
Abstract
Background:
Walking with a prosthesis requires substantial concentration on behalf of the user and places increased demands on executive functions. Little is known of the effects that prosthetic knee joint prescription may have on executive functioning.
Objectives:
Evaluate executive functioning in trans-femoral prosthesis users during single and dual-task walking, before and after they transition to a Microprocessor-controlled prosthetic knee unit.
Study Design:
Multiple case-study design.
Methods:
Single and dual task gait was evaluated while recording cortical brain activity. Testing occasion 1 occurred prior to participants receiving their microprocessor-controlled prosthetic knee, while testing occasion 2 was conducted a minimum of 8 months after they had been fitted with an microprocessor-controlled prosthetic knee.
Results:
During single-task level walking and walking while performing a dual-task key finding test, executive functions, measured as the relative haemodynamic response in the frontal cortex, reduced for most, but not all participants after transitioning to an Microprocessor-controlled prosthetic knee. There did not appear to be any difference when participants performed a trail walk test.
Conclusions:
Results suggest Microprocessor-controlled prosthetic knee prosthetic knees may have a positive effect on executive functioning for some individuals who have undergone a lower-limb amputation. A larger, longitudinal study with careful control of extraneous variables (e.g. age, training) is needed to confirm results and determine causality.
Clinical relevance
This article provides some evidence to suggest that prosthetic prescription may influence executive functioning and that microprocessor-controlled prosthetic knee mechanisms may reduce cognitive effort when walking.
Background
The term executive functions refer to a set of higher-order cognitive process that are used when we must concentrate or pay attention to something. Executive functions are thought to include impulse control, response inhibition, attention, working memory, planning and decision making.1,2 A clear link has been established between executive functioning and gait performance. 3 Of importance in the rehabilitation setting is the knowledge that individuals with body impairments affecting their mobility have increased demands on executive functions when they walk.4,5 In lower-limb prosthesis users, self-reported ability to ambulate “without thinking” is a predictor of decreased depression and improved balance confidence. 6 Microprocessor-controlled prosthetic knee components (MPKs) have been associated with a reduction in patient-reported measures of cognitive effort when walking. 7 A recent cross-sectional study by Möller et al. suggests that individuals fitted with MPKs require less cortical brain activity during level walking than those fitted with non-microprocessor controlled knees. 8 Interestingly, differences in cortical brain activity demonstrated by Möller et al. 8 existed even when no differences in temporospatial parameters were observed. In a structured review investigating the relative effects of dual-task performance on gait, it was suggested that performance of a dual task did not affect walking in individuals with lower-limb amputations more than controls. 9 This review did not include any direct measures of cortical brain activity.
To date, measures of executive functioning during gait have largely used dual-task paradigms to indirectly measure cognitive processes. 10 Recently, however, a non-invasive brain imaging technique, functional near-infrared spectroscopy (fNIRS), has received increasing attention as a means of evaluating executive functioning. 11 Anatomically, cortical activity in the frontal lobes, and specifically the prefrontal cortex, has been associated with executive functions.12,13 fNIRS provides a measure of regional cerebral blood flow (rCBF) and has been described extensively in the literature. 14 In response to a stimulus, the typical haemodynamic response to brain activation would be a rapid increase in oxygenated hemoglobin (oxyHb) and a slower, lower amplitude, decrease in deoxygenated hemoglobin (deoxyHb). 14
The aim of this study was to investigate changes in the haemodynamic response of trans-femoral prosthesis users during single and dual-task walking, before and after they transition to an MPK knee unit. It was hypothesized that activity in the prefrontal cortex would be reduced in single and dual-task walking after transitioning to an MPK knee and that the largest differences would be observed in dual-task walking when cognitive demand is considered greatest.
Methods
Approval for the study was granted by the Regional Ethics Committee, Linköping, Sweden (ref: 2015/215-31).
Participants
Convenience sampling was used to recruit participants from local prosthetic and orthotic clinics. Participants were recruited on the basis that they had been using a prosthetic limb incorporating a non-MPK for a minimum of 1 year and that they had been approved by the relevant funding agency to receive an MPK. Individuals were required to be able to ambulate for a minimum of 500 m and understand verbal and written instructions. Individuals with concomitant conditions affecting their neurological function and/or memory were excluded. As participants lived in different regions of the country, it was not possible to conduct testing at a single location. Instead, trials were conducted in a quiet gymnasium located at the participants’ own prosthetic and orthotic clinic.
