
Abstract
Background:
Transtibial amputation and subsequent prosthetic fitting can cause prolonged hospital length of stay (LOS). Recently, a two-staged admission pathway for new transtibial amputees was introduced in a local hospital to shorten hospital LOS.
Methods:
A retrospective cohort study was performed to review the 5-year outcomes of major lower extremity amputation in a local hospital and to compare the difference in LOS and functional outcomes between traditional (group 1) and two-staged (group 2) admission pathways for new transtibial amputees.
Results:
The fitting rate was 55% in transtibial amputees, 14% in transfemoral amputees, and only 3.7% in dementia patients. For new transtibial amputees, the mean postoperative LOS was significantly reduced by 32.8 days in group 2. Besides, more patients in group 2 were able to walk without aid.
Conclusion:
LOS for new transtibial amputees can be greatly reduced by the two-staged admission pathway to minimize hospital operational cost.
Introduction
Transtibial amputation and subsequent prosthetic fitting can cause prolonged hospital length of stay (LOS) that greatly increases hospital operational cost. The traditional pathway to treat new amputees in public hospitals usually takes months to remain as inpatient until the first prosthesis is fitted.
Recently, a two-staged admission pathway for new transtibial amputees was introduced in a local hospital to shorten hospital LOS (Figure 1). This new pathway includes (1) discharging amputee once medically fit and independent in walking with aid, (2) ongoing monitoring of discharged amputee and prosthetic fitting in outpatient clinics, and (3) readmission for prosthetic training.
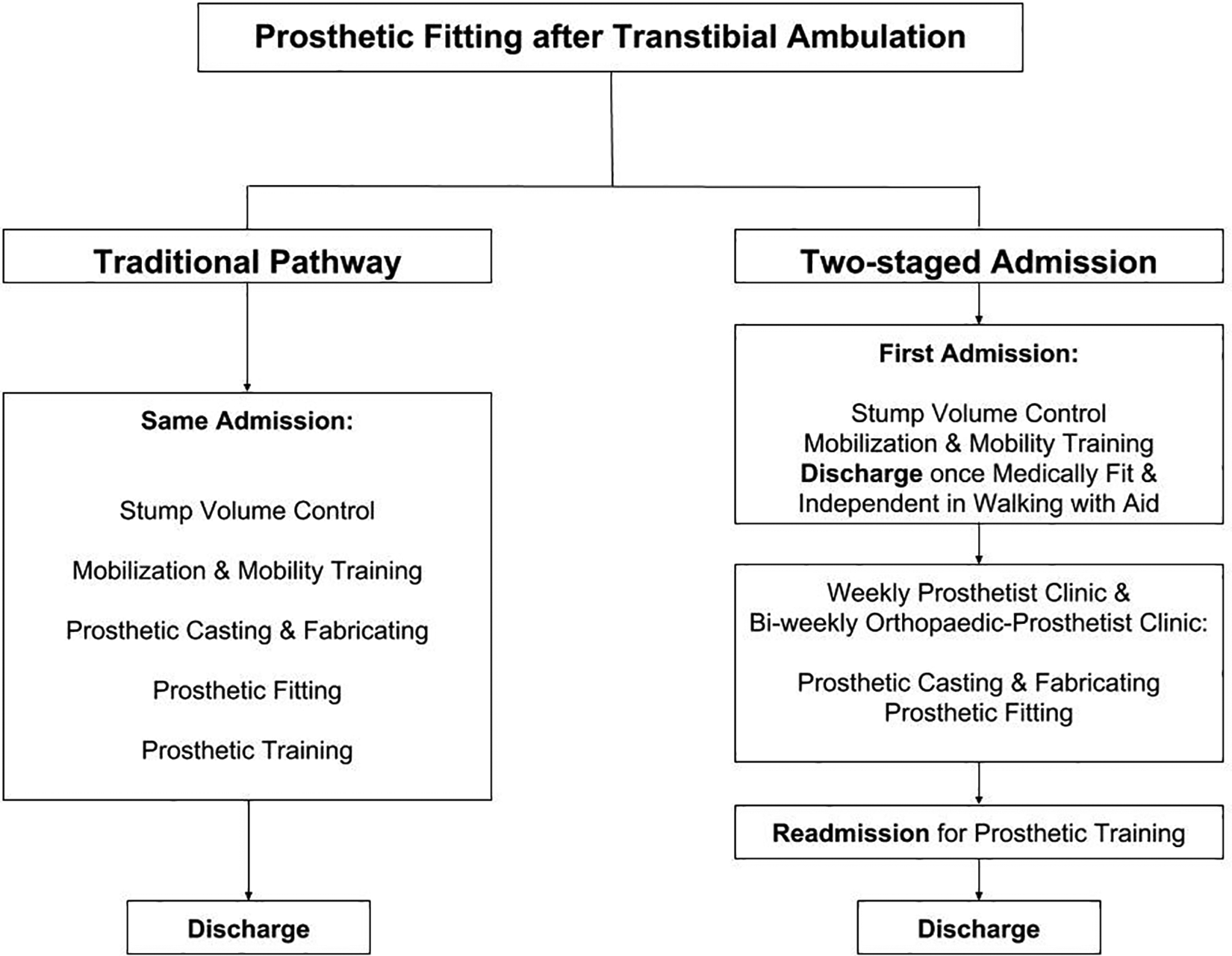
Traditional and new pathways for prosthetic fitting after transtibial amputation.
In the past, there were two major rate-determining steps in prosthetic fitting, namely, the static stump volume for casting and the availability of the prosthesis once the stump volume became static, which kept patients remained in the hospital for weeks. Through this new pathway by dividing the inpatient care into two admissions, better resource allocation could be achieved. In one of our local orthopedic centers, prosthetic fitting