
Abstract
Background:
In the assessment of three-dimensional features of adolescent idiopathic scoliosis, the plane of maximum curvature was compared with the coronal Cobb angle.
Objectives:
To investigate the intrarater reliability, variability, and difference of the prone plane of maximum curvature measurements taken from computed tomography using the constrained and unconstrained Cobb methods; to assess the difference and correlation between the prone plane of maximum curvature measurements obtained using the constrained and unconstrained Cobb methods; and to examine differences and correlation between the prone plane of maximum curvature Cobb angle and coronal Cobb angle measurements.
Study design:
Retrospective study.
Methods:
Records of 29 subjects with adolescent idiopathic scoliosis aged 15.8 ± 3.5 years were reviewed (25 thoracic and 24 thoracolumbar/lumbar curves). An experienced rater measured the plane of maximum curvature using the constrained and unconstrained Cobb methods, and the coronal Cobb angles using the conventional Cobb method on computed tomography images 3 times each with 1-week interval. The intraclass correlation coefficient (2,1), Pearson correlation coefficient (r), one-way repeated measures analysis of variance, and paired t test were applied for various analyses.
Results:
The intraclass correlation coefficients for all intrarater reliability assessments were greater than 0.87. The plane of maximum curvature measurements of the two Cobb methods were excellently correlated (r ⩾ 0.97) with no significant difference (P > 0.05). The mean plane of maximum curvature Cobb angle was moderately correlated with (r > 0.72) but significantly greater (P < 0.001) than the mean coronal Cobb angle.
Conclusion:
The plane of maximum curvature measurements obtained from computed tomography were found to be reliable while the plane of maximum curvature measurements of the two Cobb methods were comparable. The mean plane of maximum curvature Cobb angle was moderately correlated with but significantly greater than the mean coronal Cobb angle.
Clinical relevance
The plane of maximum curvature measurements taken from computed tomography was found to be reliable, hence it could be used as a supplement to the coronal Cobb angle in the assessment and management of adolescent idiopathic scoliosis. With technological advancement, the radiation dose of computed tomography can be further reduced to a safer level for a broader range of cases.
Background
Adolescent idiopathic scoliosis (AIS) is a complex three-dimensional (3D) spinal deformity characterized by lateral curvature of at least 10° and axial vertebral rotation (AVR). 1 Coronal Cobb angle (coronal-Cobb) measured on the posteroanterior (PA) radiograph is an important parameter for the assessment of AIS; however, it may underestimate the severity of spinal deformity and may not fully reflect curve types.2–5 The plane of maximum curvature (PMC) may be a promising descriptor for the 3D assessment of AIS, 5 and is increasingly valued in spinal surgery. 6 PMC is a vertical plane located between the sagittal and coronal planes that presents the maximum projected spinal curvature. 1 Parameters include the maximum Cobb angle measured in the PMC (PMC-Cobb) and the orientation of the PMC (PMC-orientation, the angle between the PMC and sagittal plane). The PMC (PMC-Cobb and PMC-orientation) may play an important role in the assessment and management of AIS. As reported in previous studies, the PMC appeared to be more informative in describing the 3D features of the scoliotic spine,5,7,8 and may be more effective in reflecting the 3D correction of treatment.9,10 Furthermore, the PMC is superior to the coronal-Cobb in differentiating curve types: as reported by Sangole et al. 4 and Labelle et al. 5 the coronal-Cobb-based curve type can be further split into different sub-types using the PMC.
Currently, several techniques allow PMC measurements. Biplanar radiography7,11 (e.g. EOS imaging system) and 3D ultrasound imaging 12 can be used to assess the PMC. However, the reliability and validity of PMC measurements using these techniques need to be investigated before clinical application. Computed tomography (CT) is a common method for 3D assessment of severe AIS in clinical practice as it allows the assessment of spinal deformity in both the coronal, sagittal and transverse planes with the same image-set. 13 CT has been used to evaluate coronal curvature with a small error of measurement (<2.7°), 13 and AVR14,15 with high reliability (intraclass correlation coefficient = 0.95) 14 . It has also been used to investigate the asymmetry of vertebral body 16 and pedicles,16,17 as well as anterior–posterior length 18 of the spinal column. However, it has never been used to measure the PMC. If the CT method can be demonstrated as reliable, it could facilitate clinical application of the PMC measurement and may serve as a supplement to coronal-Cobb measurement in the assessment and management of AIS.