Procedure
A multiple case-study design was used. Participants underwent testing on two occasions. The first testing occasion occurred with participants’ current non-MPK while testing occasion 2 was conducted a minimum of 6 months after they had been fitted with an MPK. In the absence of standard recommendations regarding the time it takes to accommodate to an MPK, a minimum of 6 months was considered to be an acceptable period.
During both testing occasions, participants were fitted with an fNIRS system incorporating 8 detector channels and 8 illumination sources, resulting in a total of 20 channels covering the frontal cortex (NIRSport, NIRx Medical Technologies) (Figure 1). Accurate positioning of fNIRS optodes is vital to ensure that specific brain regions are identified. 14 To limit positioning error, we used the international 10–20 system for optode placement and ensured that the same investigator was responsible to fitting the measurement caps and placement of optodes. Positioning of probes corresponded to Brodmann areas 8, 9, 10, 11, 44, 45, 46, and 47. fOLD software was used to determine appropriate positioning of probes. 15 Each illumination source emitted infrared light at wavelengths of 760 and 850 nm and a frequency of 7.81 Hz.
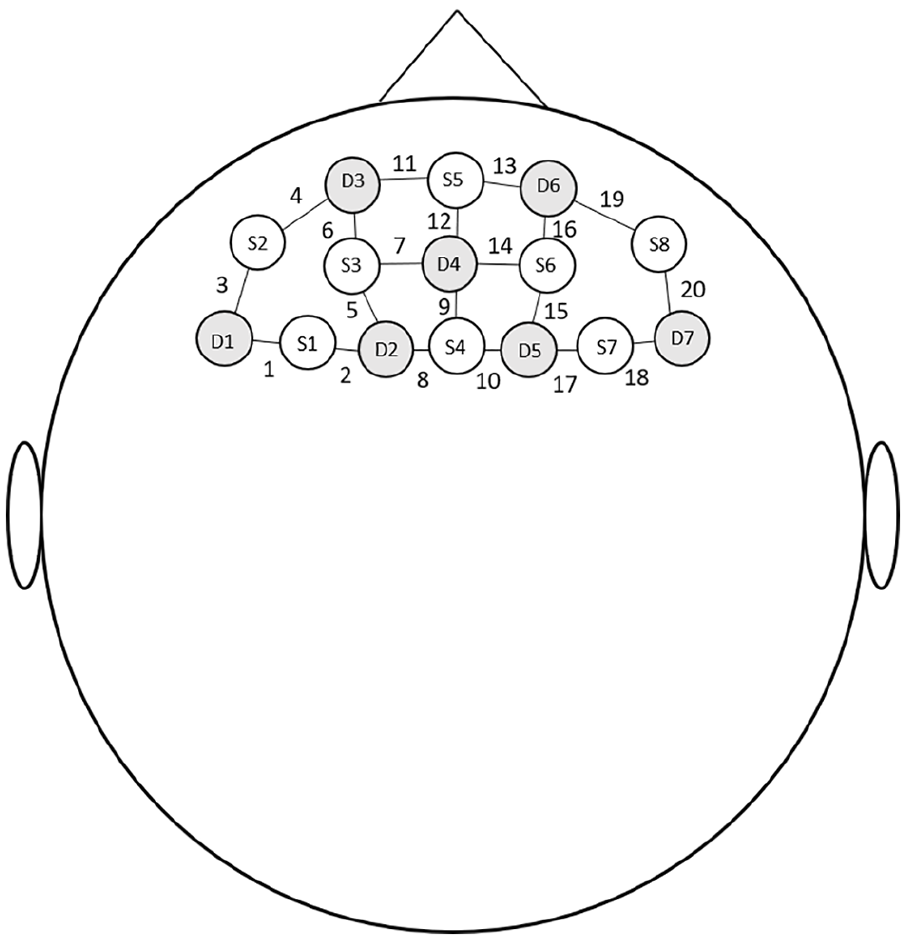
Placement of probes and designation of channels.
The fNIRS system was used to record haemodynamic responses under three walking conditions.
Single-task: Straight, level walking at a self-selected velocity (Level Walking Test—LWT)
Dual-task Key test: Straight walking while finding a key on a keyring comprised of 8 different keys with different numbers and colors. When completing this test, participants were informed of the specific key they were to find immediately prior to receiving the signal to walk. They were also instructed that they could only use one hand to find the key and to hold it up in the air when it was identified.
Dual-task trail walk test (TWT): Walking in sequence around randomly ordered, numbered cones. Six numbered cones were placed in a 1 m × 4 m area in a pre-determined, randomized order. Participants were required to circle the cones in consecutive order as fast as possible. The position of numbered cones was altered for each walking trail, and participants could not see the numbers until the signal to begin walking was given.
The single-task walking trial and the dual-task Key test were conducted on a walkway that was 15 m in length. Participants were requested to walk the full l5-m length, circle a cone and walk back to the starting position. The time taken to walk the first 10 m of the walkway was recorded along with the number of steps taken. For the dual-task TWT, only time taken to walk around the six cones was recorded.
Each condition was repeated 4 times for a total of 12 trials. The final three trials for each condition were analyzed. We chose to exclude the first trial in the analysis as participants were likely to have been more hesitant and unsure about the task the first time it was performed and this may have affected fNIRS results.
Prior to each walking condition, baseline signals were collected for 30 seconds with the participant sitting quietly, with eyes closed. The method of collecting baseline data varies in fNIRS literature. We chose to use a seated, baseline measure in accordance with recommendations of Herold et al. 16 Following the baseline measures, participants then stood for a period of 30 seconds to allow for stabilization of fNIRS signals before being given the signal to commence testing. 17 An investigator was positioned beside the participant in case they experienced balance disturbances. All instructions were given via pre-recorded verbal instructions administered using NIRStim software (NIRx Medical Technologies). This software was also used to place reference markers in the data file which conveyed the point in time each test was initiated.
Data analysis
Data were pre-processed using nirsLAB software (NIRx Medical Technologies). Bad channels were removed (gain factor > 3 or coefficient of variation > 15%), 18 as well as discontinuities and spike artifacts (threshold 5). Signals were bandpass filtered with a low-cut-off frequency of 0.01 Hz and a high cutoff if 0.2. Haemodynamic states were then calculated utilizing a procedure that is described by de Lima-Pardini et al. 19 A general linear model incorporated in nirsLAB software was used for analyzing data. Data were modeled from 5 seconds after each walking trial was initiated, and all trial durations were set to 10 s.
Results
Six individuals, including 4 males, who had undergone a trans-femoral amputation were recruited for the study. Participant details are presented in Table 1. Participants had been amputated for an average of 10.8 years (range: 1–37). None had used an MPK prior to this study and the average period of time participants had to accommodate to the MPK prior to testing was 7.8 months (range: 6–13).
Participant details. Bad channels indicate the specific fNIRS channel/s that were excluded.
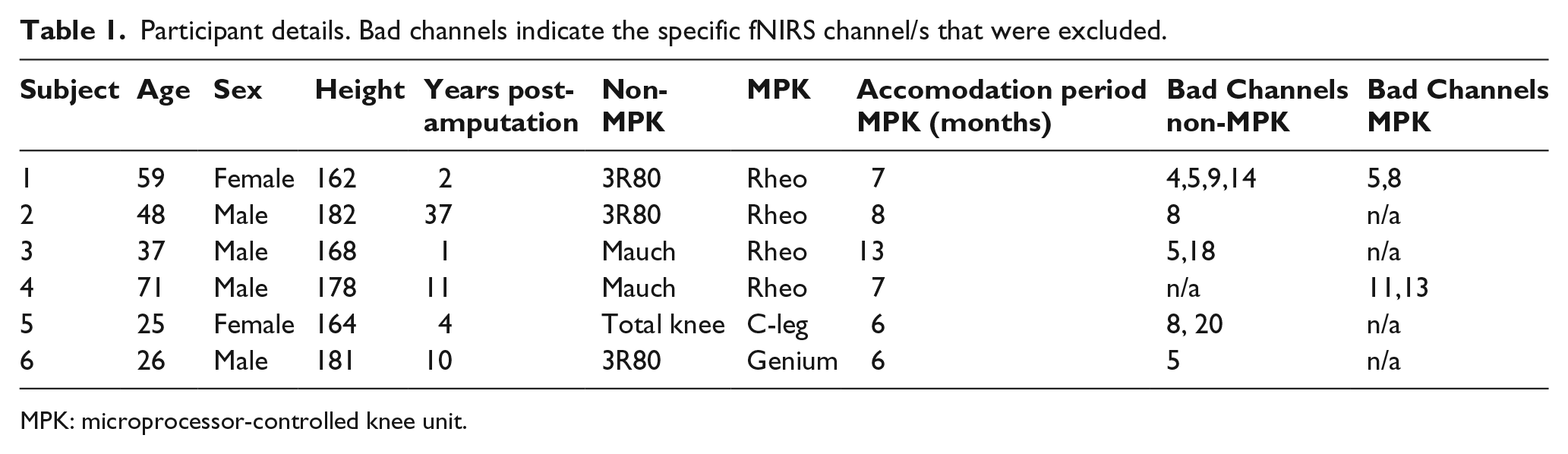
MPK: microprocessor-controlled knee unit.
Single-task walking
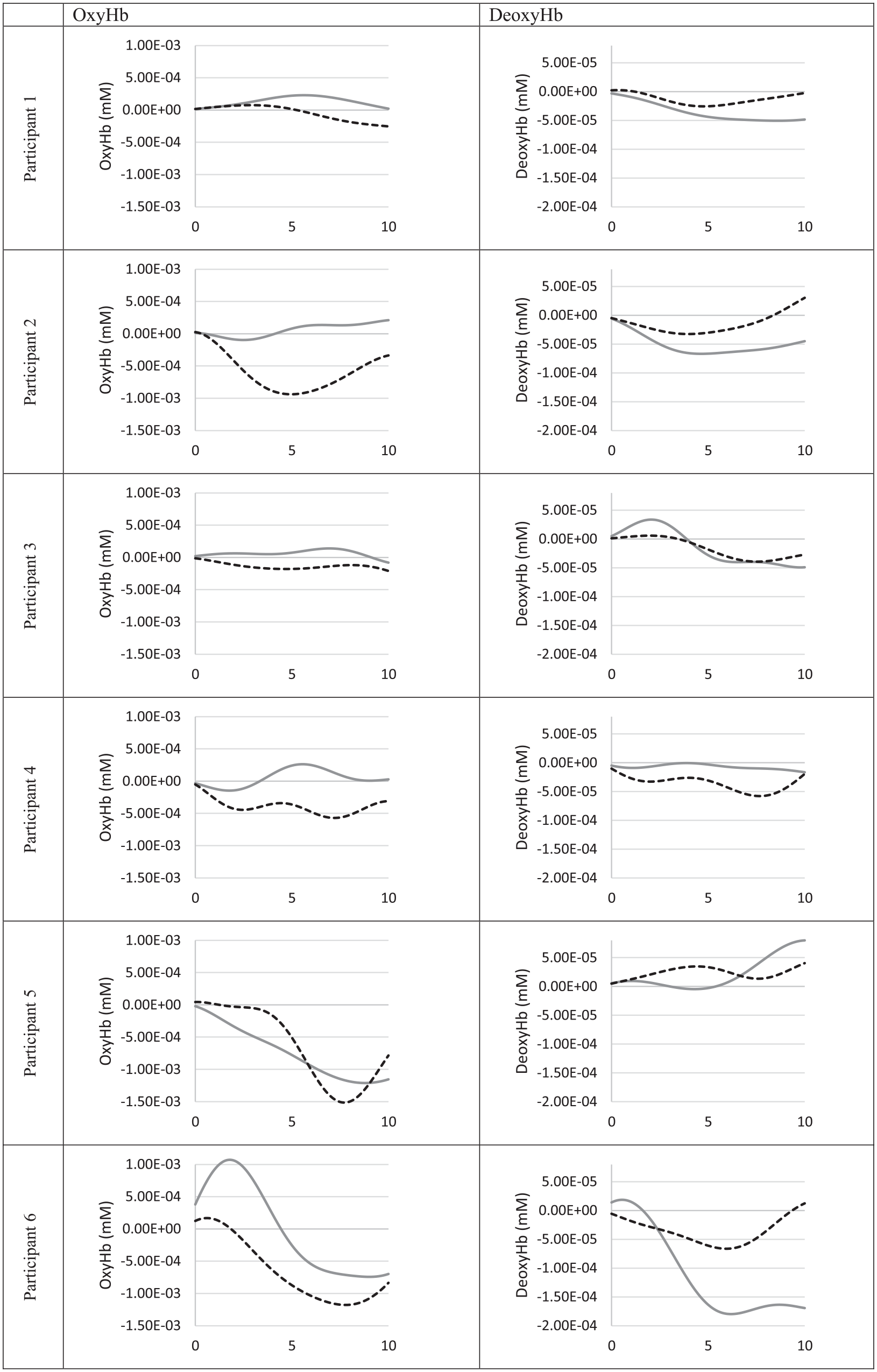
Time taken to walk 10 m and the number of steps taken are presented in Table 2. There were no consistent patterns observed across the 6 participants; however, participants 1–3 all reduced the time it took to walk 10 m when they were fitted with an MPK. Figure 2 presents the mean haemodynamic response during single-task walking for oxyHb and deoxyHb in the prefrontal cortex, presented as an average across the three walking trials included in the analysis. During single-task walking, oxyHb levels were generally higher for the non-MPK condition and this was more evident in participants who had been using a non-MPK for < 2 years and those fitted with a Rheo knee for the MPK condition (participants 1–4). DeoxyHb signals revealed greater variability between subjects.
Time to walk 10 m and number of steps taken over 10 m.
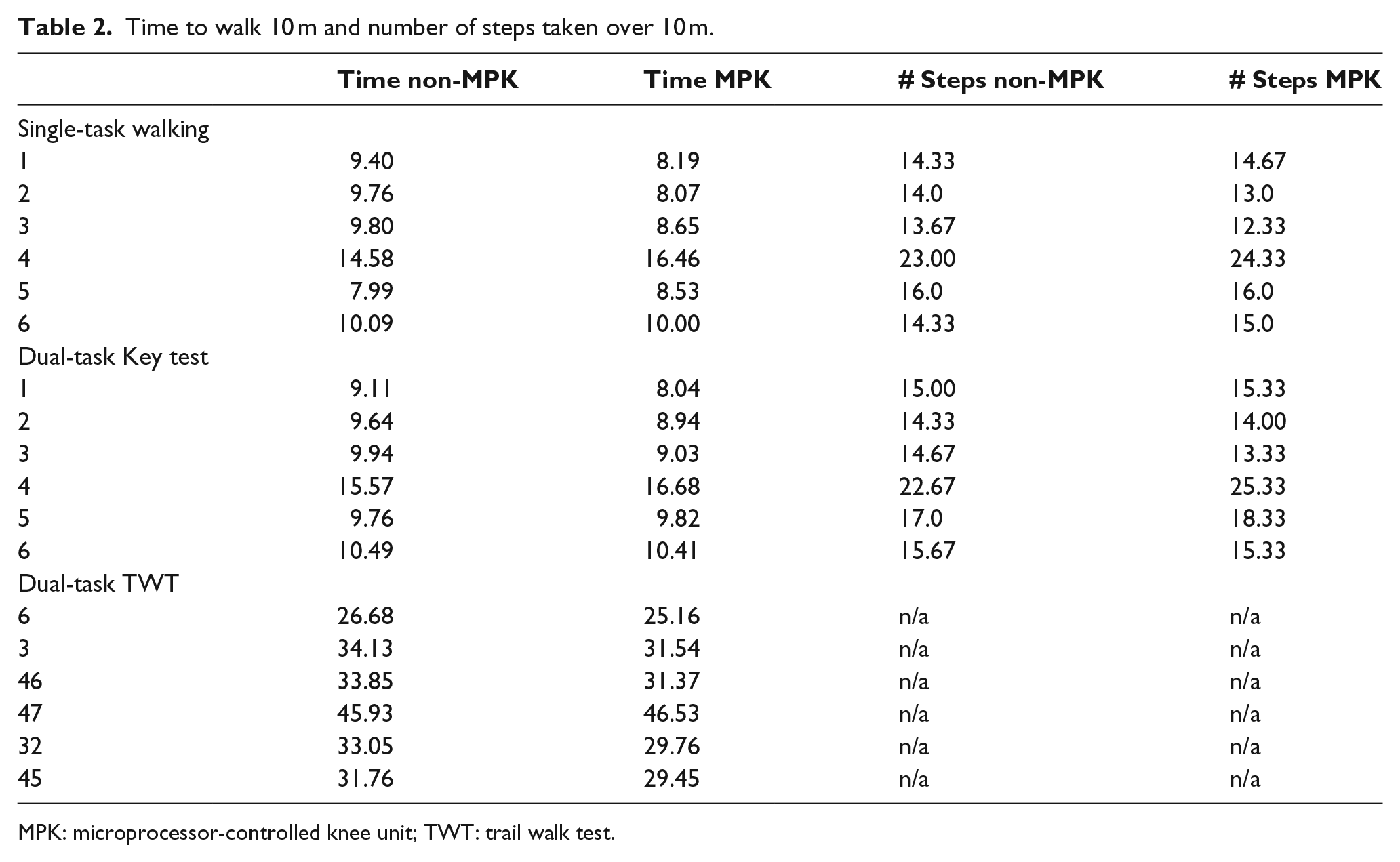
MPK: microprocessor-controlled knee unit; TWT: trail walk test.
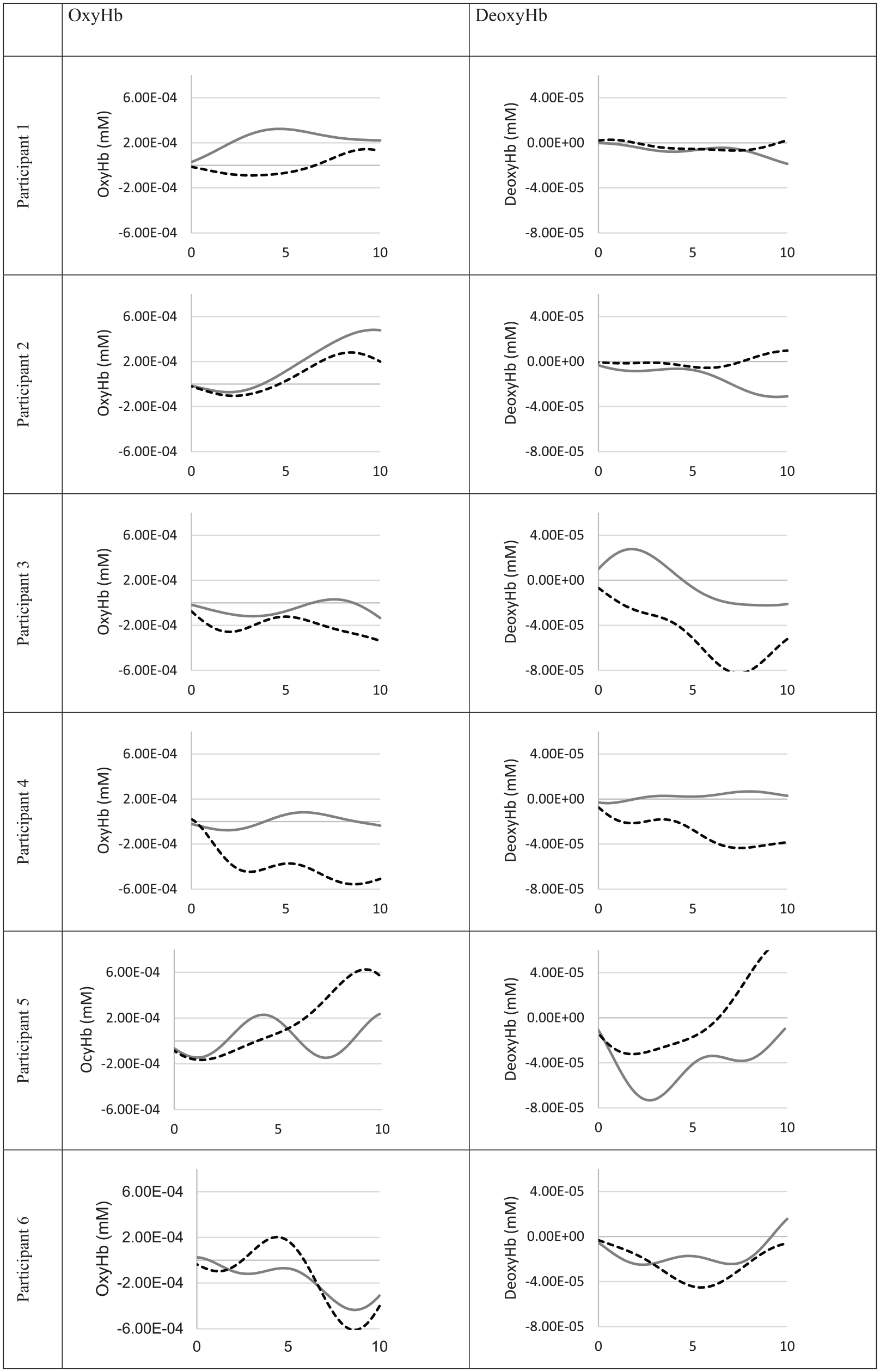
Level walking test (LWT)—individual mean haemodynamic response for oxyHb and deoxyHb in the prefrontal cortex. All units in millimoles per liter (mM). Non-MPK = solid gray line and MPK = dotted black line.
