
Abstract
Perioperative anaphylaxis is a potentially life-threatening emergency that requires prompt recognition and institution of life-saving therapy. The Australian and New Zealand College of Anaesthetists and Australian and New Zealand Anaesthetic Allergy Group have partnered to develop the anaphylaxis management guideline along with crisis management cards that are recommended for use in suspected anaphylaxis in the perioperative setting. This is the third version of these guidelines with the second version having been published in 2016. This article contains the revised Australian and New Zealand Anaesthetic Allergy Group/Australian and New Zealand College of Anaesthetists perioperative anaphylaxis management guideline, with a brief review of the current evidence for the management of anaphylaxis in the perioperative environment.
Keywords
Introduction
Perioperative anaphylaxis remains the most common cause of death directly attributable to anaesthesia in Australia and New Zealand. The Australian and New Zealand College of Anaesthetists (ANZCA) safety of anaesthesia report for the 2015–2017 triennium 1 identified eight deaths in which anaphylaxis directly related to anaesthesia or other factors under the control of the anaesthetist could with reasonable certainty be established as the cause. The report also highlighted the need for training in crisis management to maximise the benefit of resuscitation when anaphylaxis is suspected and that simulation-based training is recommended for such very low frequency events. Anaphylaxis is one of the options included in ANZCA’s continuing professional development mandatory emergency response activities. 2 The pathophysiology of anaphylaxis can escalate quickly, and therefore the management of anaphylaxis should place emphasis on early recognition and treatment in order to avoid serious morbidity and mortality.
Scope
These recommendations are intended for use only in the perioperative setting. They reflect the special circumstances of perioperative anaphylaxis in which there is continuous dedicated monitoring by an anaesthetist and a higher frequency of sudden onset severe symptoms compared with non-perioperative anaphylaxis. For anaphylaxis in the non-anaesthesia setting the Australasian Society of Clinical Immunology and Allergy (ASCIA) guidelines 3 apply.
One of the features of the Australian and New Zealand Anaesthetic Allergy Group (ANZAAG) and ANZCA perioperative anaphylaxis management guideline is in its presentation rendering it applicable to crisis management in the perioperative setting. This paper presents the updated ANZCA and ANZAAG co-badged perioperative anaphylaxis management guideline, 4 which was released in May 2022. It provides the rationale for the update, outlines guideline development, and highlights key changes.
Guideline development
The second version of the ANZCA/ANZAAG perioperative anaphylaxis management guideline
5
was released in 2016. The most recent 2022 review was performed as part of a routine 5 yearly review of the ANZCA guideline. It is timely as there have been a number of significant publications in the years since the 2016 guideline was published, including:
NAP6 (6th National Audit Project: Perioperative Anaphylaxis) reported the findings of a year-long UK-wide audit of perioperative anaphylaxis focusing on grade 3, 4 and 5 reactions, published in May 2018.
6
British Journal of Anaesthesia special perioperative anaphylaxis issue, 2019, included international consensus guidelines and reviews.
7
Updated resuscitation guidelines: Resuscitation Council of the UK,
8
European Resuscitation Council,
9
American Heart Association,
10
Association of Anaesthetists of Great Britain and Ireland (AAGBI),
11
Brazilian Society of Anaesthesiology and Brazilian Association of Allergy and Immunology,12,13 Japanese Society of Anesthesiologists,
14
Australian and New Zealand Committee on Resuscitation (ANZCOR)
15
and ASCIA.
3
The key changes to the revised guideline are:
Cardiac compressions should be initiated at a systolic blood pressure of less than 50 mmHg in the anaesthetised patient. A graded approach to volume replacement: ○ An initial crystalloid fluid bolus of 500 mL in a moderate (grade 2), and 1000 mL in a life threatening (grade 3) reaction, repeated as required and titrated to clinical response. ○ In a cardiac arrest (grade 4) reaction the recommendation remains for an initial bolus of 2000 mL. Graded intravenous (IV) adrenaline (epinephrine) bolus doses, with lower starting doses for each grade of reaction and suggested dose escalation depending on response. Pregnancy: Manual left uterine displacement, rather than left lateral tilt, should be applied during the management of hypotension or cardiac arrest due to anaphylaxis in the pregnant patient to minimise aortocaval compression. Oesophageal intubation has been added to the differential diagnosis list for refractory bronchospasm and has been included on the immediate management cards for adults and paediatrics.
