
Abstract
Intermediate and high-risk patients undergoing surgery are often managed on a surgical ward in the absence of haemodynamic or ventilatory support requirements necessitating intensive care unit or high dependency unit admission. We describe a model of care for the multidisciplinary management of selected postoperative patients and the epidemiology of patients managed using this model at a tertiary Australian hospital.
Of 25,139 patients undergoing inpatient surgery at our institution over a two-year period, 506 (2%) were referred to the Perioperative Medicine team. The median age of patients referred was 74 years; 85% had an American Society of Anesthesiologists physical status ≥3, and 44% underwent emergency surgery. Major complication or death within 30 days was 44.2% (213/482). The most common complications, as defined by the American College of Surgeons National Surgical Quality Improvement Program were transfusion within 72 h (17.4%), pneumonia/aspiration pneumonitis (11.3%), and acute renal failure (10.6%); median time to Medical Emergency Team call was 146 (interquartile range 77–279) h.
Sixty-six percent of referred patients (280/423) required an intervention during their time under the service. This high incidence indicates that this population of patients merits closer attention, including routine measurement and reporting of postoperative outcomes to monitor and improve quality of care at our institution as part of an integrated perioperative service. We believe that with so much current focus on perioperative medicine, it is important we translate this to clinical care by evolving traditional models of management into more innovative strategies to meet the complex demands of today’s surgical patients.
Keywords
Introduction
Perioperative medicine is a multidisciplinary specialty which has evolved in response to an increasing global volume of surgery 1 and an increasingly comorbid patient population. 2 Major postoperative complications occur in 32% of patients who have significant comorbidities (American Society of Anesthesiologists Physical Status (ASA-PS) 3 or 4) when undergoing inpatient elective surgery. 3 Elderly patients are particularly at risk, with 20% developing at least one complication within five days postoperatively. 4 Major postoperative complications predict long-term survival, 5 and early intervention may prevent death after complications (‘failure to rescue’). 6
Intermediate and high-risk patients undergoing surgery are often managed on the ward in the absence of haemodynamic or ventilatory support requirements that predicate an intensive care unit (ICU) or high dependency unit (HDU) admission. Surgical teams increasingly look to involve perioperative physicians and anaesthesiologists to assist with care in these complex patients. The Australian and New Zealand College of Anaesthetists (ANZCA) aims in its 2018–2021 Strategic Plan 7 to create ‘a collaborative, integrated and effective model of perioperative medicine.’ ANZCA are also developing a qualification in Perioperative Medicine which will require clinicians to meet perioperative clinical experience requirements. 8
In the context of high healthcare costs and limited access to critical care beds (e.g. ICU or HDU), alternative models of care involving a multidisciplinary perioperative team targeting the highest-risk patient throughout the perioperative journey is desirable. Postoperative ward rounds by dedicated perioperative teams targeting intermediate and high-risk patients may be efficacious and cost-effective, although such perioperative services are challenging to establish. There is no guidance in the literature on how to practically implement perioperative teams to assist in the development of integrated postoperative care.
In 2015, a Perioperative Medicine (PoM) team was introduced at the Alfred Hospital, a tertiary referral hospital in Melbourne, Australia. In this paper we describe the PoM model of care at our institution, including the referral criteria and processes, and present the epidemiology and outcomes of patients referred to the service in its first two years. We also present baseline quality indicators of care to facilitate ongoing improvement and adaptation of our postoperative service.
We have previously published outcome data used in this paper as part of a study that investigated the statistical agreement between administrative data and clinical audit by anaesthetists in identifying major postoperative complications. 9 This study highlighted the limitations of using coding data and retrospective clinical audit by senior clinicians leading to potential under-reporting of complications data that we report here.
Methods
Perioperative Medicine team
In 2015 the Alfred Hospital introduced a postoperative review service, complementing a nine session per week consultant-led pre-anaesthetic assessment clinic and the existing orthopaedic geriatric perioperative team.
The PoM team comprises a consultant anaesthesiologist and/or Fellow, a senior general medicine trainee or ortho-geriatric trainee. Nursing staff from the ward on which the patient is located are engaged in the review and access to allied health services such as respiratory physiotherapy is available.
All patients are reviewed within 24 h postoperatively by an anaesthesiologist (consultant or Fellow) and a general medical registrar, with ongoing reviews by either team later that day or subsequent days if indicated. Anaesthesiologists review patients up to 48 h postoperatively, while the general medicine arm of the PoM team may continue assessments until discharge with the possibility of postoperative clinic follow-up if indicated. Discharge from the service would occur on clinical judgement by the medical registrar and when clinical examination, physiological observations and investigations indicated an uncomplicated recovery. All interventions are communicated to the surgical team verbally and written in the clinical notes. Out of hours (2000–0700), a hospital clinical lead is dedicated to non-ICU ward care (intensive care Fellow/senior registrar) and could be requested to review patients if required (Figure 1).
