
Abstract
Various perioperative interventions have been demonstrated to improve outcomes for high-risk patients undergoing surgery. This audit assessed the impact of introducing a multidisciplinary perioperative medicine clinic on postoperative outcomes and resource usage amongst high-risk patients.
Between January 2019 and March 2020, our institution piloted a Comprehensive High-Risk Surgical Patient Clinic. Surgical patients were eligible for referral when exhibiting criteria known to increase perioperative risk. The patient’s decision whether to proceed with surgery was recorded; for those proceeding with surgery, perioperative outcomes and bed occupancy were recorded and compared against a similar surgical population identified as high-risk at our institution in 2017.
Of 23 Comprehensive High-Risk Surgical Patient Clinic referrals, 11 did not proceed with the original planned surgery. Comprehensive High-Risk Surgical patients undergoing original planned surgery, as compared to high-risk patients from 2017, experienced reduced unplanned intensive care unit admission (8% versus 19%, respectively), 30-day mortality (0% versus 13%) and 30-day re-admission to hospital (0% versus 20%); had shorter postoperative lengths of stay (median (range) 8 (7–14) days versus 10.5 (5–28)) and spent more days alive outside of hospital at 30 days (median (range) 18 (0–25) versus 21 (16–23)). Cumulatively, the Comprehensive High-Risk Surgical patient cohort compared to the 2017 cohort (both n=23) occupied fewer postoperative intensive care (total 13 versus 24) and hospital bed-days (total 106 versus 212).
The results of our Comprehensive High-Risk Surgical Patient pilot project audit suggest improved individual outcomes for high-risk patients proceeding with surgery. In addition, the results support potential resource savings through more appropriate patient selection.
Keywords
Major surgical procedures are associated with postoperative complications 1 which, if they occur, can significantly reduce patients’ quality of life and substantially increase healthcare costs. 2 Older adults with comorbid conditions are disproportionally affected by postoperative complications. 3 In a British study by Pearse et al., high-risk patients accounted for less than 15% of those treated with surgery but experienced 80% of postoperative complications. 4 The effect of population ageing is more evident in patients referred for surgical procedures than the general population, 5 so meeting the challenge of postoperative complications is likely to continue into the future. An increasing demand on physical and financial healthcare resources, 6 exacerbated by unpredictable events such as the coronavirus disease 2019 (COVID-19) pandemic, 7 means those responsible for allocating healthcare resources can face difficult decisions. Interventions preoperatively and postoperatively can improve perioperative outcomes of high-risk patients,8,9 resulting in more efficient use of health resources.
An established service with preoperative input from a perioperative medical team in both elective and emergency settings is the proactive care of older patients undergoing surgery (POPS) model at Guys and St Thomas’ Hospital in London, England. Since 2003 it has provided a multidisciplinary service of risk assessment, optimisation and collaboration, with the aim of reducing postoperative complications and supporting safe discharge from hospital. Several studies have shown improvements in postoperative complications, including pneumonia, delirium and delayed mobilisation as well as shorter length of stay associated with this model of care. 10 Alongside this evolution in perioperative pathways, healthcare professionals have been encouraged to advocate for patients assuming a leading role in determining their care through shared decision-making. 11 The Choosing Wisely® 12 (American Board of Internal Medicine Foundation, Philadelphia, PA, USA) initiative, initially based in the United States but now a global project, was set up in this spirit. Currently, the Australian and New Zealand College of Anaesthetists (ANZCA) Choosing Wisely recommendations include avoiding initiating anaesthesia for high-risk patients without discussing expected outcomes or goals of care. 13 Despite such recommendations, the uptake and implementation of such principles has been slow. 14
The aim of this audit was to explore whether a pilot perioperative programme, based on the above principles of risk stratification, shared decision-making and targeted intervention for high-risk patients, improved our perioperative outcomes.
Methods
The institution at which this project was carried out is a tertiary referral centre for the lower part of the North Island of New Zealand. The catchment population for tertiary services (neurosurgical, cardiothoracic, urological and upper gastrointestinal surgery) is 500,000 and for secondary services (general and orthopaedic surgery) is 250,000. The main regional hospital performs 9100 elective and 10,000 emergency procedures a year and has around 135 surgeons.