and training were done in entirely outpatient basis. In our experience, the second-stage admission was necessary to gather the multidisciplinary team (including orthopedic surgeon, nurse, prosthetist, physiotherapist, occupational therapist and medical social workers, etc.) together to convert the fragmented outpatient care into becoming interdisciplinary approach.
This retrospective cohort study aims at (1) reviewing the 5-year outcomes of major lower extremity amputation (LEA) in a local hospital and (2) comparing the difference in LOS and functional outcomes between traditional pathway and two-staged admission pathway for new transtibial amputees.
Methods
The hospital database was reviewed from January 1, 2013, to December 31, 2017. Seventy-five patients with major LEA performed were identified. They were male-dominant (50 males and 25 females) with a mean age of 70.7 ± 14.5 SD. There were 42 transfemoral and 33 transtibial amputations. Etiology for major LEA, LOS, mortality rate, premorbid functional status, prosthetic fitting rate, and ambulatory status on last follow-up was evaluated.
Besides, transtibial amputees with prosthetic fitting were identified for further analysis. Our exclusion criteria included death or loss to follow-up during study, noncompliance in using prosthesis, bilateral lower limb amputees, and poor upper limb or contralateral lower limb function. They were divided into two groups: first prosthetic fitting in same episode of admission (group 1) versus first prosthetic fitting in two admissions (group 2). The inclusion criteria for group 2 were no major perioperative medical comorbidities or complications that affect mobility (such as stroke and myocardial infarction), no significant stump wound complications, good self-stump bandaging technique, independent walking with aid (modified functional ambulation category (MFAC) V or above) postoperatively, no major psychosocial factors preventing early discharge (such as living in nonlift landing apartment or living alone), and lastly, patient’s and relatives’ understanding and acceptance for early discharge. Independent t-test was performed to compare the difference in LOS between the two groups. The p value <0.05 was considered statistically significant.