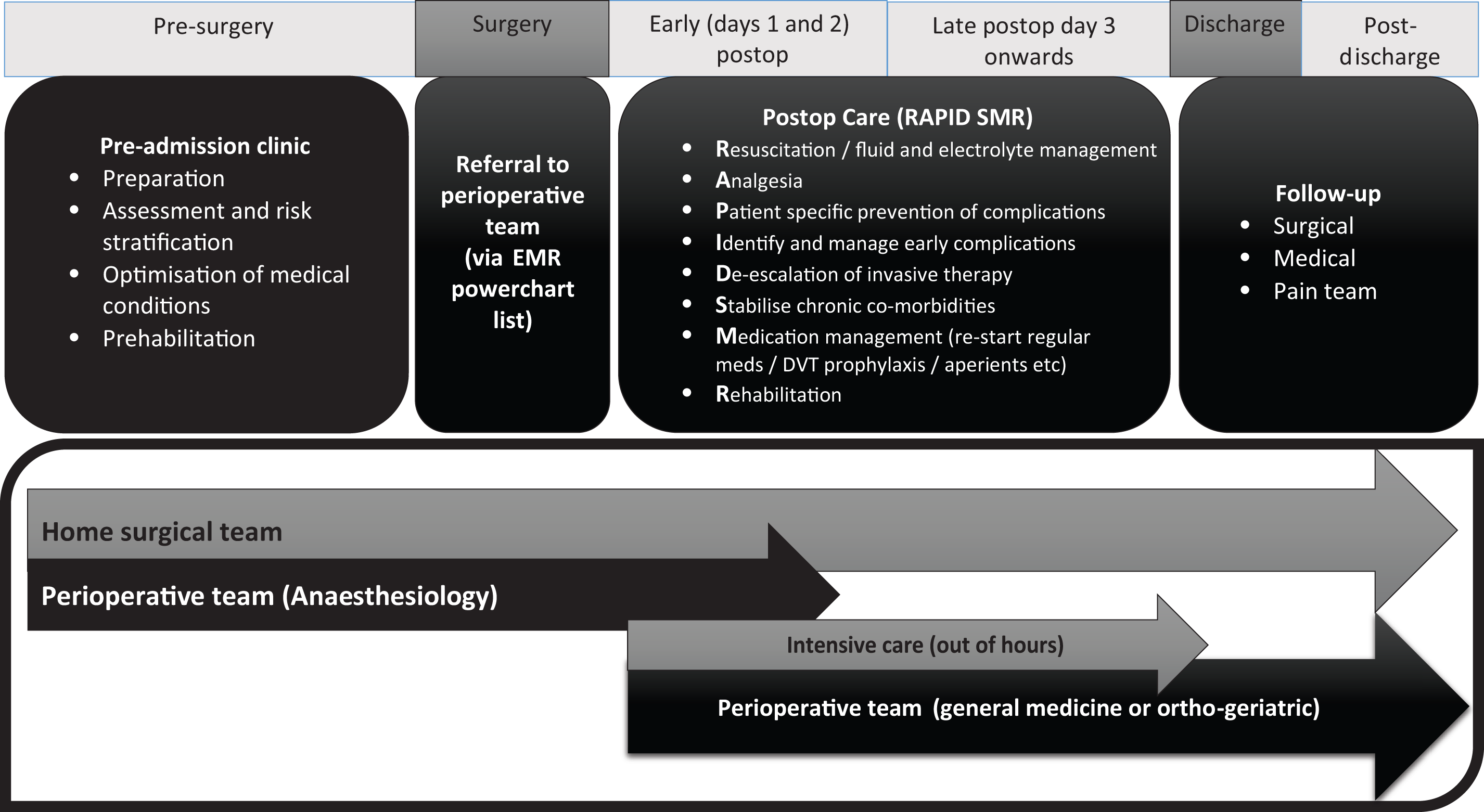
Schematic of roles and how the perioperative multidisciplinary team integrates throughout the perioperative journey.
Criteria for referral to the service (Table 1) are based upon identified risk factors for major complications and mortality from the REASON study, 4 which included a similar patient population. Patient details are added to an electronic patient list that can be accessed by all members of the PoM and ICU team.
Referral criteria.
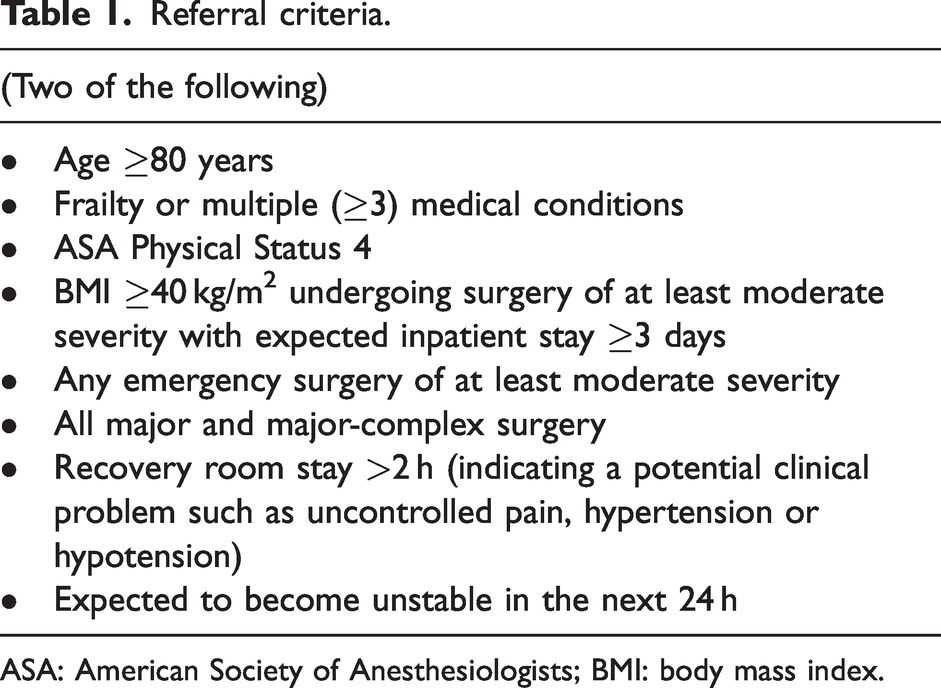
ASA: American Society of Anesthesiologists; BMI: body mass index.
The service is promoted to anaesthesiologists through education and posters displayed in the operating theatres.