16
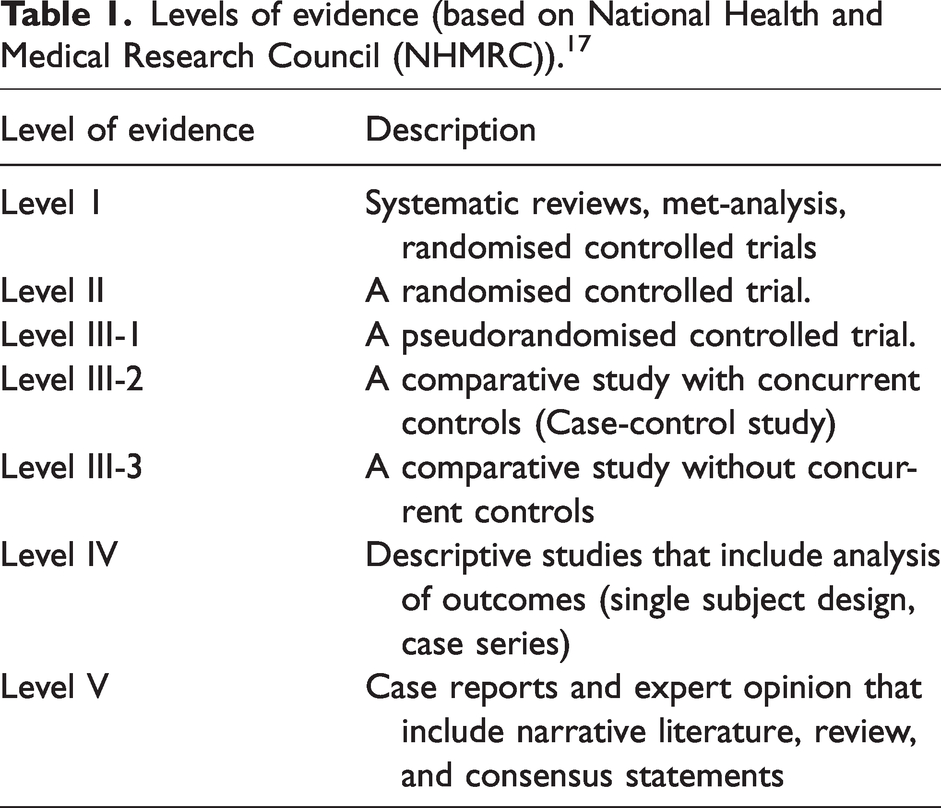
Due to the paucity of randomised controlled trials of sufficient quality on the management of anaphylaxis the recommendations in this guideline are consensus statements developed by ANZAAG and ANZCA after an extensive literature review. In common with other guidelines, most of the recommendations are grade D and are based on level IV or level V evidence. When stronger evidence is available it has been noted alongside the recommendation (Tables 1 and 2).
Levels of evidence (based on National Health and Medical Research Council (NHMRC)). 17
NHMRC grades of recommendation. 17
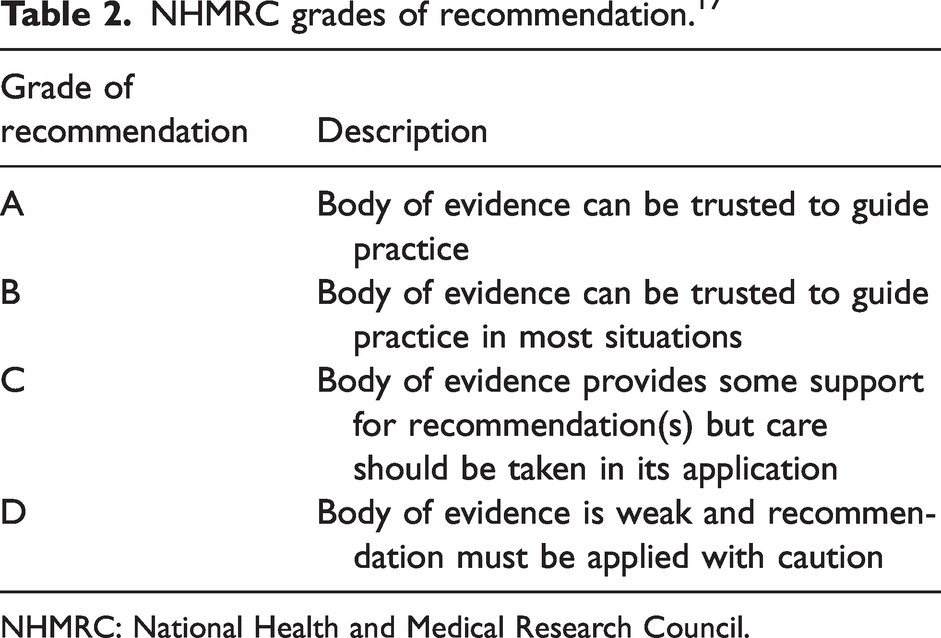
NHMRC: National Health and Medical Research Council.
Use of the ANZAAG/ANZCA anaphylaxis management cards
The cards have been designed for use in real time during a perioperative anaphylaxis event, with one team member assigned to read the cards and ensuring all items have been checked off.
As with any clinical emergency it is recommended that all members of the anaesthesia team are familiar with the cards and their likely roles.
Team structure
It is important to send for help early during a suspected perioperative anaphylaxis, due to the potential for multiple simultaneous tasks. A consultant anaesthetist should be present or notified.
The anaesthesia team for anaphylaxis management has at least three team members with specific roles:
Team leader; Card reader—this role requires no specific anaesthesia expertise and requires the cards to be read out verbatim to ensure no omissions; Adrenaline preparation and administration.
Additional roles if resources allow:
Fluid management and preparation; cannulation—IV and intra-arterial access; scribe; cardiopulmonary resuscitation (CPR) rotators (in the case of cardiac arrest).