Dual-task walking—Key test
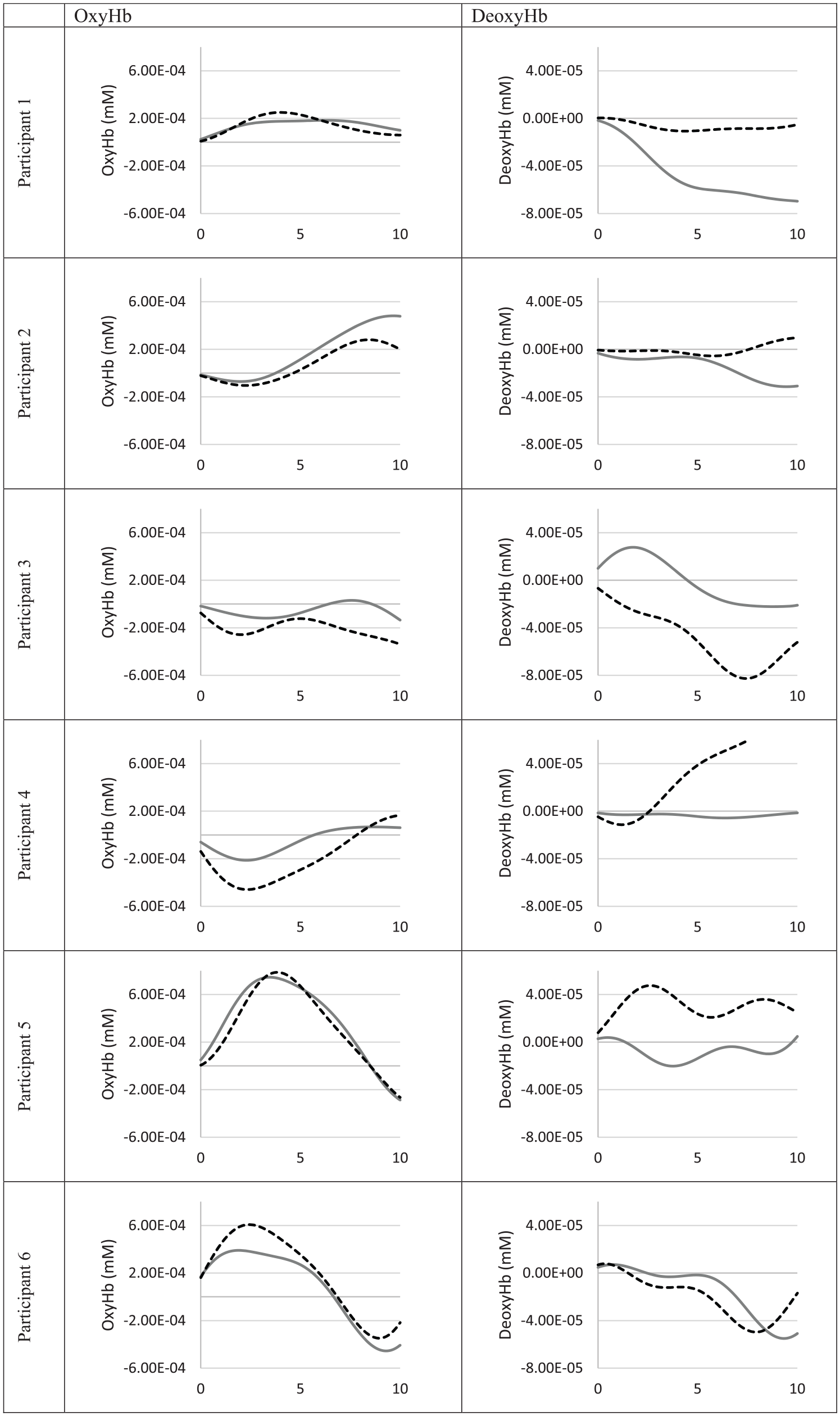
Time taken to walk 10 m was less in the MPK condition for participants 1, 2, 3, and 6. Participants 4 and 5 took more time to walk 10 m and took more steps in the MPK condition (Table 2). When performing the dual-task key test, higher oxyHb levels in the non-MPK condition were seen for all except participant 5 (Figure 3).
Keys test—individual mean haemodynamic response for oxyHb and deoxyHb in the prefrontal cortex. All units in millimoles per liter (mM). Non-MPK = solid gray line and MPK = dotted black line.
Dual-task walking—TWT
Time taken to complete the TWT was lower in the MPK condition for all except participant 4 (Table 2). Results for oxyHb and deoxyHb were varied for the six participants and no consistent pattern was observed (Figure 4).
Trail walk test (TWT)—individual mean haemodynamic response for oxyHb and deoxyHb in the prefrontal cortex. All units in millimoles per liter (mM). Non-MPK = solid gray line and MPK = dotted black line.