The pilot programme for improvement of perioperative care was delivered through a Comprehensive High-Risk Surgical Patient (CHRISP) clinic. This was a pilot project launched in 2019 by the Capital and Coast District Health Board ((CCDHB), Wellington region, New Zealand) which followed New Zealand Medical College’s Choosing Wisely principles. 15 The CHRISP programme aimed to improve perioperative outcomes for elective surgical patients deemed ‘high risk’. The key principles of perioperative medicine utilised, included: shared decision-making, optimisation of medical comorbidities and collaborative behavioural change. 16
To evaluate the impact of this new service, the CHRISP pilot project was presented to the CCDHB audit review committee in January 2019. The CCDHB audit review committee approved the collection of data from patients attending the CHRISP clinic and comparison of outcomes against a cohort of high-risk patients who had undergone surgery at the institution previously.
In the pilot programme, patients aged 65 years and older, with significant underlying comorbidities and being considered for surgery, were invited to attend the clinic with a support person. These patients were identified in surgical clinic by one of the surgical team using the criteria shown in Table 1. The CHRISP clinic involved 90 minutes of patient contact with subsequent discussion between the clinic team members. The format included: a comprehensive geriatric assessment; completion of the Rockwood clinical frailty scale; screening for cognitive impairment; and cardiopulmonary exercise (CPEX) testing. Subsequently, an open discussion of perioperative risks, goals of care and alternative treatments, was facilitated by a consultant anaesthetist, consultant geriatrician, and nurse specialist. Following CHRISP assessment, patients could be referred to community allied health professionals and other specialist medical teams as needed. The outcomes of the CHRISP clinic were communicated to the surgical team and primary care using clinic letters as well as verbal discussion when necessary. Possible outcomes of the CHRISP clinic assessment were: proceeding with original planned surgery; an alternative procedure; or conservative management. All patients, whether proceeding with surgery or not, were engaged in advance care planning discussions and received supporting literature to help clarify and document their future preferences.
CHRISP clinic referral criteria and audit inclusion criteria.
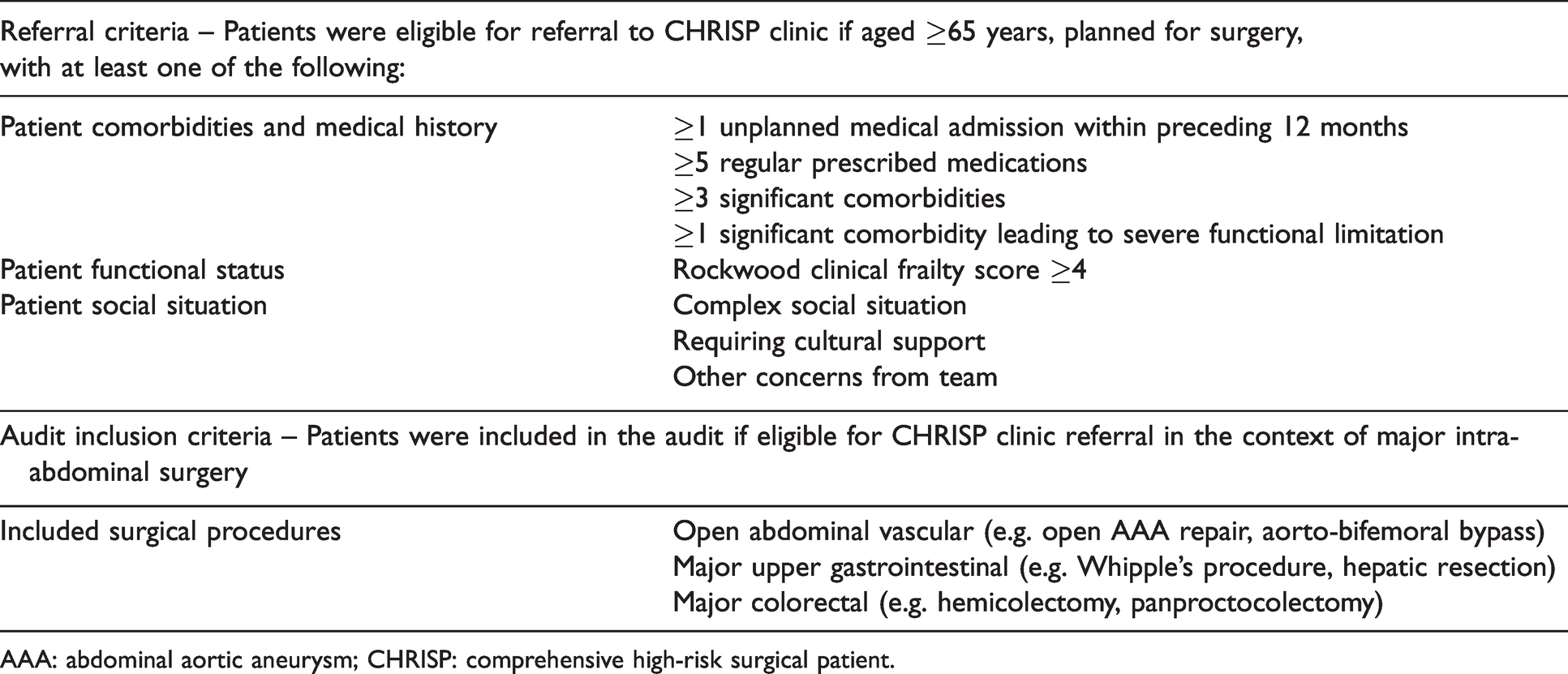
AAA: abdominal aortic aneurysm; CHRISP: comprehensive high-risk surgical patient.
As a pilot project the number of patients attending the CHRISP clinic has been limited by the available clinical resources. Retrospective analysis of anaesthetic records estimates that approximately 120–150 patients undergoing major intra-abdominal surgery could be eligible for referral to the CHRISP clinic every year. This represents 20% of patients 65 years and older listed for vascular, upper gastrointestinal and general surgical procedures, and 10% of the total number of patients listed by these specialties.
Between January 2019 and March 2020, 42 patients attended the CHRISP clinic, referred in the context of proposed surgery ranging from relatively minor procedures; for example, J-J stent replacement, to complex, major surgery. In order specifically to examine those patients most at risk of adverse events, only outcomes for CHRISP patients referred in the context of major intra-abdominal surgery were assessed (Table 1). Through selecting only CHRISP clinic attendees 2019–2020 proposed for major intra-abdominal surgery, a group of 23 patients was generated and their outcomes compared to a matched cohort.
The group of matched patients was generated by first identifying all patients who underwent major intra-abdominal surgery in 2017 and had attended a double-slot anaesthetic pre-assessment clinic (APAC) consultation. At the time, a double-slot APAC consultation represented our institution’s approach for patients identified as high-risk. Thirty-eight patients were identified as having undergone major intra-abdominal surgery and attended a double-slot APAC consultation; to these patients we retrospectively applied the same CHRISP referral criteria (Table 1). By applying these criteria, 23 high-risk patients who underwent surgery in 2017 and who would have been eligible for referral to the CHRISP clinic, were identified; these have been labelled matched patients 2017.
A selection of individual perioperative outcomes, some recently recommended by the standardising end points in perioperative medicine (StEP) initiative, 17 were used to compare outcomes. Clinical indicators were: ICU length of stay; planned and unplanned admission to the intensive care unit (ICU); postoperative length of stay; and re-admission to hospital within 30 days of surgery. 18 Days alive outside hospital at 30 days after surgery (DAOH30) 19 was also included as a patient-centred outcome measure. Total postoperative surgical bed-days and ICU bed-days were also calculated for each cohort.
Hospital electronic and paper healthcare records were accessed to collect perioperative data using a standard template, and the information was collated using Excel (Microsoft, Redmond, WA, USA). The normality of numerical data was assessed using Q-Q plots and the Shapiro–Wilk test. It was not possible to state confidently that the numerical data were normally distributed, therefore the Mann–Whitney U test was used to assess for statistical significance and presented as P- values. Regarding categorical data, due to small sample sizes, Fisher’s exact test was used to assess for statistical significance. Odds ratios (ORs) and associated confidence intervals (CIs) were calculated for categorical variables. Statistical analysis used R (the R Foundation, Auckland, New Zealand) software and prediction of future sample sizes was made using G*Power (Heinrich-Heine University, Düsseldorf, Germany) software.
Results
Characteristics of the comparison cohort of matched patients from 2017 and CHRISP clinic attendees 2019-2020 and CHRISP clinic attendees 2019-2020 are summarised in Table 2; the characteristics of CHRISP clinic attendees who did proceed and did not proceed with the original planned surgery have been presented separately. In summary, of the 23 patients referred to the CHRISP clinic for assessment before planned major intra-abdominal surgery, 12 proceeded with the original proposed surgery. Of those 11 patients who did not proceed with the original surgery, eight patients underwent non-surgical management, while three patients were referred for endovascular procedures.
Characteristics of matched patients from 2017 and CHRISP clinic attendees 2019–2020.
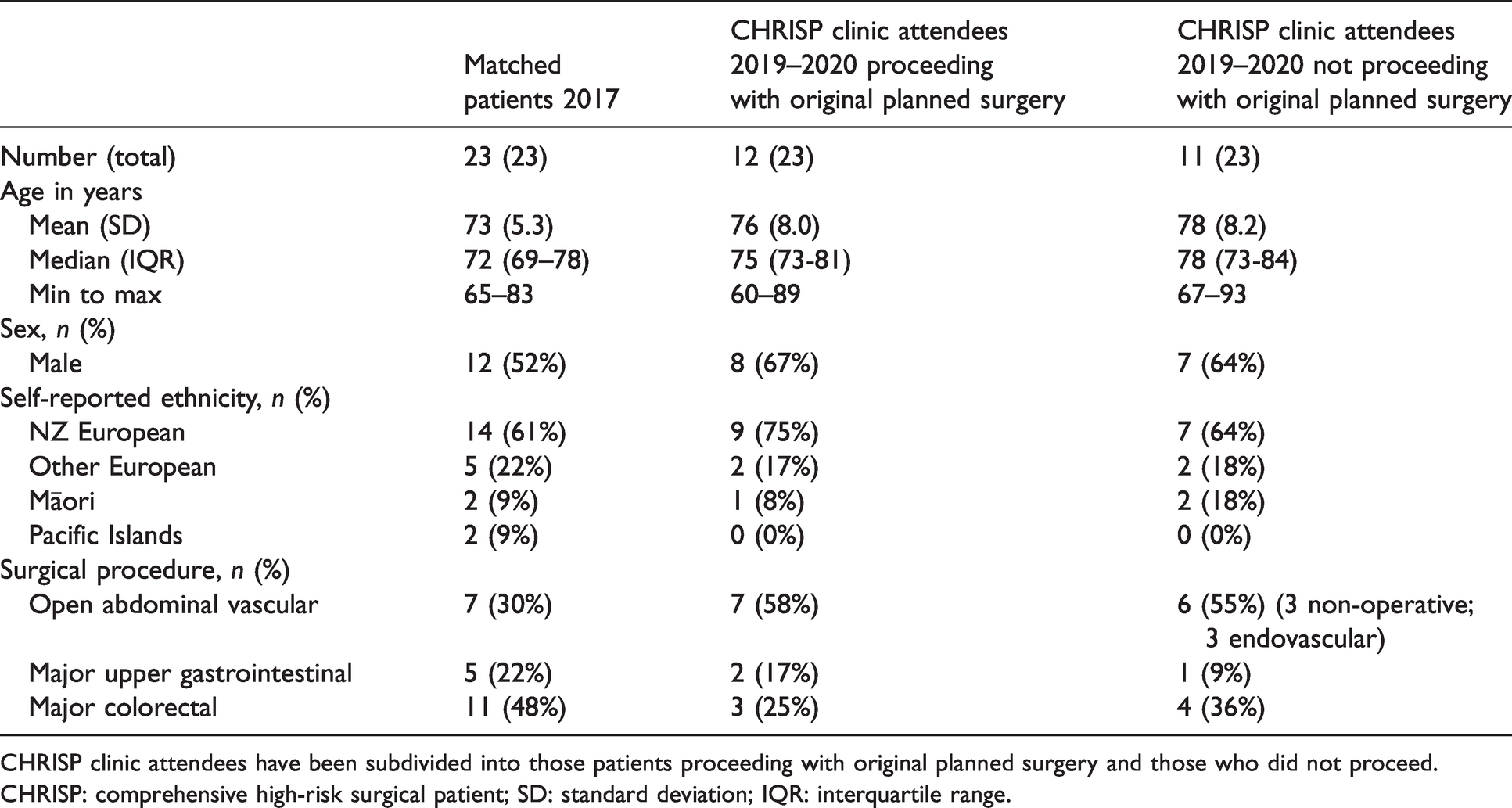
CHRISP clinic attendees have been subdivided into those patients proceeding with original planned surgery and those who did not proceed.
CHRISP: comprehensive high-risk surgical patient; SD: standard deviation; IQR: interquartile range.
A summary of the perioperative outcomes for matched patients 2017 and CHRISP clinic attendees 2019–2020 proceeding with original planned surgery is shown in Table 3. The overall ICU admission rate was higher in the CHRISP patients proceeding with surgery compared to matched patients (75% versus 57%; P = 0.4630; OR 2.308, 95% CI 0.492 to 10.818); however, the unplanned ICU admission rate was lower in the CHRISP patients (8% versus 19%; P = 0.6301; OR 0.386, 95% CI 0.038 to 3.927). The ICU length of stay was shorter in CHRISP patients proceeding with surgery versus matched patients (median (range) 1.8 (0.9–2.0) days versus 1.9 (0.2–4.1) days; P = 0.4621). As a cohort, the CHRISP patients who proceeded with surgery occupied fewer total ICU bed-days in comparison to matched patients (13 days versus 24 days).
Comparison of perioperative outcomes for matched patients from 2017 and CHRISP clinic attendees 2019–2020 proceeding with original planned surgery.
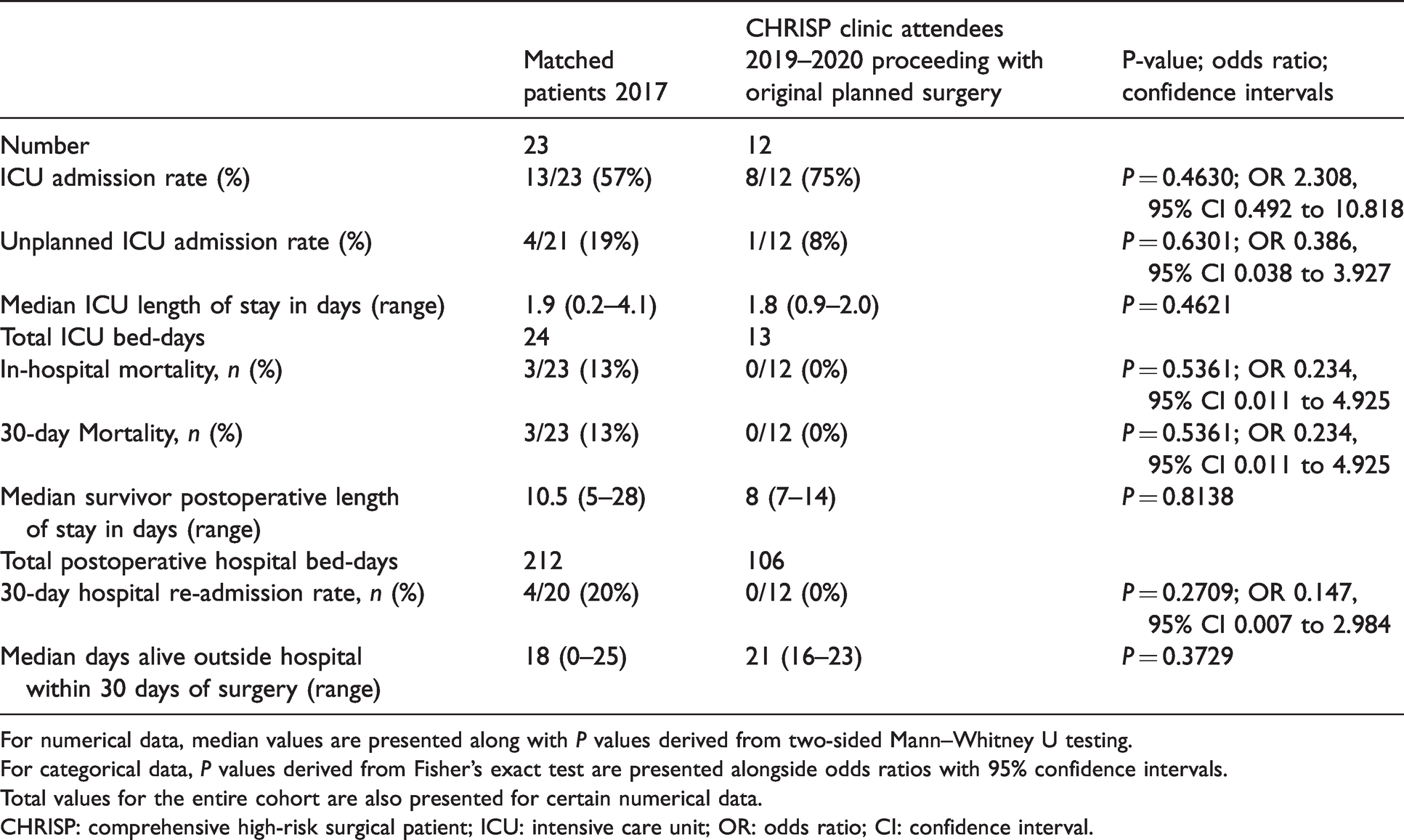
For numerical data, median values are presented along with P values derived from two-sided Mann–Whitney U testing.
For categorical data, P values derived from Fisher’s exact test are presented alongside odds ratios with 95% confidence intervals.
Total values for the entire cohort are also presented for certain numerical data.
CHRISP: comprehensive high-risk surgical patient; ICU: intensive care unit; OR: odds ratio; CI: confidence interval.
Regarding mortality, both in-hospital and 30-day mortality were lower in the CHRISP patients who proceeded with surgery versus the matched patients (both 0 versus 13%; P = 0.5361; OR 0.234, 95% CI 0.011 to 4.925). Of those patients who survived, the median length of postoperative hospital stay was lower in the CHRISP patients who proceeded with surgery compared to the matched group (median (range) 8 (7–14) days versus 10.5 (5–28) days; P = 0.8138). The proportion of CHRISP patients re-admitted to hospital within 30 days of surgery was lower in comparison to matched patients (0 versus 20%; P = 0.2709; OR 0.147, 95% CI(0.007 to 2.984)). The median DAOH30 was higher in the CHRISP patients proceeding with surgery in comparison to the matched group (median (range) 21 (16–23) days versus 18 (0–25) days; P = 0.3729). As a cohort, the CHRISP patients who proceeded with surgery occupied fewer total postoperative hospital bed-days in comparison to matched patients (106 days versus 212 days).
In the group that did not proceed with the original planned surgery, at the time of writing none had died or re-presented for emergency surgery. Within this group, two patients referred for alternative endovascular procedures had undergone treatment at the time of analysis; neither was admitted to the ICU and their average length of postoperative hospital stay was 3.5 days.
Discussion
The CHRISP pilot project finished in March 2020 when the COVID-19 pandemic forced a change in the delivery of preoperative care within the region. To review the impact of the pilot we compared the perioperative outcomes of patients attending the CHRISP clinic against a matched cohort of patients from 2017.
It was striking to observe that almost half (48%) of patients referred for major intra-abdominal surgery who attended the CHRISP clinic did not proceed with the original proposed surgery. These findings are in keeping with those recently published by Omundsen et al., who recently introduced a shared decision-making scheme into their perioperative medicine service. 20 It is possible that the extensive shared decision-making discussion presented patients with further opportunity to explore their treatment options, re-evaluating risks and aligning treatment with their goals of care. Some characteristics, for example sex and surgical specialty (see Table 2), were similar between those who proceeded and those who did not proceed with the original planned surgery. However, the median age of those who did not proceed was higher than those who proceeded (78 years versus 75 years). In the group who did not proceed there was a higher proportion of Māori patients (18%, two patients) compared to those who proceeded with the original planned surgery (8%, one patient). It is recognised that shared decision-making risks health inequity through various forms of bias. 21 Should the pilot service continue and expand, systems need to be implemented to ensure the availability of appropriate cultural support to minimise these risks.