Diagnosis of anaphylaxis
As anaphylaxis is a clinical diagnosis and symptoms mimic other perioperative events, diagnosis can be challenging. A high index of suspicion by anaesthetists is therefore essential for early diagnosis and treatment. In conscious or minimally sedated patients, anaphylaxis may also have additional respiratory, gastrointestinal, or central nervous system symptoms and signs in addition to itching or flushing. These include rhinorrhoea, cough, dyspnoea, circumoral tingling, difficulty swallowing, nausea, abdominal pain, irritability, confusion, or a sense of impending doom.
18
The diagnosis of anaphylaxis should be considered when hypotension is unexplained and out of proportion to that which could be expected on the basis of patient factors (age, co-morbidities) and the stage of the operation and/or when there has been a lack of sustained response to usual restorative measures. While tachycardia is common it can be masked by concomitant β-blocker use, and bradycardia may be observed in some patients.
19
The diagnosis of anaphylaxis should be suspected when bronchospasm and difficulty with ventilation are resistant to commonly employed treatment manoeuvres. The differential diagnosis card aids the consideration of alternative causes of clinical signs by classifying the common ones with a view to expedite management (e.g. needle decompression to treat tension pneumothorax). Oesophageal intubation has been added as a differential diagnosis for refractory bronchospasm. During cardiac arrest and CPR, the end-tidal carbon dioxide (CO2) trace is attenuated but present. In oesophageal intubation the end-tidal CO2 trace is a flat line.
16
Severity of anaphylaxis
The severity of anaphylaxis will guide the recommended doses of IV fluid and adrenaline, therefore it is suggested that the anaesthetist characterises the grade of reaction.
The four severity classes are described in detail on the differential diagnosis card (Figure 1) and can be referred to during an anaphylaxis event.
Differential diagnosis card and grading of anaphylaxis.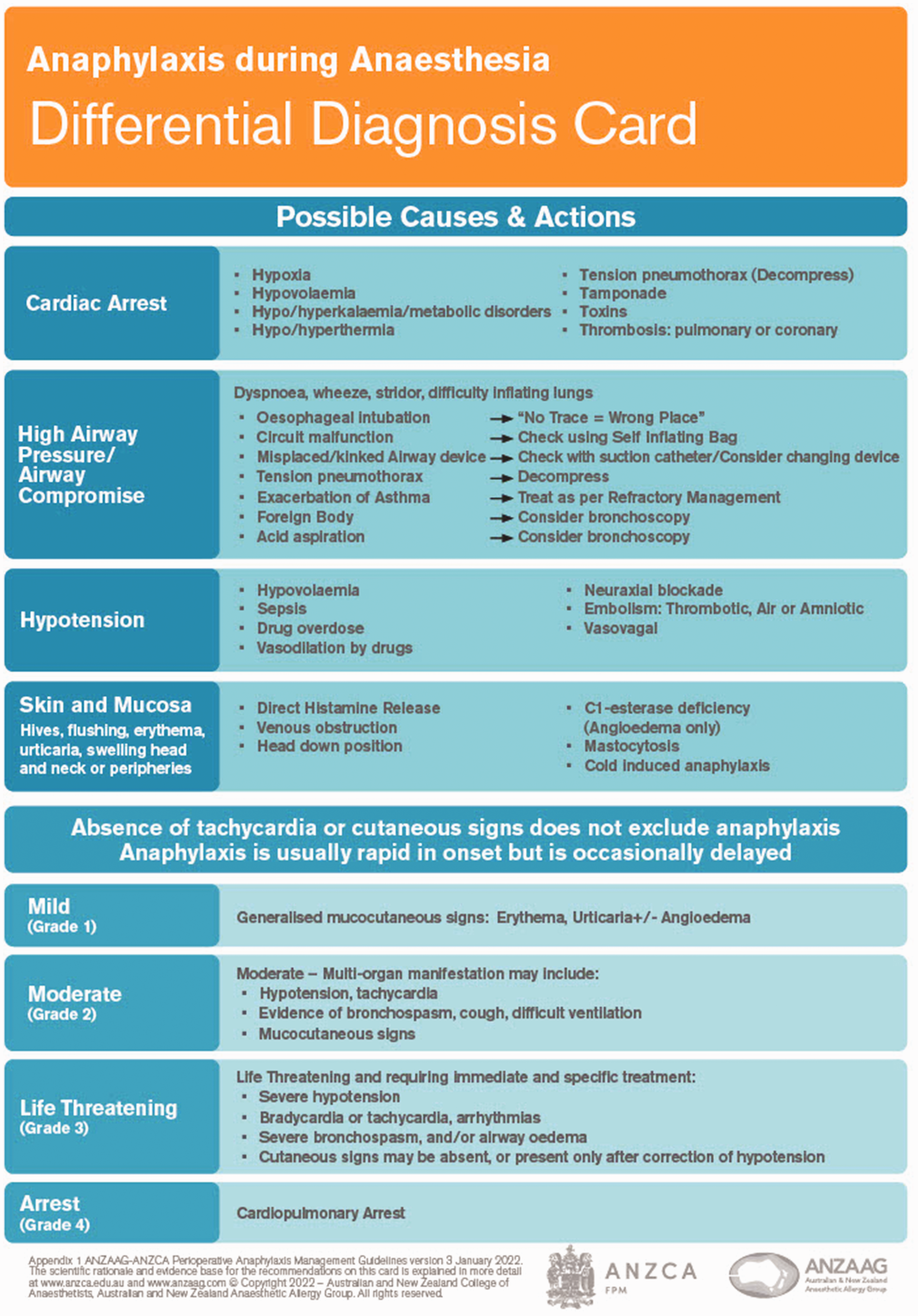
The immediate management card outlines treatment options based on the grade of anaphylaxis, when these grading descriptors are utilised: mild (grade 1); moderate (grade 2); life-threatening (grade 3); and cardiac arrest (grade 4).
