
Abstract
Background:
The Comprehensive Lower limb Amputee Socket Survey (CLASS) is a self-reported measure developed to assess prosthetic socket fit in individuals with lower limb amputation.
Objective:
To assess the reliability and validity of the Persian version of the CLASS.
Study Design:
Cross-sectional and repeated-measures.
Methods:
We evaluated the translation and back translation of the CLASS and made the required changes according to expert committee feedback. Then, we recruited 124 participants with unilateral lower limb amputation (89.5% men). Internal consistency was analyzed with Cronbach’s alpha and test–retest reliability using intra-class correlation coefficients. Convergent construct validity was assessed by comparing the CLASS scores with the Persian version of the Trinity Amputation and Prosthesis Experience Scales (TAPES) scores. In addition, known groups construct validity was assessed by comparing CLASS scores between groups with different causes and levels of amputation.
Results:
Cronbach’s alpha coefficient represented a very good internal consistency for all domains of the Persian CLASS (ranged from 0.86 to 0.92). The intra-class correlation coefficient for test–retest reliability for the Persian CLASS was good to excellent (ranged from 0.73 to 0.97). There was a significant correlation between the subscales of the Persian CLASS and satisfaction subscales of the Persian TAPES (p < 0.001). There was no significant difference between the Persian CLASS scores by cause or level of amputation.
Conclusion:
The Persian CLASS is a reliable and valid measure for evaluating prosthetic socket fit.
Background
People with amputation have different physical, psychological and social challenges. 1 Dysvascular conditions, traumatic injuries, cancers, and congenital limb deficiencies are the most common reasons for lower limb amputation (LLA). 2 Prosthetic limbs aim to restore mobility function and improve health-related quality of life for people with LLA. 3
A high-quality prosthetic limb with good socket fit is necessary for assuring functional use. 4 Factors such as prosthetic socket design, 5 suspension technique, 6 socket fit and comfort, 7 and prosthetic limb appearance 7 are related to satisfaction and rehabilitation outcomes among individuals with LLA. An appropriate suspension system can reduce the rotary, vertical, and horizontal movement of the residual limb in the prosthetic socket, which increases the socket’s stability. 8 Furthermore, proper fit and comfort are highly associated with higher patient satisfaction and quality of life among individuals with LLA.4,9,10
Several objective techniques are available to assess the fit of the lower limb prosthesis. They include the roentgenographic method, 11 photoelectric sensors, 12 photographic technique, 13 and motion capture system. 14 However, such techniques are not always accessible to prosthetists as they are costly and data gathering is time-consuming. 15 In a clinical setting, subjective measures are obtained by the prosthetist, who gets verbal feedback from an individual with LLA to evaluate his or her prosthetic socket fit during different tasks such as standing and walking. However, a standardized tool is needed to measure prosthetic socket fit and record changes over time.
Subjective tools such as the Trinity Amputation and Prosthesis Experience Scales (TAPES), 16 the Prosthesis Evaluation Questionnaire (PEQ), 17 and the Socket Comfort Score (SCS) 18 have been developed to assess prosthetic-related outcomes. The TAPES and the PEQ evaluate the impact of a prosthetic limb, as a whole, with respect to psychosocial parameters, functional limitations, satisfaction, weight, and aesthetics. The SCS is a self-reported, one-item scale to assess prosthetic socket comfort. 19 However, the specific task that causes discomfort or movement of socket’s position in relation to the residual limb is not clear with this scale. Furthermore, the test–retest reliability of the SCS is affected by administration mode (paper vs electronic). 19
Prosthetic-based daily activities of an individual with LLA include a variety of tasks such as sitting, standing, walking, and ascending or descending stairs that require a proper socket fit. Therefore, a reliable measure with strong validity is required to assess the fit of a prosthetic socket. Recently, Gailey et al. 20 developed the Comprehensive Lower limb Amputee Socket Survey (CLASS). It is intended to provide a self-reported measure for evaluating prosthetic socket satisfaction in individuals with LLA. It is a reliable, simple, and easy to use tool for monitoring and evaluating the static and dynamic characteristics of a prosthetic socket while doing different tasks such as walking, sitting, standing, and stairs.