Because of the complicated global, regional, and local deformity of AIS,1,16–18 it is unknown if the end-vertebrae most tilted in the coronal plane would also be most tilted in any other vertical planes (different from the coronal plane). Thus, constrained and unconstrained Cobb methods were proposed. As shown in Figure 1, the constrained Cobb method measures the Cobb angle in other vertical planes but with the upper and lower end-vertebrae constrained to the upper and lower end-vertebrae pre-selected from the coronal plane;1,7,19 while the unconstrained Cobb method measures the Cobb angle in other vertical planes with the upper and lower end-vertebrae determined from that particular vertical plane. 7 In the constrained Cobb method, there is no need to select the end-vertebrae in other vertical planes, thus, it would be less time-consuming and appear to be used more frequently for determining the PMC when using the other techniques (e.g. biplanar radiology).7,11,19 Although possible discrepancy of the PMC measurement between these two methods has been reported in some studies,7,19 their comparability has not yet been specifically investigated.
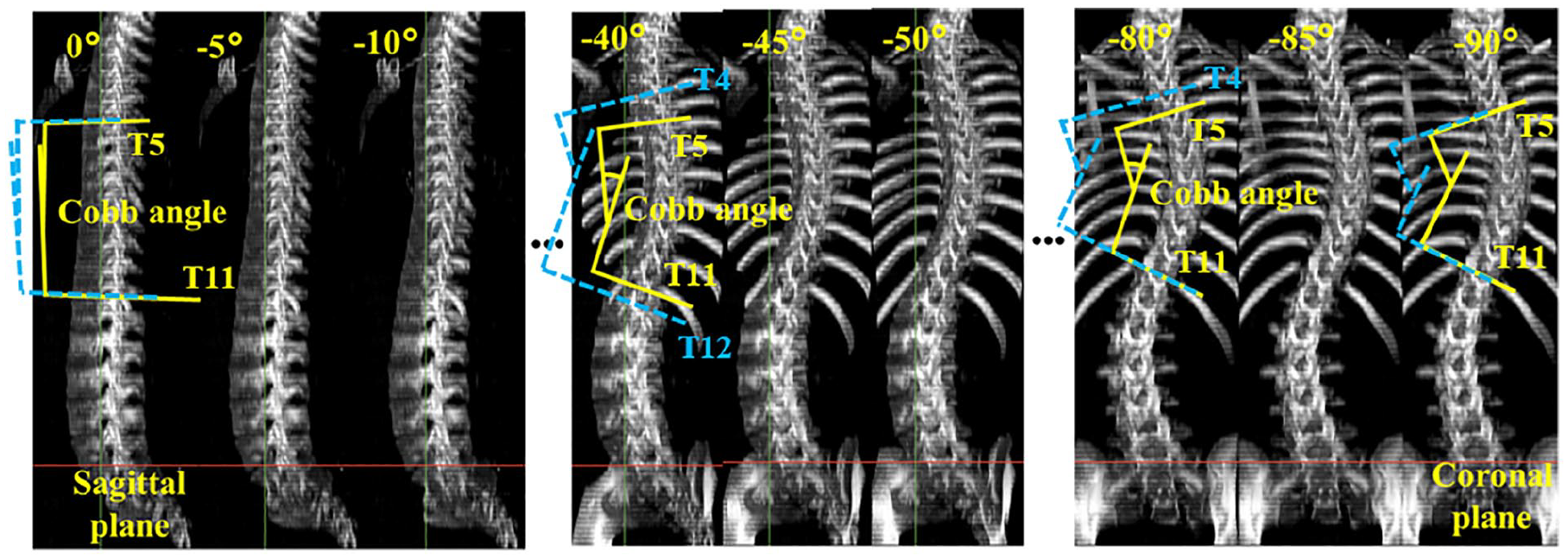
Constrained (solid lines) and unconstrained (dashed lines) Cobb methods (the rotated planes (n = 19) were generated by rotating a vertical plane 90° around the vertical axis from the sagittal to coronal plane with an increment of 5°; counterclockwise rotation was for a right thoracic curve and recorded as negative (−)).
