
Abstract
Background and aims:
(1) To demonstrate that a 13-year-old male can be successfully fitted with a C-Leg® microprocessor-controlled knee. (2) To use validated outcome measurement tools to assess change in mobility, physical function, fatigue and quality of life after fitting.
Case description and methods:
A 13-year-old unilateral traumatic trans-femoral amputee was studied pre-C-Leg fitting and 2 weeks and 10 months post C-Leg fitting.
Findings and outcomes:
The 6-Minute Walk Test improved by 33% from 360 to 480 m. PedsQL™ Multidimensional Fatigue Scale improved by 32% from 68 to 90, and PedsQL™ Quality of Life Scale improved 14 points, with minimal clinically important difference of 4.36 points.
Conclusion:
In this case, the provision of a microprocessor-controlled knee in the context of a new prosthesis with new socket system produced improvements for the patient in walking speed, fatigue and quality of life.
Clinical relevance
This case report shows that n = 1 methodology can be used to demonstrate clinical improvement in an adolescent subject when using an intervention (C-Leg) which is not supported in this age group by published evidence.
Background
Adolescents are demanding prosthetic users, whose day-to-day activities include participation in school, social activities, physical activity and sport. Physical activity in adolescence improves long-term physical and mental health, contributes to better academic performance and facilitates peer relationships and community integration. 1
Child unilateral trans-femoral amputees (TFA) have higher aerobic demands during gait and slower chosen walking speed compared with able-bodied subjects. 2 The C-Leg® (Otto Bock Healthcare, GmbH Dunderstadt, Germany) decreases oxygen consumption in adults at both typical and fast-paced walking when compared to non-microprocessor-controlled (MP) prosthetic knees. It also results in a statistically significant decrease in the number of steps and time to complete an obstacle course in adult users with a mean age of 46 years (standard deviation (SD) = 13 years). 3 A recent review supports the fact that there is sufficient evidence that the C-Leg has safety, energy-efficiency and cost-effectiveness advantages over non-MP knees, 4 although results for energy efficiency were less conclusive than for safety and cost-effectiveness. We were unable to find published evidence supporting the use of the C-Leg in either children or adolescents.
The aims of this study were:
To demonstrate that a 13-year-old boy can be successfully fitted with a C-Leg MP knee;