Immediate management
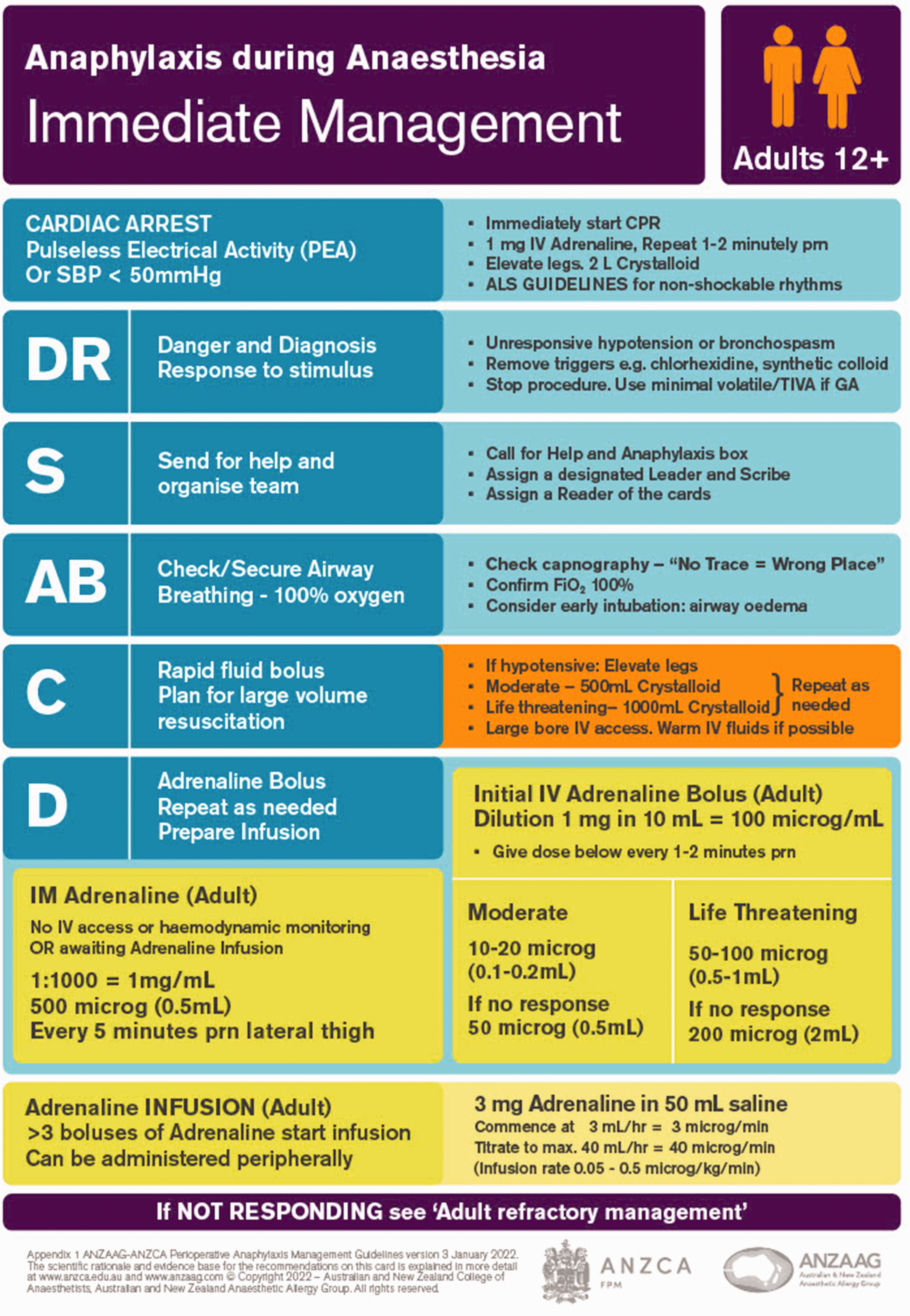
The immediate management of anaphylaxis cards include adult (Figure 2) and for children under 12 years old, paediatric (Figure 3) cards.