There are no data to support validity and reliability of the CLASS in languages other than English. Therefore, we aimed to translate and cross-culturally adapt this survey for Persian speaking individuals with LLA.
Methods
This cross-sectional and repeated-measures study took place from February to August 2018. We collected the data from an orthotics and prosthetics center in Tehran, Iran. All participants signed an informed consent before participating in the study. In addition, we contacted the CLASS developers (Advanced Rehabilitation Therapy, Inc., Miami, FL) by email before the study to obtain the required permission to translate the questionnaire.
Translation and cultural adaptation
We performed the translation and cultural adaptation processes according to guidelines for cross-cultural adaptation process for self-report measures. 21 In the first stage, two professional bilingual translators whose native language was Persian were invited to translate the original English version of the CLASS into Persian. We gave the necessary information to one translator about the study purpose and conditions of individuals with LLAs. However, the other translator, who had no health sciences’ knowledge background, received no information in this regard. After completing the translation, two other translators and a research team compared the two versions. They identified potential differences between two versions and resolved them by group discussion.
In the second stage, two bilingual translators who were fluent in English were asked to translate the draft Persian translation of CLASS into English. Again, two translators and our research team compared the two versions and resolved any disagreements through group discussion. Finally, an expert committee consisting of four translators, a methodologist, two physical therapists, and six prosthetists reviewed all the translations to find semantic, idiomatic, experiential, and conceptual equivalence between the two versions of the CLASS. After that, a pre-final Persian version of the CLASS was prepared. Then, we asked 20 Persian-speaking individuals with LLA to complete it to ensure it was understood easily. The participants were encouraged to ask about any confusing questions or content, mark unclear content in each question, and indicate the reason why the question was not clear. None of them reported any ambiguous or unclear questions. Therefore, the final version of the CLASS was obtained using this method.
Participants
A convenience sample of 124 individuals with unilateral LLAs was recruited. The distribution of their characteristics such as gender, age, amputation level, Medicare Functional Classification Level, and amputation cause was consistent with the attributes of the general target population.20,22 The inclusion criteria were as follows: (1) having a unilateral ankle disarticulation, transtibial amputation, knee disarticulation, or transfemoral amputation, (2) being older than 18 years, (3) being able to read and write in the Persian language, and (4) having used their current prostheses for at least 3 months. 20
Instruments
The CLASS
The CLASS is a self-report instrument for assessing the fit of a prosthetic socket in individuals with LLA. It has 15 items in four subscales: stability, suspension, comfort, and appearance. Each of the first three subscales has four items that evaluate the prosthetic socket fit in sitting, standing, walking, and going up and down stairs. The appearance subscale includes three items measured in standing and sitting positions and wearing tight pants. 20
For each item, the participants rated their perception of prosthetic socket fit on a 4-point ordinal response scale from 1 to 4 (1 indicated the worst and 4 indicated the best condition). In addition, 0 indicated that the activity is unrelated to the individual with LLA. The CLASS score for each subscale was represented on a 0%–100% scale (with 100% indicating excellent satisfaction). 20
The TAPES
The TAPES is a multidimensional self-report questionnaire, specifically for individuals with amputation. It is categorized into three sections: psychosocial adjustment, activity restriction, and satisfaction. Each section has three subscales. 23 The psychosocial adjustment section includes 15 items graded on a 5-point ordinal response scale. It is divided into three parts: general, social, and limitation adjustments. Each subscale’s score ranges from 5 to 25 with higher scores indicating a greater level of adjustment.
The activity restriction section includes 12 items based on a 3-point ordinal response scale. It is divided into three parts: functional, social, and athletic activity restrictions. Each subscale score ranges from zero to eight, in which higher scores indicate a greater level of activity restriction.