Epidemiology and outcomes
We conducted a prospective observational study of all adult patients referred to the Alfred Hospital PoM team between September 2015 and August 2017. Postoperative data were prospectively recorded on a secure database for all patients reviewed by the perioperative service, including interventions undertaken, to allow for auditing and implementation of quality improvement processes where indicated. Medical record review for the study was conducted between September 2017 and February 2018. All patients were aged 16 years or older and had undergone elective or emergency non-cardiac non-obstetric surgery under general or regional anaesthesia and stayed at least one night in hospital. We excluded any patient admitted directly to critical care after surgery. Approval was granted by the Alfred Health Human Research Ethics Committee (approval 161/17), with a waiver of consent because the study was limited to a retrospective review of routinely collected data in the electronic medical record.
The primary aim was to characterise the epidemiology and outcomes of patients referred to the service in its first two years. The primary outcome was the incidence of selected complications defined by the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) and selected outcomes from the Core Outcomes Measurement in Perioperative and Anaesthesia Care Standardising Endpoints in Perioperative Medicine (COMPAC-StEP) group.10,11 Secondary aims were to measure clinical indicators of quality care and interventions by the anaesthetic arm of the perioperative service. Secondary outcomes included the incidence of Medical Emergency Team calls (triggered by standardised single abnormal clinical observations), indirect critical care admission, failure to rescue, hospital length of stay, days alive and at home within 90 days of surgery, and number of patients in which the perioperative team changed management and what these interventions were.
Demographic, comorbidity and procedural data were collected prospectively on all patients during routine clinical care. Exercise tolerance was assessed by the treating anaesthesiologist at the preoperative assessment using an estimate of metabolic equivalents (METs) into three groups, <4 METs, 4–7 METs, >7 METs. Patients were identified from the PoM team database. Medical record review was conducted by eight anaesthesiologists to determine baseline comorbidities, selected NSQIP major complications (red cell transfusion, myocardial infarction, stroke or transient ischaemic attack (TIA), cardiac arrest requiring cardiopulmonary resuscitation, pneumonia or aspiration pneumonitis, deep venous thrombosis, pulmonary embolism, major wound disruption, vascular graft failure, surgical site infections, sepsis, septic shock or systemic inflammatory response syndrome, acute renal failure) and death within 30 days of surgery. Selected COMPAC-StEP clinical outcomes were also recorded, including severe postoperative nausea and vomiting, ileus, constipation, hypothermia, delirium/confusion, arrhythmia, and heart failure. Data linkage was established with hospital administrative data and the hospital Medical Emergency Team call database. As the study was conducted prior to publication of consensus definitions for clinical endpoints in research in perioperative medicine, the most recent commonly applied research definition was used for each morbidity endpoint. 11 For morbidity endpoints without a commonly applied research definition, a clinically relevant study definition was created. Anaesthesiologists were provided with a data dictionary (see online Supplementary material) and undertook individual training prior to commencement.
Study data were collected and managed using REDCap electronic data capture tools hosted at the Alfred Hospital. 12 Each anaesthesiologist could access only the records assigned to them in the study database. Four anaesthesiologists were consultants, three were provisional Fellows and one was a registrar with prior research experience. To assess inter-rater reliability, the anaesthesiologists were grouped into four pairs and each anaesthesiologist assessed ten records of their counterpart such that each pair assessed 20 records in common. Inter-rater reliability was assessed for each morbidity endpoint for each pair. Anaesthesiologists (except JR) were blinded to the pairing allocations and to the knowledge that there was one consultant in each pair. All anaesthesiologists were blinded to which medical records were co-reviewed.
Statistics
Descriptive statistics were used to describe baseline characteristics and clinical outcomes in the study population. The denominator reported in tables and used to calculate percentages excluded missing data. Cohen’s kappa statistic was used to assess inter-rater reliability for each pair of investigators. Confidence intervals were computed by bootstrapping and a test of statistical significance was performed. Statistical analysis was performed using SPSS version 25.0.0.1 (IBM Corporation, Armonk, NY, USA, 2017).
Results
Study population
From 1 September 2015 to 31 August 2017, 46,454 surgical cases were performed at the Alfred Hospital. Of these, 18,582 (40%) were day procedures, with the remaining 27,872 (60%) of patients admitted to hospital for a minimum of one night. The number of inpatients (9.8%) admitted directly to critical care after surgery was 2733. Of the remaining, 25,139 (90.2%) were transferred to the ward; 506 (2%) were referred to the postoperative anaesthesia round. Data matching was incomplete for 24 patients, and these were excluded from the analysis, leaving a study population of 482 patients. The study population is shown in Figure 2.