Immediate management adult card
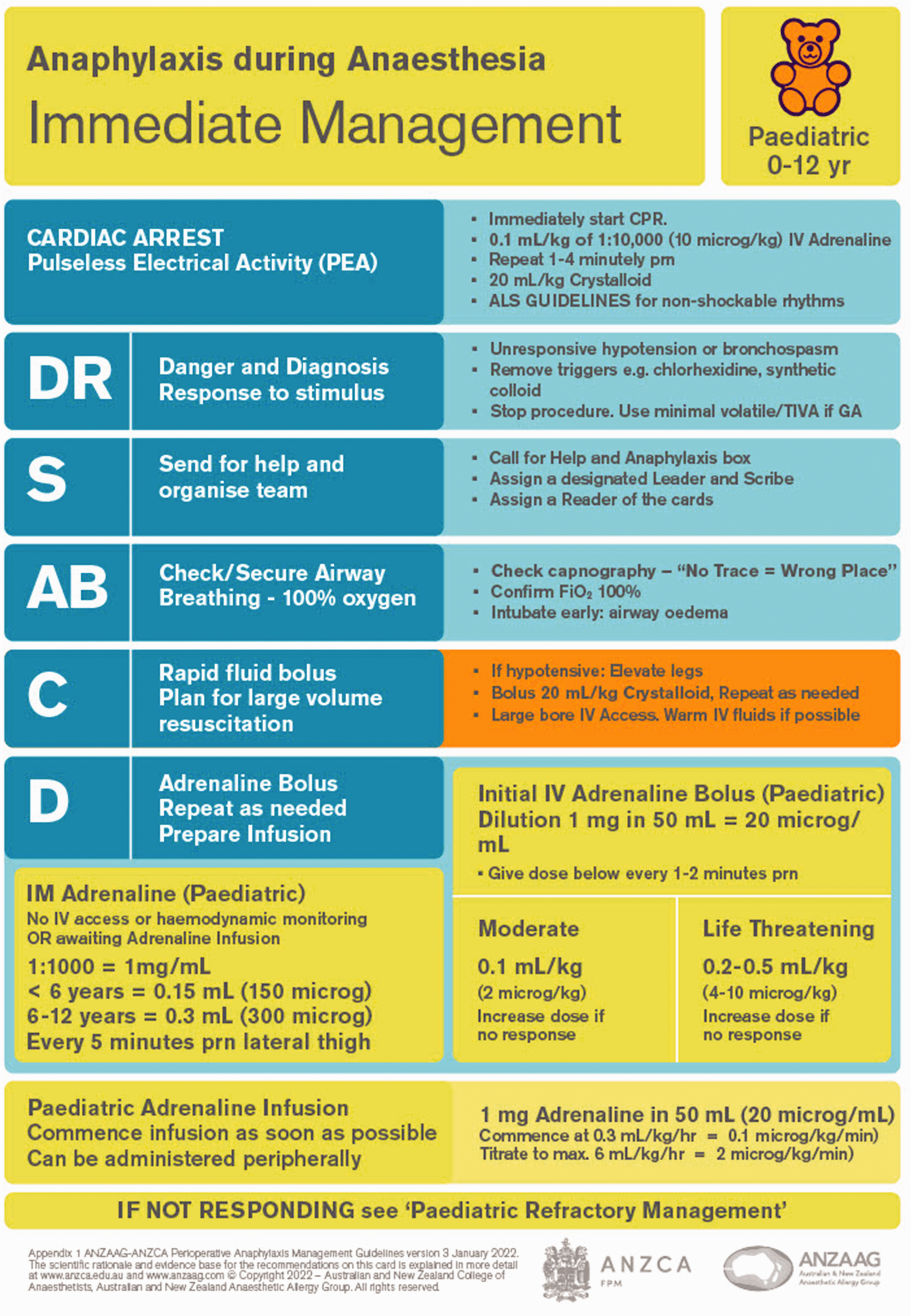
Immediate management paediatric card.
The card for immediate management has been designed as a cognitive aid for use during a crisis.
The main points of managing the crisis are listed on the left-hand side of the card, whereas the right-hand side gives more detailed instructions. Actions are listed in order of priority, with the most important at the top.
Adrenaline (epinephrine) is the first line treatment for anaphylaxis,10,20 –23 and is pivotal in the management of anaphylaxis. Adrenaline not only treats the clinical manifestations but also reduces response amplification,20,21 and cannot be substituted by any other medication. 24
Judicious use is advised in patients with higher risks of overdose: including extremes of age, patients with hypertension, ischaemic heart disease, hypertrophic cardiomyopathy (HOCM) or hyperthyroidism.
The benefits of intramuscular (IM) adrenaline20,21,24,25 for the management of anaphylaxis far exceed the risks (level 1 evidence).
Due to ease of preparation and administration of IM adrenaline into the lateral thigh, it should be considered in the initial management of many circumstances of perioperative anaphylaxis (grade B recommendation), including when there is a suspicion of evolving moderate (grade 2) anaphylaxis, or in an awake patient.
The mainstay of the management of moderate to severe perioperative anaphylaxis is carefully titrated IV adrenaline with close monitoring of cardiovascular responses. 7
The dose of IV adrenaline should be based on the severity of clinical presentation. 7
Grade 1 (mild): no adrenaline required.
Grade 2 (moderate): 10–20 µg IV adrenaline. Escalate to 50 µg if insufficient response to initial dose. Consider initial IM adrenaline as a safe and effective alternative.
Grade 3 (life threatening): 50–100 µg IV adrenaline. Escalate to 200 µg if insufficient response to initial dose.
