
Abstract
Background:
For individuals with transfemoral amputation, walking with a prosthesis presents challenges to stability and increases the demand on the hip of the prosthetic limb. Increasing age or comorbidities magnify these challenges. Computerized prosthetic knee joints improve stability and efficiency of gait, but are seldom prescribed for less physically capable walkers who may benefit from them.
Objective:
To compare level walking function while wearing a microprocessor-controlled knee (C-Leg Compact) prosthesis to a traditionally prescribed non-microprocessor-controlled knee prosthesis for Medicare Functional Classification Level K-2 walkers.
Study design:
Crossover.
Methods:
Stride characteristics, kinematics, kinetics, and electromyographic activity were recorded in 10 participants while walking with non-microprocessor-controlled knee and Compact prostheses.
Results:
Walking with the Compact produced significant increase in velocity, cadence, stride length, single-limb support, and heel-rise timing compared to walking with the non-microprocessor-controlled knee prosthesis. Hip and thigh extension during late stance improved bilaterally. Ankle dorsiflexion, knee extension, and hip flexion moments of the prosthetic limb were significantly improved.
Conclusions:
Improvements in walking function and stability on the prosthetic limb were demonstrated by the K-2 level walkers when using the C-Leg Compact prosthesis.
Clinical relevance
Understanding the impact of new prosthetic designs on gait mechanics is essential to improve prescription guidelines for deconditioned or older persons with transfemoral amputation. Prosthetic designs that improve stability for safety and walking function have the potential to improve community participation and quality of life.
Introduction
A transfemoral amputation (TFA) presents a major barrier to walking as individuals no longer have direct muscular control of their knee. This diminished muscular support, combined with absent ankle and knee proprioceptive input, threatens stability as body weight loads onto the limb and progresses forward during single-limb support (SLS). As compensation, individuals must learn to use their hip muscles to provide timely control of both the hip and prosthetic knee to prevent the knee from buckling as body weight advances over the prosthetic foot. Without kinesthetic input, the prosthetic knee remains fully extended throughout stance to avoid the potential of falling. 1 Gait is often asymmetrical with decreased loading force on the residual limb and increased loading on the intact limb. 2 Moreover, hip muscle strength is reduced in the prosthetic limb due to loss of distal insertions of the hamstrings, adductor magnus, and tensor fascia lata, necessitating compensatory movements of the trunk and hip to maintain balance and stability during walking. Consequently, for a person with a TFA, prosthetic ambulation requires increased effort (i.e. hip muscle activity and energy consumption) compared to nondisabled individuals.3–5
Advances in prosthetic technology have increased efficiency and mobility for persons with TFA. One of the newer technologies, the C-Leg (Otto Bock HealthCare, Minneapolis, MN, USA) uses microprocessors to control the prosthetic knee during stance and swing. Force transducers within the prosthetic shank and a knee angle sensor record data 50 times per second to adjust valves in the hydraulic knee unit. In stance, the hydraulic forces resist flexion to prevent knee buckling. In swing, the hydraulic forces control the rate of flexion adjusting for variations in terrain and walking speed. Compared to walking with a non-microprocessor-controlled knee (NMPK) prosthesis, using a C-Leg improved walking ability6,7 and speed,7–10 balance and stability,1,9 and ability to traverse ramps and stairs8,10,11 and reduced the number of falls.8,10,11 Biomechanical gait changes with the C-Leg included increased knee flexion angle 1 and moment in stance1,7 and decreased peak knee flexion angle in swing.7,11 The C-Leg’s impact on walking energy consumption, however, was equivocal.11–14
Most studies of microprocessor-controlled knee (MPK) prostheses focused on higher functioning walkers, typically those with traumatic TFAs. For persons who are older, more deconditioned, and often with comorbidities such as diabetes mellitus or peripheral vascular disease, walking with a prosthesis is an even greater challenge.15–17 Although the C-Leg is described as more cost-efficacious than NMPK prostheses when taking into account improved productivity and reduced need for home assistance, its purchase price is still greater than NMPK prostheses. 18 Consequently, insurers have questioned whether individuals with lower walking function and ability to vary speed and cadence would benefit from the more expensive MPK prostheses, particularly the active swing phase control.
The C-Leg Compact (Otto Bock HealthCare, Minneapolis, MN, USA) knee (Compact), one of the newest MPKs, was developed as a less expensive alternative to the C-Leg and differs from the C-Leg in that the microprocessor primarily controls the stance phase of gait. With the C-Leg, there is microprocessor control of the knee hydraulics during both stance and swing. The Compact has microprocessor control during stance only with normal hydraulic control during swing. This prosthesis is designed for persons who can benefit from the stability provided by stance phase MPK, but who may not gain from swing phase MPK (e.g. individuals whose walking speed and variation in cadence are limited). To date, few quantitative analyses of function while using the Compact have been published.19–21 Walking speed on ramp ascent and descent was improved, and knee flexion and ankle dorsiflexion were increased in ramp descent with the Compact compared to an NMPK. 20 The impact of the less expensive Compact on the biomechanics of level walking has not been studied in lower functioning individuals.