The satisfaction section includes 10 items scored on a 5-point ordinal response scale. It is divided into functional, weight, and aesthetic satisfaction subscales. The scores are from 5 to 25 for aesthetic and functional satisfaction and 1 to 5 for weight satisfaction. Higher scores indicate a higher level of satisfaction. Overall, there are nine subscale scores for the TAPES. The TAPES was selected as a validation measure for the CLASS because it has a subscale that evaluates the individual’s satisfaction with their prosthesis, and satisfaction was expected to correlate strongly with socket fit.
Internal consistency and test-retest reliability
We evaluated the internal consistency and test–retest reliability for the Persian CLASS. Internal consistency of a scale reflects the extent of relationship between each item and the total score, and was calculated using Cronbach’s alpha (α). Test–retest reliability was assessed through the intra-class correlation coefficient (ICC), which is the correlation between the scores of a scale over repeated trials. According to Cohen’s formula, a minimum of 30 cases are needed for test–retest reliability to achieve a power of 0.8, effect size of 0.25, and alpha of 0.05. 24 Based on this, 32 participants were randomly selected and asked to complete the CLASS again after 2 weeks. We also calculated the standard error of measurement (SEM) and minimal detectable change (MDC) to evaluate response stability of the CLASS. The SEM and MDC were calculated with the following formulas: SEMagreement = (standard deviation difference (test score – retest score)÷√2); MDC = (1.96 × √2 × SEMagreement). 25
Convergent construct validity
Convergent construct validity refers to the relationship between two measures of a similar construct. 26 We asked all participants to fill the Persian CLASS and the Persian TAPES 27 to assess the convergent construct validity of the CLASS. We hypothesized that the satisfaction subscales of the TAPES woudl be most correlated with subscales of the CLASS.
Known groups construct validity
Known groups construct validity refers to the ability of a measure to distinguish between individuals who are known to have different characteristics. 28 We assessed the known groups construct validity of the CLASS regarding the cause (vascular, traumatic, and cancer) and level of amputation (ankle or knee disarticulations and transtibial or transfemoral amputation). Previous studies demonstrated that a transfemoral prosthesis can be less comfortable to wear than prostheses for other levels of amputation, and satisfaction of individuals with LLA is related to the appearance, prosthetic fit, residual limb pain, use of a prosthesis, and level of amputation.29,30
Statistical analyses
Descriptive statistics were reported by mean, standard deviation, range, and percentage of ceiling and floor effects. Cronbach’s α was used to assess the internal consistency. A value of 0.70 ⩽ α ⩽ 0.95 for Cronbach’s α indicated satisfactory internal consistency. 24 The ICC analysis with 95% confidence interval (CI) was used to assess the test–retest reliability. The distribution of the CLASS was skewed according to the Kolmogorov–Smirnov test (p < 0.05). Therefore, Spearman’s correlation coefficient was used to assess the association between the CLASS and TAPES scores for convergent construct validity. The correlation strength was evaluated as follows: good to excellent (r > 0.75), moderate to good (0.50 < r < 0.75), small (0.25 < r < 0.50), and little to no correlation (r < 0.25). 31 We assessed the known groups construct validity of the CLASS with respect to the causes and levels of amputation using the Kruskal–Wallis test.
We considered a threshold of p < 0.05 as the statistical significance level for all correlation coefficients. All statistical analyses were conducted using SPSS version 17 (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of the study population
A total of 124 individuals with LLA (111 males, 13 females) participated in this study. Their mean of age was 49.5 ± 11.9 years. There were 93 cases (75%) with trauma-related LLA, 23 (18.5%) with dysvascular causes of LLA, and 8 (6.5%) with cancer-related LLA. Among participants with transtibial amputation (65 participants), there were 32 (49.2%) with soft insert socket, 25 (38.4%) with pin and lock mechanism, and 8 (12.3%) with suction suspension socket. Among participants with transfemoral amputation (35 participants), there were 26 (74.3%) with suction suspension socket and 9 (25.7%) with seal-in liner systems. All participants with Syme disarticulation (11 participants) had sleeve suspension systems. Of the 13 participants with knee disarticulation, 7 (53.9%) had a soft insert mechanism and all others (46.1%) had a silicone sealing liner. Among our participants 27% had K2 and 73% had K3 activity levels. Table 1 summarizes characteristics of the participants.