It may improve understanding of the 3D features of spinal deformities to assess the potential difference and correlation of AIS parameters obtained from the images taken in different positions. The dependent relationships between the PMC (PMC-Cobb and PMC-orientation) and coronal/sagittal-Cobb have been assessed in the standing position.4,15,20 The PMC-Cobb was notably greater than the corresponding coronal-Cobb in the standing position;2,3,7–10,21 however, the difference and correlation between the PMC-Cobb and coronal-Cobb were not investigated in a recumbent (prone/supine) position.
Thus, the objectives of this study were to (1) investigate the intrarater reliability, variability, and difference of the PMC measurements taken from CT using the constrained and unconstrained Cobb methods in the prone position; (2) assess the differences and correlations between the PMC measurements obtained using the constrained and unconstrained Cobb methods in the prone position; and (3) examine differences and correlations between the PMC-Cobb and coronal-Cobb measurements in the prone position.
Methods
Subjects
This study investigators retrospectively reviewed the 3D images of the scoliotic spine taken from CT. Ethical approval for this study was granted by the Human Subjects Ethics Sub-committee of The Hong Kong Polytechnic University. Subjects were selected from the database of a local scoliotic clinic according to the following inclusion criteria: (1) diagnosed with AIS; (2) age: ⩾10 years; and (3) underwent CT of the whole spine. Subjects were excluded if they had received surgical treatment of the spine before CT scan or were diagnosed with other conditions that might affect spinal morphology.
All subjects were imaged in the prone position with a CT scanner (LightSpeed®16, GE Healthcare, USA, with parameters set at 400 mA s, 120 kVp, 0.625 mm thicknesses, and 5 mm gap between slices) between 2015 and 2017 for the purpose of their own clinical examinations.
Acquisition of PMC measurements
All CT slices of the whole spine (Dicom format) were visualized three-dimensionally using an open-source image processing software named 3DSlicer (version 4.8.1, 3DSlicer Platform: www.slicer.org). As shown in Figure 2, a vertical plane, upon which the scoliotic spine was projected, was rotated 90° around the z-axis of the global axis system. 22 According to the location of each curve type in this axis system, the vertical plane was rotated from 0° to −90° for right thoracic curves (RTs); 0° to + 90° for left thoracic curves (LTs); −180° to −270° for left thoracolumbar/lumbar curves (LTLs/LLs) and + 180° to + 270° for right thoracolumbar/lumbar curves (RTLs/RLs) in increments of 5°. The Cobb angle of a spinal curve was measured separately in each rotated plane (n = 19) using the constrained and unconstrained Cobb methods (Figure 1) with Digimizer image analysis software (version 4.3.5, MedCalc Software bvba, Belgium), and was recorded as an absolute value. The maximum Cobb angle was then determined, and the rotated plane showing the maximum Cobb angle was the PMC. The determined maximum Cobb angle was the PMC-Cobb, and the orientation of that rotated plane was considered the PMC-orientation. Additionally, the coronal-Cobb was measured on the CT coronal image using the conventional Cobb method. 1
