
Abstract
Thyroid eye disease is an autoimmune inflammatory disorder of the orbit in adults. It causes inflammation, expansion and fibrosis of orbital fat, muscles and the lacrimal gland, leading to facial disfigurement, functional disability and, in severe cases, blindness. Overall, approximately 20% of affected patients need some form of surgical intervention requiring anaesthesia. This narrative review explores the background of thyroid eye disease, surgical procedures performed and their implications for anaesthesia. General anaesthesia is used for orbital decompression procedures, strabismus correction surgery and complex oculoplastic procedures. Local anaesthetic infiltration or regional anaesthesia under monitored anaesthesia care are the techniques most commonly employed for eyelid retraction surgery. It is important to limit the volume of local anaesthetic agent used during infiltration and continuously monitor the orbital volume and ocular pressure with a ballottement technique. In addition, the contralateral eye should be checked and, if necessary, protected against corneal exposure. Retrobulbar, peribulbar and sub-Tenon’s blocks are best avoided. Topical anaesthesia has been used for some strabismus correction surgery but its use is limited to motivated and cooperative patients only.
Introduction
Thyroid eye disease (TED), also known as thyroid-associated orbitopathy and Graves’ ophthalmopathy, is an autoimmune inflammatory disorder and is the most common cause of orbital disease in adults. 1 The estimated prevalence is 19 per 100,000 population, with a female to male ratio of 5:1. 2 It can cause facial disfigurement, functional disability and, in severe cases, permanent visual loss. Although the majority of patients have only mild self-limiting ocular involvement, 3 approximately 3%–7% of patients have a severe sight-threatening condition due to persistent corneal exposure or compressive optic neuropathy. 2 Overall, about 20% of TED patients require surgical intervention. 4
There are no specific recommendations on anaesthesia care for ophthalmic procedures in patients with TED. This narrative review provides a brief background of TED, related surgical procedures performed and the anaesthetic considerations in patients with TED presenting for ophthalmic procedures.
Search strategy
A literature search was conducted in March 2020 using MEDLINE (Ovid) with the aim of identifying English language articles published between January 1970 and March 2020. The search keywords used included ‘anaesthesia’ in various combinations and ‘thyroid eye disease’. Relevant case reports were also included. A total of 34 articles were retrieved in the initial search result, including two case reports.5,6 The authors examined these articles in terms of quality and relevance to anaesthesia for TED. Further related key articles were retrieved from the references of the searched articles. Additional references were added for major topics (hyperthyroidism, hypothyroidism, perioperative management of patients on long-term steroid therapy) that are beyond the scope of this review article. As a result, a total of 67 relevant articles are included in this review.
Thyroid eye disease: Clinical features and treatment options
TED causes inflammation, expansion and fibrosis of orbital fat, muscles and lacrimal glands, but the exact pathophysiology remains unclear.7,8 Many clinical manifestations are related to an increased soft tissue volume, leading to higher pressures within an unexpandable bony orbital cavity. Accurate clinical evaluation is essential for early diagnosis, identification of high-risk disease, planning of medical and surgical interventions and assessment of response to therapy. Clinical features may be assessed using the VISA classification (V, vision, optic neuropathy; I, inflammation, congestion; S, strabismus, motility restriction; and A, appearance, exposure) (Table 1), which helps in determining disease severity and activity using both subjective and objective measures. 7
VISA classification on disease grading of thyroid eye disease.
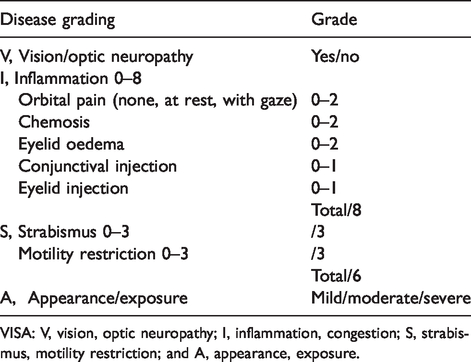
VISA: V, vision, optic neuropathy; I, inflammation, congestion; S, strabismus, motility restriction; and A, appearance, exposure.
