
Abstract
Background:
Many people with lower limb loss report the need to concentrate on walking. This may indicate increased reliance on cognitive resources when walking compared to individuals without limb loss.
Objective:
This study quantified changes in walking associated with addition of a concurrent cognitive task in persons with transfemoral amputation using microprocessor knees compared to age- and sex-matched controls.
Study design:
Observational, cross-sectional study.
Methods:
Quantitative motion analysis was used to assess walking under both single-task (walking alone) and dual-task (walking while performing a cognitive task) conditions. Primary outcomes were walking speed, step width, step time asymmetry, and cognitive task response latency and accuracy. Repeated-measures analysis of variance was used to examine the effects of task (single-task and dual-task) and group (transfemoral amputation and control) for each outcome.
Results:
No significant interactions between task and group were observed (all p > 0.11) indicating that a cognitive task did not differentially affect walking between groups. However, walking was slower with wider steps and more asymmetry in people with transfemoral amputation compared to controls under both conditions.
Conclusion:
Although there were significant differences in walking between people with transfemoral amputation and matched controls, the effects of a concurrent cognitive task on walking were similar between groups.
Clinical relevance
The addition of a concurrent task did not differentially affect walking outcomes in people with and without transfemoral amputation. However, compared to people without limb loss, people with transfemoral amputation adopted a conservative walking strategy. This strategy may reduce the need to concentrate on walking but also contributed to notable gait deviations.
Background
Many people with lower limb loss (LLL) report the need to “concentrate on every step.”1,2 This need to concentrate has been associated with a heightened fear of falling in people with LLL. 3 Although modern prostheses can replace physical limb structures, users do not have direct motor control of the prosthesis, nor do they receive direct sensory feedback from peripheral components of the prosthetic limb. As a result, people with LLL may need to concentrate on walking and use cognitive resources to monitor and control movements of the prosthetic limb. The need to concentrate on walking may be greater for those with proximal limb loss levels, such as people with transfemoral amputation (TFA).
Use of cognitive resources during walking can be examined with a dual-task paradigm. In a dual-task paradigm, walking is measured with (dual-task) and without (single-task) performance of a concurrent task to study interactions between cognition and walking. Although the heightened need to concentrate on walking has been identified as a concern by people with LLL,1,2 few studies have applied dual-task paradigms to examine interactions between cognition and walking in people with LLL compared to non-amputee peers.4–6 Comparing people with LLL to peers without amputation is important to understand if, and subsequently how, the need to concentrate on walking differentially impacts mobility in people with LLL. Researchers have previously concluded that addition of a cognitive task did not significantly impact walking in persons with TFA compared to non-amputee control participants.4,5 However, these studies recruited small samples using heterogeneous prosthetic components, which may limit statistical power necessary to detect group differences.
The aim of this study was to quantify changes in walking associated with the addition of a concurrent cognitive task in persons with TFA using standardized microprocessor knee (MPK) components compared to age- and sex-matched controls. Walking over a flat, level surface was assessed through measurement of three critical aspects of walking: walking speed, step width, and step time asymmetry. Additional spatiotemporal measures were examined to further characterize walking. We hypothesized that performance of a concurrent cognitive task while walking would cause declines in the speed, step width, and symmetry in people with LLL, but not in people without limb loss.
Methods
An observational, cross-sectional study was conducted to compare walking performance of participants with TFA to participants without limb loss. Participants were evaluated in a single session at the University of Washington Motion Analysis Laboratory Human Motion Analysis Laboratory.
Participants
Participants with TFA were recruited using posted flyers at local prosthetic clinics and matched-control participants were recruited through flyers and emails. Eligibility criteria common to all participants were as follows: (1) age of 18 years or older; (2) ability to walk without an assistive device for 15 min; (3) ability to ascend and descend ramps and stairs; (4) no diagnosis of medical conditions that affect walking, cognition, or the ability to complete the protocol; and (5) no uncorrected visual or hearing impairment. Additional eligibility criteria for participants with TFA were as follows: (6) unilateral involvement; (7) most recent amputation surgery more than 1 year prior; (8) use of a stable, comfortable prosthesis for at least 3 months; and (9) daily use of a prosthesis with a MPK. Non-amputee (i.e. control) participants were matched to participants with TFA in both age (within 5 years) and sex. This study was conducted with approval from an institutional review board. Participants provided informed consent before beginning the study.
Procedure
A self-report survey was administered to solicit demographic and health information such as age, sex, education, assistive device use, history of falls, and presence of other health conditions. Balance confidence was assessed with the Activities-specific Balance Confidence (ABC) Scale, a self-report measure of perceived confidence in performing daily activities. 7 Cognition was tested using the Montreal Cognitive Assessment (MoCA), a short screening exam for detection of mild cognitive impairment. 8 Participants with TFA were additionally queried about their amputation date and etiology. They were also asked to comment on whether they paid extra attention to walking and to note situations or activities that required attention.
Cognitive task
The cognitive task selected for this study was an auditory analog of the Stroop test, a choice reaction time test. Participants wore a wireless headset (Plantronics Inc., Santa Cruz, CA, USA) that transmitted auditory stimuli (i.e. the words “high” and “low” said in either a high or low pitch) via a Bluetooth adapter (Jabra Corporation, Nashua, NH, USA). Participants were instructed to name the pitch as quickly and accurately as possible after each stimulus. Stimuli were presented every 3 s in blocks of eight. A random delay of 0–1 s occurred prior to each stimulus. Order was randomized and balanced to ensure equal presentation of each stimulus. A multichannel sound mixer (RadioShack, Fort Worth, TX, USA) and custom software (LabView, National Instruments Corporation, Austin, TX, USA) were used to record each stimulus and response for offline processing. Cognitive task performance was assessed in single-task (while participants were seated) and dual-task (while participants were walking) conditions. Participants completed 60 practice stimuli prior to data collection to reduce learning effects. Outcomes used to quantify cognitive task performance were response latency (i.e. the time between the onset of the stimulus and the onset of the response) and response accuracy (i.e. the percentage of correct responses relative to the number of stimuli).
Walking task
Participants walked back and forth at their self-selected speed on an 8.8-m firm, flat surface. Spatiotemporal data were recorded in the middle 4 m of the pathway to minimize the effects of acceleration and deceleration. Walking was assessed in single-task (walking alone) and dual-task (walking while performing the cognitive task) conditions, with two 24-s trials performed in each condition. In the dual-task condition, participants were asked to focus on the cognitive task in an effort to standardize the focus of attention and task prioritization under dual-task conditions. 9
Retroreflective markers were placed on the participants’ trunk (sternum and thorax), pelvis (anterior and posterior superior iliac spines, iliac crests), bilateral arms (acromion, deltoid insertion, lateral epicondyle, mid-lower arm, and wrist), and bilateral legs (trochanter, mid-thigh, patella, lateral knee joint, tibial tubercle, lateral malleolus, posterior heel, and second metatarsal-phalangeal joint). For the prosthetic leg of participants with TFA, markers were placed over the prosthetic socket (trochanter, distal end, and anterolateral socket), knee (prosthetic knee joint, anterior knee, and knee/pylon junction), pylon (pylon/foot junction), and foot (lateral, posterior, and dorsal aspects). Three-dimensional (3D) marker position data were collected at 120 Hz using an 8-camera Qualisys Motion Capture System (Gothenburg, Sweden). Qualisys Track Manager was used to identify markers, interpolate gaps in marker position data (generally <0.25 s long), and truncate trials to data collected in the center of the capture volume, where data quality was optimized. