
Abstract
Background:
Prosthetic knee joint function is important in the rehabilitation of individuals with transfemoral amputation.
Objectives:
The objective of this study was to assess the gait patterns associated with two types of mechanical stance control prosthetic knee joints—weight-activated braking knee and automatic stance-phase lock knee. It was hypothesized that biomechanical differences exist between the two knee types, including a prolonged swing-phase duration and exaggerated pelvic movements for the weight-activated braking knee during gait.
Study design:
Prospective crossover study.
Methods:
Spatiotemporal, kinematic, and kinetic parameters were obtained via instrumented gait analysis for 10 young adults with a unilateral transfemoral amputation. Discrete gait parameters were extracted based on their magnitudes and timing.
Results:
A 1.01% ± 1.14% longer swing-phase was found for the weight-activated braking knee (p < 0.05). The prosthetic ankle push-off also occurred earlier in the gait cycle for the weight-activated braking knee. Anterior pelvic tilt was 3.3 ± 3.0 degrees greater for the weight-activated braking knee. This range of motion was also higher (p < 0.05) and associated with greater hip flexion angles.
Conclusions:
Stance control affects biomechanics primarily in the early and late stance associated with prosthetic limb loading and unloading. The prolonged swing-phase time for the weight-activated braking knee may be associated with the need for knee unloading to initiate knee flexion during gait. The differences in pelvic tilt may be related to knee stability and possibly the different knee joint stance control mechanisms.
Clinical relevance
Understanding the influence of knee function on gait biomechanics is important in selecting and improving treatments and outcomes for individuals with lower-limb amputations. Weight-activated knee joints may result in undesired gait deviations associated with stability in early stance-phase, and swing-phase initiation in the late stance-phase of gait.
Background
As part of a transfemoral (TF) prosthesis, the knee joint mechanism serves several important functions to facilitate mobility. Working in tandem with human motor control and residual musculoskeletal systems, knee mechanisms control lower-limb movements and stability to facilitate efficient and safe gait. Mechanisms that concurrently prevent undesired knee flexion during weight-bearing and allow knee flexion for the swing-phase of gait are termed stance control knee joints. Stance control performance is critical as it aids in minimizing falls and related injuries, and promotes confidence and utilization of the prosthesis. 1 From a physiological perspective, selection of knee mechanisms is also seen to influence efficiency of gait,2–4 and biomechanically have an effect on the gait-related movement and loading patterns which are commonly quantified in terms of spatiotemporal, kinematic, and kinetic measures.
Individuals with TF amputations exhibit numerous biomechanical deviations of abnormal movement and loading patterns, such as hip-hiking and asymmetric limb loading.5–7 Gait deviations are typically determined on the comparative basis to normative/able-bodied controls, or symmetry in relation to the intact limb in the case of unilateral amputation.8–10 Management of biomechanical differences is an important part of rehabilitation, including restoration of function and prevention of long-term musculoskeletal health problems.11,12 As such, quantitative gait assessments have played an important role in evidence-based research and development of prosthetic technologies.13,14 Gait analyses also inform clinical practice, including the optimization of treatments and the selection of prosthetic componentry. 13
For many decades, weight-activated braking (WAB) knees have seen widespread use globally lending to their affordability, good function, and compact and lightweight form. 15 In developed countries, WAB knees are primarily prescribed for older individuals with limited mobility. In most under-resourced countries, WAB knees and other simple mechanical knees are universally applied due to their low-cost, ease of use, and durability. WAB knees utilize a brake that engages upon loading of the prosthetic limb; once the weight on the limb is removed, knee flexion can be initiated for transitioning into swing-phase. By providing a locked and stable knee during weight-bearing, WAB knees offer more functionality over basic single-axis knees which are also commonly used in under-resourced countries.16–18 Despite the global clinical utilization of WAB knees, only one study has assessed their gait performance. This study found biomechanical deviations that include slow gait and greater spatiotemporal asymmetry compared to a four-bar knee. 19 However, evidence about the performance of WAB knees in relation to newer and emerging knee joint technologies is limited. Such information could help to inform clinical practice and the selection of components, particularly in under-resourced countries.
A more recent technology, the automatic stance-phase lock (ASPL) knee joint is also seeing deployment in both low- and high-income countries due to its simple, durable, and cost-effective design. 20 However, the ASPL knee functions differently during gait since it uses a contrastingly different stance control mechanism. Unlike WAB knees which lock upon weight-bearing to provide stability, the ASPL locks in full extension in late swing-phase prior to limb loading. A late stance unweight-bearing releases the WAB brake, whereas a forefoot load triggers initiation of swing-phase flexion in the ASPL mechanism. Hence, the two stance control mechanisms of the WAB and ASPL knees provide distinct stance control function during both the initiation (i.e. stability during weight-acceptance) and termination (pre-swing flexion) of stance phase. Evidence suggests that these divergent control strategies elicit different functional and physiological effects including walking speeds, energy expenditure during walking, and feeling of stability.20,21 However, the underlying biomechanical effects associated with the two mechanisms have not been investigated.