Demographic and clinical characteristics of the study population.
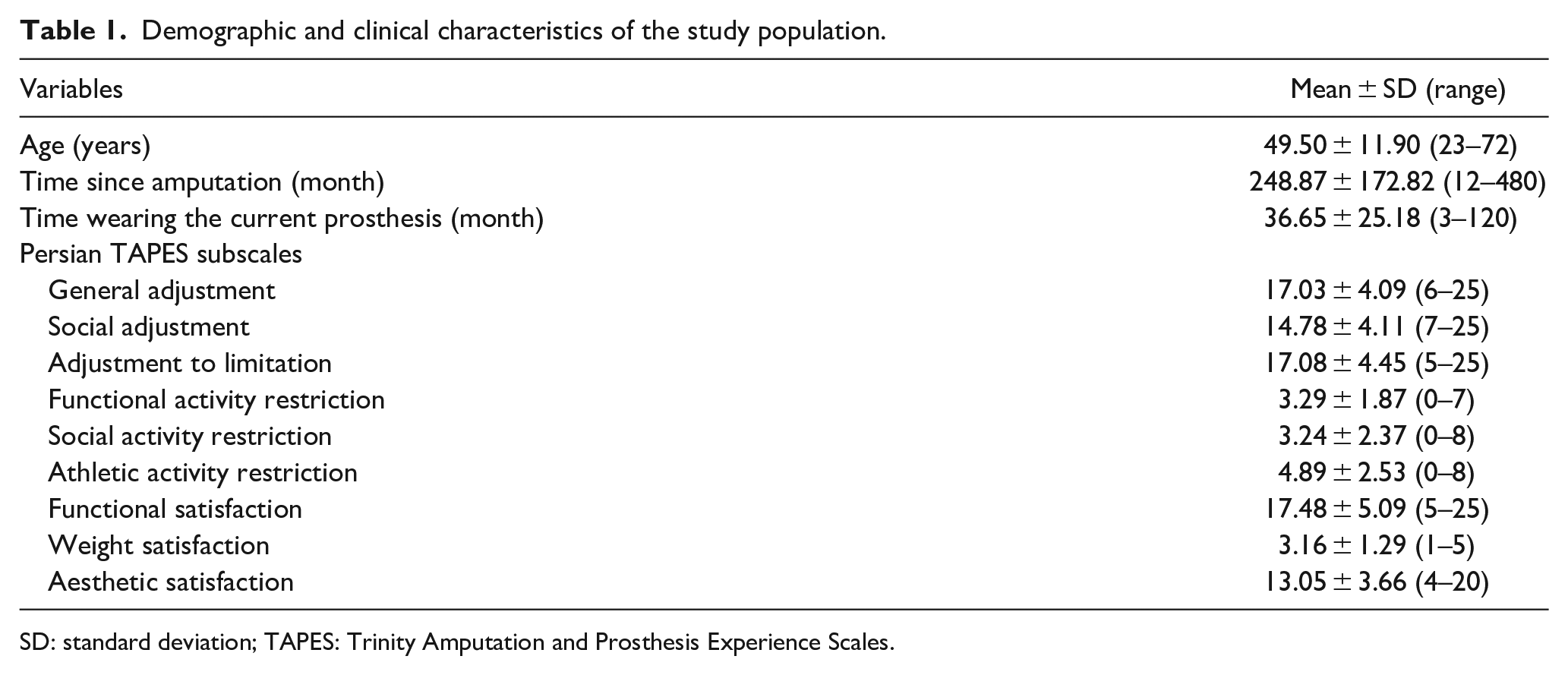
SD: standard deviation; TAPES: Trinity Amputation and Prosthesis Experience Scales.