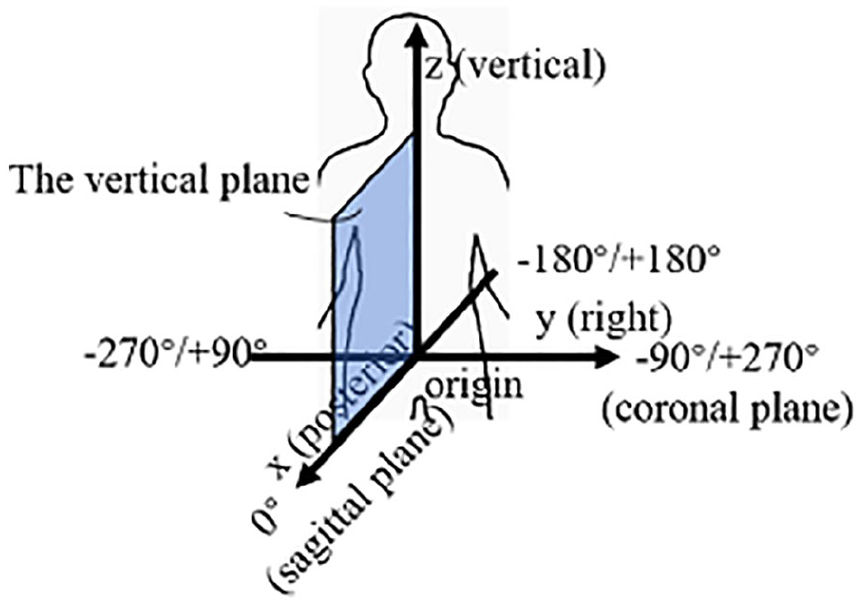
Global axis system in the human body. The x and y axes pointing posteriorly and to the right side represent the sagittal and coronal planes, respectively. The orientation of the vertical plane was referred to separately as negative (−) for counter-clockwise rotation and positive (+) for clockwise rotation, being at 0°/±180° or ±90°/±270° when overlapping with the sagittal or coronal planes, respectively.
A rater with 3+ years of experience in scoliosis clinical research repeated the PMC (PMC-Cobb and PMC-orientation) measurements 3 times using the constrained and unconstrained Cobb methods, with a 1-week interval between each time to reduce recall bias. The coronal-Cobb was measured repeatedly using the same protocol. The average of the repeated measurements, including the PMC (PMC-Cobb and PMC-orientation) and coronal-Cobb, was used for the subsequent analyses.
Statistical analyses
Statistical analyses were performed using SPSS (version 21; IBM, Chicago, IL, USA) with the critical alpha set at 0.05. For the first objective, the intraclass correlation coefficient (ICC (2,1) two-way random model and absolute agreement) with 95% confidence interval was used. The strength of reliability was evaluated via the criteria proposed by Currier: 23 very reliable (ICC = 0.8–1.0), moderately reliable (ICC = 0.60–0.79), and questionably reliable (ICC < 0.60). Besides, the one-way repeated measures analysis of variance (ANOVA), mean absolute difference (MAD), standard deviation (SD), and standard error of measurement (SEM) were evaluated. For the second objective, the paired t test (two-tailed), MAD, SD, SEM, and Pearson correlation coefficients (r) were evaluated. The strength of each correlation was categorized using the following criteria: very good to excellent (r = 0.75–1.00), moderate to good (r = 0.50–0.75), and poor correlation (r = 0.25–0.50). 24 For the third objective, the paired t test (two-tailed), MAD, SD, and Pearson correlation coefficients (r) were evaluated.
Results
Twenty-nine subjects (27 females and 2 males; aged 15.8 ± 3.5 years with a range of 12–24 years) were selected from the database for this study. Forty-nine curves from these subjects were analyzed, including 25 RTs (mean prone coronal-Cobb = 45.9°± 12.2° with a range of 26.2°–71.1°) and 24 LTLs/LLs (mean prone coronal-Cobb = 31.8°± 11.8° with a range of 16.4°–54.2°).
Intrarater reliability assessment of PMC measurements
As shown in Table 1, for both the RTs and LTL/LLs groups, the PMC (PMC-Cobb and PMC-orientation) measurements of the constrained and unconstrained Cobb methods were very reliable (ICC = 0.92–0.98 for the PMC-Cobb, and ICC = 0.87–0.94 for the PMC-orientation). Moreover, the intrarater variability of the PMC measurements between the two methods was small, with MAD = 0.3°, SD = 1.5°–1.8° and SEM = 0.3°–0.4° for the PMC-Cobb, and MAD = 0.4°–1.5°, SD = 5.4°–7.3°, and SEM = 1.1°–1.5° for the PMC-orientation. No significant intrarater differences were found among all the repeated PMC measurements (P > 0.05 for the PMC-Cobb and P > 0.05 for the PMC-orientation).