The main aim of this prospective study was to examine and compare the biomechanical responses associated with the WAB and ASPL prosthetic knee joint mechanisms. Based on the need for late stance-phase unloading of the ASPL and WAB mechanisms (Figure 1), it was hypothesized that the ASPL knee would result in a shorter prosthetic swing-phase duration (longer stance-phase percentage) compared to the WAB knee. Associated with this were expected differences in the prosthetic ankle timing including an earlier push off. Secondarily, this study aimed to examine kinematics of the lower limbs, with a focus on the pelvis. Pelvic postural alignment has been closely linked to prosthetic function with pronounced pelvic excursions indicating poorer walking ability.22,23 In addition, greater than normal anterior pelvic tilt has been observed to be a means of increased weight-bearing stability in pathological gait. 15 With previous studies reporting user preferences for the ASPL knee over the WAB knee due to greater perceived knee stability, reduced anterior pelvic tilt was expected for the ASPL knee. 20
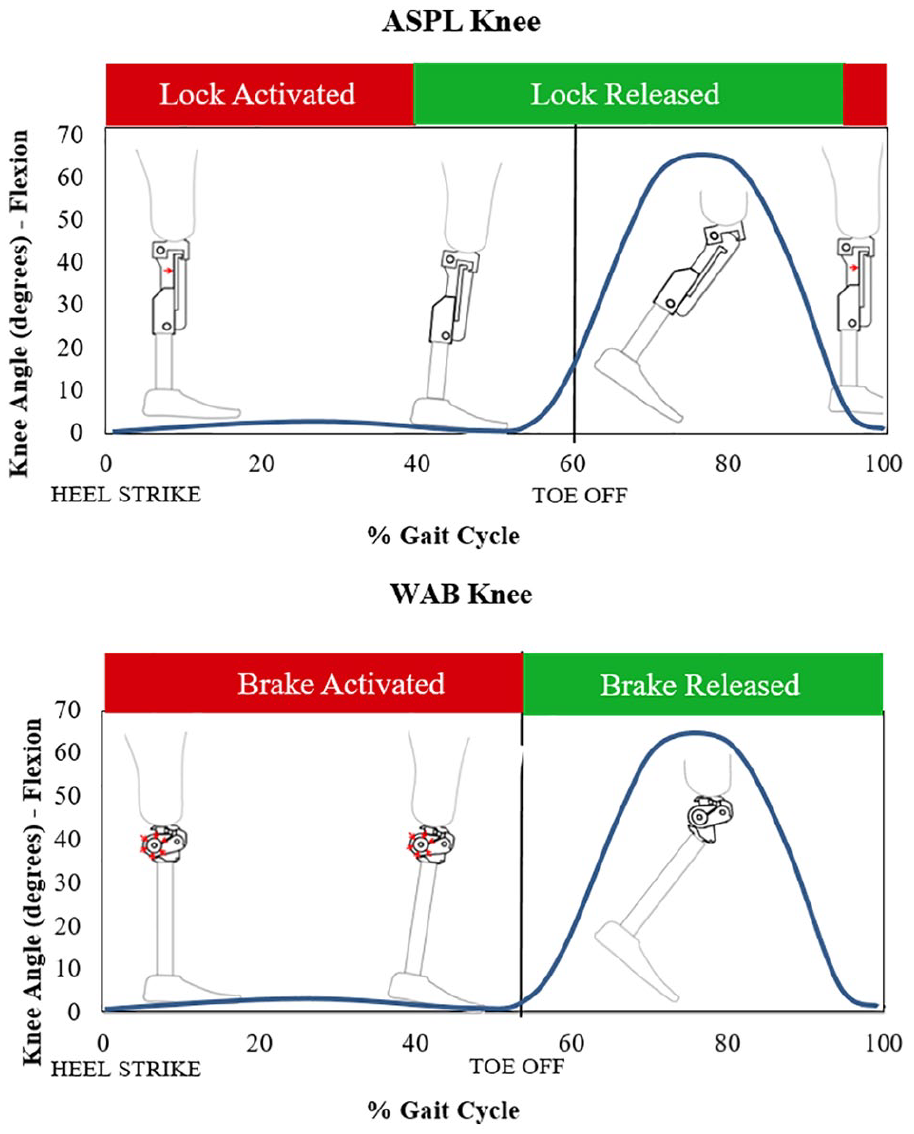
Depiction of stance-phase control strategies utilized by automatic stance-phase lock (ASPL) and weight-activated braking (WAB) prosthetic knee joints during one gait cycle. Activation and deactivation of stance control shown. The vertical line indicates toe-off.
Methods
In this crossover study, each participant was tested walking with each of the WAB (the participant’s current knee) and the ASPL knee joint (introduced to each participant during the study) integrated into their prosthesis.
Study population
A convenience sample of 10 individuals with TF amputations were recruited from a large rehabilitation center in Santiago, Chile. Inclusion criteria included (1) 16 years or older, (2) weighing less than 100 kg, and (3) a community ambulator. All participants provided written informed consent.
Equipment
Two commercially available mechanical prosthetic knee joints were used. The WAB knee units used in this study were model 3R15 (Otto Bock, Duderstadt, Germany). All the participants had already been using WAB knees prior to joining the study. The ASPL knee joint used in this study was the All-Terrain Knee (LegWorks Inc., Toronto, Canada), to which all participants transitioned. Both types of knee joints had similar friction-based swing-phase control and an extension assist spring but different stance-phase control function (Figure 1).