Grade 4 (cardiorespiratory arrest) 1000 µg IV adrenaline immediately, repeated every 1–2 min.
9. Adrenaline infusions without bolus administration 26 (level III evidence) can be effective in the management of severe refractory anaphylaxis.
10. In a profoundly hypotensive patient, cardiac compressions should be initiated at a systolic blood pressure of less than 50 mmHg in the anaesthetised patient. 6
11. The excessive use of adrenaline in association with inadequate volume replacement can result in a hyperdynamic underfilled heart and dynamic left ventricular outflow obstruction even in an anatomically normal heart. 27
The new recommendation is for an initial fluid bolus of:
a) 500 mL in grade 2 (moderate) and 1000 mL in grade 3 (life-threatening) reactions, to be repeated as required, and titrated to clinical response;
b) grade 4 reactions (cardiac arrest) initial bolus of 2000 mL.
13. Crystalloids are recommended for fluid resuscitation in anaphylaxis.3,9,11,15
14. Cease administration of potential triggers such as colloids and medications (chlorhexidine, dyes) particularly in cases of refractory anaphylaxis. 24
15. In the pregnant patient, manual left uterine displacement should be performed as part of the management of anaphylaxis, in the presence of hypotension or cardiac arrest. 28
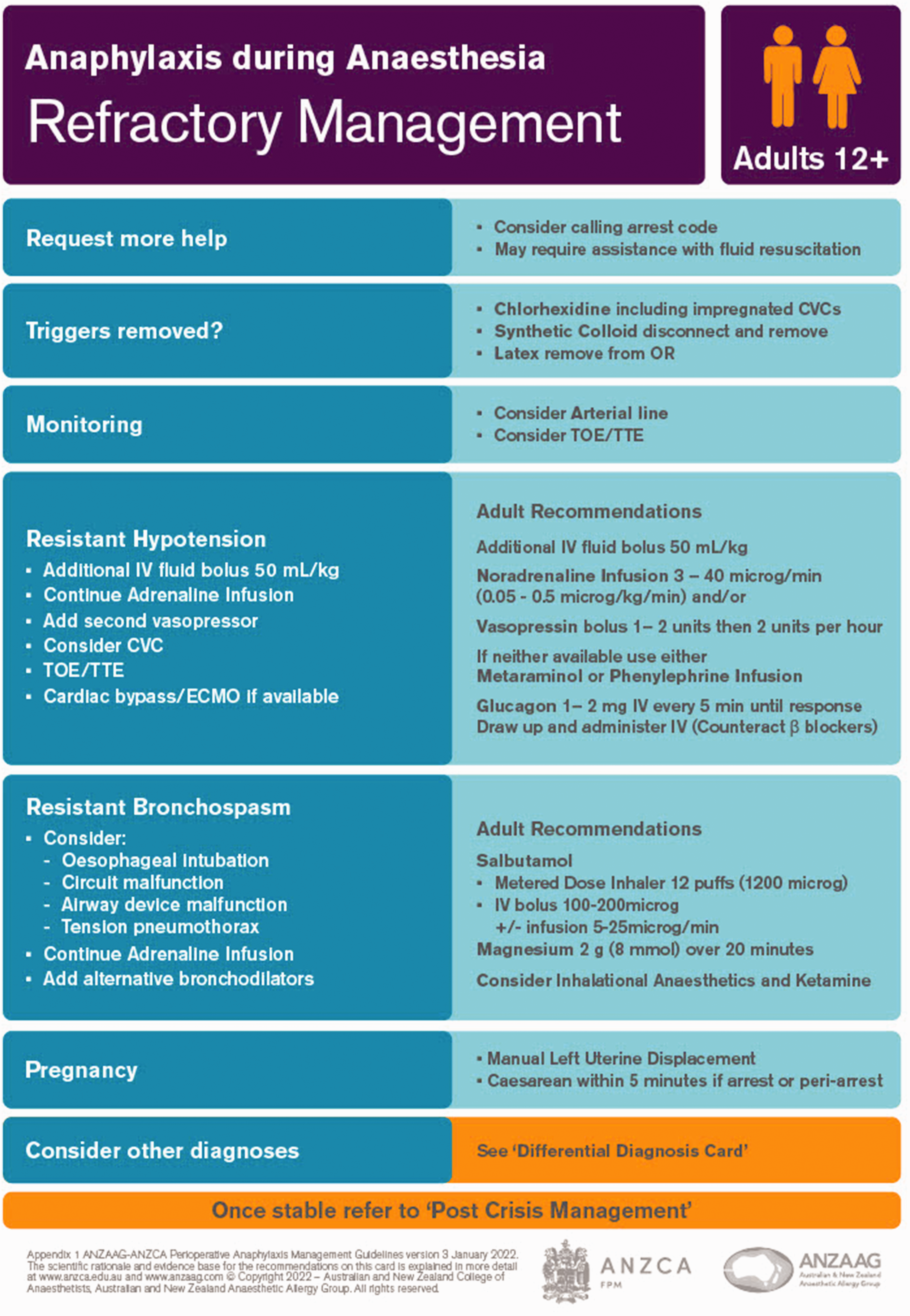
Refractory management
Adult (Figure 4) and paediatric (Figure 5) cards:
Adult refractory management card.