Patients presenting with TED have variable thyroid status (90% hyperthyroid, 6% euthyroid, 3% Hashimoto’s thyroiditis and 1% hypothyroid). 9 The biphasic disease course of TED (active and quiescent) does not always coincide with systemic thyroid activity. 10 Inflammation during the active phase can lead to enlargement of orbital muscles, conjunctival injection and chemosis, swelling of the periocular tissues and eyelids and ocular pain. The active phase may last for months to years with fluctuation of symptoms. The quiescent phase (following spontaneous resolution of the active phase), is characterised by atrophy, fibrosis and sclerosis of extraocular muscles, leading to subsequent restrictive strabismus. 2
Cigarette smoking, both active and passive, is the most important modifiable risk factor for the development or worsening of TED1,8,10 (odds ratio 7.7). 11 Smoking is associated with a higher degree of disease severity and a lower effectiveness of medical treatment, although the underlying mechanism is unclear. 1 The American Thyroid Association guidelines recommend that patients with TED should stop smoking and be referred to a structured smoking cessation programme. Passive smokers should also be identified and advised of its negative impact. 10
Conservative measures (e.g. lubrication with artificial tears and ointment, sunglasses, sleeping with elevated head position) are considered useful. 1 Oral selenium, an essential component of antioxidant enzymes, can retard the progression of mild TED.3,12,13 In moderate to severe TED, management includes the use of corticosteroids, immunosuppressants (non-specific immunosuppressants: e.g. cyclosporin, azathioprine, mycophenolate, mofetil and methotrexate; lymphocyte-specific immunosuppressants: e.g. rituximab, tocilizumab, teprotumumab), orbital irradiation and surgery.3,10,14 However, no treatments have been shown to prevent or reverse the underlying tissue changes in TED. 15 When surgery is indicated, orbital decompression is typically performed first, then strabismus surgery and eyelid retraction considered last, as each preceding procedure may influence the appearance and outcome of the following operation.16,17
Thyroid diseases have several implications for anaesthetists. Patients with well-controlled hyperthyroidism and hypothyroidism do not present with much difficulty. 18 However, patients presenting for emergency surgery with uncontrolled hyperthyroidism or myxoedema are at considerable risk. 19 The management of hyperthyroidism10,20 and hypothyroidism 21 is an extensive subject that has been covered comprehensively in the references cited. It is beyond the scope of this review, and only issues relevant to anaesthesia in the context of this paper are covered.
Hyperthyroidism
The classic features of thyrotoxicosis include hyperactivity, weight loss and tremor. Of particular importance to anaesthetists are the cardiovascular effects, which may include atrial fibrillation, congestive cardiac failure and ischaemic heart disease. 22 Treatment includes antithyroid drugs (e.g. methimazole, carbimazole, propylthiouracil), beta-blockers (e.g. propranolol, metoprolol, atenolol) and corticosteroids. 23 In order to prevent ‘thyroid storm’, a rare but dreaded complication, attempts are made to make patients euthyroid before surgery.19,23,24
Hypothyroidism
Cardiovascular effects of chronic hypothyroidism include bradycardia, hypertension, increased systemic vascular resistance, decreased myocardial contractility and decreased cardiac output. Myxoedema coma, the most severe form, may progress to cardiovascular collapse and death. 23
There is some debate about whether surgery should be postponed in mild or subclinical hypothyroidism. 23 One prospective study found an increased incidence of transient postoperative atrial fibrillation in subclinical hypothyroidism patients compared to euthyroid patients undergoing coronary artery bypass grafting, but no significant differences in other outcomes. 25 One retrospective study found no significant differences in the outcome of anaesthesia and surgery in hypothyroid patients presenting for all types of surgery compared with matched euthyroid patients, and the authors concluded there was no evidence to justify deferring surgery in patients with mild to moderate hypothyroidism. 26 However, it is preferable to postpone elective surgery as the pathophysiological changes are generally reversible with thyroid hormone replacement. 23 Most hypothyroid patients who are receiving hormonal replacement and are clinically euthyroid do not appear to have an increased risk of perioperative morbidity. 27
Common surgical procedures in thyroid eye disease
Orbital decompression
The orbit is cone-shaped, bounded by bone posteriorly, medially and laterally and by the orbital septum anteriorly. It limits forward displacement of the eye in response to increased orbital volume—described as compartment syndrome. 28 The orbital contents are subject to the pressure–volume dynamics of a closed compartment. A significant rise in intraorbital pressure may compromise blood supply to susceptible tissues, resulting in potential optic nerve damage and visual loss.
