
Abstract
Background and Aim:
During post-amputation recovery or rapid body mass change, residual limb volume can change quickly, requiring frequent adjustments or replacement of the socket to maintain fit. The aim of this pilot test was to evaluate the feasibility of using a three-dimensional-printed insert to extend the service life of a prosthetic socket after substantial residual limb volume loss.
Technique:
One research subject with a well-fitting transtibial prosthetic socket had an oversized socket fabricated to simulate substantial limb volume loss. The digital shapes of the oversized and well-fitting sockets were used to create a three-dimensional-printed insert to restore fit.
Discussion:
Two-minute walk test distance decreased when using the oversized socket without the insert, but not when using the socket with the insert. Socket comfort score was 8+ under all conditions. These results suggest that three-dimensional-printed inserts may be an effective method of extending the service life of prosthetic sockets when rapid limb volume loss occurs.
Clinical relevance
Three-dimensional (3D) printing gives prosthetists a new tool to manage large volume changes without refabricating entire sockets. Sockets can be fabricated in anticipation of volume gain/loss, using replaceable 3D-printed inserts to maintain fit and comfort.
Background and Aim
Traditional prosthetic sockets have a rigid, fixed volume but the human body is a dynamic system that is always changing. Prosthetic sockets are fabricated with the expectation of some limited limb volume changes, both increases and decreases. Minor fluctuation in limb volume throughout the day and from day to day are traditionally managed by adding or removing residual limb socks or periodically doffing the prosthesis.1–4 Limb volume changes due to long-term trends such as slow physiological changes (e.g. muscle atrophy, steady body mass gain/loss) may result in poor fit due to excessive limb volume loss. 4 The Amputee Coalition of America recommends keeping weight (body mass) loss or gain to within 2% of body weight (mass) to preserve socket fit. 5 Large volume changes as the residual limb matures (the first 6 months post-amputation and at a slower rate up to 18 months post-amputation)6–8 require frequent new prosthetic sockets or socket alterations to improve fit, 4 leading to an increased cost of care. Some prosthetic socket designs, (such as the Revo Fit socket, by RevoLabs, Salt Lake City, UT) are intended to accommodate some volume change, but the fabrication challenges of such systems remain a barrier for clinical application to patients with rapidly changing limb volume, such as during the post-amputation recovery phase, despite recent evidence of the benefits for patients.9,10
The rise of three-dimensional (3D) printing in the prosthetics industry has enabled many novel approaches to traditional tasks and novel solutions to problems for which traditional technologies fail to provide a solution. 11 The aim of this study was to pilot test the effectiveness and feasibility of a novel approach to limb volume management based on 3D printing technology to extend the service life of prosthetic sockets when substantial volume changes have occurred or are anticipated.
The traditional approach to socket fit management presumes use of residuum socks to manage short-term minor volume fluctuations and periodic re-fabrication of new sockets when the number of sock ply exceeds a manageable level. “15 ply” was used as the threshold for this study, although research has shown that the number of sock ply worn is not a clear indication of the amount of volume accommodation needed. 12
When the prosthesis user is using an overly large volume of socks, a new socket would be fabricated using traditional methods.6,13 The prosthetist would follow the traditional process of casting or scanning the patient’s limb, rectifying (whether hand-modifying a plaster positive model or electronically modifying a digital positive model), and then fabricating a check socket.
Technique
The alternative approach to volume management, currently being studied, replaces the traditional socket fabrication process with a 3D-printed socket insert. The original socket is first internally scanned, or a scan may already exist if this is how the original socket was fabricated. The patient’s limb would then be cast or scanned again, and the model rectified to generate a well-fitting check socket. The original socket positive model and the new socket positive model would be combined to generate a custom 3D-printed insert that converts the old oversized socket interior shape into the new correctly fitting interior shape.
Pilot testing the use of inserts for managing volume change was performed with a single subject. Human subject testing was overseen by the Minneapolis VA Health Care System’s Institutional Review Board (Study 4727-B) and occurred in the prosthetics clinic. Written informed consent was obtained from the subject prior to participation.
For purposes of the test, an experienced (~10 years) K3 prosthesis user’s current well-fitting socket was used as the traditional control and an oversized socket was fabricated to simulate the case of decreased residual limb volume. The subject normally used 5-ply of residual limb socks, so the oversized socket was expanded globally by “10 ply” using Omega software (WillowWood Co., Mt. Sterling, OH). The oversized socket and current well-fitting socket were digitized using a Provel D2 Digitizer (Provel Inc., Cle Elum, WA) such that there was a digital model of the “ill-fitting, old socket” (simulated oversized socket) interior and another of the “well-fitting, new socket” (subject’s current socket) interior. The two digital models were converted into an insert which was 3D printed on a fused filament fabrication printer (Raise3D, Irvine, CA) using a 95 Shore A thermoplastic polyurethane (TPU). The subject returned to the clinic and performed a 2-min walk test (2MWT) and a post-2MWT socket comfort score (SCS) 14 under three test conditions:
Baseline data using the subject’s usual socket.
The subject’s usual socket was replaced with the oversized socket with an insert and the measures were repeated.
The insert was removed and the measures repeated again.
The number of sock ply necessary to achieve satisfactory fit was recorded (Table 1). After all three test conditions were completed, the subject’s prosthesis was restored to its usual condition.
Number of sock ply used to achieve satisfactory fit, distance (in meters) walked during the 2-min walk test (2MWT), and socket comfort score (SCS) under the three socket conditions.