Discussion
There is currently little understanding of the effects of transitioning to a microprocessor-controlled prosthetic knee on executive functioning in individuals who have undergone a lower-limb amputation. This study has presented a novel means of assessing changes in executive functioning that may be associated with prosthetic prescription, by recording haemodynamic signals during single and dual-task walking. Results from single-task walking and the dual-task Key Test appear to support the hypothesis of reduced haemodynamic response following a transition to an MPK. The observed decrease in prefrontal cortex activation following transition to an MPK is likely attributable to a reduced need for allocating attention to the task of walking, a reduced postural demand and a more natural gait pattern. 14 Results of this study provide objective physiological measures to support findings of a recent structured review regarding dual-task walking in people with lower limb amputation. This study provided some evidence that use of MPKs improves dual-task performance compared to non-MPKs. 9
The dual-task TWT test produced results with greater variance, and no clear difference in haemodynamic responses could be discerned between the non-MPK and MPK conditions. Interestingly, this is the test where most consistent time differences were observed between the non-MPK and the MPK conditions. The TWT could be considered the most difficult test for the prosthesis users to perform, as it involves identifying numbered cones while performing sharp turning movements. Results in this test may reflect the fact that the task is so complex that neither prosthetic prescription offers measurable cognitive benefits. It should also be recognized that the TWT test was always last to be performed and fatigue may have confounded results. Research has indicated that fatigue can affect the central nervous system and result in a reduction in cortical haemodynamic response. 14
The most reliable indicator of brain activation when using fNIRS is an increase in oxyHb together with a decrease in deoxyHb. 14 In the present study, this pattern of activity was present in some trials, but absent in others, particularly in relation to an observable decrease in deoxyHb. OxyHb has been suggested as the more sensitive parameter and provides good indication of rCBF, but it is also the parameter most susceptible to contamination by physiological artifacts such as pulse, breathing, and so on. An increase in oxyHb without a subsequent decrease in deoxyHb should therefore be interpreted with caution. 14
The limited number of subjects does not allow for group-level analysis. The ability to perform before and after measurements on the same individual was considered a strength of this study however the design, with only one testing occasion for each prosthetic knee does not allow for conclusion to be drawn regarding causation. It is subsequently unclear if the observed changes are due to the prosthetic knee or training that may have occurred in the period between testing occasions. Future research should aim at establishing a stable baseline with repeated measurement before and after transitioning to the MPK. Design of future studies should also include an addition non-MPK period following the MPK period. This would address potential training effects that may have influenced the results.
Limitations
This case-study design included only a limited number of participants and group-level analysis could not be performed. While a minimum of 1-year using a non-MPK was considered sufficient to allow participants to achieve a stable gait pattern, the duration of non-MPK use prior to the first testing occasion varied greatly. The order of testing in this study was not randomized and single-task walking was always followed by the dual-task Key test and finally the dual-task TWT. The testing order cannot be excluded as a potential confounding factor in the results.
It must be acknowledged that the placement of fNIRS probes in this study, guided by fOLD software, 15 is not optimal and does not guarantee accurate identification of specific regions of the brain. This process could be improved by using fMRI or a 3D digitizer with NIRS spatial mapping. Given the relatively crude placement of probes, we chose to average all data channels for our analysis. More valid probe placement methods could allow researchers to divide the channels into more specific regions of interest allowing for a more detailed analysis regarding the areas of the brain most affected by MPK joint prescription.
It should also be acknowledged that fNIRS data can be influenced by motion artifacts, positioning of probes and individual characteristics of the participants. While every attempt was made to standardize the testing procedure, we cannot determine the degree to which these factors have influenced the fNIRS data.
While fNIRS is in its infancy as a tool for measuring brain activity during gait, our study has demonstrated it as a useful technique for use in the rehabilitation setting. Clear differences in patterns of haemodynamic activity in the prefrontal cortex were recorded before, and a minimum of 8 months after, transitioning to a MPK. While results may have been influenced by training that has occurred between the two testing occasions, it is also likely that prosthetic prescription has had an affect on the observed changes in cortical brain activity and suggests that use of MPKs may have a positive effect on limiting the need for executive functioning during single and dual-task gait.
Conclusion
Results of this study suggest that prescription of MPK prosthetic knee joints can reduce demand placed on executive functions during single-task walking and dual-task walking for some individuals. Our results support continued investigation into the role that assistive technology design can have on reducing cognitive loads.
Footnotes
Acknowledgements
The authors wish to thank the study participants.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Össur, Team Olmed and the Promobilia Foundation.