Orbital decompression surgery increases the volume inside the bony orbit by removing orbital bone and adipose tissue. 29 Indications include optic nerve compression, globe subluxation, exposure keratopathy and restoration of premorbid appearance. 30 There are many surgical approaches (e.g. transcaruncular, transconjunctival and transnasal endoscopic) to perform this operation. 31 The average duration of anaesthesia is 134 minutes for unilateral and 184 minutes for bilateral surgery. 32 Diplopia after surgery is common, with the highest rate (38%–60%) reported after inferomedial decompression. 2 Blindness is the most devastating complication, with an incidence of approximately 0.5%, related to surgical trauma, pressure damage, or retrobulbar haemorrhage. 31 Cerebral spinal fluid leak and meningitis, although rare, are known to occur. 32
Strabismus surgery
In TED, extraocular muscles undergo a characteristic fusiform enlargement due to inflammatory cell infiltration. This may involve one or all extraocular muscles, either unilaterally or bilaterally. 33 Degenerative changes and fatty infiltration follow, with eventual replacement by fibrous tissue, causing strabismus. 34 The inferior rectus and medial rectus muscles are often involved in TED. 35 Most strabismus-related diplopia does not require surgical intervention as it can be managed effectively with prism spectacles. 36 Surgery is indicated for intractable diplopia, abnormal head positioning, or cosmetic purposes.
The surgical aim is recession of affected fibrotic extraocular muscles. Muscle resection should be avoided as it may worsen the existing restriction.2,17 Adjustable suture strabismus surgery, performed as a two-stage procedure, is considered beneficial. 37 Conventional recession with an adjustable suture knot is performed usually under general anaesthesia in the first stage. Once the patient recovers from general anaesthesia, ocular alignment and diplopia is re-assessed, and if necessary, the suture is adjusted under topical anaesthesia as a second stage procedure.
Injection of botulinum toxin to the affected extraocular muscles may temporarily relieve restrictive strabismus and may have some lasting effects. 17 In cooperative adult patients, it can be performed transconjunctivally with electromyographic guidance under topical anaesthesia 38 while intravenous sedation may be required for anxious patients. 39
Eyelid retraction surgery
The aetiology of eyelid retraction is multifactorial (increased sympathetic tone, muscle fibrosis and scarring). Non-surgical management includes injection of hyaluronic acid gel fillers and botulinum toxin to the affected muscles. 40 Tarsorrhaphy is useful to limit corneal exposure. 29 Other surgical procedures include implantation of a weight (e.g. gold or titanium) into the upper lid, recession of eyelid retractors, blepharotomy, insertion of ‘spacer’ material to lengthen the eyelid and eyelid contouring. 17 These procedures are increasingly performed under local anaesthetic infiltration, usually with sedation under monitored anaesthetic care. 41
Anaesthetic considerations
The long-term management of TED is best done in a multidisciplinary clinic consisting of endocrinologists and ophthalmologists with expertise in the condition. Other specialties may be consulted (e.g. radiation therapy, plastic surgery, endocrine surgery and otolaryngology). 10 Patients should ideally be euthyroid and have been in the quiescent phase of TED for at least six months before undergoing ophthalmic surgical intervention.2,4,17,31 Patients with uncontrolled thyroid dysfunction are more likely to experience severe pathology from TED2 and may have an increased risk of thyroid storm.19,23,24 In one study, the intraoperative use of beta-blockers was significantly higher in patients with mild to moderate biochemical hyperthyroidism when compared to euthyroid patients for thyroidectomy (not reported during surgery for TED) (28.1% versus 8.5%, P = 0.002), although there was no statistical difference in mortality, length of postoperative stay or intraoperative signs consistent with thyrotoxicosis. 42
Preoperative considerations
In TED patients, attention should be directed to the possibility of comorbidities, including autoimmune disorders (such as diabetes mellitus), or smoking-related disease. 32 In addition, difficulty with airway management may arise in the presence of a goitre. 18 Preoperative screening for coagulation disorders is important and radiological imaging of both orbits is essential in patients scheduled for orbital decompression. 32 Further investigations are dependent on the nature of any preoperative morbidity.