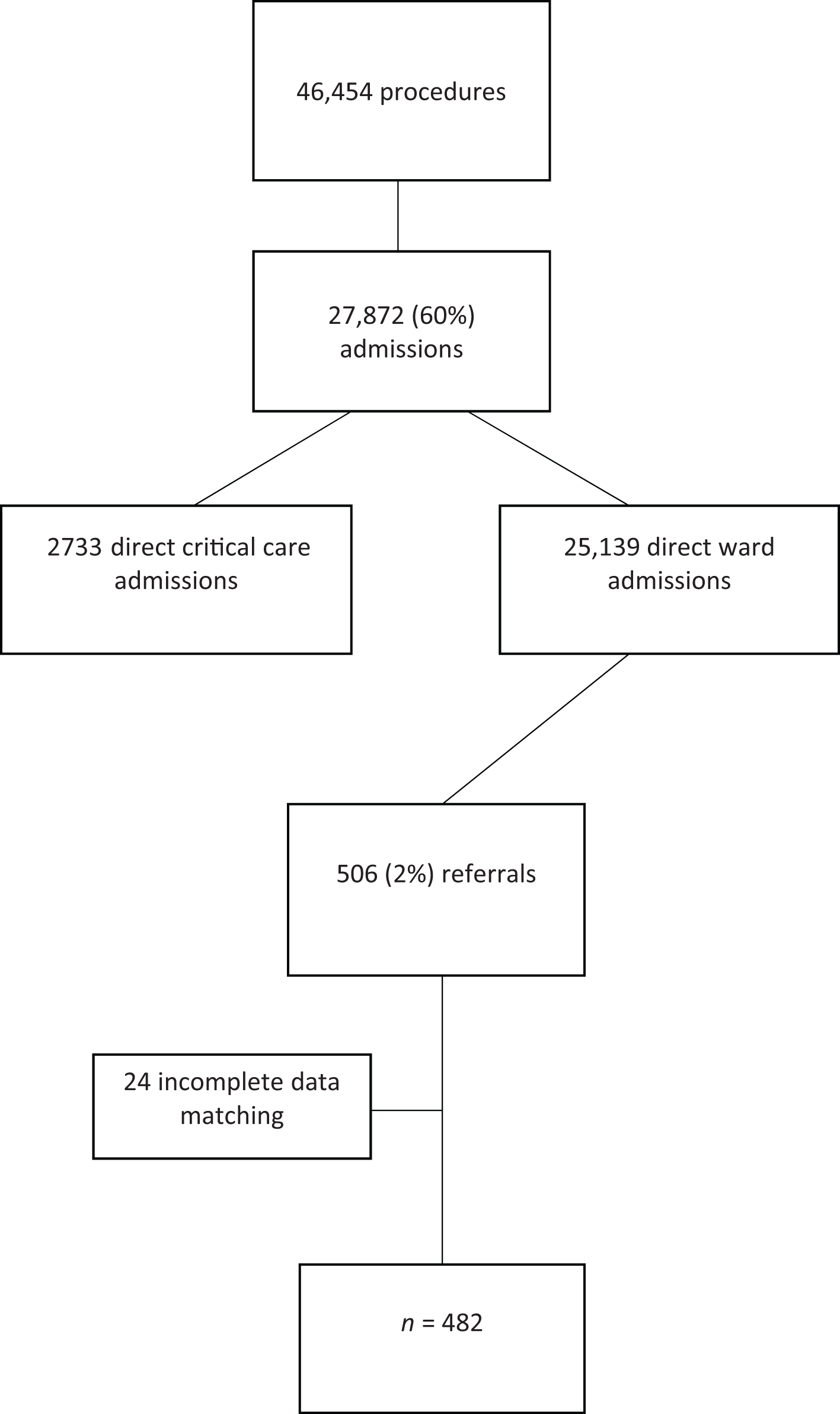
Study population.
Patient characteristics are shown in Table 2. The median age was 74 years, with 282/482 (59%) being male. Two hundred and twelve patients (44%) underwent emergency surgery, with the remaining 270 (56%) undergoing scheduled elective surgery. Most patients were of high American Society of Anesthesiologists (ASA) physical status, with 318 (66%) being ASA 3, 90 (19%) being ASA 4 and two (0.4%) being ASA 5. Of the 432 patients with complete data, functional status was poor (<4 METs) in 199 patients (46%), moderate (4–7 METs) in 207 patients (48%) and good (>7 METs) in 26 patients (6%). The most common surgical specialties represented were orthopaedic (n = 138, 29%), colorectal (n = 75, 16%), upper gastrointestinal (n = 72, 15%), vascular (n = 52, 11%) and neurosurgery (n = 38, 8%).
Patient characteristics.
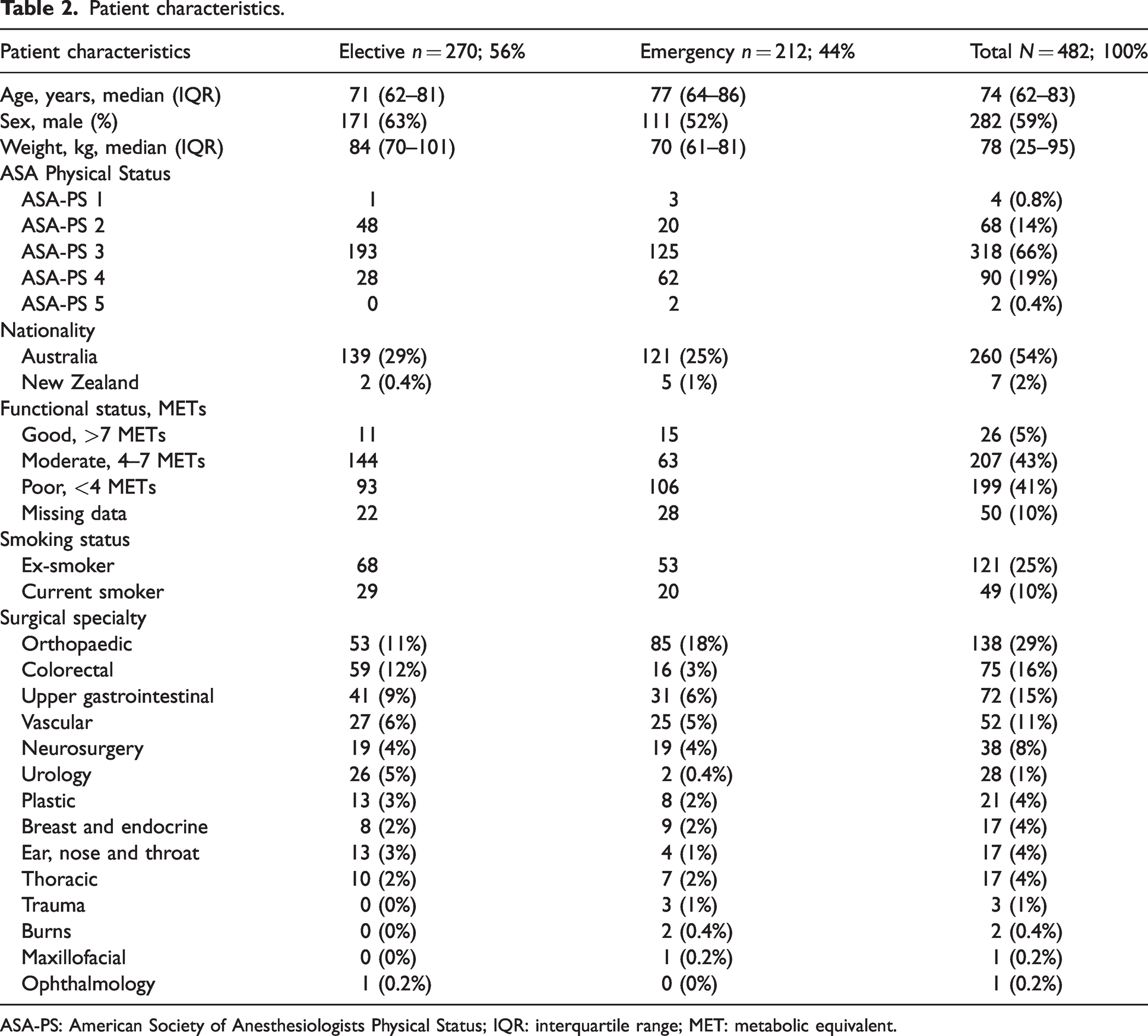
ASA-PS: American Society of Anesthesiologists Physical Status; IQR: interquartile range; MET: metabolic equivalent.