Intrarater reliability of PMC (PMC-Cobb and PMC-orientation) measurements.
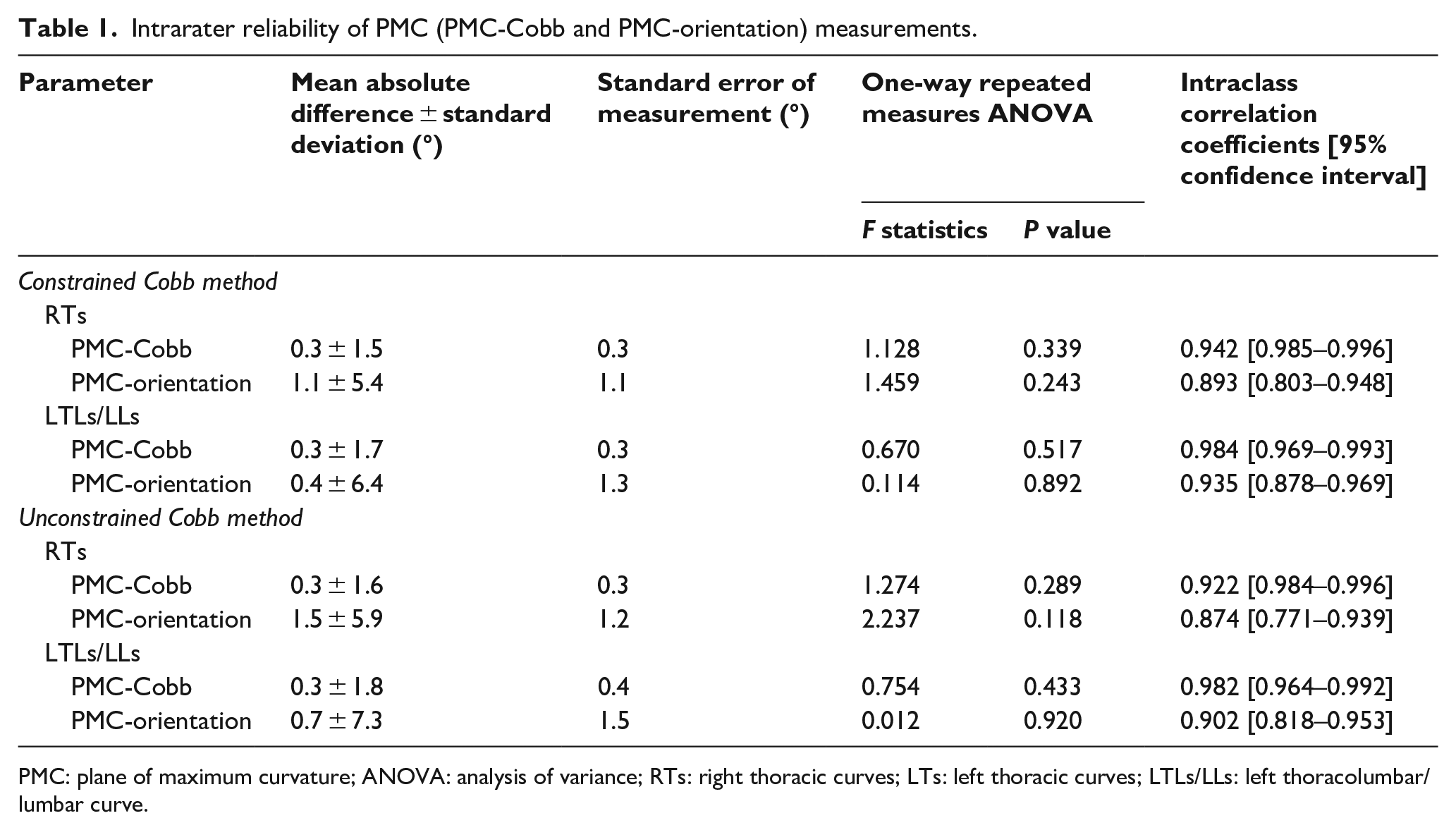
PMC: plane of maximum curvature; ANOVA: analysis of variance; RTs: right thoracic curves; LTs: left thoracic curves; LTLs/LLs: left thoracolumbar/lumbar curve.