Patients receiving triiodothyronine (T3, half-life 1.5 days) are advised to continue their usual dose on the day of surgery, while it is optional for patients taking tetraiodothyronine (T4, half-life seven days).18,23 All anticoagulant medications (warfarin, antiplatelet agents, novel oral anticoagulants) should be discontinued, whenever possible, especially before orbital decompression. 32
This patient group may be on long-term corticosteroids. Surgery and anaesthesia pose several problems in these patients such as an increased risk of infection for both superficial and deep surgical site infections, 43 poorly controlled blood glucose levels 44 and acute adrenocortical insufficiency. 45 The Association of Anaesthetists, the Royal College of Physicians and the Society of Endocrinology, United Kingdom, have published a consensus document providing guidelines for the management of these patients during the perioperative period. 44 Supplementary corticosteroids and prophylactic antibiotics should be considered. In addition, these patients may have fragile skin, difficult intravenous access and an increased incidence of bruising.
Choice of anaesthetic techniques
General anaesthesia
In general, the duration of surgery varies between one and three hours, depending on the complexity and extent of surgery. General anaesthesia is typically the chosen modality for orbital decompression,32,41 strabismus correction surgery 35 and complex oculoplastic (plastic and reconstructive surgery of the periorbital and facial tissues) procedures. In addition to the usual anaesthetic considerations, patients with TED require other special consideration. Careful positioning of the facemask is important during the induction of anaesthesia as proptosed eyes are more prone to abrasion injury. 32 The airway can be maintained with either a south-facing endotracheal tube (such as RAE, i.e. Oral Ring–Adair–Elwyn, Covidien, Dublin) 18 or reinforced supraglottic airway devices with spontaneous breathing or mechanical ventilation. Anaesthesia can be maintained with either a volatile agent or total intravenous anaesthesia. 32 Forced duction testing is performed before any strabismus correction surgery to evaluate the restrictive nature of the squint.17,35 A non-depolarising muscle relaxant is preferred over suxamethonium, if required, as it does not interfere with forced duction tests. 46
The Difficult Airway Society, the British Association of Oral and Maxillofacial Surgery and the British Association of Otorhinolaryngology, Head and Neck Surgery in their consensus statement no longer recommend the routine insertion of a throat pack (e.g. for transnasal endoscopic surgery) by the anaesthetist, as in a systematic review there was no supportive evidence of its benefit yet many documented complications, including severe postoperative airway obstruction and death. 47 They also recommended that if a throat pack is used, it should be entered into the surgical count with the anaesthetist responsible for checking its removal and the airway patency before extubation. 47 Intravenous acetazolamide is often administered as a routine during orbital decompression to reduce intraocular pressure and improve surgical access. 32
The hypermetabolic state of hyperthyroidism may affect some anaesthetic drugs. The infusion rate of propofol during total intravenous anaesthesia, for instance, should be increased in the initial setting as its clearance and volume of distribution are significantly increased in the presence of hyperthyroidism when compared to euthyroid patients (e.g. clearance: 5.1 l/min versus 2.5 l/min; volume of distribution: 10.0 l/kg versus 2.8 l/kg in one study) 48 and the depth of anaesthesia titrated to the desired effect using an anaesthetic depth monitor.