Ceiling and floor effects
No significant floor effects were observed in any subscales of the Persian CLASS. However, there was a significant ceiling effect (16.1%) in the suspension domain (Table 2).
Descriptive statistics and results of the reliability analyses.
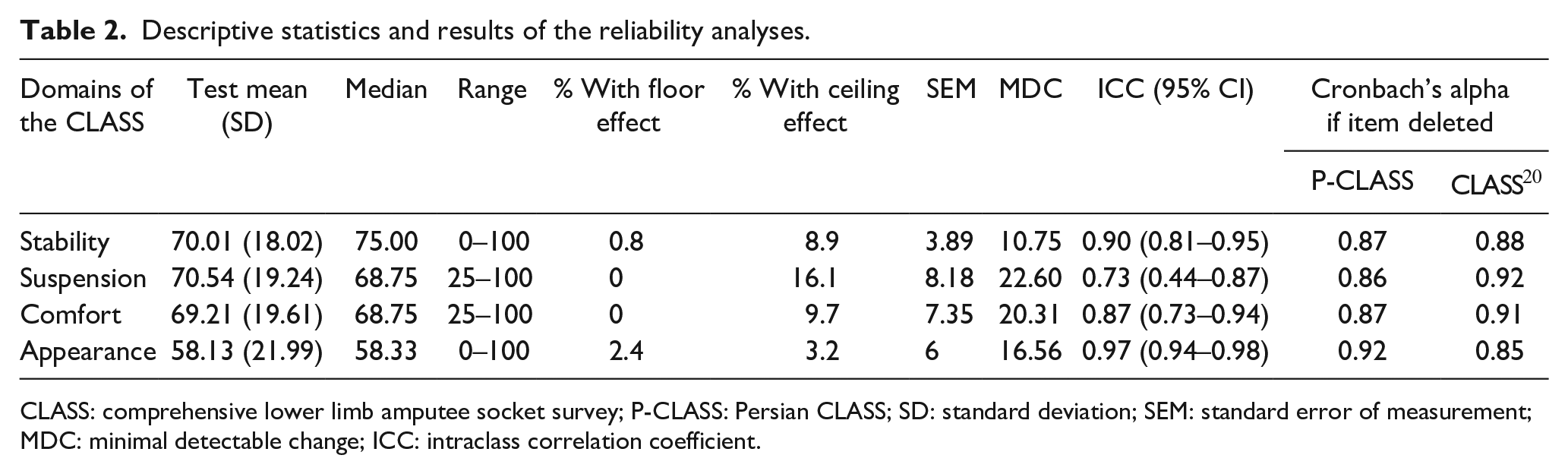
CLASS: comprehensive lower limb amputee socket survey; P-CLASS: Persian CLASS; SD: standard deviation; SEM: standard error of measurement; MDC: minimal detectable change; ICC: intraclass correlation coefficient.
Reliability
The Cronbach’s alpha for the Persian CLASS subscales ranged from 0.86 for suspension to 0.92 for appearance subscales (Table 2). The ICC analysis indicated that the stability of the Persian CLASS over time is good (0.73) to excellent (0.97).
Convergent construct validity
Table 3 illustrates the matrix of correlations between the subscales scores of the Persian CLASS and those of the Persian TAPES. There was a positive, moderate to good correlation between the stability and suspension subscales of the CLASS and the functional and weight satisfaction subscales of the TAPES (p < 0.001). In addition, there was a positive, moderate to good correlation between the comfort subscale of the CLASS and the functional satisfaction of the TAPES (p < 0.001). Finally, there was a positive, moderate to good correlation between the appearance subscale of the CLASS and the aesthetic satisfaction subscale of the TAPES (p < 0.001).
The relationship between the domains of the Persian CLASS and the Persian TAPES questionnaires.