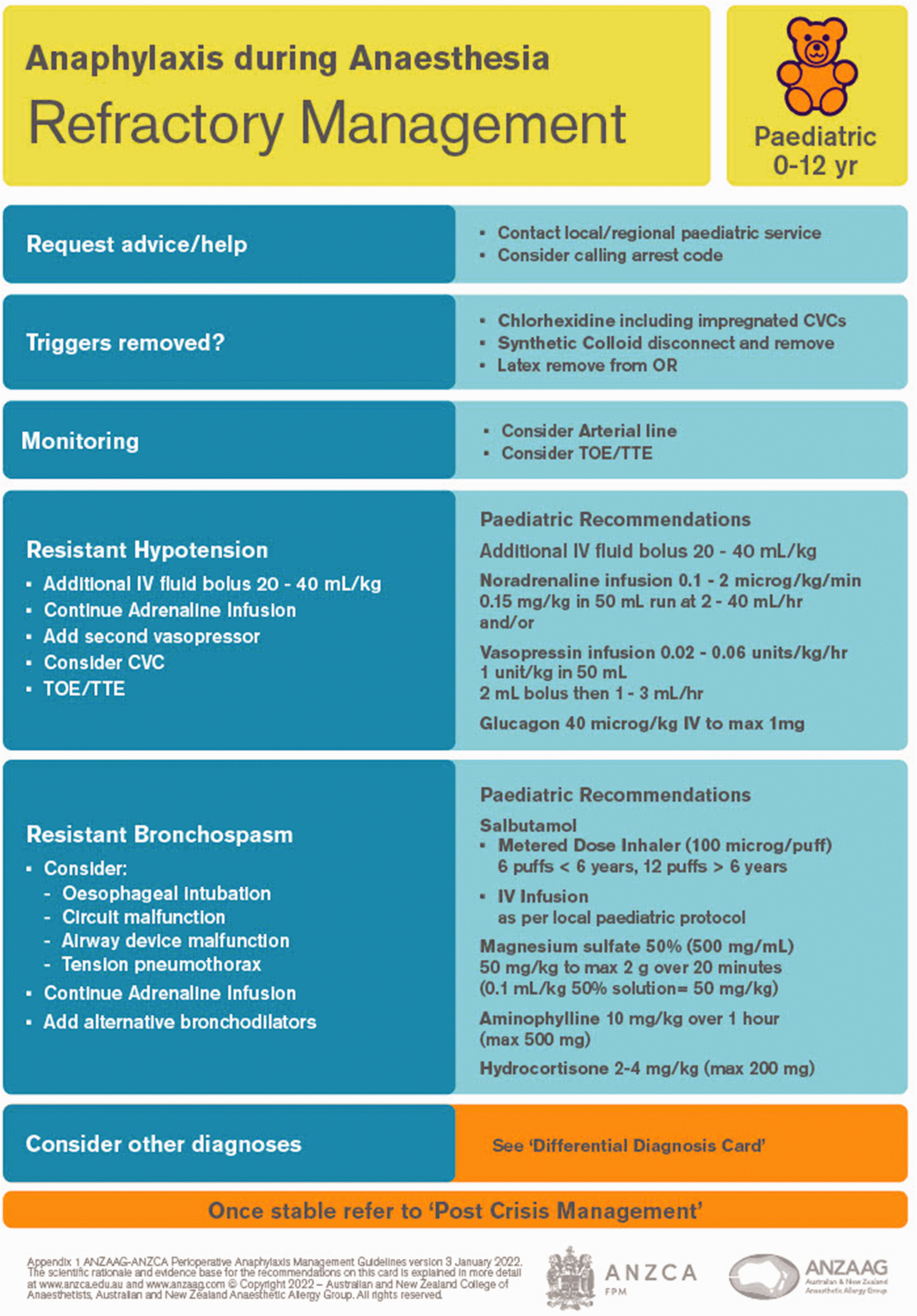
Paediatric refractory management card.
For a patient who fails to respond to appropriate therapy for presumed anaphylaxis, echocardiography may be helpful in confirming the diagnosis of anaphylaxis or suggesting another diagnosis, such as decompensated HOCM or Takotsubo cardiomyopathy.
When extracorporeal membrane oxygenation is available, it should be considered in the management of perioperative anaphylaxis refractory to maximal standard treatment.
In the presence of adequate cardiac contractility as shown on echocardiography, vasopressors may be added, when adrenaline infusions and fluid boluses have been inadequate in achieving targeted blood pressure.