Manipulation of the globe, especially during traction of extraocular muscles, may precipitate the oculocardiac reflex and result in sudden bradycardia or arrhythmia. 49 Symptoms are generally mild and transient in most cases, with the cessation of globe traction usually restoring normal cardiac rhythm. If sustained or severe, it can be managed with an anticholinergic agent. In a retrospective case series of 98 orbital decompression procedures, anticholinergic therapy for bradycardia was required in 30% of cases. 32
Urgent orbital decompression for severe optic neuropathy in uncontrolled hyperthyroid patients, although rare, presents the biggest challenge to anaesthetists. Such patients’ cardiac status should be optimised and beta-blockers are most commonly used for this purpose. 23 Intraoperative invasive monitoring may be indicated. 23
Regional ophthalmic anaesthesia
Retrobulbar, peribulbar and sub-Tenon’s blocks are best avoided in TED as the orbit is already congested. Any rise in intraocular pressure resulting from injected local anaesthetic solution50,51 or accidental orbital haemorrhage 52 may be detrimental. Severe deterioration of Graves’ ophthalmopathy in a stable mild patient after a retrobulbar block for cataract surgery has been reported. 5 Anterior globe dislocation during a peribulbar block in a TED patient with marked exophthalmos has also been reported. 6
Sensory innervation to the periocular area is via the ophthalmic and maxillary divisions of the trigeminal nerve. Selective block of an individual branch of the trigeminal nerve (e.g. supraorbital nerve, supratrochlear nerve and infraorbital nerve) or combined nerve blocks have been described for upper eyelid procedures.53,54 This is considered useful in extensive eyelid surgery and medically unwell patients, but in modern oculoplastic surgery, however, these techniques are not commonly used despite no tissue distortion by the local anaesthetic infiltration at the surgical site.
Local anaesthetic infiltration
Local anaesthetic infiltration is the technique most commonly employed for eyelid retraction surgery 41 as it allows patient cooperation during surgery and has better postoperative outcomes.17,54 Other advantages include rapid recovery, good postoperative analgesia and a reduction of morbidity associated with general anaesthesia. 55 However, it is unsuitable for complex oculoplastic procedures, as it causes tissue distortion at the operative site that may hinder surgical accuracy, especially when aggravated by a further risk of bleeding. Minimally invasive orbital decompression surgery for mild to moderate proptosis under local anaesthesia with sedation has been described. 56 Of importance is that the orbits are significantly altered in TED, which affects the way an injection is performed. The increased tissue volume and fibrosis limit both the injectable volume and the way the anaesthetic fluid tracks. The likely changes are hard to estimate and quantify as each patient is different, therefore it is important that the orbital volume and ocular pressure are continuously checked by manual ballottement. If there is suspected high orbital pressure, it is important to assess whether the patient has maintained vision (direct questioning, bedside hand movements and counting fingers check). The retinal artery should be visualised, if necessary, to assess adequate retinal perfusion.
Adrenaline is often added to the local infiltration solution to prolong its anaesthetic effect, reduce peak blood levels and provide haemostasis. Adrenaline in concentrations of 1:50,000, 1:100,000 and 1:200,000 has been shown to have the same effect on vasoconstriction, therefore using the lowest effective concentration is recommended. 57 Hyaluronidase may also be added to enhance the diffusion of local anaesthetic solution and limit the rise in orbital pressure. However, it should not be used in patients with known allergy to bee stings, as cross-reactivity between bee venom and hyaluronidase exists. 57 There is no evidence to suggest that there is any difference in dose requirement of adrenaline or hyaluronidase in patients with TED.