Procedures
The study was conducted over three sessions. During the initial session, demographic data were collected and prosthetic fitting of the ASPL knee joint was initiated. Adjustments were made to the WAB prosthesis as needed to ensure optimal function as determined by the treating certified prosthetist. Data collection for the WAB knee (session 1) followed 4 weeks after the initial session to allow participants to acclimate to any prosthetic adjustments. 24 Data collection for the ASPL (session 2) followed 4 weeks after session 1 to allow acclimation to the ASPL knee. At the end of session 1, the participant’s WAB knee was exchanged for the pre-fitted ASPL knee. Prosthetic alignment was based on the manufacturer’s recommendation and determined by the treating certified prosthetist for the ASPL knee. The composition of the prosthesis (i.e. socket, foot, connectors) remained the same for each data collection session, except for the knee joint.
During sessions 1 and 2, each participant completed a minimum of six walking trials at a self-selected speed over an 8-m linear and level path. Movement data were obtained with an eight–camera optoelectronic system (BTS Bioengineering, Milan, Italy) at a 100-Hz recording frequency filtered with a 6-Hz Butterworth filter. Body markers were installed based on the protocol described by Davis et al. 25 Three markers were placed on the pelvis, one over each anterior superior iliac spine and one centered directly over the midpoint of the posterior superior iliac spines. For the thigh, markers were placed on the femoral lateral condyle, great trochanter and a “bar” marker on the mid-thigh collinear with the trochanter and condyle markers. This way, the segment coordinate system was oriented so that the longitudinal axis of the thigh lay in the plane formed by the three markers. The same criterion was used for the shank but with a marker over the head of the fibula, one on the lateral malleolus and a bar marker midway along the shank. For the foot, a marker was placed on the lateral aspect of the shoe in the projection of the fifth metatarsal head. The same procedure was used for the prosthetic limb by making equivalences wherever necessary, including placing the marker at the prosthetic knee joint axis instead of the femoral lateral