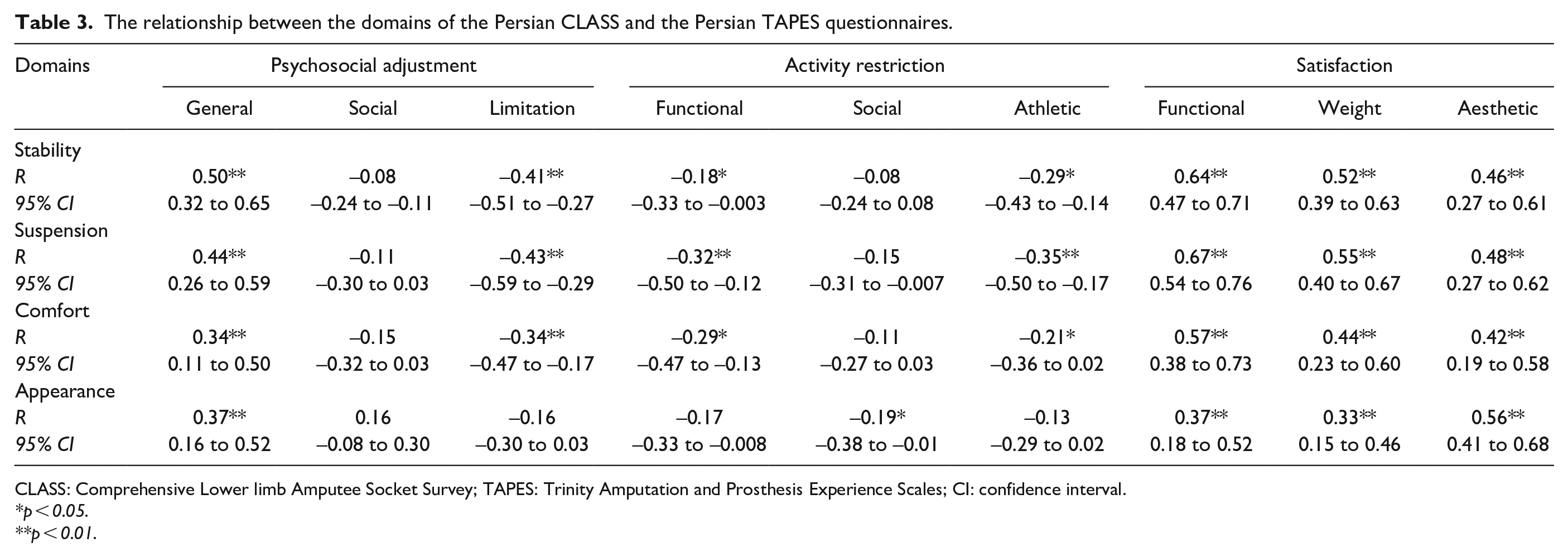
CLASS: Comprehensive Lower limb Amputee Socket Survey; TAPES: Trinity Amputation and Prosthesis Experience Scales; CI: confidence interval.
p < 0.05.
p < 0.01.
Know groups construct validity
There were no statistically significant differences in CLASS subscales scores between groups of participants by causes of amputation (dysvascular, trauma, and cancer). However, there was a significant difference in comfort subscale scores between individuals grouped by different levels of amputation (ankle or knee disarticulations and transtibial or transfemoral amputations (p=0.03, Figure 1). As shown in Figure 1, individuals with transfemoral amputation reported the lowest level of satisfaction with socket comfort, and individuals with ankle disarticulation reported a highest level of satisfaction with socket comfort.