To use validated outcome measures to assess change in mobility, physical function, fatigue and quality of life after fitting.
Case description and methods
The subject is a 13-year-old boy who sustained extensive traumatic injuries to his right leg at the age of 11 years and underwent trans-femoral amputation followed by staged debridement of the residual limb and extensive skin grafting. He was left with a bony residuum with poor distal soft tissue cover; the majority of surface area of the residuum was covered in skin graft. Details of the subject and clinical interventions are provided in Table 1.
Timeline and description of rehabilitation management from the time of injury to intervention.
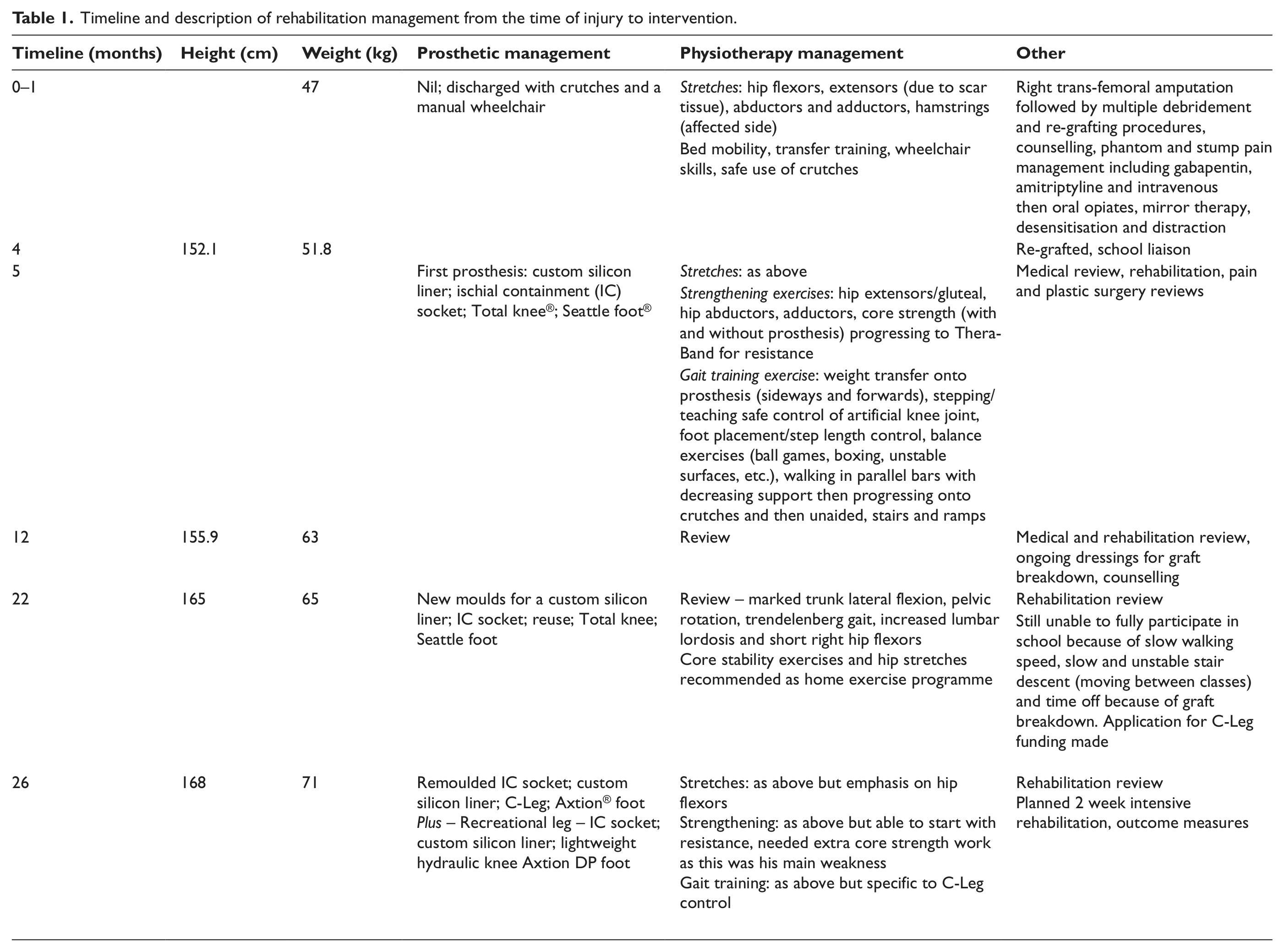
He was fitted with his first prosthesis (ischial containment (IC) socket, custom-made silicon liner with suction suspension, Total knee® and Seattle foot®) 5 months post injury. The delay was due to multiple skin debridement and re-grafting procedures. Phantom pain and adjustment issues lead to difficulties with early management but improved. Phantom pain resolved by 5 months post injury. At 22 months post injury, he was provided with a newly made socket system and custom silicon liner from a new impression due to growth. At 2 years post injury and with regular ongoing rehabilitation, core work, hip flexor stretches, hydrotherapy and gait retraining, the patient was mobilising unaided and able to attend high school full time.
Ongoing issues included frequent breakdown of grafted areas under the socket necessitating time off his prosthesis to rest. He reported problems participating in school, physical and social activities. He needed to leave school classes 5 min early to negotiate the stairs safely without his peers present, was unable to keep up with peers at faster walking pace and during physical activities and had difficulty negotiating uneven surfaces and unpaved walking paths when accessing the local community.
This is a case study with a defined intervention and set of quantitative outcome measures taken before 2 weeks and 10 months after intervention in an A-B design. Outcome measurements chosen were qualitatively, patient’s reported change, and quantitatively, the 6-Minute Walk Test (6MWT) to measure mobility, the Childhood Health Assessment Questionnaire (CHAQ) to measure physical function and activities of daily living, the PedsQL™ Multidimensional Fatigue Scale to measure both physical and cognitive fatigue and the PedsQL™ Quality of Life Inventory as a global measure.