Baseline comorbidities are shown in Table 3. The median modified Charlson comorbidity index score 13 was 5, with 395 patients (82%) having a total score of at least 4. The most common comorbidities present were moderate to severe renal disease (n = 129, 27%), chronic obstructive pulmonary disease (n = 118, 25%) non-metastatic malignancy within the last five years (n = 103, 21%) and congestive cardiac failure (n = 94, 20%). Data for PoM team intervention were complete in 423 out of the 482 patients. Intervention occurred in 279/423 (66%) of patients. The types of intervention performed by the PoM team are outlined in Figure 1. Of the 279 patients who had an intervention, the type of intervention was missing in 64 patients.
Patient comorbidities using the modified Charlson comorbidity index.13
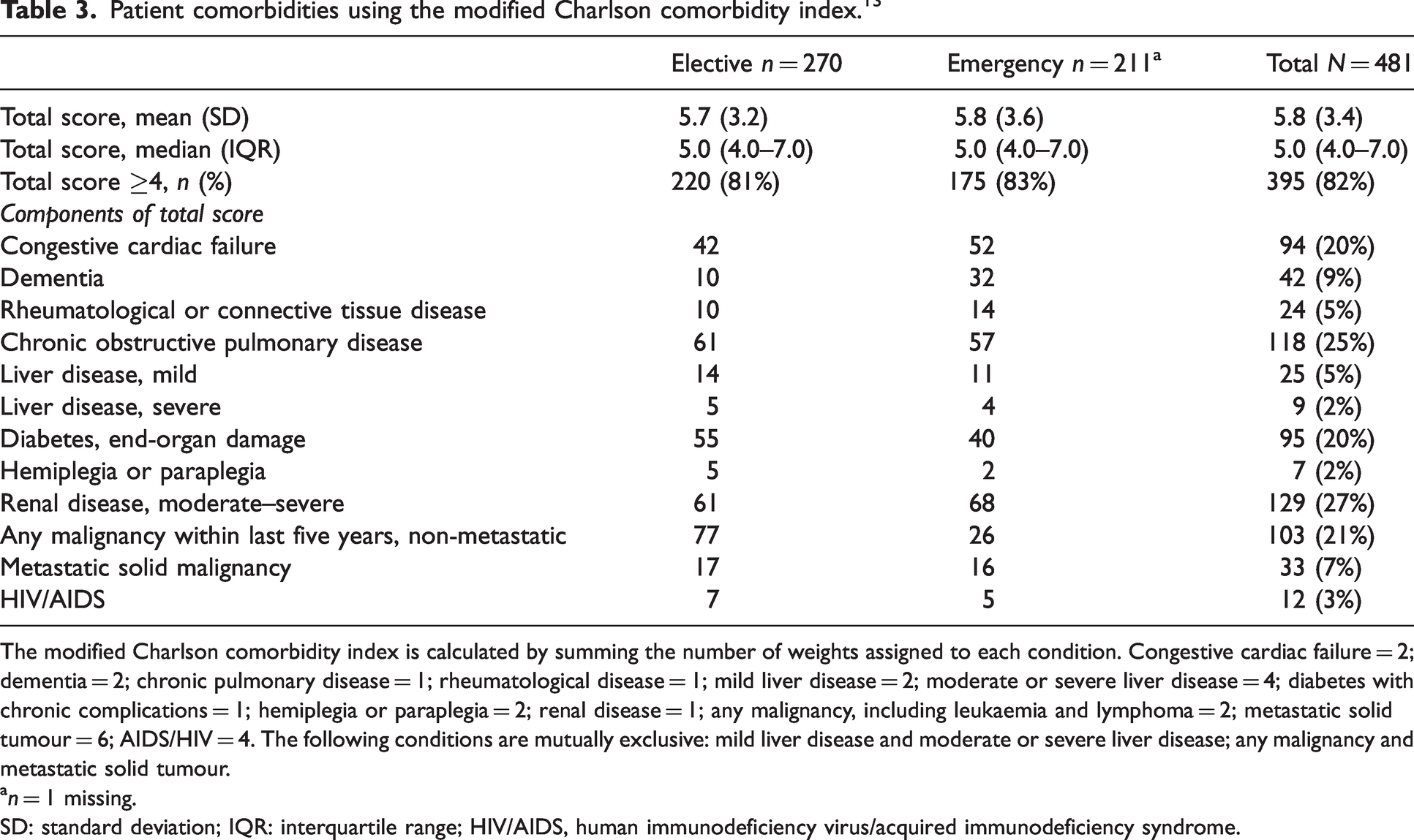
The modified Charlson comorbidity index is calculated by summing the number of weights assigned to each condition. Congestive cardiac failure = 2; dementia = 2; chronic pulmonary disease = 1; rheumatological disease = 1; mild liver disease = 2; moderate or severe liver disease = 4; diabetes with chronic complications = 1; hemiplegia or paraplegia = 2; renal disease = 1; any malignancy, including leukaemia and lymphoma = 2; metastatic solid tumour = 6; AIDS/HIV = 4. The following conditions are mutually exclusive: mild liver disease and moderate or severe liver disease; any malignancy and metastatic solid tumour.
an = 1 missing.