Immediate postoperative care was standardized. Bandaging was applied immediately after operation to control stump volume. Knee extension splint was then applied to protect the wound and to prevent knee flexion contracture until first prosthetic fitting. Regarding the designs of prosthesis, amputees were fitted with modular endoskeletal prostheses. Total surface bearing socket with a liner was used to enhance socket comfort and protect the stump wound (Figure 2). Either dynamic response feet or solid ankle cushioned heel feet were prescribed based on activity level, age, premorbid functional capability, body weight, medical comorbidities, and residual limb condition. Prosthetic fitting for cosmetic purposes was excluded in this study.
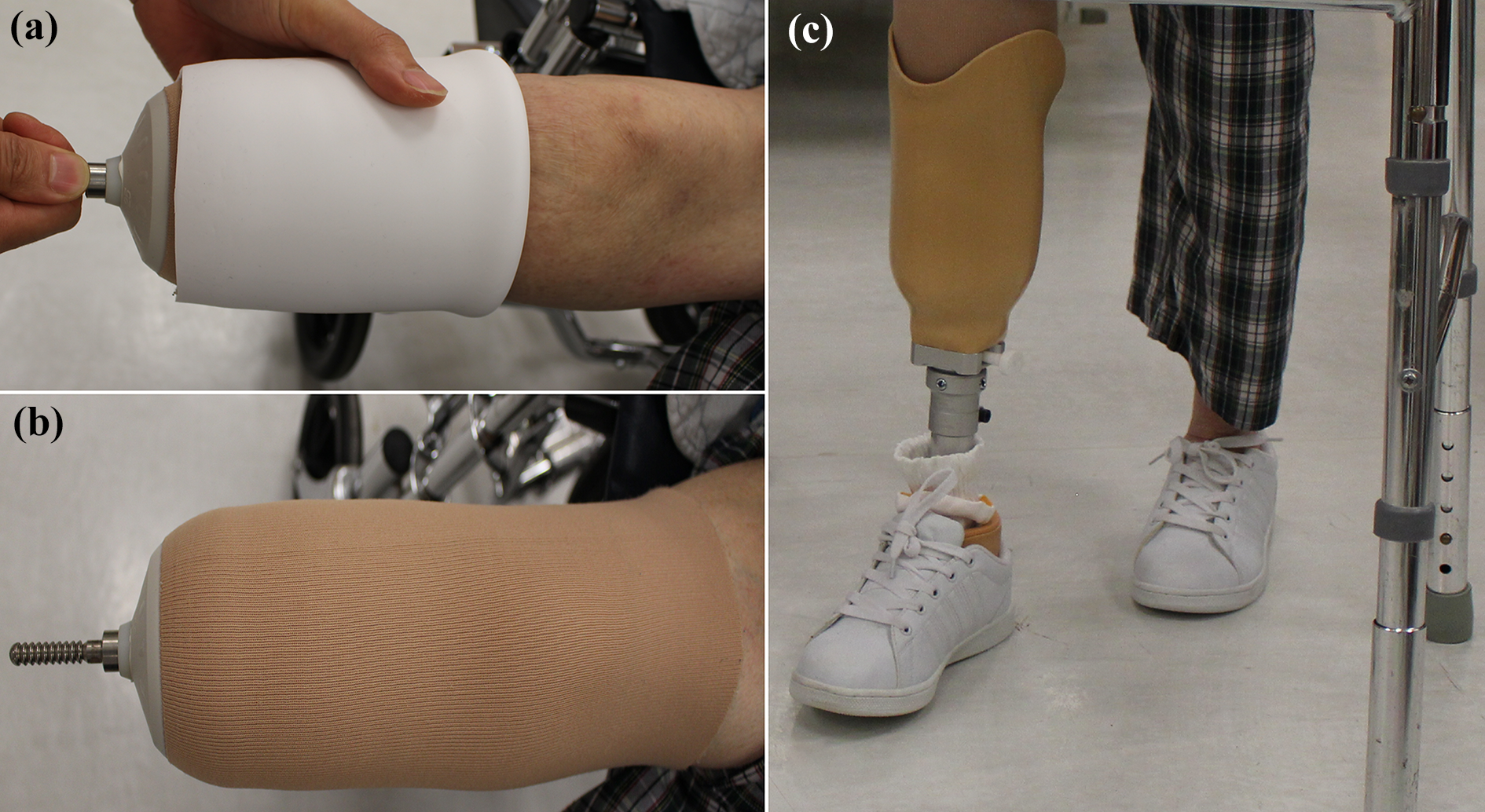
Donning of prosthesis. (a) The silicone liner was rolled up the stump and (b) the pin lock system connects the liner to the socket (c).