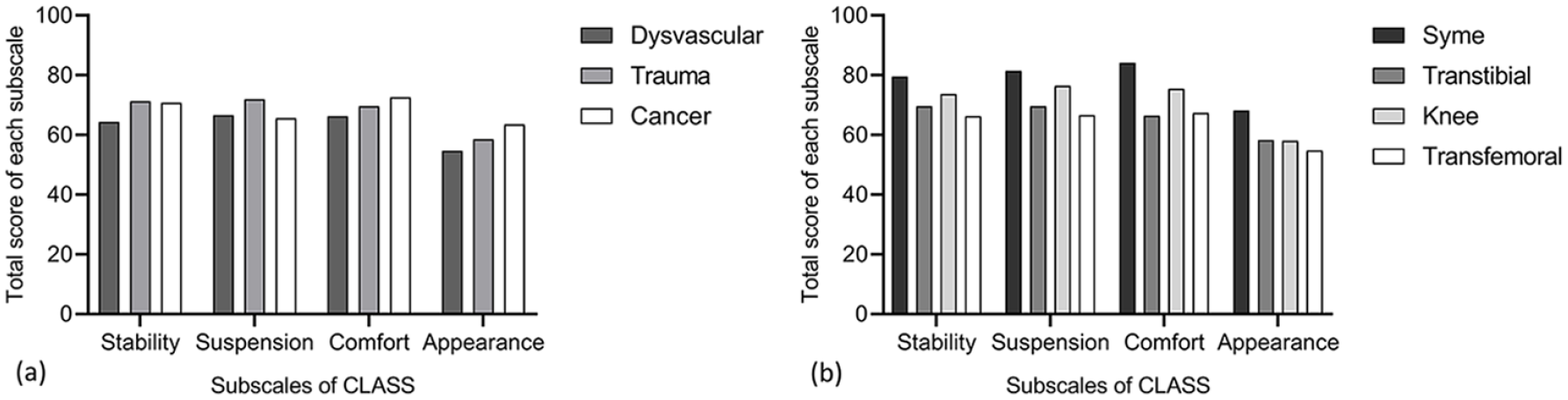
Comparison of Persian CLASS subscale scores among participants with different amputation (a) causes and (b) levels.
Discussion
Our study aimed to assess the psychometric properties of the Persian CLASS for individuals with unilateral LLA. The results sowed that there is a good internal consistency, test-retest reliability, and moderate to good correlation between the Persian CLASS subscales and satisfaction subscales of the Persian TAPES. In addition, we found significant differences in Persian CLASS comfort subscale scores between individuals with different levels of amputation.
Resuming walking ability is the most important objective of a rehabilitation team for individuals with LLA. An amputee’s satisfaction with a prosthetic limb is highly associated with the time spent using it.7,32 Enhancing socket fit and comfort can increase the optimal use of the lower limb prosthesis, as well as the ability to do daily activities. 33 In a study on individuals with trauma-related LLA, Dillingham et al. 34 found that only 43% of participants were satisfied with their prosthesis comfort. Dissatisfaction with the prosthetic socket fit may lead to its rejection or frequent visits to the prosthetic center. 35 In a clinical setting, if a person with LLA has a problem with the prosthetic socket, the prosthetist does his or her best to deal with it. Indeed, this modification can be optimized if there is a common language or similar terminology between the prosthetist and the patient so that they understand each other. When a prosthetist asks a patient about his or her prosthetic socket fit, different individuals may have a different understanding of what socket fit is, which will affect the answer they give. Some individuals may express that their “socket is too loose or too tight.” Others may report that when they wear the socket, they need to use additional prosthetic socks to attain and sustain socket fit. Therefore, using a reliable measure such as the CLASS is an efficient method for creating a common language between individuals with LLA and prosthetist. Individuals with amputation can easily and accurately describe aspects of their prosthetic socket fit during standing, sitting, walking, and going up and down stairs using this tool. This may help the prosthetist to accurately assess the extent of a person’s socket fit and troubleshoot the cause of problems in each visit.