Local anaesthetic infiltration to the eyelid can also be administered as adjuvant therapy to general anaesthesia during orbital decompression procedures to reduce intraoperative bleeding and provide postoperative analgesia. 32
Topical anaesthesia
Recession strabismus surgery has been performed under topical anaesthesia. 58 Topical anaesthesia also allows immediate assessment and correction in adjustable suture strabismus surgery, enabling completion of the procedure in a single stage. 59 A major drawback, however, is the inability to perform intraoperative forced duction testing, 58 an important assessment in evaluating the restrictive nature of the squint. Only motivated and cooperative adult patients are suitable for this technique as pain and discomfort are common, especially during disinsertion of extraocular muscle. 60
Monitored anaesthesia care
Conscious sedation, in conjunction with local or regional anaesthesia, is useful in reducing anxiety and providing comfort to the patients. A variety of sedative agents and techniques are popular, including propofol, midazolam and a short-acting opioid, alone or in various combinations. Low-dose midazolam (e.g. 0.5 mg bolus before local anaesthetic infiltration, then 1 mg per hour infusion) has been effective in a prospective clinical trial. 55 No technique is absolutely safe, and care rendered by an appropriately skilled anaesthesia practitioner is of paramount importance.
Overall, local anaesthetic infiltration with monitored anaesthetic care is most commonly employed for eyelid retraction surgery while general anaesthesia is used for orbital decompression, strabismus surgery and complex oculoplastic procedures. 41
For all anaesthetic care in patients with TED, the cornea is at greater risk of exposure damage. This, in part, is due to increased orbital volume expansion, as well as lagophthalmos (inability to close the eyelids completely) from upper lid retraction. The contralateral eye will need increased vigilance and protection from desiccation. It should be checked and, if necessary, protected with ointment and taping.
Postoperative considerations
To minimise bruising and swelling after oculoplastic procedures, patients are instructed to apply ice-cold water compresses at all times while awake for the first 72 hours. 61
A retrospective case series of 98 orbital decompression procedures in TED patients noted an 8% incidence of postoperative nausea and vomiting (PONV). Intraoperative antiemetic prophylaxis with intravenous ondansetron had been administered in 64% of the patients in the case series. 32 The authors did not specify whether the 8% of patients with PONV were or were not part of the 64% who had received intraoperative ondansetron.
There are no specific data on PONV after strabismus correction surgery in TED. In general, PONV occurred less frequently in adult strabismus surgery of all causes (e.g. adult 30% versus children 60%), independent of the general anaesthetic technique used.62,63 The recommendation from one study is a prophylactic ondansetron (150 µg/kg, maximum 4 mg) and dexamethasone (150 µg/kg, maximum 8 mg) combination for strabismus surgery in children. 64 The same combination is often administered prophylactically in adults. 65
There is a lack of research on postoperative pain in ophthalmic surgery, but some ophthalmic operations have been associated with significantly different postoperative pain intensities. 66 Ye et al. found that orbital decompression was more likely to induce significant postoperative pain compared with other minor ophthalmic surgical procedures (52% versus 26%). 67 Stannard et al., on the other hand, reported a postoperative pain score of zero in 86% of their patients (total n = 98) after orbital decompression procedures (49% of patients used only simple analgesia whereas 27% used no supplementary analgesia in the postoperative period). 32 Their analgesic regimen consisted of local anaesthetic infiltration to the eyelid in all the patients, while some received intravenous ketorolac 10 mg (n = 34) and intramuscular pethidine 50 mg (n = 3).
Conclusions
TED can cause facial disfigurement, functional disability and blindness. Patients may require some form of surgical intervention under anaesthesia. It is important to understand TED, its associated surgical procedures and their implications on anaesthesia and anaesthetic techniques.
The results of this review indicate that anaesthesia for patients with TED is similar to anaesthesia for any patient with thyroid disease. There are, however, a few specific considerations. It is essential to check and, if necessary, protect the contralateral eye for corneal exposure. General anaesthesia is used for orbital decompression, strabismus correction surgery and complex oculoplastic procedures. Retrobulbar, peribulbar and sub-Tenon’s blocks are best avoided as the orbit is already congested. Local anaesthetic infiltration and sometimes regional anaesthesia under monitored anaesthesia care are most commonly employed for eyelid retraction surgery. It is important to limit the volume of local anaesthetic infiltration and continuously monitor the orbital volume and ocular pressure by manual orbital ballottement. Topical anaesthesia has a very limited role for strabismus correction surgery because of the inability to perform intraoperative forced duction tests.
Footnotes
Authors’ contribution(s)
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was not supported by any external funding sources.