
Abstract

Dear editor
“Lung-protective” mechanical ventilation may improve mortality from acute respiratory distress syndrome (ARDS), 1 but compliance with lung-protective ventilation protocols is low. 2 Calculating appropriate tidal volumes based on ideal body weight (IBW) is only defined for heights >152 cm, and extending protective ventilation, for example into paediatrics, has been shown to be complex. We present a case of ARDS in a patient with achondroplasia and spina bifida, where we used computed tomography (CT) reconstruction to guide tidal volume estimation. The patient’s written consent for publication was obtained.
A 30-year-old male with achondroplasia presented with dyspnoea, cough, and production of sputum. His past history included obesity, obstructive sleep apnoea, and spina bifida. Findings on exam were a height of 1.14 m, a weight of 68 kg, sinus tachycardia, respiratory distress, tachypnoea, rhonchi in all lung fields, and an SaO2 of 78% on non-rebreather facemask. A chest X-ray and subsequent CT diagnosed the patient with bilateral pneumonia. An arterial blood gas on high-flow nasal cannula showed hypercarbic and hypoxaemic respiratory failure, and he was converted to non-invasive bilevel positive airway pressure ventilation and admitted to our intensive care unit. The following morning, he demonstrated increased work of breathing, his SaO2 deteriorated, and he became obtunded. He was intubated and diagnosed with ARDS. We became concerned that the patient’s body habitus and height of 1.14 m made calculation of appropriate tidal volumes based on IBW unreliable.
Radiology was consulted and performed 3D reconstructions of his chest CT, providing an age-matched control with a stature of 1.63 m (Figure 1). In the control, we calculated a ratio of IBW tidal volume estimation to CT-derived lung volume. Assuming similar lung mechanics, we applied this ratio to derive an appropriate tidal volume for our patient. From the patient’s CT-derived lung volume of 612 mL, we calculated a tidal volume between 82 and 107 mL.
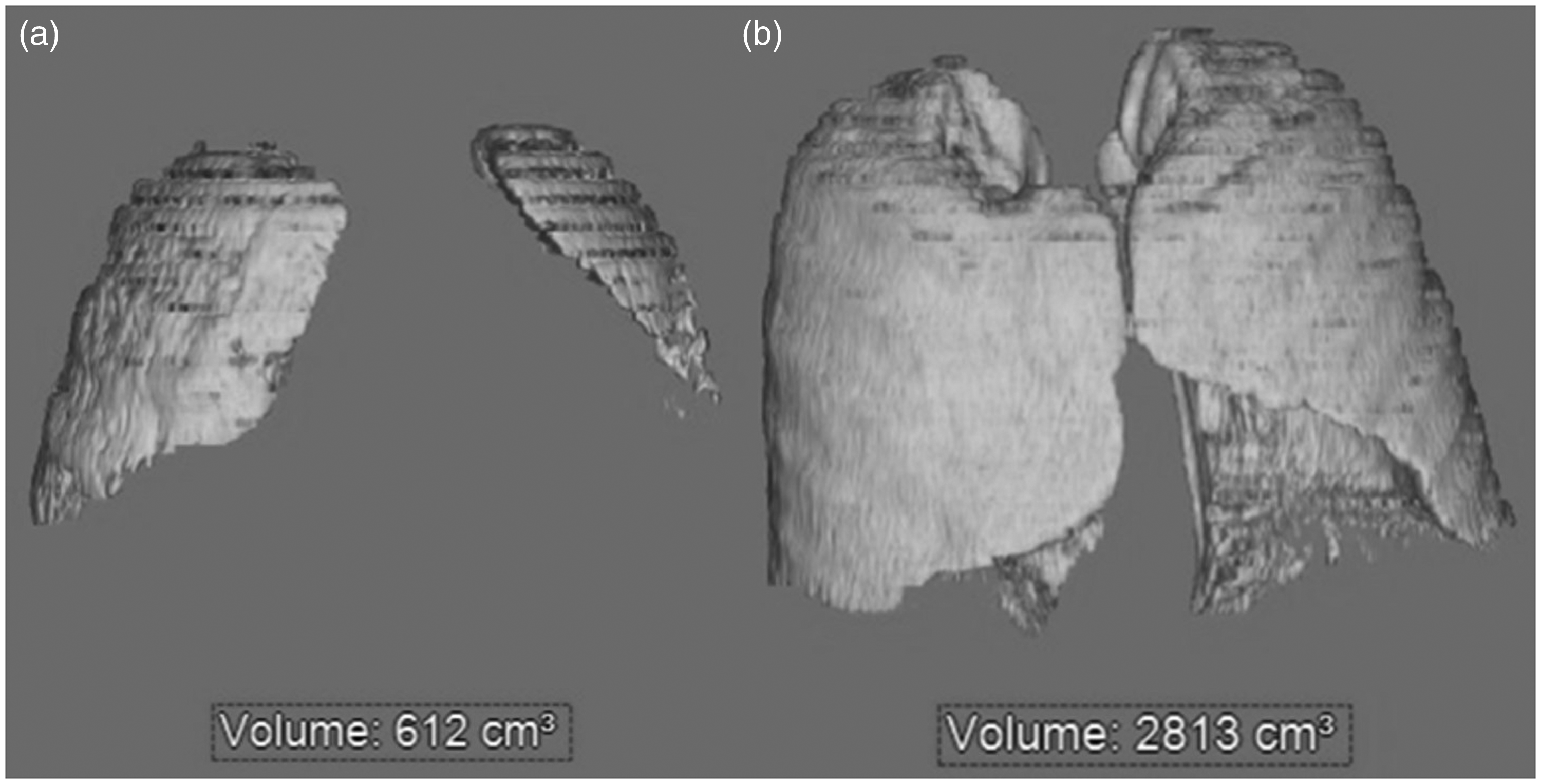
(a) Three-dimensional computed tomography reconstruction of the patient’s lungs with estimated volume during inhalation and (b) estimated volume during inhalation in an age-matched control.
After sedation and analgesia, his settings were adjusted to a tidal volume of 100 mL, positive end-expiratory pressure of 8 cm H2O, a rate of 30/min, and an FiO2 of 50%. Given that his initial settings were based on an estimated appropriate lung volume, his tidal volume was adjusted at the bedside for patient comfort. The tidal volume where he became appropriately synchronous with the ventilator was 200 mL. After this adjustment, an arterial blood gas demonstrated a pH of 7.46, a PaCO2 of 43 mmHg, and a PaO2 of 103 mmHg.
The remainder of his stay was uneventful. His pneumonia was treated, and he was extubated on hospital day 3 before being discharged on hospital day 7.
Reviewing the literature on lung mechanics in individuals with achondroplasia, we encountered two articles.3,4 Both suggest that stature and weight are very poor predictors for estimation of pulmonary volumes. Given the individual nature of our patient’s lung volumes, we attempted to gain an understanding of volumes using a CT scan that had already been obtained. Lung volume was calculated with an approach that is routinely used to characterise volumes in three-dimensional structures. 5 Assuming that our patient’s lungs would be functionally normal,3,4 we calculated a ratio of CT-derived volume to ARDSnet recommended tidal volume 1 in a normal-height adult and applied it to our case to estimate a functionally similar tidal volume.
This approach has limitations. Decreased aeration impacts pulmonary volume and may impact CT-derived pulmonary metrics. While we thus would not recommend this technique as a routine measure, it may be useful as a tool to help guide the initial estimation of appropriate tidal volumes in the group of patients in whom conventional formulae cannot be applied.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, or publication of this article.