Results
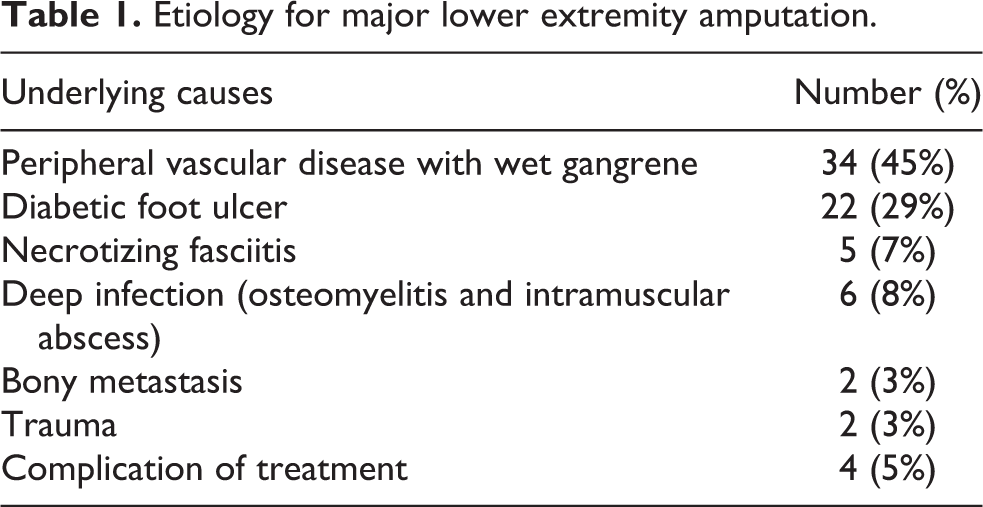
Infection (presented as wet gangrenous changes of peripheral vascular disease, infected diabetic ulcer or osteomyelitis, etc.) accounted for nearly 90% of the etiology for major LEA (Table 1). Four cases were classified as complication of treatment secondary to high-dose inotrope under intensive care unit, rhabdomyolysis and acute renal failure after angioplasty for acute ischemic limb, and decubitus heel sores after prolonged bed confinement.
Etiology for major lower extremity amputation.
Two patients with bony metastasis at ankle regions received transtibial amputation for pain and tumor control. One of them was a 52-year-old man with renal cell carcinoma, presented with progressive right ankle pain after radical nephrectomy. X-rays showed an expansile lytic lesion over right distal tibia and fibula (Figure 3). Further radiological studies confirmed that it was a solitary metastasis but too extensive for wide local excision and reconstruction. Therefore, transtibial amputation was performed. He was able to walk unaided with prosthesis during adjuvant oncological treatment and remained alive for more than 1 year after amputation.

X-rays ((a) anteroposterior and (b) lateral) and MRI ((c) T1 and (d) T2) of metastasis of renal cell carcinoma to distal tibia and fibula. MRI: magnetic resonance imaging.
The mean LOS was 55.0 days, whereas the mean postoperative LOS (defined as days from last operation to discharge) was 31.1 days. Fourteen patients (nearly 20%) died of multiorgan failure in the same admission and the mortality rate was highest in necrotizing fasciitis (60%). For those who survived after amputation, 46% died of other medical causes within 5 years.