condyle. The kinetic data were sampled at 200 Hz from two staggered force plates located midway along the walkway (Kistler, Winterthur, Switzerland). The force plate data were synchronized with the kinematics by SmartClinic capture software (BTS Bioengineering). Anthropometric measures were obtained from each subject including height, weight, pelvis width, knee diameter, ankle diameter, and total length of both lower limbs for use in the musculoskeletal model.
After the acquisition, BTS® TrackLab (BTS Bioengineering) software was used for the optoelectronic system’s acquisition labeling process. The labeled trials were then processed using an ad hoc protocol, developed via biomechanical software BTS® Smart-Analyzer. From each trial, the data were analyzed from the stride (two contralateral steps) occurring during forceplate strikes. Spatiotemporal data were based on the marker data, with timing events verified from forceplate strike data. Swing time data were normalized to the percentage of gait cycle (GC) by dividing the swing/stance times by stride times for each trial. 13 Normalizing the GC eliminates the confounding effect of different walking speeds and cycle times. Ankle, knee, and hip- joint angles and moments were analyzed in the sagittal plane, and pelvic movement in all three planes, for the intact and prosthetic limbs. Discrete parameters were based on global and local curve minimums and maximums and range of motion (ROM) values. These were extracted using a custom MATLAB program (MathWorks, Natick, USA). 13 For the minimum and maximum values, the timing of these events was assessed as a percentage of the GC. The parameters were derived from a total of six strides per participant.
Data analysis
The normality of the distribution of each condition was tested using the Shapiro–Wilk test (p < 0.05). Since 10% of the parameters assessed were not normally distributed (p < 0.05), a non-parametric two-tailed Wilcoxon signed-rank test was used for all analyses. The significance level was set at p < 0.05. All statistical analyses were performed using SPSS version 24.0 (IBM, Armonk, USA).
Results
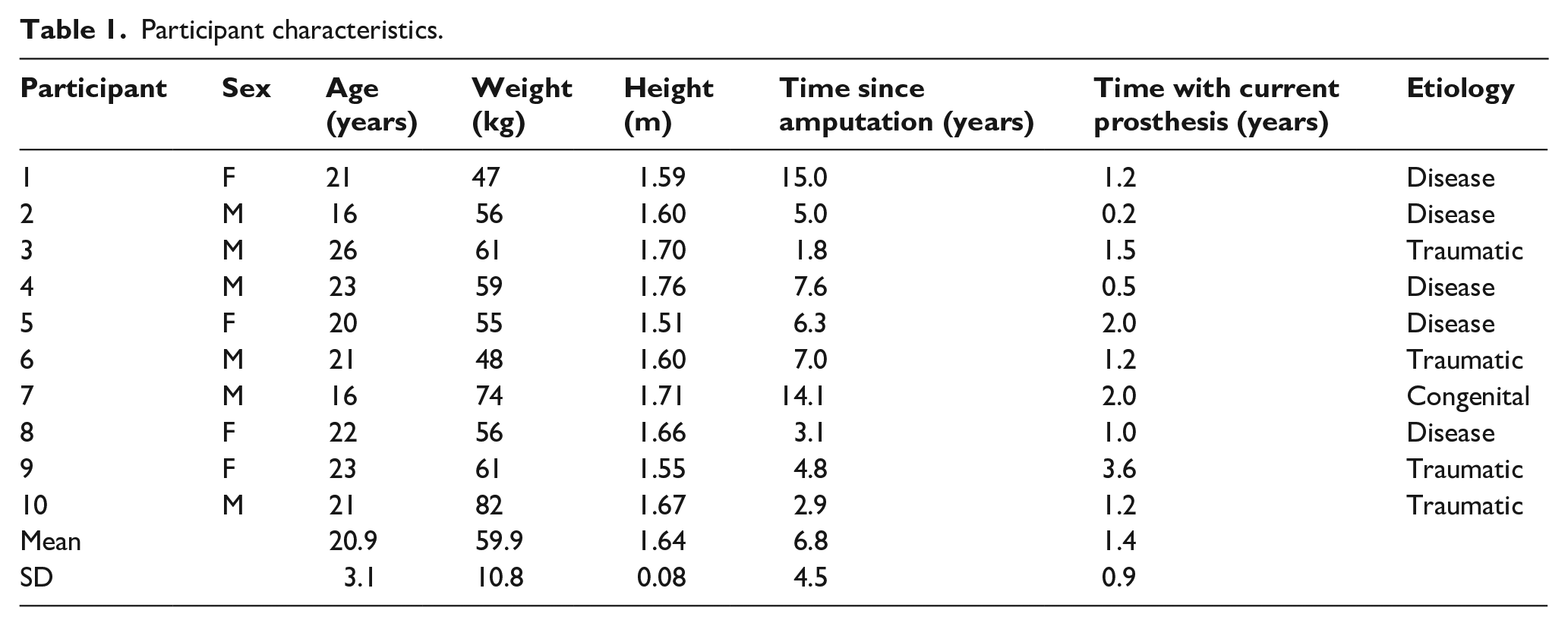