Noradrenaline, vasopressin and metaraminol are included for the management of refractory anaphylaxis. Metaraminol and phenylephrine are included to accommodate those environments where alternatives to adrenaline are limited. 29
Adrenaline remains the first line treatment of bronchospasm in cases of anaphylaxis. Bronchodilators are not first line in suspected anaphylaxis, as they do not prevent or relieve other manifestations of anaphylaxis such as hypotension.3,8
Additional treatments for resistant bronchospasm include inhaled or IV bronchodilator,7,8,30 IV magnesium, 31 which needs to be infused slowly due to its potential to cause hypotension, inhalational anaesthetics, and ketamine. 7
Post-crisis management
(Figure 6)
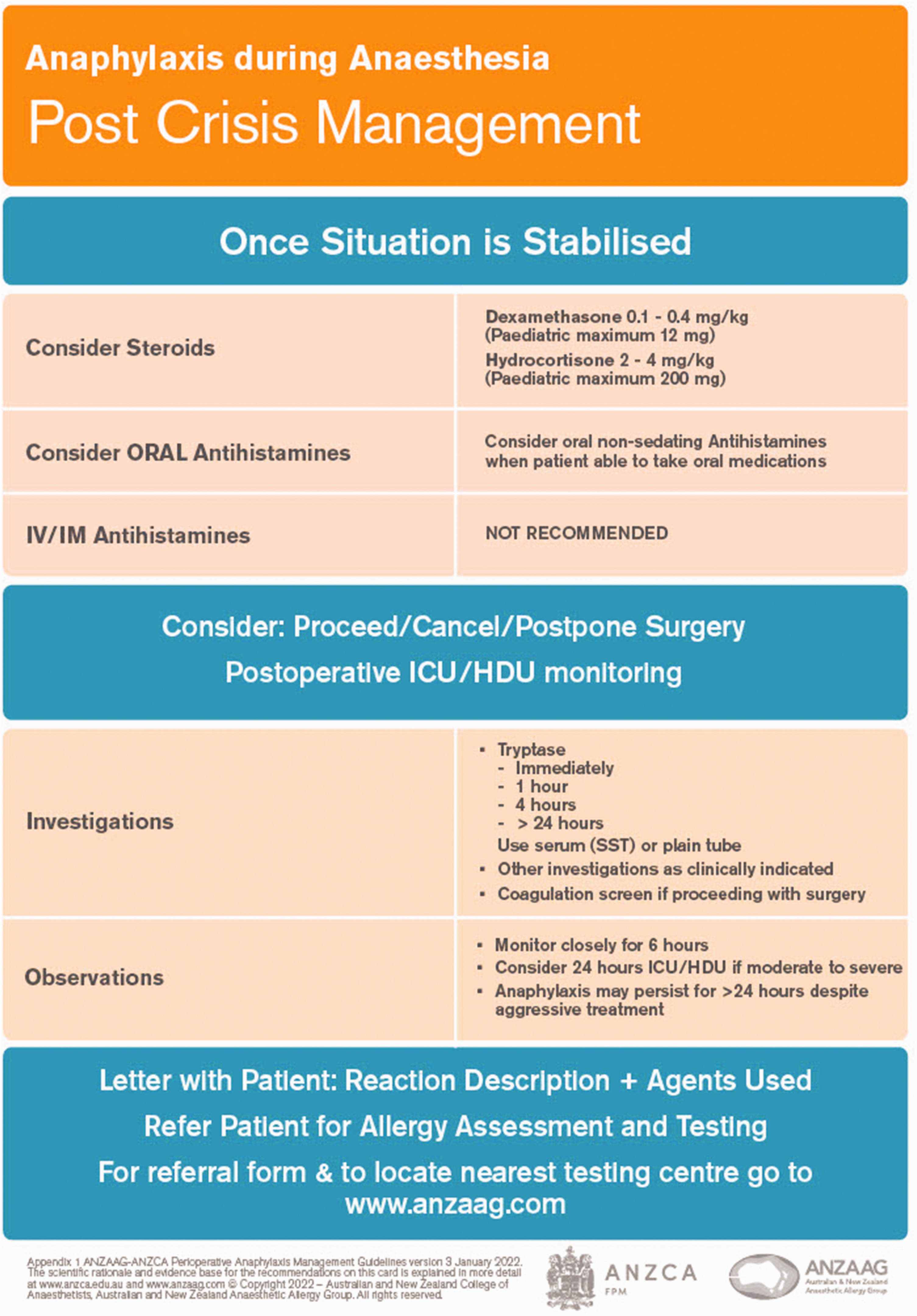
Post crisis management card.
Steroids are recommended to be administered after all acute management has been completed and patients are stable, and may be useful in cases of protracted reactions or biphasic response.25,32
Oral antihistamines, particularly non-sedating antihistamines, are suitable in the post-acute period.
Tryptase levels are important in differentiating anaphylaxis from other causes, and should be collected when any suggestion of perioperative anaphylaxis is raised.
A serum tryptase sample should be taken as soon as possible after the onset of symptoms and then repeated at 1 h, 4 h and after 24 h.
Conclusion
Perioperative anaphylaxis is an uncommon challenging and potentially life-threatening event. The updated perioperative anaphylaxis management guideline and the anaphylaxis cards replace the previous 2016 guideline, and can guide a perioperative team to achieve crucial time-critical management steps. It is recommended that the guideline be widely promoted, be made available in all anaesthetising locations, and used in current anaphylaxis management continuing professional development teaching.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) wish to forward their sincere thanks to those who worked on the earlier editions of the perioperative anaphylaxis management guidelines, ANZAAG and ANZCA members for their valued suggestions and feedback during the revision of the guidelines, Frances Rowsell and the ANZCA design team for assistance in card design.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.