Since level walking is a primary locomotor activity for less physically capable persons who have experienced TFAs, the specific aim of this project was to determine to what extent walking with an MPK stance phase prosthesis enhances users’ function during level walking and creates a more efficient, stable, and normal pattern of gait in this population. Our hypotheses were based on expectations of finding similar stance phase benefits in the Compact as have been documented in higher functioning walkers for the C-Leg. Stance phase stability is arguably even more critical for walking in those with lower function as they typically have less muscular reserve and margin for error in the face of threats to balance and stability than higher functioning individuals. Therefore, we hypothesized that compared to the NMPK condition, walking with a Compact MPK stance phase prosthesis would result in (1) faster walking and a longer stride length; (2) improved stance stability on the residual limb as indicated by increased SLS and heel-rise times; (3) a gait pattern with stance phase joint motions, moments, and powers that indicate improved loading of body weight at the knee (increased knee flexion angle, moment, and power absorption in loading) and improved forward progression in late SLS (increased kinematics and kinetics of the hip and ankle in terminal stance and pre-swing); and (4) reduced muscle effort (average percentage maximal voluntary contraction (MVC) electromyography (EMG)) in key remaining muscles in the residual and intact limbs.
Methods
Participants were first tested in their existing NMPK. The knee joint was then converted to an MPK Compact, and the foot was converted to a Compact-compatible foot. The participants then received training in their Compact and a 3-month accommodation period prior to the second laboratory testing session. Training consisted of five to seven 1-h sessions with a physical therapist which included education to enhance each participant’s understanding of the Compact’s capabilities and practice on stairs, ramps, curbs, and uneven surfaces. The study protocol was approved by the Institutional Review Board at Rancho Los Amigos National Rehabilitation Hospital.
Participants
The primary criteria for inclusion into this study included having a unilateral TFA and a classification as a Medicare Functional Classification Level (MFCL) K-2 ambulator as determined by a certified prosthetist. The K-2 classification indicates that the person has the ability or potential to ambulate with the capacity to traverse low-level environmental barriers (e.g. curbs, stairs, and uneven surfaces). These individuals walk at a limited community level and have a limited ability to vary their cadence with a conventional NMPK prosthesis. All participants were independent ambulators with or without an assistive device, over 21 years of age, free of current skin ulceration and had adequate vision to complete all walking tasks and no secondary pathologies that would physically or cognitively limit participation in the study.
Participants were recruited from a prosthetic clinic and support groups in the local area. Participants included 5 men and 5 women with a mean age of 62 years (39–78 years). Six had a TFA of the left lower extremity. The average time since their amputation was 9 years (2.5–21 years). Each signed a Health Insurance Portability and Accountability Act of 1996 (HIPAA) protection of health information form and an informed consent approved by the Institutional Review Board at Rancho Los Amigos National Rehabilitation Center.
Prostheses
Participants first met with the certified prosthetist to ensure that their existing NMPK was optimally adjusted and that the socket fit appropriately. After initial testing in their NMPK, each participant met again with the prosthetist for an initial fitting with the Compact. During the fitting, the Compact knee, shank, and foot were interchanged with the corresponding componentry on the participant’s existing NMPK prosthesis. The prosthetic foot was interchanged with a comparable foot approved for use with the Compact componentry using the manufacturer’s guidelines. The prosthetist chose a foot that most closely matched each subject’s NMPK prosthetic foot in functional performance. The existing socket from the customary prosthesis was reassessed to ensure proper fit and was reused to reduce the potential confounding influence of socket design on walking ability (see Table 1 for NMPK and Compact components). For similar reasons, the same shoe used during assessment with the NMPK was used during fitting and assessment with the Compact. The Otto Bock Laser Posture Alignment system was used to ensure that prosthetic alignment was consistent with the manufacturer’s specifications. An experienced prosthetist with Otto Bock C-Leg Compact certification adjusted the electronic stance settings according to manufacturer’s guidelines with input from the subject and observational gait analysis. Follow-up appointments with the prosthetist were made as needed for further prosthetic adjustments.
