
Abstract

Paediatric cuffed endotracheal tubes were developed to effectively seal the airway around the tube while avoiding excessive transmucosal pressure, because the micro-thin polyurethane cuff membrane seals the airway at ultra-low pressure. 1 However, the manufacturer’s website reported that the micro-thin polyurethane material used to make endotracheal tube cuffs could exhibit water condensation within the cuff, 2 and condensation in the inflation line and pilot balloon could cause inaccurate reading of intracuff pressure. We experienced a case of cuff leakage by the combination of water condensation and a continuous automatic cuff pressure monitor.
Consent of the patient’s next of kin was obtained for publication. A six-year-old boy with viral pneumonia caused by severe influenza A was admitted to the intensive care unit (ICU). He was 110 cm in height and weighed 20 kg. Immediately after admission to the ICU, his trachea was intubated with a 5.5 mm cuffed endotracheal tube (Microcuff® Paediatric Endotracheal Tube, Halyard Health Inc, Yokohama, Japan). His lungs were mechanically ventilated (Puritan Bennett 840® ventilator, Covidien Japan, Tokyo, Japan). He was on pressure control ventilation set at a fraction of inspiratory oxygen of 60%, a driving pressure of 15 cmH2O, an inspiratory interval of 0.8 s, positive end-expiratory pressure of 10 cm and 20 mandatory breaths by mechanical ventilation. Intracuff pressure was set at 15 cmH2O and monitored by a continuous automatic cuff pressure monitor (Electronic cuff pressure controller®, Covidien Japan, Tokyo, Japan). At two days after ICU admission, ventilatory failure occurred because of endotracheal tube cuff leakage. The child showed no signs of inadequate sedation or change in position, so cuff damage was suspected; however, the alarm did not sound on the automatic cuff pressure monitor. The cuff worked well for short intervals whenever the cuff was manually inflated, but cuff leakage repeatedly occurred. By close examination of the tube line, we could see that the tube line was occluded with water condensation (Figure 1). After the intracuff pressure was reset to 25 cmH2O, cuff leakage did not occur. The manufacturer has recommended that the water be cleared from the inflation line by gentle manipulation of the pilot balloon to push the water back to the cuff and pressure readings should be done after the manipulation. In this case, we used an automatic cuff pressure monitor that was recently developed. It is currently being used in clinical settings to overcome difficulties in maintaining a specific cuff pressure. This minimizes the damage to the respiratory tract mucosa and prevents cuff leakage. 3 Therefore, we did not recognize that we measured the pilot balloon pressure but not the intracuff pressure. An intracuff pressure of 25 cmH2O rather than 15 cmH2O could have been more effective in pushing the water back to the cuff; however, applying an intracuff pressure of 25 cmH2O could be harmful for children. 4 Careful monitoring of cuff tube water condensation is essential, especially when using an automatic cuff pressure monitor.
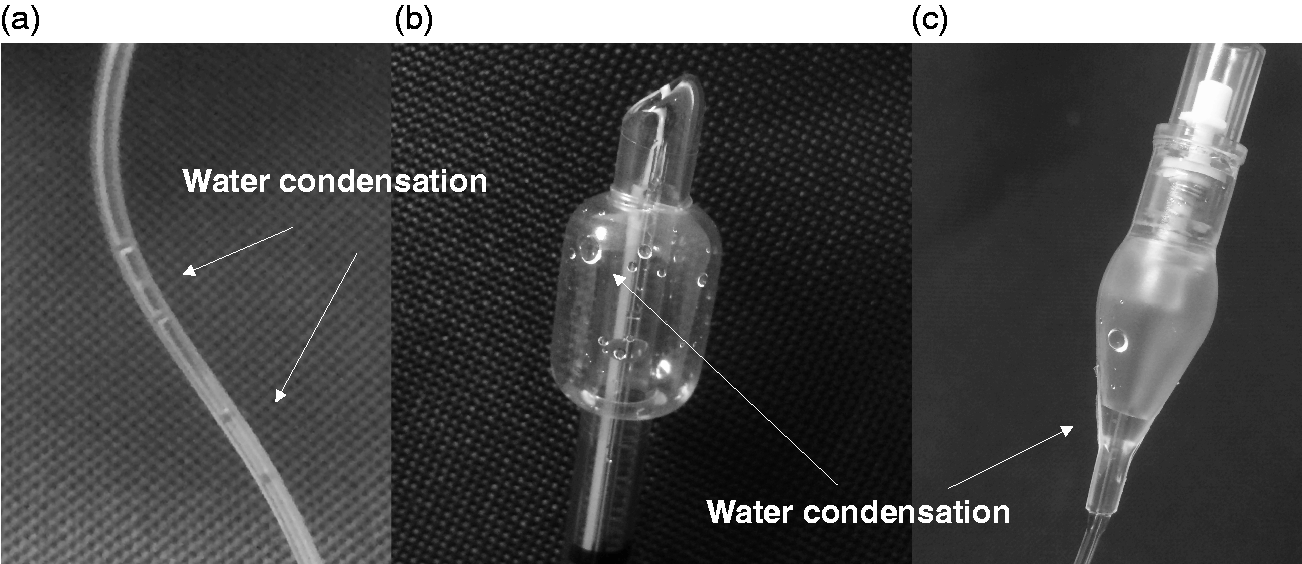
Water condensation in the cuff tube. (a) Cuff tube. (b) Cuff. (c) Pilot balloon.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure
Consent was obtained from the patient’s next of kin for this case report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was solely through departmental sources.