Comparability assessment of the constrained and unconstrained Cobb methods
In the RTs and LTL/LLs groups (Table 2), differences between the PMC measurements obtained using the constrained and unconstrained Cobb methods were small, with MAD = 0.0°–0.6°, SD = 0.6°–3.0°, and SEM = 0.1°–0.6° for the PMC-Cobb, and MAD = 0.1°–0.6°, SD = 1.4°–2.2°, and SEM = 0.3°–0.4° for the PMC-orientation. None of these differences were significant (P > 0.05 for the PMC-Cobb and P > 0.05 for the PMC-orientation). Furthermore, excellent correlations were observed between the PMC measurements of these two Cobb methods (r = 0.97–0.99 for the PMC-Cobb and r = 0.98–0.99 for the PMC-orientation).
Differences and correlations between the PMC (PMC-Cobb and PMC-orientation) measurements obtained using the CT constrained and unconstrained Cobb methods.
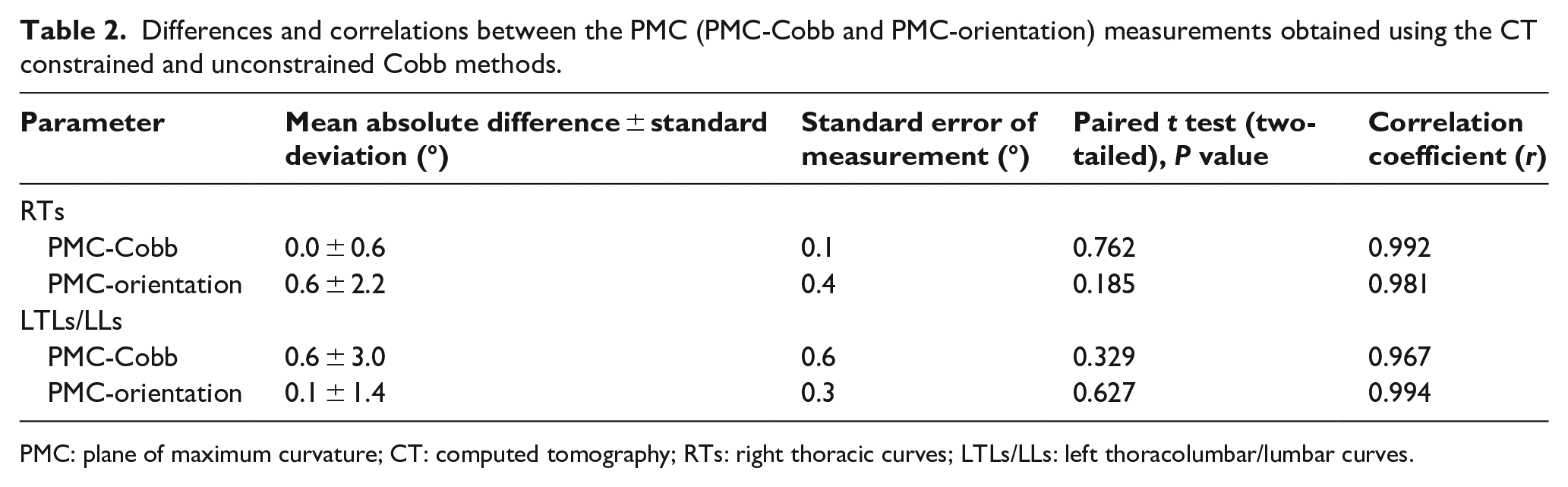
PMC: plane of maximum curvature; CT: computed tomography; RTs: right thoracic curves; LTLs/LLs: left thoracolumbar/lumbar curves.
Difference and correlation assessment of PMC-Cobb and coronal-Cobb measurements
In the RTs and LTL/LLs groups (Table 3), the PMC-Cobb acquired using the two Cobb methods were significantly greater than the corresponding coronal-Cobb (MAD = 4.5°–5.4°, SD = 4.2°–4.9°, P < 0.001). The correlations between the measurements of these two parameters was excellent in the RTs group (r = 0.94), and moderate to good in the LTL/LLs group (r = 0.72–0.75).
