limits associated with adverse health outcomes. 30 Their level of disability preoperatively was higher than has been reported in general populations: 34% in our study compared to reports in other patient groups of 27% and 18%.23,26 Their 6MWT distances were much lower than previously reported (see below). Our institution is an outer metropolitan hospital with moderate resources. Despite all of these factors, patient outcomes were generally good. Our median quality of recovery score at one month was 130, which compares well to the score of 133 found in previous work in general surgical patients. 26 Only 7% developed increased disability at six months, which is similar to the proportion of 9% in the general population. 26 One-third of our patients were disabled before surgery but only 10% were disabled six months after surgery. Those having operations requiring an overnight stay were more disabled preoperatively but showed greater improvement in their disability level at six months postoperatively than patients having day stay operations. It appears that the majority of patients in this cohort benefited from their surgery. Our findings suggest that severe obesity and disability are probably not valid reasons to withhold non-bariatric surgery in most patients. Patients with low functional capacity such as a low 6MWT distance may benefit from further preoperative assessment to inform shared decision-making.
6MWT distances in this population were lower than previously described. 6MWT distances in healthy normal weight individuals have been reported as approximately 600 m, with mean distances of 450–475 m in people with BMIs of 37 and 42 kg/m2.14,31,32 The reported value closest to our finding of 322 m is a mean 6MWT distance of 339 m, and was described in a cohort of non-surgical patients with a mean BMI of 51 kg/m2. 33 The potential reasons in our study include the high proportion of elderly patients, the high prevalence of disability, or the presence of a surgical condition. Individuals with severe obesity may be reluctant to participate in a walking test, as suggested by the reasons given by people who declined enrolment in our study, such as walking being too difficult or too painful. Even after agreeing to such a test, they may find that walking in a monitored situation requires more effort than they had anticipated or were prepared to do, and therefore produced a result lower than expected. 34
Patients who were unable to complete the 6MWT had worse postoperative outcomes than those who completed the test. The interaction between obesity, disability, comorbidities and functional capacity has previously been explored, albeit not in surgical patients.25,35 In our multivariate analysis, the baseline level of disability significantly predicted the quality of postoperative recovery but no other outcomes. Our study found age to be associated with both the 6MWT distance and baseline WHODAS, whereas weight and BMI were not. The complex interaction between disability and functional capacity in surgical patients with obesity could be investigated further in the future and could include modelling with direct measures of CPET and allometric scaling for body mass.
It is not reasonable to expect one simple test to have a powerful predictive ability in itself. Including other variables in the risk analysis did not increase the predictive ability in our study, so we could not construct a multivariate model. The negative predictive value of the 6MWT was high, suggesting that if a surgical patient with severe obesity can walk over 308 m, they are likely to do well postoperatively. This is similar to the CPET concept of an anaerobic threshold cut-point of 9–11 ml/kg/min. 36 The 6MWT distance of approximately 300 m has been suggested as a cut-point in many other studies, albeit in non-obese populations with a wide range of medical conditions.15,17,37,38 Those who walk less than this distance or who cannot complete the test may benefit from further investigation or more meticulous management plans. Our difference of approximately 70 m between patients with good and poor disability outcomes agrees with the suggested values of a 6MWT minimally clinically important difference of between 50 and 80 m. 39
While it is difficult to compare different study populations directly, the 8% incidence of serious adverse medical outcomes in our study is similar to that published in other populations including but not limited to patients with obesity. Other reports of postoperative complication rates vary from 4% to 15%.2,5,7 In our study, the patients in whom complications occurred were of a similar age to the overall cohort but had more serious comorbidities preoperatively, and more of them underwent major rather than minor operations. These factors may be more relevant to the development of complications than preoperative weight or disability. We had no deaths or confirmed myocardial infarctions by one month, compared to reported rates in large studies of high-risk patients of 0.5%–1%. 8 As has previously been reported in studies in obesity, complications related to infection were the most frequent in our population.40,41 Our work is consistent with other publications suggesting that obesity in itself does not necessarily predict poor outcomes.5–7 Our study was powered for the primary outcomes, and so provides an estimate of the frequency of adverse medical complications in this population that could be used in future studies designed to address this question.
Patient weight, BMI, waist and hip circumference were not found to be associated with postoperative outcomes related to quality of life. Waist circumference is a theoretically biologically reasonable measure of overall health due to its association with visceral fat and adverse health conditions.30 It has been found to be more predictive than BMI of intraoperative and postoperative medical and surgical complications.41,42 Our study did not find an association with quality of recovery and disability outcomes. One possible explanation is that these patient-centred outcomes may be less influenced by body morphology measures than by more biological outcomes. 6MWT distance was not associated with adverse medical outcomes in our study. It may also be more relevant for patient-centred rather than biological outcomes.
Our study contained patients undergoing a wide range of operations, including but not limited to major surgery, and including low- and high-risk patients according to ASA physical status scores. This makes our findings more generalisable but may have decreased our chances of finding adverse postoperative outcomes. One-quarter of patients approached for this study did not consent, which compares favourably with rates of recruitment in other walking studies in non-obese surgical populations. 8
We used one method to test functional capacity: the relative and additive values of other methods such as other submaximal exercise tests, the Duke activity status index, CPET, or obesity-specific tools could be investigated in future studies. Our data show that we cannot assume that every person with severe obesity is severely disabled or will have poor postoperative outcomes. Patients with limited walking ability may constitute a higher risk group who are suitable for more detailed investigation. We suggest a 6MWT cut-point that can now be tested prospectively in larger groups of patients to determine the predictive abilities of these tests more reliably.
Several general questions arise from this work: does surgery actually improve overall health in patients with severe obesity; what, if anything, should be done preoperatively to mitigate risks in patients with obesity, disability and poor functional capacity; and is it feasible to attempt to do so?
We studied an adult population with severe obesity who underwent a wide range of elective non-bariatric operations. There were few poor postoperative outcomes and an overall improvement in the level of disability. Functional capacity assessed by a 6MWT and disability assessed by the WHODAS were weakly related to postoperative patient-centred outcomes, and were better predictors than the body habitus measures of weight, BMI and waist circumference. The degree of functional capacity was more important than the degree of obesity when assessing postoperative function. We found a walked distance of approximately 308 m to give the best discrimination in this population. We propose that incorporating a measure of functional capacity such as a 6MWT, rather than relying only on patient self-report and weight measures, will improve the preoperative assessment of patients with severe obesity.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20981969 - Supplemental material for Predicting recovery and disability after surgery in patients with severe obesity: The role of the six-minute walk test
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20981969 for Predicting recovery and disability after surgery in patients with severe obesity: The role of the six-minute walk test by Smith Natalie A Conceptualization Data curation Formal analysis Funding acquisition Investigation Methodology Project administration Resources Supervision Writing original draft Writing review editing Batterham Marijka Data curation Formal analysis Writing review editing Shulman Mark A Investigation Methodology Supervision Writing review editing in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
E Lobb: main research assistant. J Paton: help with data management. P Myles: assistance with writing and data analyses. G Peoples: assistance with data analysis and production of figures.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a project grant from the Australian and New Zealand College of Anaesthetists (16/018). Equipment was provided by the Illawarra Health and Medical Research Institute. NT-proBNP testing was supported by an Illawarra Health and Medical Research Institute collaborative project grant (2016).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.