The 6MWT is widely used in clinical practice as an outcome measure, and paediatric normal values are published for British 5 and North American 6 children. The CHAQ is widely used as a functional outcome measure in paediatric rheumatology practice and paediatric musculoskeletal disorders and has been shown to be valid, reliable and sensitive. 7 It measures physical function across a range of activities of daily living and physical activities with a normal score of 3 (no limitation). The 18-item PedsQL™ Multidimensional Fatigue Scale shows good consistency, validity and reliability in a general rheumatology group and normal children.8,9 The PedsQL™ Quality of Life measure is independent of type of impairment and measures health-related quality of life with published normal values available. 10
Ethics approval was obtained from Sydney Children’s Hospitals Network Human Research Ethics Committee this included informed consent from the patient and parent.
The subject was 13 years and 2 months old at the time of fitting the C-Leg with a height of 168 cm, weight of 71.7 kg and body mass index (BMI) of 25.2 kg/m2. The prosthesis was a custom-made carbon fibre socket, custom-made silicon liner with suction suspension, C-Leg and Axtion® foot. A waterproof sports leg for ‘wet’ recreational activities and multiple sports was also provided with the same components except for replacement of the computerised knee with a lightweight hydraulic knee. After fitting, he received rehabilitation (as described in Table 1), but did still have gait deviations after this period.
Findings and outcomes
The subject felt he could walk more confidently following fitting and rehabilitation and reported less skin breakdown. The socket and silicone liner had been remade from new impressions, but his pre-intervention socket was only 5 months old when baseline measurements were taken. He reported that the new leg was ‘100% better than my old leg’. He reported the prosthesis has given him the ability to multitask so that he can mobilise and concentrate on a cognitive task rather than having to concentrate fully on his prosthesis. We observed him walking and texting on his mobile phone with ease, a combination of tasks he was unable to perform on his non-MP knee. Multitasking is a key skill for high school and peer integration, where he needs to mobilise while holding a conversation with peers or concentrate on the game while playing sport. He reported improvement in his walking speed but described the ability to multitask when walking as the most significant gain in function to him. He also reported more confidence in navigating the uneven surfaces in his local community.
The subject had improvements in the quantitative outcome measures (Table 2). The 6MWT distance improved from 360 m to 480 m at 2 weeks post C-Leg fitting and 487 m at 10 months post C-Leg fitting. This is an improvement of 127 m or 33%. His walking speed improved from 60 to 80 m/min.