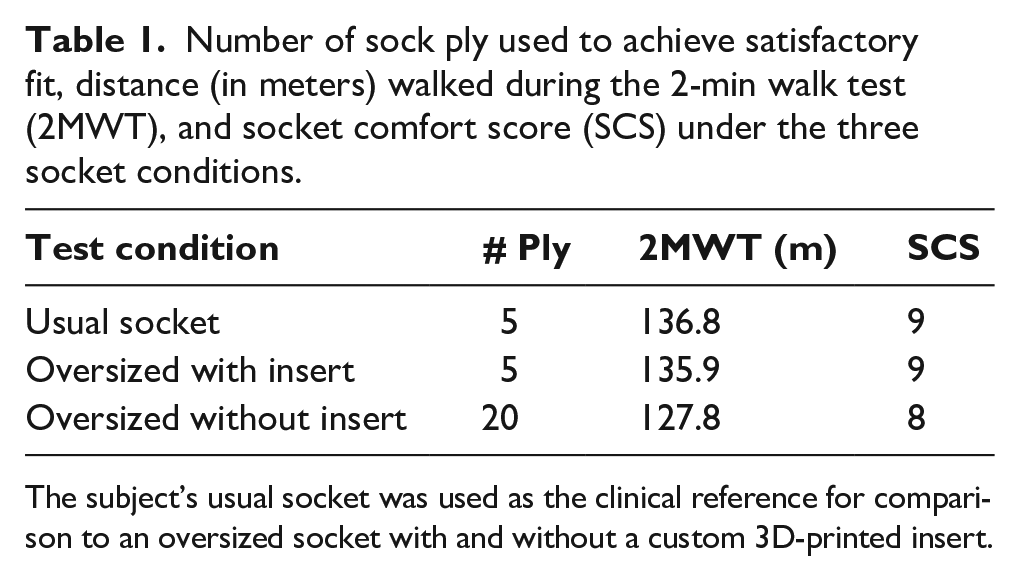
The subject’s usual socket was used as the clinical reference for comparison to an oversized socket with and without a custom 3D-printed insert.
Discussion
This single-subject pilot study demonstrated feasibility of the method and prepares for a future clinical study that would entail more quantitative measures in a larger population, such as gait analysis or socket interface pressures. The subject felt that all sockets were comfortable (SCS 8+). The subject used the same number of socks for his usual socket and oversized socket with insert (one 5-ply sock) but had to add three more 5-ply socks for the oversized socket without insert, bringing his total to 20 ply. The subject’s walking distance when using the oversized socket with the insert (135.9 m) was 0.6% less than when using his usual socket (136.8 m). The walking distance when using the oversized socket without the insert (127.8 m) was 6.6% less than when using his usual socket. A 5.5 m difference is considered clinically meaningful 15 and the change was 9.0 m from the subject’s current socket and 8.1 m from the oversized socket without insert, indicating a clinically meaningful difference between the oversized socket and both correctly fitting sockets.
When trying the oversized socket with the insert the subject stated “I feel level” meaning that he perceived no change in leg length without the prosthetist adjusting distal components. With regard to the fit and comfort of the oversized socket with the insert, he stated “I think it is just as good as my existing socket.” Due to a recent snowfall, the subject had worn boots and stated that under all conditions “I feel ever so slightly like I’m being pulled forward” while qualifying that statement with “I am only perceiving a difference in my footwear, not the socket.” While wearing the oversized socket without the insert, the subject stated “I couldn’t feel a heat difference with that short walk, but after 30 minutes [with the additional socks] it would probably be hotter [than my current socket].” In response to follow-up questions, the subject clarified that he used to feel excess heat in his socket after extended activity when wearing a large number of socks to accommodate limb volume changes. Use of an insert may similarly result in the sensation of excess heat buildup in an oversized socket.
One limitation of this pilot test was that the limb volume was globally increased to simulate a reduction of limb volume. Natural limb volume changes are not uniform and could result in areas with little volume change while other areas experience dramatic volume change. The insert has a minimum wall thickness of approximately 1 mm, but print quality and structural integrity are better at wall thicknesses >2 mm. These factors should be accounted for in future clinical testing and applications.
This pilot test suggests that the use of 3D-printed inserts to correct substantial residual limb volume loss may provide equivalent fit and function to fabricating a new socket since it performed similarly to an existing well-fitting socket. The oversized socket with insert allowed the participant to walk further than when using the oversized socket with a large number of socks. Other potential applications of this approach could include intentionally creating oversized sockets with inserts for individuals expected to gain volume or, in the case of pediatric sockets, expected to grow both in length and circumference.
Key Points
A 3D-printed insert can fill excess volume in a serviceable, but oversized, prosthetic socket to restore better fit.
Using an insert may provide equivalent fit and comfort to a well-fitting traditional socket.
Using an insert may restore functional mobility to the equivalent of a new socket compared to the reduced mobility of using many ply of socks in an oversized socket.
The technique may also be used to prepare for anticipated volume gain by fabricating an oversized socket initially worn with an insert and then creating new inserts as the patient’s limb gains volume.
Footnotes
Authors’ note
The views, opinions, and interpretations expressed in this article are those of the authors and do not represent the views of the Department of Veterans Affairs, the Defense Logistics Agency, the Department of Defense, or the United States Government.
Author contributions
E.N. led the writing of the manuscript. All other authors contributed equally, providing critical review and editing of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.H. is owner and president of Reify LLC and could stand to benefit should this approach be successful.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Defense Logistics Agency under Small Business Innovations Research contract numbers SP4701-16-C-0027 and SP4701-17C-0037. It was also partially supported by Reify, LLC, and Extremiti3D, LLC (a Reify subsidiary).