SD: standard deviation; IQR: interquartile range; HIV/AIDS, human immunodeficiency virus/acquired immunodeficiency syndrome.
Primary outcomes
The incidence of selected in-hospital major complications defined by NSQIP was 43.6% (210/482, Table 4). Subgroup analysis showed the incidence of in-hospital major complication defined by NSQIP was 34.4% (93/270) among elective surgery patients and 55.2% (117/212) among emergency surgery patients.
Clinical outcomes.
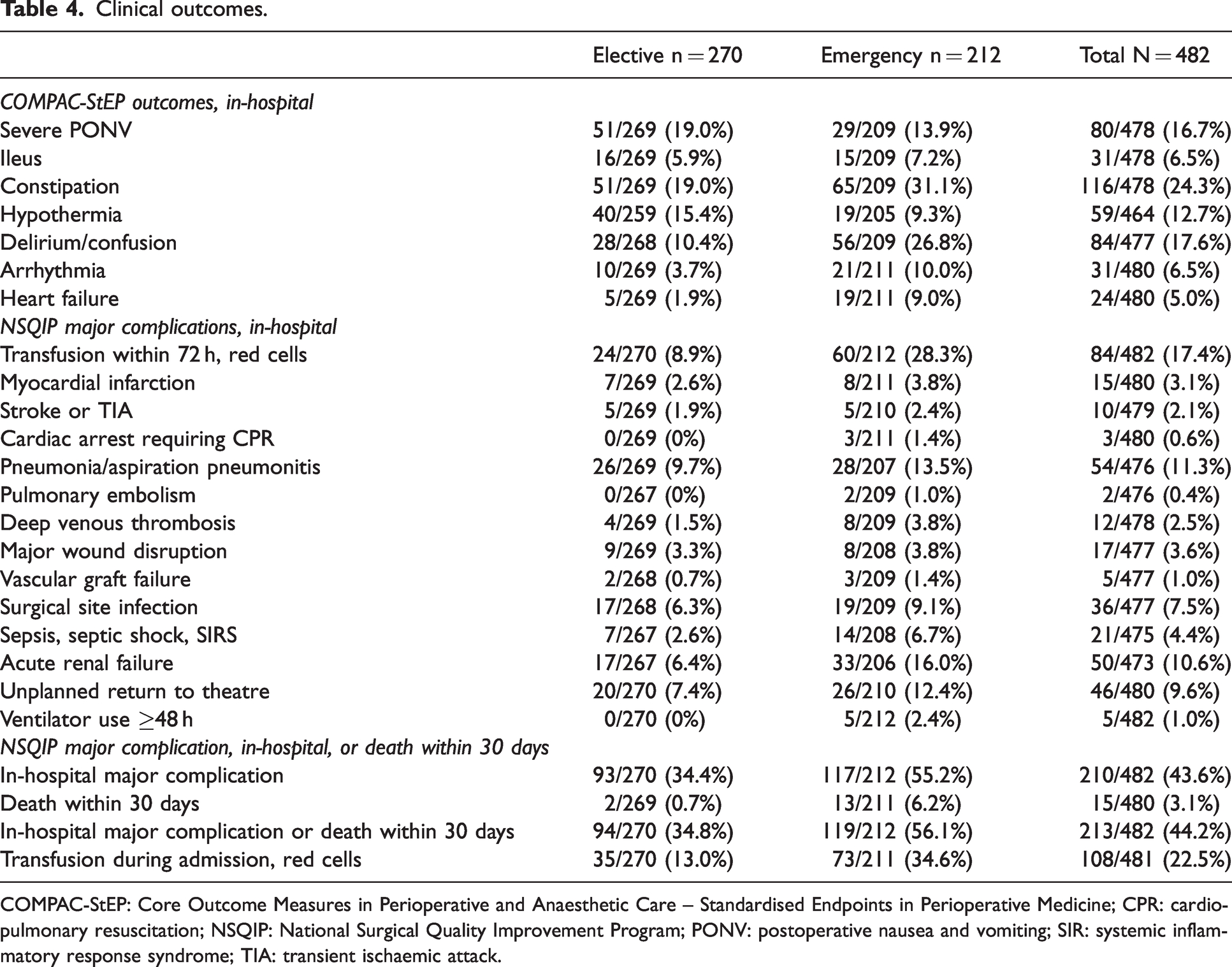
COMPAC-StEP: Core Outcome Measures in Perioperative and Anaesthetic Care – Standardised Endpoints in Perioperative Medicine; CPR: cardiopulmonary resuscitation; NSQIP: National Surgical Quality Improvement Program; PONV: postoperative nausea and vomiting; SIR: systemic inflammatory response syndrome; TIA: transient ischaemic attack.
The three most common major complications overall were transfusion of red cells within 72 h of surgery (84/482, 17.4%), pneumonia/aspiration pneumonitis (54/476, 11.3%) and acute renal failure (50/473, 10.6%). Subgroup analysis showed that among elective surgery patients the three most common major complications were pneumonia/aspiration pneumonitis (26/269, 9.7%), transfusion of red cells within 72 h of surgery (24/270, 8.9%) and unplanned return to theatre (20/270, 7.4%). Among emergency surgery patients the three most common major complications were transfusion of red cells within 72 h (60/212, 28.3%), acute renal failure (33/206, 16.0%) and pneumonia/aspiration pneumonitis (28/207, 13.5%).