Differences and correlations between the PMC-Cobb and coronal-Cobb measurements.
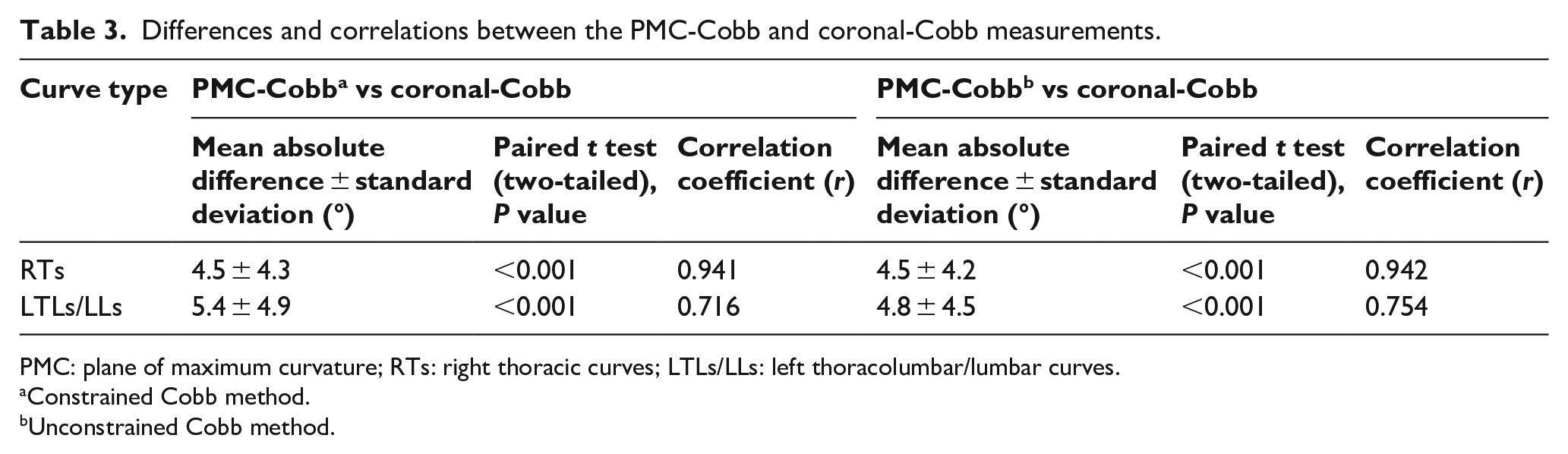
PMC: plane of maximum curvature; RTs: right thoracic curves; LTLs/LLs: left thoracolumbar/lumbar curves.
Constrained Cobb method.
Unconstrained Cobb method.
Discussion
This is the first study to investigate the intrarater reliability of PMC measurements acquired from CT using the constrained and unconstrained Cobb methods, and the comparability of PMC measurements from two methods in the prone position. The differences and correlations between the PMC-Cobb and coronal-Cobb measurements were also analyzed. The main findings of this study were that (1) the PMC measurements (PMC-Cobb and PMC-orientation) taken from CT using the two Cobb methods in the prone position were very reliable; (2) no significant differences but excellent correlations between the PMC measurements of the two Cobb methods in the prone position were observed; and (3) the PMC-Cobb measurements were excellently correlated with, and significantly greater than, the corresponding coronal-Cobb measurements in the prone position.
In the RTs and LTL/LLs groups, the PMC measurements of the constrained and unconstrained Cobb methods were very reliable and showed small intrarater variability (ICC > 0.92 and MAD ⩽ 0.3° for the PMC-Cobb; and ICC > 0.87 and MAD ⩽ 1.5° for the PMC-orientation). The intrarater MAD was much smaller than the clinically acceptable threshold (5°). 25 The intrarater reliability of PMC-Cobb measurements acquired using the two methods was similar to that obtained using 3D ultrasound (ICC > 0.93). 12 These results suggest that the constrained and unconstrained Cobb methods could be used to assess the PMC reliably from CT. Although the CTs used in this study were generally taken from patients with relatively severe AIS (due to radiation exposure concern, patients with mild to moderate AIS were not scanned), it is believed that, with technological advancement, the radiation dose of CT systems can be further reduced to a safer level. If low-dose CT systems became widely available, the two Cobb methods might allow the PMC measurement to be used in a broader range of cases. Furthermore, biplanar radiography may be an option for 3D reconstruction of the spine, for which the constrained or unconstrained Cobb method might also be used for the PMC measurement.