In terms of functional outcomes, 37 patients were premorbid-independent walker with MFAC VI to VII, one was assisted walker (MFAC IV), and remaining 37 were bed- or chairbound with MFAC I to II. The median premorbid MFAC was IV (interquartile range: II–VII). Around 40% had dementia before amputation. The overall prosthetic fitting rate was 32% (24 patients). In transfemoral amputees, who had poorer premorbid ambulatory and mental statuses and higher mortality rate, the fitting rate was 14% (six patients). On the other hand, the fitting rate was 55% (18 patients) in transtibial amputees. For those who remained to survive on the last follow-up, 25 of them were independent walkers and 39 were bed or chairbound. The median MFAC on the last follow-up was II (interquartile range: II–VII). In terms of premorbid mental status, the fitting rate in nondementia patients was 52.5%, while in dementia patients, it was only 3.7%.
Since our two-staged admission pathway was introduced in 2016, there were five transtibial amputees with first prosthesis fitted under this new pathway (group 2). After exclusion of eight patients in group 1 (four died or lost to follow-up, two with noncompliance and two with poor function of other limbs), there were 10 transtibial amputees with a mean age of 55.7 ± 9.3 SD recruited, five in each group. All of them had premorbid MFAC VII without dementia.
The mean LOS upon first discharge was significantly reduced in group 2 by 55.8 days when compared with group 1 (Table 2 and Figure 4). Moreover, mean total hospital LOS (including readmission for prosthesis training in group 2) and mean postoperative LOS were also significantly reduced by 46.2 and 32.8 days, respectively. It is notable that the mean postoperative LOS of 67.8 days in group 1 implied that it took more than 2 months to remain as inpatient after amputation for the first prosthesis to be fitted in traditional pathway. Furthermore, mean readmission interval in group 2 was 29.6 days, which implied that group 2 started using the first prosthesis for walking as outpatient 2 weeks earlier on average than group 1 (84.8 − 38.6 − 29.6 = 16.6 days).
Comparison of length of stay.
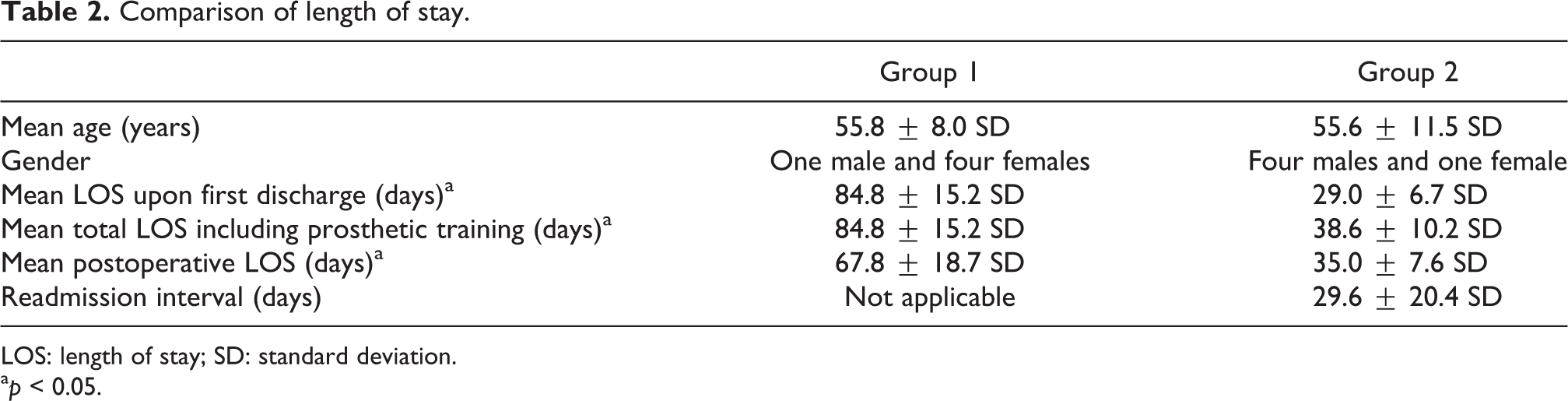
LOS: length of stay; SD: standard deviation.
a p < 0.05.