Our results revealed a satisfactory internal consistency for each subscale of the Persian CLASS. In the original English version of the CLASS, 20 the internal consistency ranged from 0.85 to 0.92, which is consistent with the Persian CLASS. Except for the appearance domain, the value of Cronbach’s alpha in our study was less than that of the original English version. Although test–retest reliability was not reported for the English version of the CLASS, the Persian version had an acceptable level of test–retest reliability (0.73 to 0.97). There are no other studies reported in the literature to which we can compare our reliability results. We found a moderate to good correlation between the Persian CLASS subscales and the functional, weight, and aesthetic satisfaction domains of the Persian TAPES. This provides initial evidence of construct validity for the Persian CLASS as a measure of prosthetic socket fit. However, the correlations between the Persian CLASS subscale scores and the other Persian TAPES subscales, including psychosocial adjustments and restrictions, were small. A reason might be the differences in constructs measured by these instruments. The CLASS measures the satisfaction with prosthetic socket fit, while these TAPES subscales evaluate an individual’s quality of life and overall experience of using a prosthetic limb. 27
We found that the Persian CLASS could not distinguish between individuals with different causes of amputation. This might be because of our small number of participants for each group, hence reducing the statistical power of this analysis. In our study, most of the participants had transtibial amputation (52%), and 75% of LLAs were traumatic. Furthermore, the overall satisfaction with a prosthetic socket fit was more than 60%, with a lower satisfaction for those with dysvascular LLAs, compared to those with cancer-or trauma-related LLAs. We assumed that a more distal level of amputation might be associated with a higher level of satisfaction, which was inconsistent with the outcomes. The participants with ankle disarticulation showed the highest level of satisfaction, followed by knee disarticulation, transtibial, and transfemoral amputation. Amputation through the joints provides less bony and muscular disruptions for the residual limb. Therefore, individuals with ankle or knee disarticulation can have more balanced muscular control and are better able to load bear at the distal end. In addition, the distal bony contours provide anatomic suspension of the prosthetic limb that increase the stability of the prosthetic socket. 36
Limitations
This was the first study on the translation and cross-cultural adaptation of CLASS to another language and culture. However, it has several limitations. Most of the participants were men. Thus, we cannot generalize the results to women with unilateral LLAs. The cause of amputation and gender distribution in this study was generally consistent with the greater population of persons with amputation in Iran. 22 Furthermore, the physical characteristics of individuals with bilateral LLAs are different from those with unilateral LLAs. 37 This may limit generalizability of these findings to bilateral LLAs. We cannot compare the satisfaction from prosthetic socket fit between participants with different activity levels. The reason is the absence of individuals with K1 and K4 activity levels since all of our participants had K2 and K3 activity levels.
Conclusion
Our results provided support for the reliability of a Persian version of the CLASS instrument, with some initial evidence of construct validity. Therefore, the Persian CLASS may be a useful measure to assess the prosthetic socket fit for individuals with LLA. Additional work is still needed to assess the responsiveness of the Persian CLASS in this population.
Footnotes
Acknowledgements
The authors thank Muhammed Hussein Mousavinasab and Marjan Saeedi for editing this text.
Author contributions
NR, EE, TB, MK, VM, BB, and HP were responsible for Conceptualization. NR, TB, VM, BB, and HP were responsible for Data curation. NR, TB, EE, and VM were responsible for Formal analysis. NR, EE, TB, MK, VM, BB, and HP were responsible for Methodology. NR, EE, TB, and MK were responsible for Writing—original draft. NR, EE, TB, MK, VM, BB, and HP were responsible for Writing—review & editing. TB was responsible for Funding acquisition. NR, EE, TB, MK, and VM were responsible for Investigation. TB was responsible for Project administration. NR, TB, VM, BB, and HP were responsible for Resources. NR, TB, and VM were responsible for Software. TB was responsible for Supervision. NR, EE, TB, MK, VM, BB, and HP were responsible for Validation. NR, TB, and EE were responsible for Visualization.
Ethical Approval
All study procedures were approved by the Iran University of Medical Sciences ethics review board, approval number 1397.1343.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant no. 1397.1343 from the Rehabilitation Research Center of Iran University of Medical Sciences.