The PMC (PMC-Cobb and PMC-orientation) measurements of the constrained and unconstrained Cobb methods were comparable in both the RTs and LTL/LLs groups in the prone position (MAD ⩽ 0.6°, P > 0.05, r ⩾ 0.97). This indicated that the PMC measurements obtained using the constrained Cobb method reflected the maximum spinal deformity as compared to that acquired using the unconstrained Cobb method. Thus, using the constrained Cobb method in assessing PMC is suggested since it is less time-consuming and more user-friendly in comparison with the unconstrained Cobb method. Also, this study may provide scientific evidence to support the use of the constrained Cobb method in assessing PMC.
The PMC-Cobb overestimated the curve magnitude as compared to coronal-Cobb (MAD = 4.5°–5.4°, P < 0.001). Similar results were reported in previous studies.2,3,7–10,21 In comparison to coronal-Cobb, the PMC could provide information for both the maximum curve magnitude (PMC-Cobb) and the degree of curve segment being rotated toward the coronal plane (PMC-orientation). It has been applied to 3D classification of AIS. Sangole et al.4,5 pointed out that two curves with the same coronal-Cobb could present remarkably distinct maximum spinal curvature (PMC-Cobb) and sagittal thoracic kyphosis. Moreover, Labelle et al. 5 reported that a curve type classified by the Lenke system could be further split into different curve sub-types based on the PMC-orientation. This should be considered when making clinical decisions since different curve sub-types may need different treatment strategies. Thus, it is worthwhile to explore the application of PMC to orthotic decision-making in future studies. PMC has been used for evaluating 3D correction provided by orthotic treatments.9,10 In two studies, significant correction in the coronal-Cobb and PMC-Cobb were found.9,10 However, the PMC-orientation was significantly increased instead of being reduced as expected,9,10 indicating that the curve segment rotated toward the coronal plane even more after wearing the orthosis. In a scoliotic spine, the coronal curve may result from a curve segment (thoracic/thoracolumbar/lumbar segment) rotated from the sagittal plane toward the coronal plane with or without alteration in physiological curvature. The goal of orthotic intervention is to push the rotated curve segment back to the sagittal plane (coronal-Cobb = 0°) while keeping a normal spinal profile in the sagittal plane (physiological curvature). Thus, only emphasizing the coronal-Cobb correction but ignoring the changes in PMC-orientation when evaluating the treatment correction, the physiological curvature of the thoracic/thoracolumbar/lumbar region may not be maintained. This indicates that the coronal-Cobb alone may not be comprehensive enough for evaluating the “true” correction of treatment and reflecting the “real” condition of AIS. Therefore, it might be necessary to employ the corresponding PMC (PMC-Cobb and PMC-orientation) measurements as a method to supplement the coronal-Cobb measurements in orthotic management of AIS.
There are several limitations to this study. As only one rater was involved in measurement of the PMC, the study lacks interrater reliability. It should also be noted that this retrospective study did not allow us to check whether all the patients maintained a standardized position when taking the CT. The sample size, range of curve magnitude and curve pattern should be increased for more conclusive results.
Conclusion
The PMC measurements (PMC-Cobb and PMC-orientation) taken from the CT were found to have intra-rater reliability, and the PMC measurements of the constrained and unconstrained Cobb methods were comparable. The difference and correlation between the PMC-Cobb and coronal-Cobb measurements in the prone position demonstrated the importance of using PMC measurements to supplement coronal-Cobb measurements in the assessment and management of AIS.
Footnotes
Acknowledgements
The CT images were obtained from the Department of Imaging and Interventional Radiology, The Prince of Wales Hospital, Chinese University of Hong Kong.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.