The participants had a mean age of 20.9 ± 3.1 years. Their mean heights and weights were 1.64 ± 0.08 m and 59.9 ± 10.8 kg, respectively (Table 1). All participants normally used a hybrid socket (quadrilateral and ischial containment) and classic vacuum system for suspension, and a WAB knee joint. Participants 4 and 5 used a single-axis foot, and the others had a Solid Ankle Cushion Heel (SACH) foot. Locomotor Capabilities Index (LCI-5) mean scores were 53.7 (range, 50–56) out of a maximum of 56. 26 No fit or alignment issues were found for the prosthetic devices during the first assessment, and thus no corrections were required or performed during the study.
Participant characteristics.
Relating to the primary hypothesis, differences were found in the prosthetic swing-phase timing (Table 2). On average, the WAB knee produced a longer prosthetic swing-phase percentage by 1.01% ± 1.14% (Z = –2.192, p = 0.028). In absolute terms, the swing-phase percentages were 45.6 ± 2.6 and 44.6 ± 2.4 for the WAB and ASPL knees respectively. Mean temporal differences of events were also found in the prosthetic ankle peak dorsiflexion angle which occurred at mean 41.0% ± 3.7% of GC for the WAB and 43.2% ± 2.7% of GC for the ASPL (Z = –2.344, p = 0.019), as well as the prosthetic ankle peak internal plantarflexion moment which occurred at 39.1% ± 2.5% of GC for the WAB and 40.3% ± 2.8% of GC for the ASPL (Z = –2.344, p = 0.019). From the kinematic analysis, the WAB knee produced greater maximum anterior pelvic tilt (3.3 ± 3.0 degrees; Z = –2.497, p = 0.013), and greater anterior pelvic tilt excursions (1.4 ± 1.7 degrees; Z = –2.090, p = 0.037) and greater intact side hip flexion in early stance (3.7 ± 3.9 degrees; Z = –2.293, p = 0.022), compared to the ASPL knee (Tables 3 and 4, Figures 2 and 3).
Spatiotemporal and pelvic kinematic measures.
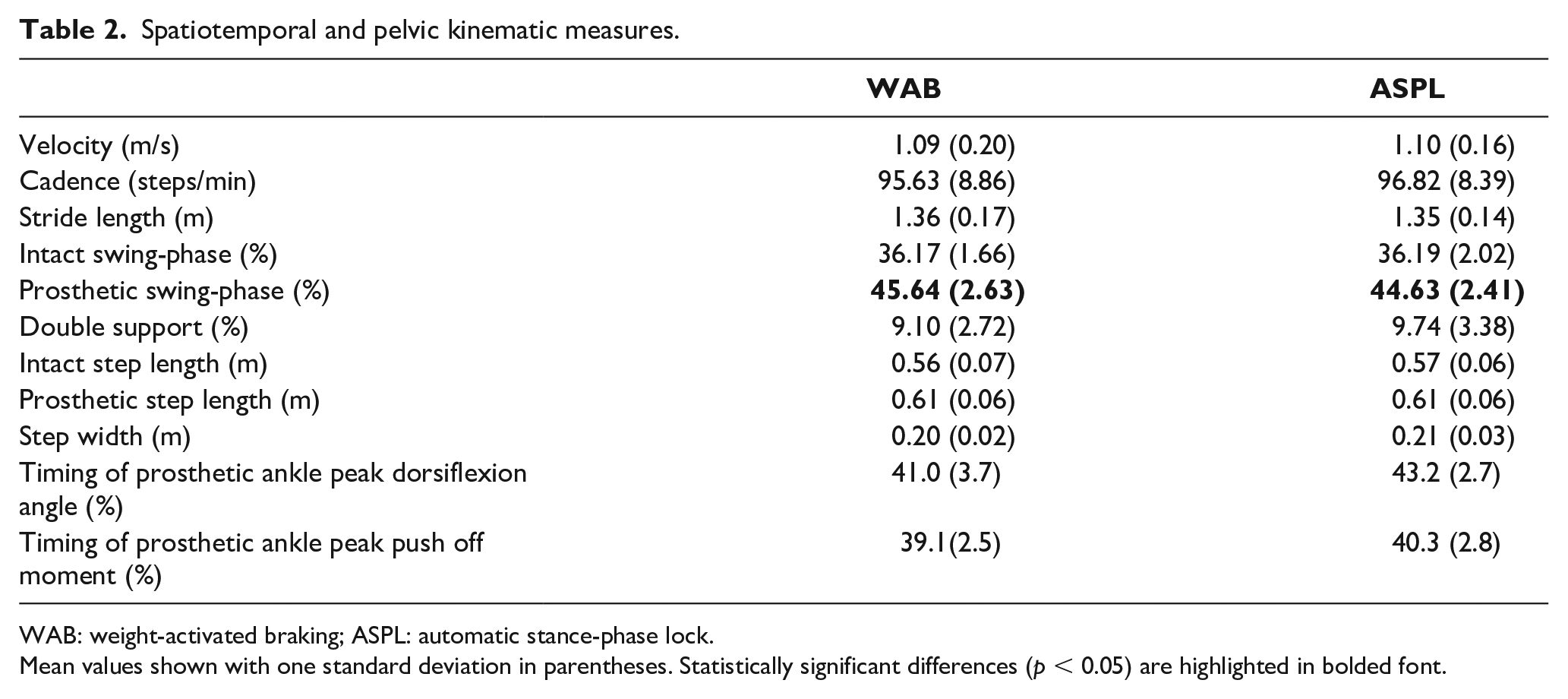
WAB: weight-activated braking; ASPL: automatic stance-phase lock.
Mean values shown with one standard deviation in parentheses. Statistically significant differences (p < 0.05) are highlighted in bolded font.
Pelvic kinematic measures.
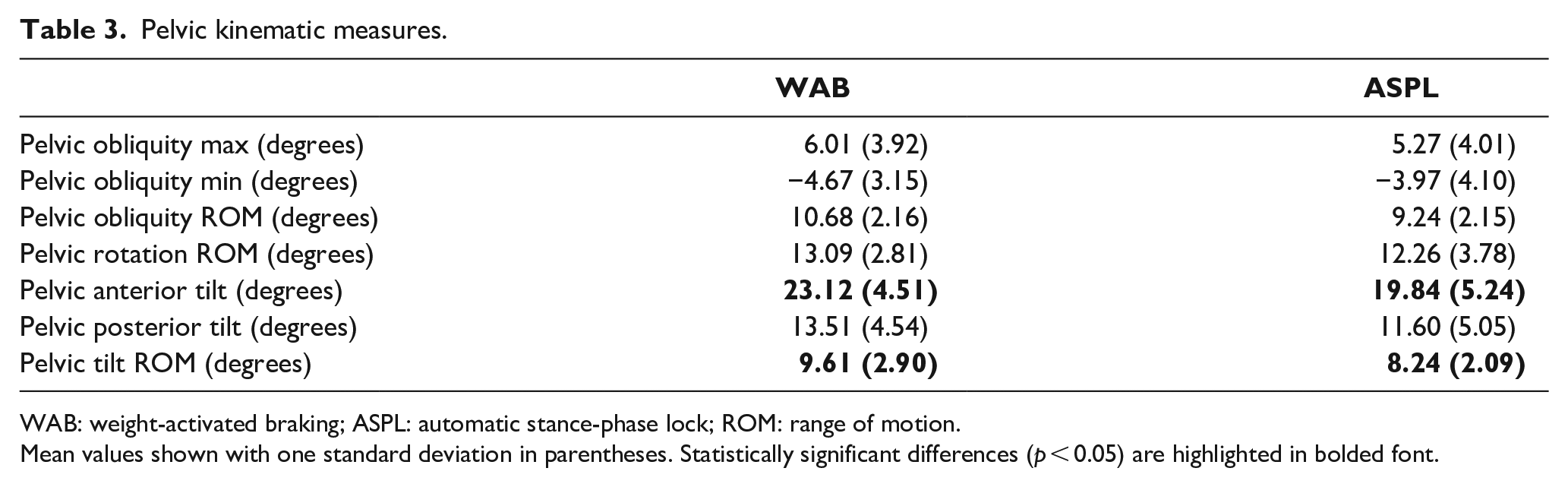
WAB: weight-activated braking; ASPL: automatic stance-phase lock; ROM: range of motion.
Mean values shown with one standard deviation in parentheses. Statistically significant differences (p < 0.05) are highlighted in bolded font.
Minimum and maximum joint angles.