Results for the COMPAC-StEP outcomes are shown in Table 4. The most common adverse outcome was constipation requiring medical treatment, present in 24.3% (116/478) of patients. The three most common outcomes were constipation, delirium/confusion (84/477, 17.6%) and severe postoperative nausea and vomiting (80/478, 16.7%).
The overall 30-day mortality was 3.1% (15/480) and was 0.7% (2/269) among elective surgery patients and 6.2% (13/211) among emergency surgery patients (Table 4). The incidence of the composite outcome major complication or death within 30 days was 44.2% (213/482). The composite outcome major complication or death within 30 days occurred in 34.8% (94/270) of elective surgery patients and 56.1% (119/212) of emergency surgery patients.
Inter-rater reliability
Inter-rater reliability for the diagnosis of morbidity and mortality endpoints was high within each pair of anaesthesiologists. Among COMPAC-StEP outcomes, there was very good agreement within each pair (kappa >0.81) for the diagnoses of ileus, delirium/confusion, arrhythmia, and heart failure. Agreement for constipation and hypothermia ranged from moderate to very good agreement.
Among NSQIP major complications, there was very good agreement within each pair (kappa >0.81) for the diagnosis of myocardial infarction, stroke/TIA, cardiac arrest requiring cardiopulmonary resuscitation, pulmonary embolism, deep venous thrombosis, major wound disruption, vascular graft failure, surgical site infection, sepsis/septic shock/systemic inflammatory response syndrome, and acute renal failure. Agreement was only slightly lower for diagnosing transfusion within 72 h of surgery and pneumonia or aspiration pneumonitis, with one pair demonstrating good agreement (kappa 0.61–0.80) and the other three pairs demonstrating very good agreement (kappa >0.81).
Agreement within each pair was very good (kappa 0.81–1.0) for death within 30 days of surgery.
Secondary outcomes
At least one postoperative Medical Emergency Team call was triggered in 20.7% (100/482) of patients, including 17% (46/270) of elective surgery patients and one-quarter of emergency surgery patients (54/212, 25.5%). The median (interquartile range (IQR)) time from discharge from the recovery unit to first Medical Emergency Team call was 99 (63–148) h among elective surgery patients and 178 (76–328) h among emergency patients (Table 5).
Medical Emergency Team calls.

IQR: interquartile range; MET: Medical Emergency Team.
Clinical indicators are summarised in Table 6. Indirect critical care admission (transfer to critical care from the ward) occurred in 3.3% (16/482) of patients, and there was no difference in incidence between elective and emergency surgery patients. The failure to rescue rate at 30 days was 7.1% (15/210), being 2.2% (2/93) among elective surgery patients and 11.1% (13/117) among emergency surgery patients. Median (IQR) length of hospital stay was 8.0 days (5.0–16.0), being 6.0 days (4.0–10.25) among elective surgery patients and 11.0 (7.0–20.75) among emergency surgery patients. Median (IQR) days alive and at home within 90 days of surgery was 78 days (59–84), being 82 days (72–85) among the elective surgery cohort and 68 days (14–82) among the emergency surgery cohort.
Clinical indicators.
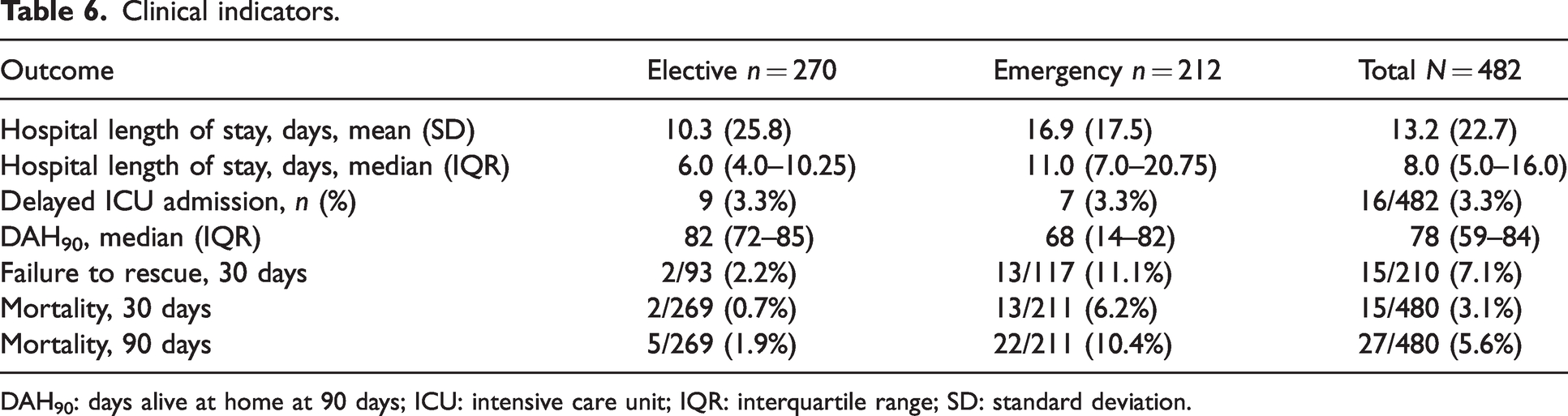
DAH90: days alive at home at 90 days; ICU: intensive care unit; IQR: interquartile range; SD: standard deviation.