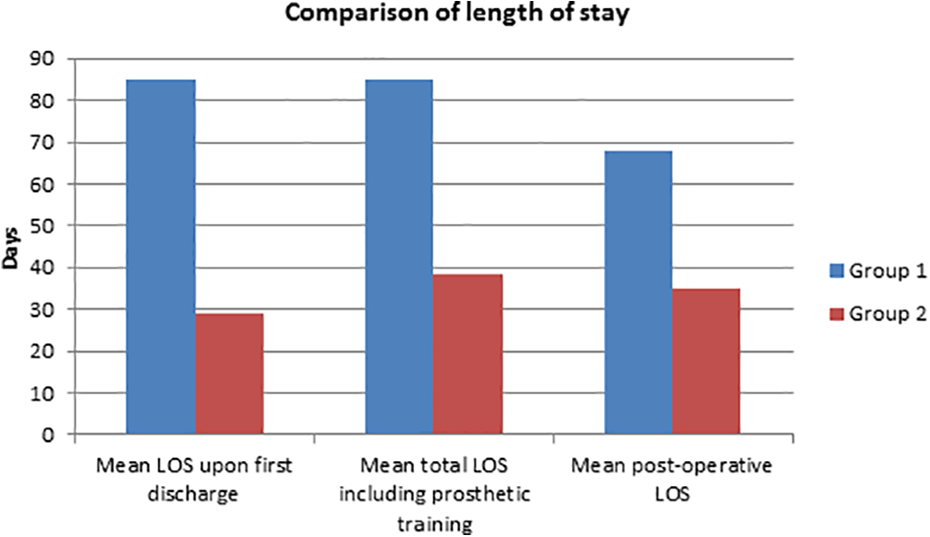
Comparison of length of stay in bar chart.
Concerning functional outcomes, although K level after 1 month of use of prosthesis was similar in two groups, more patients in group 2 were able to walk unaided and perform daily walking for more than 2 h (Table 3). Moreover, complication of sore within 3 months was less frequent in group 2.
Functional outcomes and complications.
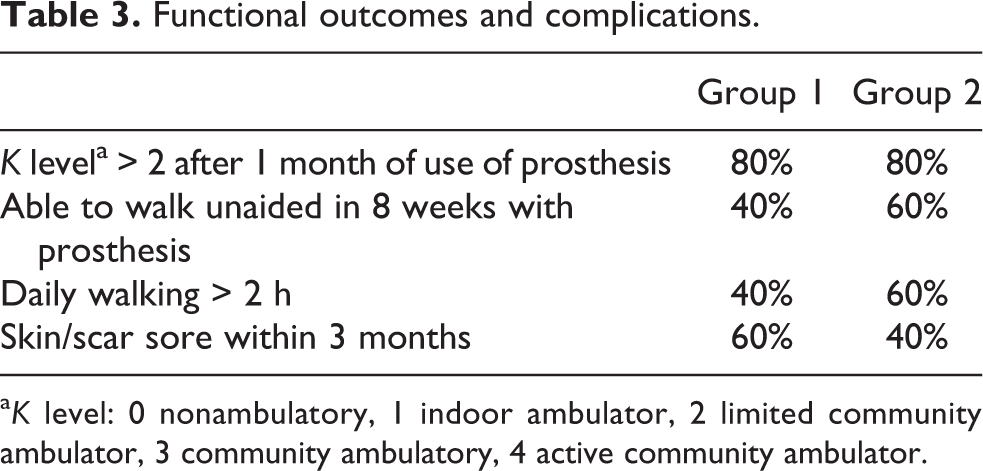
a K level: 0 nonambulatory, 1 indoor ambulator, 2 limited community ambulator, 3 community ambulatory, 4 active community ambulator.