Prosthetic components of the NMPK prosthesis foot and knee and the C-Leg Compact prosthesis foot.
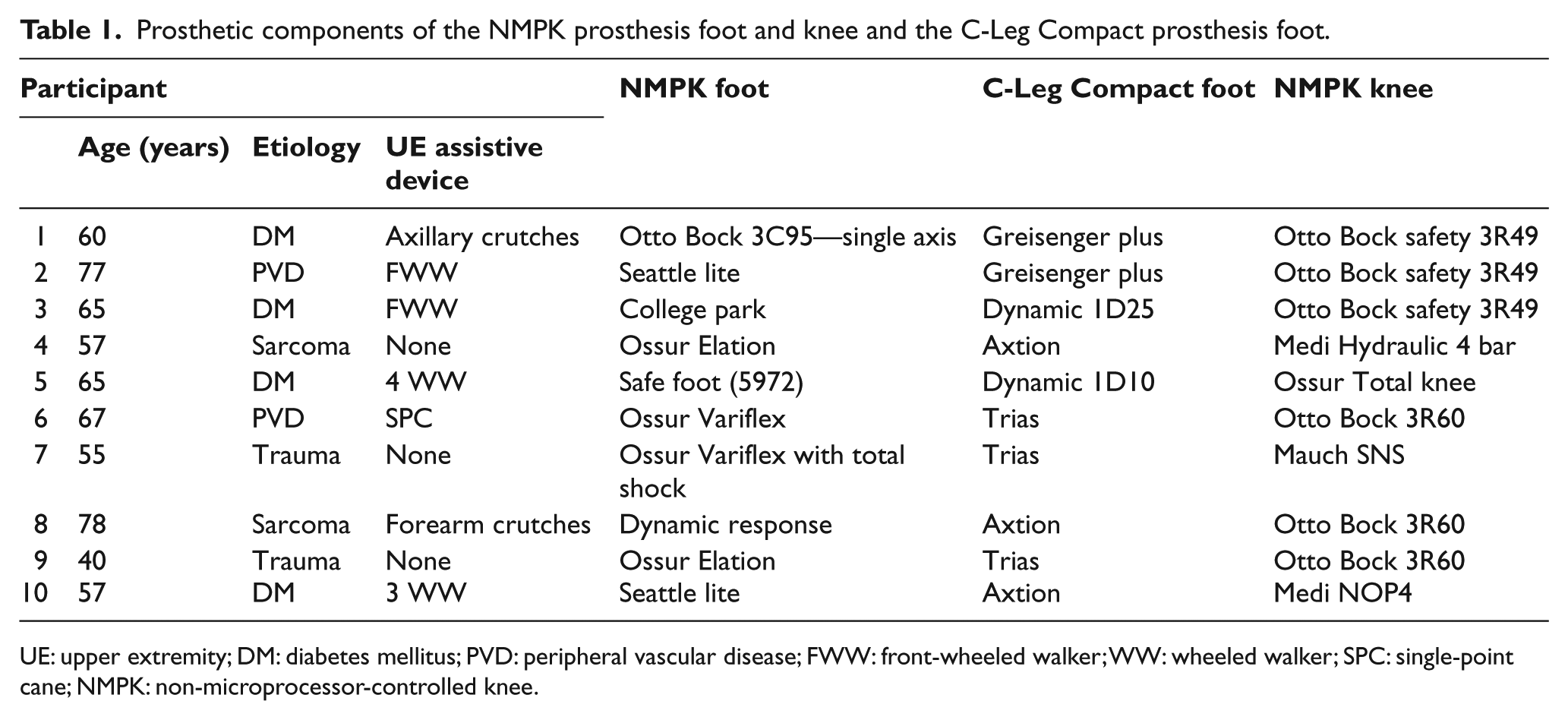
UE: upper extremity; DM: diabetes mellitus; PVD: peripheral vascular disease; FWW: front-wheeled walker; WW: wheeled walker; SPC: single-point cane; NMPK: non-microprocessor-controlled knee.
Procedures
Instrumented gait analysis was conducted in the NMPK and, after training and the accommodation period, in the Compact. Participants walked using their customary upper extremity assistive devices at their self-selected customary walking speed (free) and at a self-selected fast speed. Simultaneous recordings were made of foot–floor contacts, lower extremity kinematics, ground reaction forces, and EMG activity as participants traversed a 10-m walkway with the middle 6 m delineated for data collection by photoelectric beams. Walking was repeated until two successful trials with the participant’s foot landing completely within the force plate were recorded. Any trial that resulted in only part of the foot landing within the force plate was discarded. If an assistive device was used, it was not permitted to contact the force plate. Foot–floor contact patterns were recorded with a Stride Analyzer System (B & L Engineering, Tustin, CA, USA) using compression-closing footswitches taped to the bottom of the participant’s shoes. The procedures were repeated for the contralateral leg.
Kinematics
Three-dimensional (3D) kinematics of the participant’s lower extremities were documented with the VICON motion analysis system (Vicon Motion Systems, Oxford, UK). Greater detail on the kinematic procedures is provided in article by Burnfield et al. 20
Kinetics
Ground reaction forces of both lower extremities during free walking and the residual limb during fast walking were recorded by a force plate embedded in the center of the walkway. Anthropometric measures were obtained for each participant including height, weight, limb segment length, and limb segment circumference. Ground reaction forces were sampled at 2500 Hz with a Kistler force plate (Kistler Instrument Corp., Amherst, NY, USA) imbedded in the walkway.
EMG
Intramuscular EMG was recorded with indwelling, fine-wire electrodes inserted into the belly of eight lower extremity muscles including gluteus medius (GMED) and lower fibers of gluteus maximus (GMAX) of both limbs, iliacus (ILIAC) of the residual limb, and vastus intermedius (VI), soleus (SOL), and tibialis anterior (TA) of the intact limb using the technique of Basmajian and Stecko. 22 Greater detail on the EMG procedures is provided in article by Burnfield et al. 20 EMG was recorded for each muscle at rest to determine the baseline threshold for myoelectric activity and during a 5-s resisted isometric MVC for normalization.
Data analysis
Footswitch data were processed using the EMG-Stride Analyzer Software (B & L Engineering, Tustin, CA, USA). Spatiotemporal parameters (speed, cadence, and stride length) were averaged across two gait trials for each prosthetic test condition. Kinematic data were processed with Adtech Motion Analysis Software (Adtech Inc., Honolulu, HI, USA) to produce 3D trajectories for each marker. The position and orientation of each lower extremity segment were obtained, and lower extremity joint angles for each percent of the gait cycle (GC) were determined with computer algorithms using Euler embedded coordinates. An inverse dynamics model as described by Meglan et al 23 . was utilized to calculate external net joint moments from force, kinematic, and anthropometric data using linear interpolation to allow expression for each 1% of the GC. The external moments indicate that an opposing internal moment from either muscle or passive structures is required to meet the net joint demands. Moments were normalized by body weight and limb length. Motion and kinetic data analysis was limited to the sagittal plane for the hip, knee, and ankle joints. An ensemble average of all strides (2–6) for each prosthetic condition was calculated from the kinematic and kinetic data of each participant. Peak values of ankle, knee, and hip joint motion, moments, and powers were extracted from the ensemble averaged data.
Intensity of EMG activity during walking was determined with the EMG Analyzer Software (B & L Engineering, Tustin, CA, USA). The EMG Analyzer identified the relative intensity of EMG (normalized by manual muscle test value) for each percent of the GC where the intensity was at least 5% of the maximum recorded during the MVC. The average EMG intensity was calculated for each muscle during the time when the intensity exceeded 5% of maximum.
Statistical analysis
Paired t-tests were used to compare the spatiotemporal characteristics, peak values of lower extremity joint motion, moments, and powers, and average intensities of EMG activation during walking when using the NMPK prosthesis to those values during walking with the C-Leg Compact prosthesis. Statistical significance was set at p = 0.05. The analyses were conducted using the SPSS statistical software (SPSS Inc., Chicago, IL, USA).
Results
Spatiotemporal characteristics
Walking speed increased by approximately 20% in the Compact compared to the NMPK in both free (0.66 vs 0.55 m/s; p = 0.002) and fast conditions (0.86 vs 0.69 m/s; p = 0.000; Table 2). This resulted from increases in both stride length (12%–14%; p = 0.003) and cadence (9%–10%; p = 0.001) when walking with the Compact. The percentage of the GC spent in SLS modestly, but statistically significantly, increased on the prosthetic limb with the Compact during free walking (29.3 vs 28.3%; p = 0.048). The duration of heel rise during SLS was markedly increased on the prosthetic limb using the Compact during both free and fast walking (30.1 vs 12.1% SLS; p = 0.033 and 34.7 vs 13.1% SLS; p = 0.019, respectively).
Mean ± standard deviation for spatiotemporal characteristics at self-selected free and fast velocities.
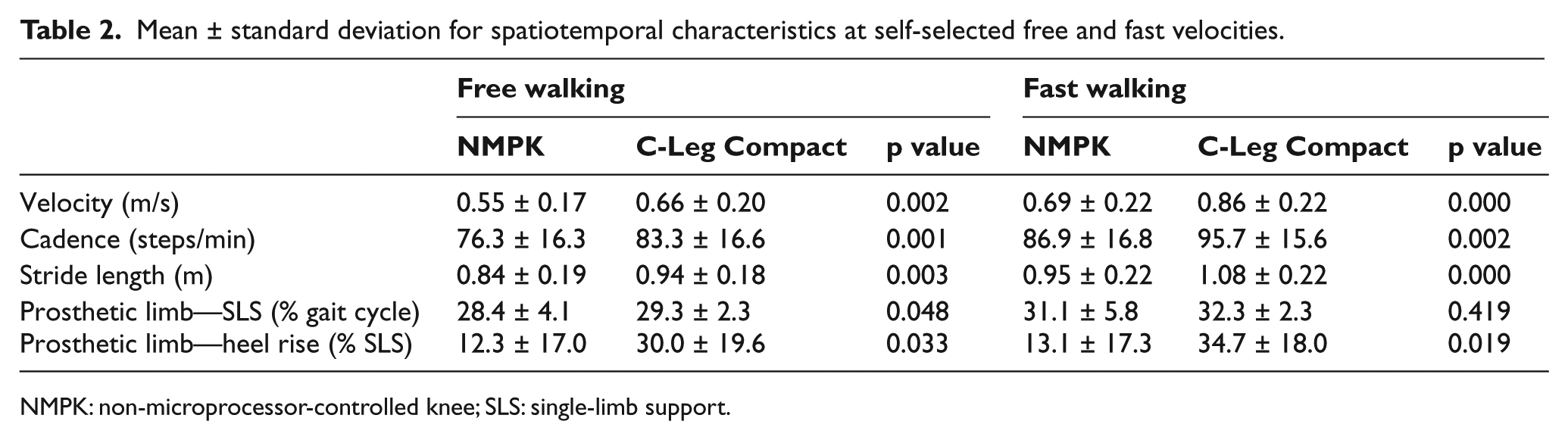
NMPK: non-microprocessor-controlled knee; SLS: single-limb support.
Kinematics
There were no statistically significant differences between prostheses in peak ankle or knee joint angles of either limb during free or fast walking (Figures 1 and 2). Both limbs’ peak thigh and hip extension angles during stance were greater when walking with the Compact compared to the NMPK (p < 0.05). Thigh extension increased by 2°–3° in both limbs, while hip extension increased by 6°–7° in the intact limb and only 2°–3° in the prosthetic limb. These results indicate that anterior tilt of the pelvis was reduced in the Compact during stance in the intact limb but not the prosthetic limb.
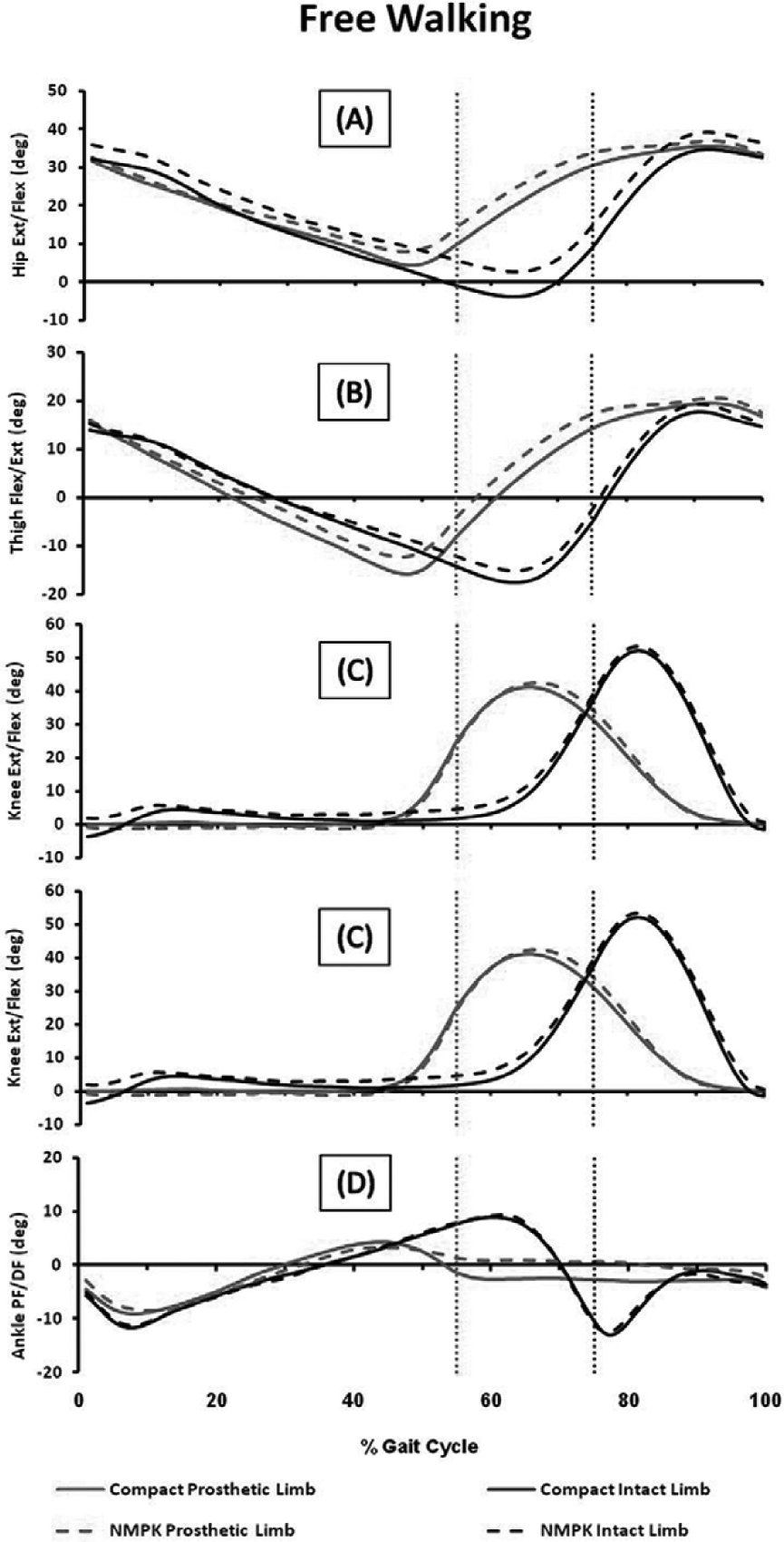
Sagittal plane kinematics of the prosthetic (gray) and intact (black) limbs during free walking wearing the C-Leg Compact (solid line) and NMPK (dashed line) prostheses: (a) peak hip and (b) thigh extension angles during stance were significantly greater when walking with the C-Leg Compact prosthesis compared to the NMPK prosthesis (p < 0.05). No significant differences were found between prostheses in peak angles at the (c) knee or (d) ankle. Dotted vertical line delineates onset of swing for the prosthetic limb (gray) and the intact limb (black).
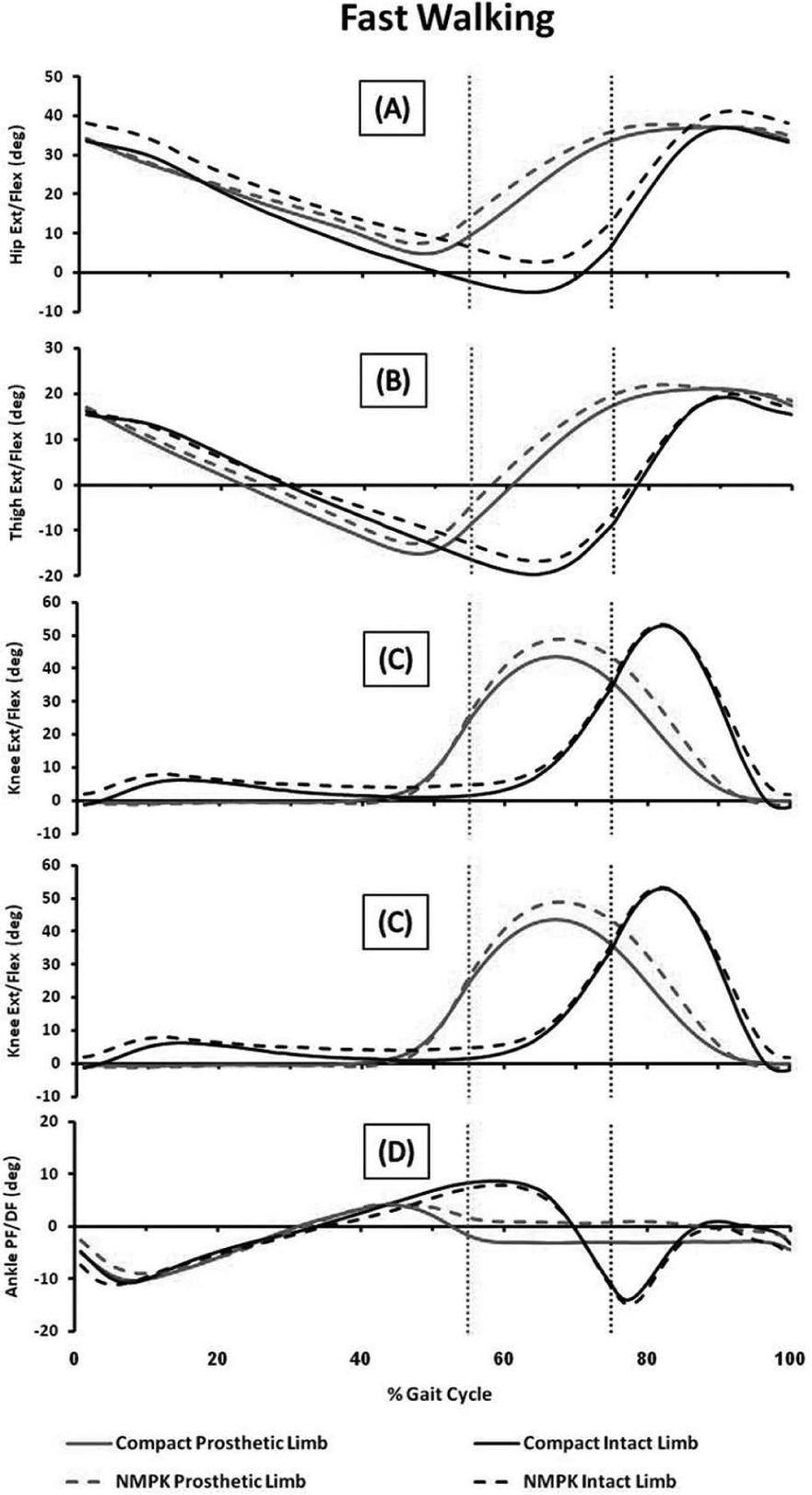
Sagittal plane kinematics of the prosthetic (gray) and intact (black) limbs during fast walking wearing the C-Leg Compact (solid line) and NMPK (dashed line) prostheses: (a) peak hip and (b) thigh extension angles during stance were significantly greater when walking with the C-Leg Compact prosthesis compared to the NMPK prosthesis (p < 0.05). No significant differences were found between prostheses in peak angles at the (c) knee or (d) ankle. Dotted vertical line delineates onset of swing for the prosthetic limb (gray) and the intact limb (black).
Moments
Prosthetic limb
The peak external ankle dorsiflexion moment in late stance increased by more than 20% while walking with the Compact compared to the NMPK during both free (p = 0.001) and fast (p = 0.008) walking (Table 3). During fast walking, the external knee flexion moment in early stance (loading response) was significantly decreased with the Compact compared to the NMPK (p = 0.045), although both values were low compared to the normal range. Walking with the Compact also resulted in a statistically significantly greater external knee extension moment in SLS (mid and terminal stance) during free and fast ambulation (p < 0.05). At the hip, fast walking with the Compact resulted in a significantly greater external flexion moment in early stance compared to the NMPK (0.46 vs 0.29 N m/kg m; p = 0.015).
Mean ± standard deviation for peak moments of the prosthetic limb during self-selected free and fast velocities.
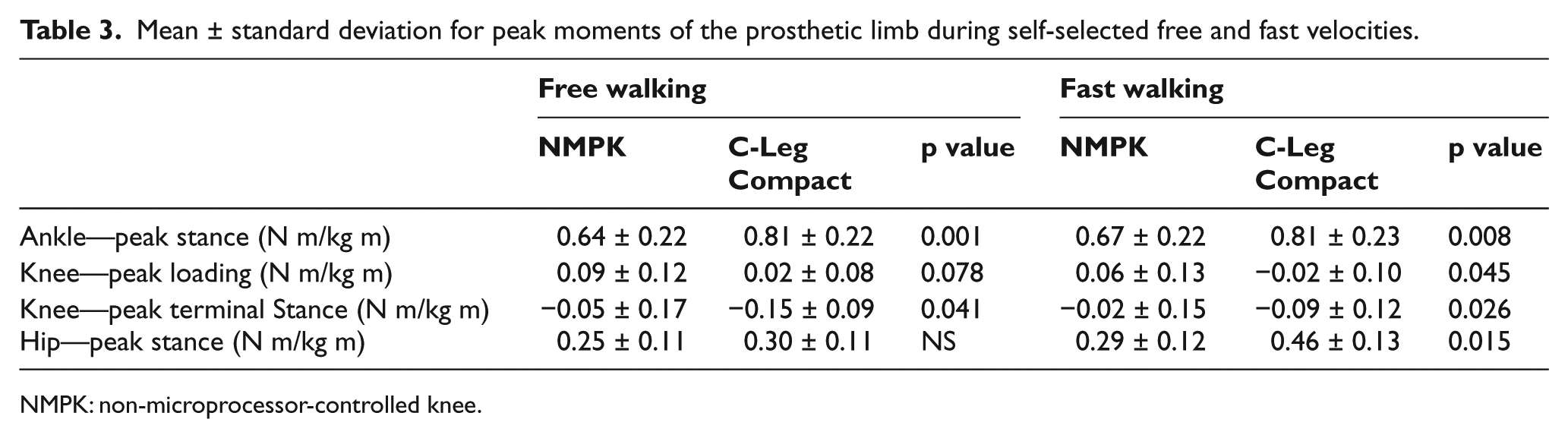
NMPK: non-microprocessor-controlled knee.
Intact limb
We found no statistically significant differences between prostheses in peak external moments at the ankle, knee, or hip joints during free walking. Moments of the intact limb were not recorded during fast walking.
Powers
At the ankle, there was a trend for increased peak power absorption in terminal stance and peak power generation in pre-swing (second, third, and fourth rockers) 24 during free walking and peak power generation in pre-swing during fast walking of the prosthetic limb in the Compact (Table 4). At the hip, fast walking with the Compact produced a 76% increase in peak extensor power absorption during loading of the prosthetic limb (p < 0.05). There was also a trend for increased peak hip power absorption in terminal stance during free walking with both the prosthetic and intact limbs (increases of 45%, p = 0.076, and 50%, p = 0.095, respectively). We found no statistically significant differences between prostheses in peak powers at the knee in either limb during free or fast walking.
Mean ± standard deviation for peak power of the prosthetic limb during self-selected free and fast walking.
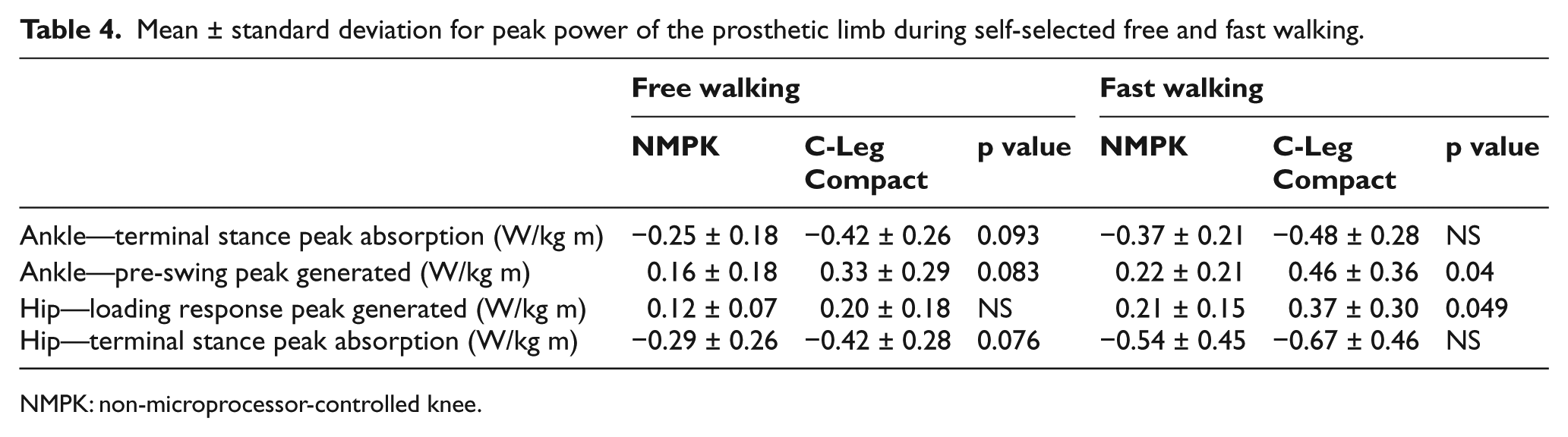
NMPK: non-microprocessor-controlled knee.
Mean EMG
Walking with the Compact produced modestly higher TA activity in the intact limb (6%–8% MVC increase) and moderately more intense lower gluteus maximus (LGMX) activity (19% MVC increase) in the prosthetic limb in both free and fast walking compared to walking with the NMPK (p < 0.05; Table 5). There were no significant differences between the prostheses in mean EMG activity of the remaining muscles during free or fast walking.
Mean ± standard deviation for mean EMG values during self-selected free and fast walking.
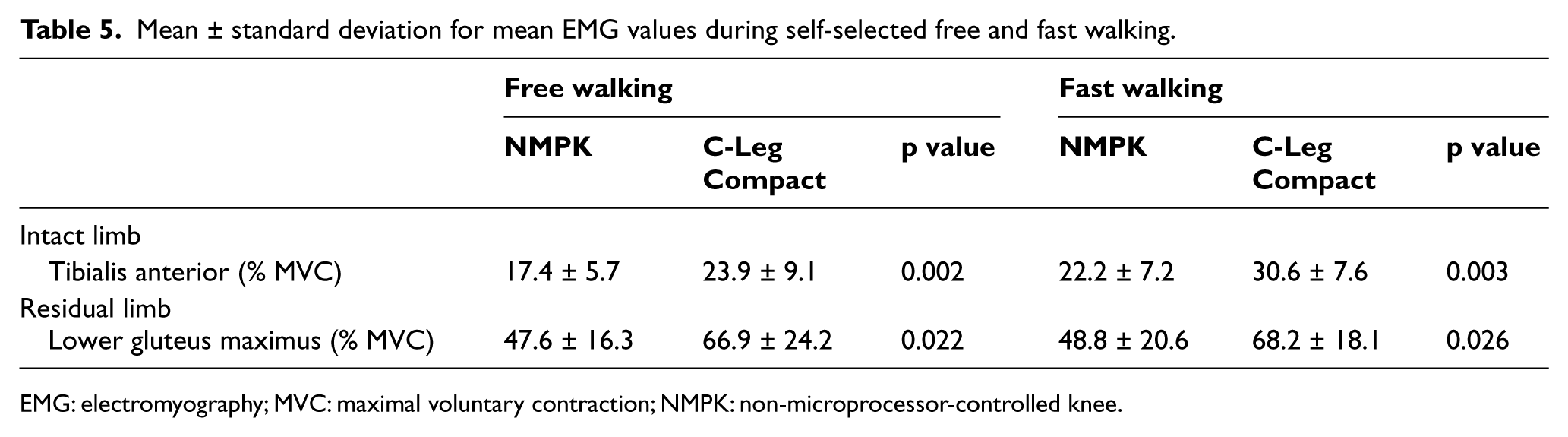
EMG: electromyography; MVC: maximal voluntary contraction; NMPK: non-microprocessor-controlled knee.
Discussion
The MFCL K-2 participants in this study demonstrated significant improvements in level walking with the Compact compared to ambulation with an NMPK. As hypothesized, they walked faster, had a longer stride length, and were more stable as demonstrated by increased time spent on the prosthetic limb during SLS and heel rise when walking with the Compact. This increase in percentage of the GC spent in SLS and heel rise on their prosthetic limb more closely approximated that of their intact limb resulting in greater symmetry. Our participants also were able to increase their cadence when walking with the Compact.
The temporal–spatial improvements in this study are similar to those seen for persons with TFA during level walking while using a C-Leg and for those during ramp descent while using a Compact.7,8,20 Our finding of improved walking stance stability is consistent with previous reports of enhanced function for K-2 walkers during standing activities requiring balance (e.g. hanging out laundry) when wearing a C-Leg or Compact compared to an NMPK. 21 Their finding was stronger, however, in those with high to intermediate walking speeds and activity levels than in lower functioning individuals. Our participants had walking speeds that would have placed them in the lower functioning subgroup demonstrating that the Compact improved stance stability during level walking even for slower K-2 walkers.
Contrary to our hypotheses, we did not find increased knee flexion motion or moments during loading of body weight in the stance phase with the Compact. In fact, the weight acceptance knee flexion moment was actually diminished during fast walking and the SLS knee extension moment was enhanced while using the Compact. Two previous studies that found increased knee flexion moments while walking with the C-Leg had younger (aged 42 and 47 years vs 62 years) and higher functioning participants (K-3-4 level) than those in our study.1,7 Participants in the study by Kaufman and colleagues who demonstrated increased flexion angle and moments also had a longer accommodation period (4.5 vs 3.0 months) than those in our study. Individuals in the study by Segal and colleagues with the same accommodation time as in our study demonstrated a small increase in the knee flexion moment in loading, but not in the knee flexion angle.
The increased walking velocity and stride length with the Compact in our K-2 walkers were obtained primarily by alterations in the biomechanics of the hip. Walking with the Compact produced a significant increase in peak hip power absorption during loading in early stance for the prosthetic limb. In late stance, hip extension motion was increased in both the prosthetic and intact limbs. This was accompanied by statistically significant increases in the peak moments at the ankle and hip and trends for peak power absorption at the hip and ankle during late stance of the prosthetic limb only. The Compact’s resistance to knee flexion in stance improved the body’s forward progression over the prosthetic foot resulting in greater hip extension and a longer heel-off in terminal stance.
Despite improvements in stance stability, we did not find a reduction in intensity of muscle activity in the muscles of either leg with the Compact. In the prosthetic leg, GMAX was actually more active when walking with the Compact than the NMPK. This increased muscle effort is consistent with improvement in the trailing limb posture and increased power absorption seen during terminal stance in the prosthetic limb. Thus, the increased stability allowed improved forward progression, but required increased hip extensor activity to control the increases in hip extensor motion and moment.
In the intact limb, the TA was the only muscle demonstrating an increase in EMG intensity during walking with the Compact. The increased activity was likely due to the increase in walking velocity and the need for more rapid dorsiflexion to ensure foot clearance. More important is the lack of a significant increase in activity of the primary stabilizers of the intact limb as it demonstrates that the intact limb is not working harder with the improvements seen in gait with the Compact. Previous studies have shown an increase in the prevalence of osteoarthritis in the intact limb of persons with amputations.25,26 Our subjects were older and many had comorbidities (e.g. vascular disease and diabetes) that impacted their intact limb and contributed to their decreased mobility. Thus, the ability of our subjects to improve their velocity, stride length, and cadence without increased stress on their intact lower extremity is significant.
Limitations to this study include a small sample size and relatively large intersubject differences for some types of data which may have reduced our statistical power for finding significant differences between prostheses. In addition, the number of variables tested in this study increases the likelihood of type I statistical error, and thus, the results must be viewed with caution. However, inclusion of variables from multiple domains (kinematic, kinetic, and muscle activation) provides evidence regarding the gait parameters associated with improved walking speed with the Compact as well as an indication as to how the changes occurred. Because of a relatively small sample size and low statistical power, correcting for the number of comparisons would be overly conservative and would likely eliminate many valid results along with any type I errors.
Additionally, our participants did not use a standardized NMPK knee joint prior to using the Compact. We chose to test them in their customary prosthesis rather than fit and train them in a new NMPK prosthesis which would require accommodation to two novel prostheses in a relatively short period of time. All participants were tested first in their NMPK prosthesis for this reason also. Moreover, changing the prosthetic foot between the two conditions from their customary foot to a C-Leg Compact-compatible foot may have impacted our results. Schmalz et al. 27 found the advantages of energy-storing prosthetic feet were only significant at higher walking speeds (≥5 km/h). Even the fast velocity of our subjects was far below those speeds. We did not find a significant difference in ankle motion of the prosthetic limb between the two prostheses. The increased ankle moment in the prosthetic limb was more likely the result of increased terminal stance hip extension, stride length, and velocity.
A longer accommodation period may be necessary for persons who are older and more deconditioned. Our participants had used their NMPK for a number of years and may have benefited with more time to adjust to the Compact which required changes in their walking mechanics. Both the NMPK and Compact were aligned by the prosthetist based on the manufacturer’s guidelines with input from the participants. Therefore, the settings may not have been the most efficient but were where the person felt most comfortable and safe.
Conclusion
The participants in this study made significant gains in their walking function when using a microprocessor-controlled stance phase prosthesis. These findings have important clinical implications when considering prosthetic options for more deconditioned or older persons living with a TFA. Individuals with TFAs functioning at a MFCL K-2 walking level may benefit from new prosthetic designs to improve their performance and safety in their environment.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research is funded in part by a grant from Otto Bock HealthCare LP.