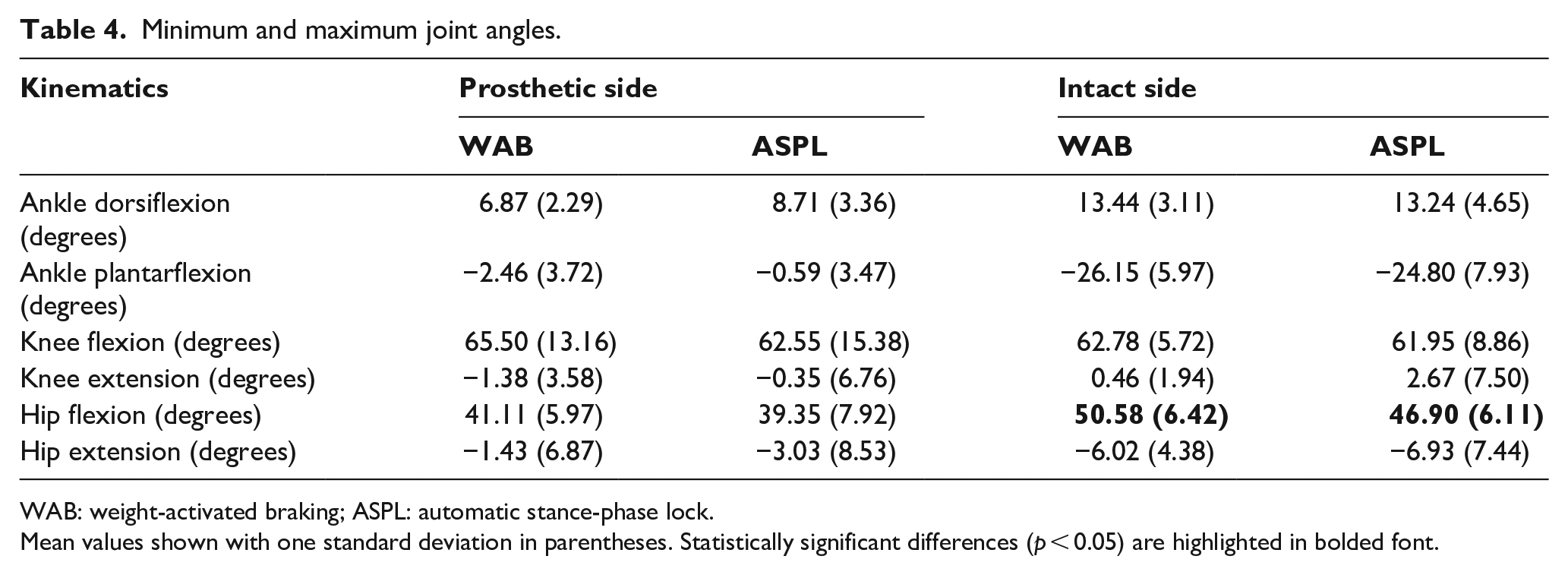
WAB: weight-activated braking; ASPL: automatic stance-phase lock.
Mean values shown with one standard deviation in parentheses. Statistically significant differences (p < 0.05) are highlighted in bolded font.
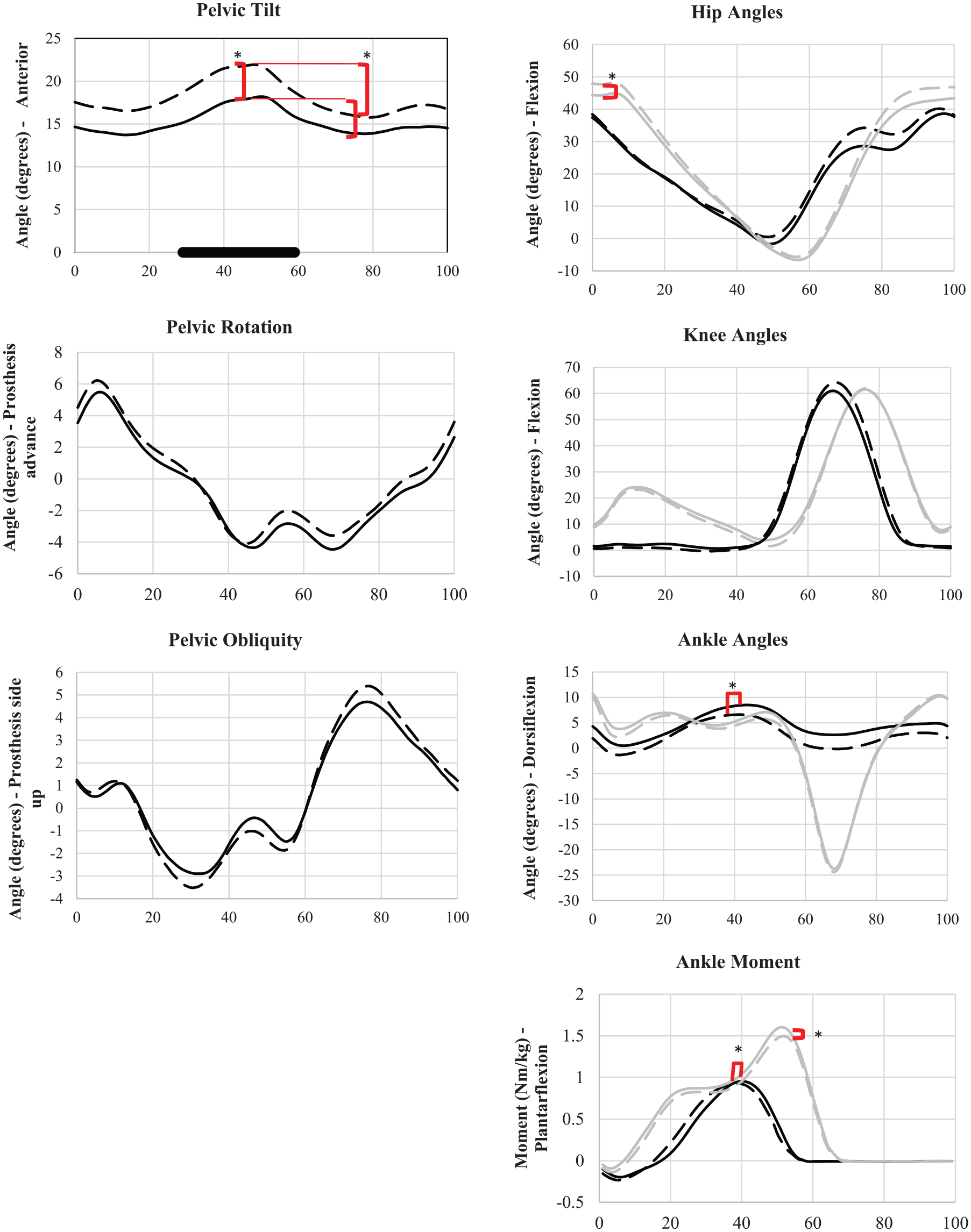
Kinematics and ankle moment data as percentage of gait cycle (%). Dashed line indicates WAB knee and solid line ASPL. Gray line indicates intact side and black line prosthetic side or overall movement as in the case of pelvic kinematics. Internal moments are indicated. For clarity, standard deviations are omitted from the graphs and included in Tables 2 and 3. Statistically significant differences (p < 0.05) are denoted by asterisks.
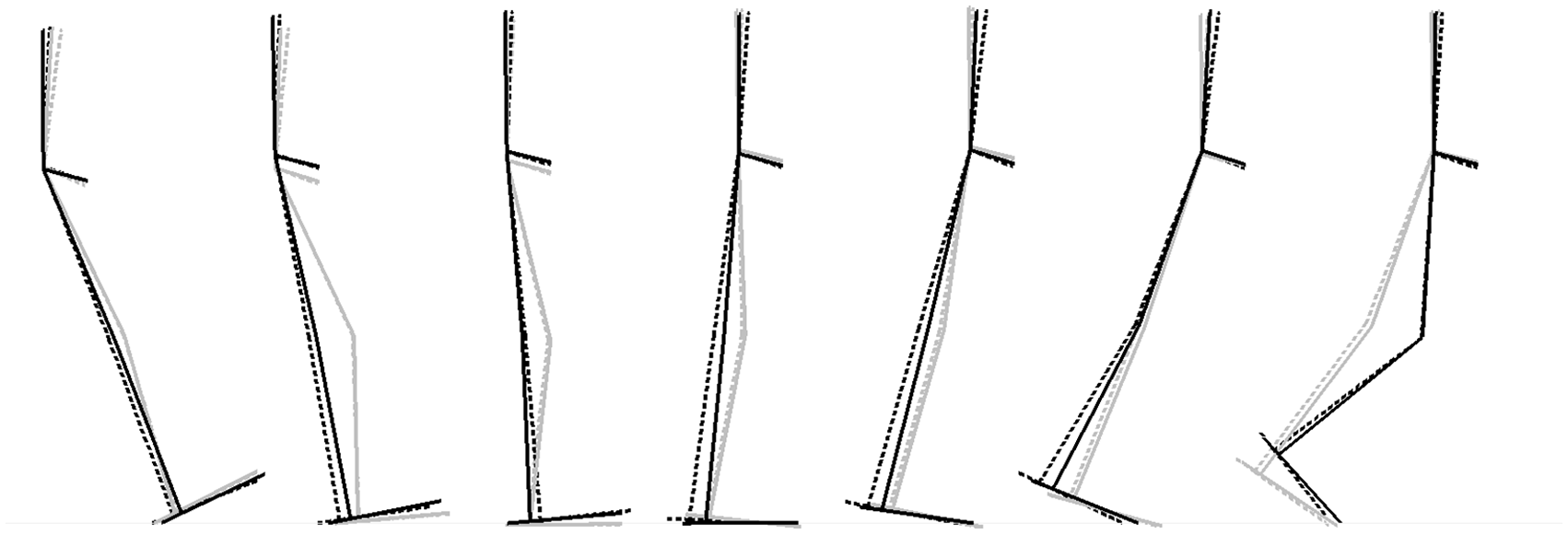
Stance cycle at 0%, 10%, 20%, 30%, 40%, 50%, and 60% of gait cycle. Dashed line indicates the weight-activated braking (WAB) knee and solid line the automatic stance-phase lock (ASPL) knee. Gray line indicates intact side and black line prosthetic side.
Discussion
Leading research in the field has focused on identifying the biomechanical effects of prosthetic mechanisms. 14 Prosthetic design variants have an influence on walking patterns; however, these relationships are not well established in existing literature. This study examined and compared the biomechanics of two commonly used stance control mechanical knees. The biomechanical results support the theoretical basis by which the control mechanisms of the tested knees differ. As hypothesized based on the mechanics of the two knees, a corresponding difference in the timing of stance-phase unloading was found. In addition, the pelvic and hip alignment and movements were found to differ between the two knees.