Discussion
There were only limited publications in the literature reviewing outcomes of major LEA in Hong Kong. Preceding our study, there were two significant articles published in different decades. Chan et al. reviewed the amputees from 1960s to 1980s in one of the major rehabilitation centers. 1 Although infective, vascular and diabetic causes accounted for 60% of LEA, as much as 26% was secondary to trauma. The rate of transtibial amputation was much higher than transfemoral amputation (36.9% vs. 16.3%). By 1990s, trauma leading to LEA has been reduced to 7.1% in one of the major trauma centers. 2 This reflected the changes in socioeconomic activities and further regulations in road and occupational safeties in our locality throughout the decades. Nowadays, the etiology for major LEA in Hong Kong follows the pattern in Western populations due to rising life expectancy and prevalence of diabetes mellitus and peripheral vascular disease. 3,4
Metastasis distal to the knee is defined as acrometastasis. 5 It is believed that tumor cell from subdiaphragmatic viscera embolizes retrogradely through the valveless Batson’s plexuses into iliofemoral venous system. Prognosis, in general, is poor and orthopedic treatment aims to alleviate pain and improve mobility and functional independence. 6 One exception would be solitary bone metastasis of renal cell carcinoma, which shall be treated with curative intent. Wide resection (including amputation) of solitary bone metastasis combined with nephrectomy was reported to achieve 100% survival rate. 7 Although some studies did not show any survival advantage when compared with intralesional resection and stabilization, wide resection is superior in minimizing local disease progression and complications. 8
The prosthetic fitting rate in our study was higher than the local data two decades ago, both in transtibial (55% vs. 30.8%) and transfemoral amputations (14% vs. 8.8%). 2 There are several predictors of walking ability following major LEA, which include age at amputation, level of amputation, preamputation mobility and independence of activities of daily living, one-leg balance on the unaffected limb, cognitive impairment, and severe comorbidity. 9 –11 Stump problems and delay in rehabilitation are predictors of poor outcomes. We hypothesized that the improved fitting rate in our study was due to the ongoing improvement in perioperative care, prosthesis designs, and most importantly, barrier-free facilities, which make the society more accessible to amputees than two decades ago. Nowadays, elderly amputees use prosthesis for indoor and short distance outdoor walking and power wheelchair for long distance travel.
Two-staged admission pathway for new transtibial amputees aims to shorten LOS and reduce hospital operational cost. When counting the cost per patient day for general inpatient services in public hospitals, which exceeds $5000 Hong Kong dollars by 2017, this new pathway saved more than $160,000 on average for each new amputee. 12 In addition to similar rehabilitation outcomes and residual limb health, amputees can also return to home-based environment and identify their functional barrier in early stage. This new pathway relies on multidisciplinary approach for close monitoring of the stump’s condition and assessing the psychosocial aspect of amputees. Perioperative care education to amputees and their carers play a keystone to success. Once amputees received a clear picture of their rehabilitation phases, their rapport with clinical staff and participation in prosthetic training would also be enhanced.
There were several limitations in our study. It was a retrospective study but not a prospective study. Concerning etiology, many patients with the peripheral vascular disease also had diabetes mellitus as they share similar cardiovascular risk factors and the underlying causes were based on operative diagnoses made by different surgeons. There might be selection bias in allocating patients with better premorbid function and social support into two-staged admission pathway. However, it was our purpose to discharge more able amputees early to their usual environment. There were individualized psychosocial factors, such as motivation for rehabilitation, anxiety to return home, availability of carer at home, and environmental barriers, such as living in nonlift landing apartment or village house, that affected postoperative LOS and prosthesis use in community.
LOS for new transtibial amputees can be greatly reduced by the two-staged admission pathway to minimize hospital operational cost. Moreover, functional outcomes in the two-staged admission pathway were compatible, if not better than the traditional pathway. It serves as a good example to transform rehabilitation service from inpatient-based to outpatient-based.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.