Despite some patients electing for alternative treatments, Table 2 is consistent with CHRISP clinic attendees who proceeded with original proposed surgery being similar to matched patients who underwent major intra-abdominal surgery in 2017. The CHRISP attendees who underwent alternative endovascular procedures were not included in this analysis to provide a fairer assessment of the new service’s impact on patients undergoing major intra-abdominal surgery only. Accordingly, we directly compared outcomes between matched patients from 2017 (n = 23) and CHRISP clinic attendees who proceeded with original planned surgery (n = 12). A range of established and recently validated perioperative endpoints was examined; this included clinical indicators such as unplanned ICU admission, 30-day mortality, postoperative length of stay and 30-day re-admission rate, 18 alongside patient-centred outcomes, such as DAOH30. 19 The patients undergoing major intra-abdominal surgery who attended the CHRISP clinic fared better in each domain, compared to the matched group. We can identify no significant changes in the delivery of perioperative care for patients undergoing major intra-abdominal surgery at our institution between 2017 and 2020 to otherwise explain the observed differences. Similar schemes have been demonstrated to produce improvements in perioperative outcomes.8–10 However, studies have also demonstrated increased mortality associated with such interventions; 22 therefore it is encouraging to observe our findings mirroring a trend of improvement.
In addition to improved individual outcomes, it is also interesting to consider the total utilisation of postoperative hospital resources within each group as a cohort. At our institution in 2017, 23 patients undergoing major intra-abdominal surgery occupied 212 postoperative hospital bed-days, of which 24 were ICU bed-days. By comparison in 2019–2020, 23 patients planned for major intra-abdominal surgery attended the CHRISP clinic; 12 patients proceeded with the original planned surgery, occupying 106 postoperative hospital bed-days, of which 13 were ICU bed-days. The finding that halving the number of patients undergoing surgery halves the utilisation of postoperative resources is perhaps unsurprising; however, this clearly illustrates the potential positive impact such preoperative risk stratification and shared decision-making can have on increasingly scarce hospital resources. As previously mentioned, it is important to remember patients electing for alternative endovascular procedures occupied seven postoperative bed-days. Furthermore, while outside the scope of this investigation, it must be acknowledged that many CHRISP attendees opting for non-surgical intervention may have undergone relatively financially costly treatments.
There are several weaknesses to our investigation, many of which are a consequence of selecting a small subset of patients from a single institution. Patients were not randomly selected; within the CHRISP group patients were referred directly by surgical teams and this may have generated selection bias. In our audit, selection bias may have resulted in only receiving referrals from surgeons engaging with the principles of perioperative medicine, thereby improving outcomes. Alternatively, despite the clinic’s emphasis on shared decision-making, it is possible that such bias was generated by surgeons only referring patients whom they wished to not operate on, again improving outcomes. In addition, selecting a cohort from 2017 for comparison introduces the possibility of hitherto unidentified confounding factors underlying the observed differences, rather than any impact of the CHRISP project. Many similar perioperative pilot projects, involving small numbers of patients, lack the necessary statistical power to demonstrate statistically significant differences, instead existing as observational or ‘proof of concept’ studies. 23 Ideally, a randomised control trial with primary outcomes; for example, DAOH30 and secondary outcomes, such as unplanned ICU admission and hospital re-admission, with observer blinding would be conducted. Based on the differences observed from this audit, for a primary outcome such as DAOH30, our statistical analysis would estimate that a minimum of 85 patients would be required within each trial arm.
In conclusion, our CHRISP pilot project demonstrated that introducing a multidisciplinary, shared decision-making clinic for high-risk surgical patients led to a significant proportion deciding not to proceed with major surgery. Our results suggest a combination of avoiding inappropriate surgery and thoroughly optimising patients choosing to proceed can improve an institution’s clinical and patient-centred outcomes for high-risk individuals undergoing major intra-abdominal surgery. These findings are in keeping with studies employing similar principles of targeted enhanced perioperative care. In addition to individual outcomes, the results support potential resource savings by more appropriate patient selection and optimisation. The next phase in the CHRISP project will hopefully see services adequately resourced to expand and include more elective as well as emergency cases, increased cultural support and continued data collection. With ever-mounting pressure on healthcare resources, it is hoped these initial findings will encourage others and contribute to the evidence base supporting the introduction of such schemes.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211017150 - Supplemental material for A multidisciplinary perioperative medicine clinic to improve high-risk patient outcomes: A service evaluation audit
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211017150 for A multidisciplinary perioperative medicine clinic to improve high-risk patient outcomes: A service evaluation audit by Aidan I Fullbrook in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The authors would like to acknowledge the CHRISP clinic nurses and clinical measurement unit staff for their invaluable contribution to the care of their patients.
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.