Outcomes before C-Leg fitting, 2 weeks post C-Leg fitting and 10 months post C-Leg fitting, with published minimally clinically important differences (MCIDs).
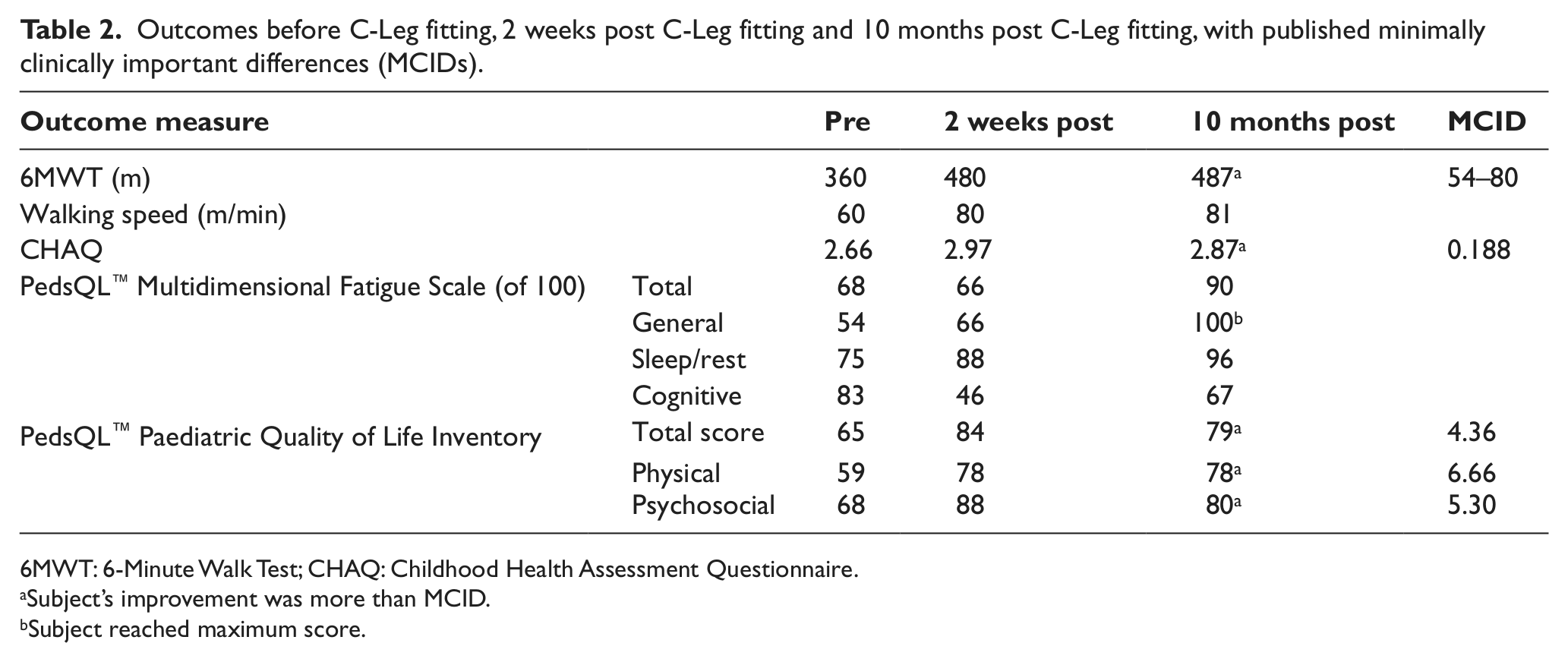
6MWT: 6-Minute Walk Test; CHAQ: Childhood Health Assessment Questionnaire.
Subject’s improvement was more than MCID.
Subject reached maximum score.
The CHAQ score improved from 2.66 before to 2.87 at 10 months. The fatigue score did not change immediately post C-Leg fitting during the period of intensive rehabilitation, but improved from 68/100 pre- and 66/100 2 weeks post C-Leg fitting to 90/100 at 10 months post C-Leg fitting, which is an improvement of 22 points or 32%. Clear improvement occurred in the general (54/100 to 100/100 maximum score) and sleep domains (75/100 to 96/100) with the cognitive domain variable with a substantial initial decrease without a return to baseline.
In clinical practice, it is difficult to achieve substantial quality of life improvements with non-curative interventions; our subject’s score improved from 65 to 84 after 2 weeks and stabilised at 79 after 10 months. This is a 19-point improvement in 2 weeks and a 14-point improvement in 10 months. The physical subscale improved from 59/100 to 78/100 and stabilised, and the psychosocial subscale improved from 68/100 to 80/100 at 10 months. The questionnaire is a 5-point scale from 0 to 4, the largest change in any single item was 2 points with 2-point improvement in walking, pain, feeling low, keeping up with peers and paying attention in class, and 2-point worsening in ‘doing things other teens can do’.
Discussion
This is a single case with patient and assessors unblinded, which will bias the reporting more positively; it would be very difficult and potentially unsafe to blind both patients and treating clinicians to variations in prosthetic knee joints. 4 Although results could be a result of rehabilitation, the patient did receive intensive gait training after his previous prosthesis was fitted, and gait was still suboptimal post C-Leg fitting. The patient was wearing a 5-month-old socket at the time of intervention, which had been made from new impressions, but providing a new socket might have improved comfort immediately after fitting. Our patient had improvements in self-care, cognitive fatigue and quality of life measures over 10 months with a combination of the C-Leg and interdisciplinary team care.
For the 6MWT, we felt that a 33% improvement was clinically significant for our patient. Minimally clinically important difference (MCID) has only been published for adult stroke and geriatric (50-m change) and chronic lung disease patients (54- to 80-m change), 11 and the improvement of 127 m clearly exceeds these values. We could not find any paediatric studies describing MCID for the 6MWT.
The 6MWT distance improved from below the normal range5,6,12 to within the normal range for children 2 years younger, but still below the range reported for 12- to 15-year-olds. 12 This normal group were given instructions to try and score as many metres as possible in the 6 min, which is a deviation from the American Thoracic Society guidelines and would have encouraged the adolescents to go further. 12 Unpublished normal data in 77 children, 4–16 years old, mean age = 9.8 years (SD = 3.4 years), from our own institution were mean distance of 495.9 m (95% confidence interval (CI) = 370.5–621.3 m) (Pin T and Lewis J, Pilot normative study of 2- and 6-MWT for typically developing children and adolescents in Australia, 2012, personal communication).
The subject’s walking speed improved from 60 to 80 m/min, which is comparable to a small group of 5 unilateral TFA, aged 14 ± 2.1 years, who walked at 80 ± 13 m/min, compared to a control group of 21 normal 13- to 18-year olds in the same study, who walked at 77.2 ± 4.17 m/min. Our subject improved from below this study’s control group range (69–86 m/min) to within the normal range, which may translate into improved ability to keep up with normal peers. One other study has demonstrated decreased oxygen consumption 3 and decreased number of steps and time to complete an obstacle course for TFA when using a C-Leg compared to non-MP knees at the same self-selected walking speed. Our subject increased his self-selected walking speed, which may have been due to increased confidence in the stability of the knee as well as decreased oxygen consumption.
Our patient’s CHAQ score was already close to the maximum score of 3, but did improve by 0.21 points; the MCID for CHAQ is 0.188. 13 The only item which changed was running, which he performed ‘with much difficulty’ pre-C-Leg fitting and ‘with some difficulty’ rather than the normal ‘without difficulty’ post C-Leg fitting. This improvement is most likely due to the provision of an additional sports prosthesis rather than the C-Leg.
In terms of fatigue, normal values in 157 healthy children, aged 10–17 years, are mean 82 and interquartile range from 70 to 94. 8 Our patient changed from a low score to a score comparable to the published control group. In adults, the C-Leg reduces oxygen consumption, and this is likely to lead to an immediate improvement in fatigue; over time, increased levels of physical activity would further improve cardiovascular fitness 1 and reduce subjective fatigue.
The MCID for the PedsQL™ measure is 4.36 points for total score, 6.66 for physical subscale and 5.30 for the psychosocial subscale. 14 Our subject has improved more than the MCID on the total score and the subscale scores, a 20% improvement from baseline. A total of 960 normal children aged 5–18 years report mean scores of 79.62 ± 15.26, 9 and our subject’s results are comparable after fitting. A recent review 15 looking at the effect of prosthesis identified three adult studies which used quality of life measures as an outcome, two of the three reported a benefit from MP knees. Kahle demonstrated increased walking speed and a 20% improvement in quality of life on the 36-item short form health survey (SF-36) after fitting a MP knee in 19 adults, similar to our results. Gerzeli compared a group of 50 adult unilateral TFA using a MP knee with 50 gender, age and cause of amputation matched controls; the MP knee group reported significantly better quality of life. Hafner studied 17 adult amputees in a controlled reversal design and found no difference in SF-36 scores after provision of an MP knee; in this study, walking speed did not increase either, and this was the smallest of the studies, so most at risk of bias.
In the future, it would be valuable to have a defined set of validated functional outcome measures for studies of new prosthetic componentry, so a meta-analysis of studies can be performed to give more robust evidence of effectiveness than single studies alone. Validation of adult amputee-specific functional measures in the adolescent population would assist in evaluating the functional outcomes of intervention in this age group.
Conclusion
This case demonstrates that an adolescent can be successfully fitted with a MP knee and that improvements in walking speed, physical function, fatigue and quality of life can be achieved when this is provided in combination with a new socket and liner and interdisciplinary rehabilitation.
Footnotes
Acknowledgements
The authors wish to acknowledge the invaluable skill and expertise Mr David Hughes, Senior Prosthetist provided in this case.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.