TF gait is characterized by underutilization of the prosthetic limb and overreliance on the intact limb, both in terms of duration and magnitude of loading.2,13,27 This may be associated with poorer mobility outcomes,2,3,5–7 and long-term disorders including back pain and osteoarthritis.11,12,28 Swing-phase percentage of gait represents the proportion of time spent in swing versus stance-phase. As typical, able-bodied values are circa 40% of GC and below,2,29 both knees produced excessive prosthetic side values, with the WAB knee being slightly higher. The analysis of ankle push-off biomechanics corresponded with the shorter WAB stance percentage. Specifically, for the WAB knee the prosthetic ankle peak plantarflexion moment and maximum dorsiflexion angles occurred earlier in the GC compared to ASPL. These results support the conclusion that the use of the WAB may produce earlier push-off and stance-phase termination. This may be indicative of a delay associated with the WAB mechanism brake deactivation.
Another main difference relates to pelvic alignment and movements. Significant differences in pelvic tilt kinematics have been reported previously in persons with lower-limb amputations, with potential implications on overall mobility and long-term musculoskeletal health.9,22,23 Greater than normal anterior tilt and ROM have been reported for TF, and found to be affected by prosthetic interventions (i.e. osseointegrated prostheses vs socket). 22 In this study, the ASPL reduced and improved both anterior pelvic tilt and tilt ROM compared to the normative values. 23 The magnitude of change in anterior pelvic tilt found in this study (WAB vs ASPL) was similar to changes seen in users switching from conventional sockets to osseointegrated prostheses. 22 Anterior pelvic tilt can be a compensatory mechanism for augmenting stability in pathological gait via a forward center-of-mass that promotes stabilizing hyper-extension moments at the knee joint. 15 Thus, differences in biomechanics at the proximal levels may be related to the stance control function of the two knees. In previous work, users perceived greater stability with the ASPL knee compared to the WAB knee which may account for the adoption of decreased anterior pelvic tilt. 20 As expected, the anterior pelvic tilt also resulted in changes in hip angles, based on the alignment of the thigh and pelvic segments in standing posture and gait.
This work is encouraging and suggests that common variants in stance control design and function can be captured via instrumented gait analysis. While the evidence in literature linking knee performance, biomechanical responses, and clinical outcomes is limited, the results of this study do indicate potential relationships between stance control and spatiotemporal and kinematic measures. In addition, it is plausible that these biomechanical differences may also play a role in previously measured differences between the two knee joints with respect to energy expenditure and perceived knee stability during walking; 20 however, future work is needed to unravel this further. This work does suggest that greater consideration should be given in the selection of prosthetic knee joints, particularly for higher level ambulators. While best practices discourage the prescription of WAB knees for active young individuals, in many under-resourced countries only WAB knees and other simple mechanical knees may be accessible. The ASPL knee may be more appropriate from a functional and biomechanical perspective; however, factors such as cost, durability, and ease of use also need to be considered in clinical practice.
Future studies should consider the following suggestions and limitations of this study. First, given the multiple parameters that were analyzed, the possibility of type I error is acknowledged, and with the small sample size the possibility of type II error exists for the “no difference” conclusions. Significant differences found in some of the parameters may not be large enough to be considered clinically important. While this magnitude of difference may have occurred in the group comparisons, on an individual basis, the difference for some of the study participants was larger than the group mean difference and potentially important functionally. Future work should focus on a systematic investigation of effects of a select subset of gait parameters, as predetermined in this study. It should be noted that other biomechanical measures not explored here could also be important to consider. Limitations of this study design include a lack of randomization and differences in acclimation time to each of the knees, since the participants on average used the WAB knee for several years, and the ASPL knee for only 4 weeks. Hence, it is possible that more acclimation to the ASPL knee may have led to more pronounced or even different changes in gait patterns. Randomization of the interventions would have required the participants to revert to using the WAB knee, which was not feasible since this study involved long-term testing with the ASPL knee. 20 The lack of randomization may have introduced biases due to confounding effects including those related to the order of testing. Future work should aim to increase sample size and statistical power to allow for analysis of co-variates such as the foot type (SACH vs single axis), ages, duration of prosthetic use, and others.
Conclusion
Developing an understanding of the influence of knee designs and their function on overall biomechanics of human mobility is a critical step toward improving treatments and outcomes for individuals with transfemoral amputations. This study provides new information about the biomechanical performance of two different types of prosthetic stance control knees. Based on our findings, promoting loading in late stance-phase may be advantageous in improving and normalizing the timing of loading patterns of the prosthetic limb, while better knee stability may improve pelvic alignment and movements. Further work is needed to help guide clinical practice around the utilization of various prosthetic knee joint mechanisms, and to establish the relationships between gait biomechanics and overall patient mobility and outcomes.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.A. is the inventor of the automatic stance-phase lock (ASPL) knee (All-Terrain Knee) and co-founder, CTO, and shareholder of LegWorks Inc., the manufacturer of the All-Terrain knee. None of the other authors have any conflicts to disclose.
Ethical approval
All participants provided written informed consent to this project which was approved by the Research Ethics Boards at Holland Bloorview Kids Rehabilitation Hospital, Toronto, Canada, and the Sociedad Pro Ayunda del Nino Lisiado, Santiago, Chile (Approval #12-284).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grand Challenges Canada (Grant no. 0048-01-04-01-01).