Discussion
Perioperative medicine is an expanding field in response to the increasing complexity of patients undergoing surgery, excess variation in care and recognition of the impact postoperative complications have on quality and length of life after surgery. 14 Models of postoperative care vary depending on the healthcare system and institution. Critical care beds are a limited and costly resource, and critical care admission has not been demonstrated to improve survival after surgery. 15 Intermediate and high-risk surgical patients not requiring postoperative organ support may be suitable for ward care but remain vulnerable to complications. Standard postoperative ward care is characterised by intermittent monitoring and is often led by junior surgical staff. Multidisciplinary ‘co-management’ of postoperative patients has the potential to improve outcomes by combining complementary skill sets of surgeons, anaesthesiologists and physicians. 16 As the Australian and New Zealand College of Anaesthetists are preparing a curriculum to provide a dedicated perioperative medicine qualification, 8 it will be important for institutions to provide to clinicians experience of working within multidisciplinary perioperative teams, managing the high-risk perioperative patients.
We describe implementation of a multidisciplinary perioperative care service targeting a broad range of high-risk surgical patients in a tertiary university public hospital in Melbourne, and the incidence of major complications and mortality after surgery. The model was established, utilising existing staffing structure, to allow for the best skills of each specialty to be involved at a timely phase in a patient’s perioperative journey. Our findings suggest that those patients referred to the PoM team were generally a high-risk group, based on patient risk factors (>85% ASA 3, 4 or 5; 46% <4 METs; median age 74 years; median Charlson comorbidity score of 5). Major complications occurred in 55.2% and 35.4% of emergency and elective surgery patients respectively (43.6% overall) and corresponding 30-day mortality was 6.2% and 0.7% (3.1% overall). The overall rate of major complications was high (43.6%), with most (39.3%) due to blood transfusion (17.4%), respiratory complications (11.3%) and acute renal failure (10.6%). Despite this, only 3.3% of patients required admission to critical care from the ward, which may reflect the ability to manage these complications in a ward environment or indicate the limitation of bed availability in critical care.
A key role of perioperative teams is to identify areas for improving perioperative care within the specific institution. By highlighting the common major complications to address, such as acute kidney injury and pulmonary complications, specific care pathways have subsequently been created and initiated in the preoperative clinic. These data also allow us to address important complications that impact length of stay in our institution, namely constipation, postoperative nausea and vomiting and delirium. The median time course of deterioration using Medical Emergency Team call as a surrogate marker was on day six postoperatively, and perhaps suggests a need for the perioperative team to follow all of these selected patients until discharge.
Because our results are not specifically adjusted for case mix, caution is required when benchmarking against the international literature. Further, direct comparisons cannot be made due to heterogeneity in published study populations and outcome measures. Our cohort was not dissimilar to the REASON study (n = 4158, Australia, 2004 to 2008; median age 78 years, 65% ASA 3–4, 34% emergency surgery); however, our study excluded patients admitted directly to critical care after surgery, while 9.4% of the REASON cohort were directly admitted to critical care. 4 The incidence of 30-day major complications in REASON was less than half the incidence that our study population experienced in hospital (20% versus 43.6%), yet the 30-day mortality was higher (5.2% versus 3.1%). 4 In Europe, the EUSOS study population (n = 46,539, 28 European countries, 2011) had lower baseline risk than our cohort, with a median age of 57 years and 28% ASA 3–5, but 8% were directly admitted to critical care. 15 EUSOS reported inpatient mortality (rather than 30-day mortality) of 4%, which compares to our 30-day mortality of 3.1%. The rate of major complications in our elective group is similar to the complication rate of higher risk patients (ASA 3) in the ISOS study (34.4% versus 30.3%). 3 However, as the ISOS did not include blood transfusion as a complication these rates are not directly comparable.
A previous single-centre observation study has reported reduced length of stay and hospital costs after implementation of a perioperative consult service for patients undergoing colorectal surgery, although this was in conjunction with implementation of an enhanced recovery programme and included only elective cases. 17 Postoperative anaesthesia co-management of patients undergoing major urologic surgery has also reduced length of stay, cost and complications in a single centre retrospective pre–post implementation study. 18 In contrast, a retrospective study of a non-anaesthetist led postoperative round (led by intensive care and general medicine registrars) suggested an increase in length of stay among high-risk patients undergoing urologic and general surgery after implementation of the postoperative round; there was no difference in secondary endpoints, including Medical Emergency Team call and mortality. 19
The strength of our study is that it relates to a real-world practical way to implement an integrated multidisciplinary perioperative team and record routinely collected clinical and administrative data that similar institutions can benchmark against.
Limitations include conduct at a single institution and the observational study design without a comparator group: therefore, no conclusions can be drawn as to whether the perioperative team impacts on patients’ outcomes. Although we have demonstrated that a high-risk surgical population was referred to the PoM team, we do not know whether there were other patients who were not referred who should have been.
The routine measurement of perioperative risk factors and outcomes in this population would be an ideal extension of our perioperative service, especially in those undergoing emergency surgery given the 30-day outcomes observed in this study. A detailed cost analysis study is also important as we demonstrate a potential for more surgical patients to be safely managed outside of critical care, because as yet we do not know whether this provides significant economic benefit. 20
As hospitals move forward with integrating information technology on wards, such as continuous non-invasive monitoring and use of electronic medical records, there is the potential to expand the number of patients included in postoperative services, but further outcomes data are needed to justify this. 21 Future studies of perioperative team involvement in high-risk patients could then investigate whether they can reduce rates of failure to rescue and mortality, as well as patient-centred outcomes such as disability-free survival. 22 Establishing a coordinated multidisciplinary perioperative team with routine outcomes measurement and reporting is a logical step towards facilitating assessment and integration of future perioperative evidence-based interventions.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221119814 - Supplemental material for Perioperative outcomes in intermediate and high-risk patients after major surgery following introduction of a dedicated perioperative medicine team: A single centre cohort study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221119814 for Perioperative outcomes in intermediate and high-risk patients after major surgery following introduction of a dedicated perioperative medicine team: A single centre cohort study by Jonathan J Nicholson, Jennifer Reilly, Mark A Shulman, Marissa Ferguson, Justin A Burke, Daragh N Lehane, Chen-Mei Liaw, Adam Mahoney, Peter Stark, Paul S Myles in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.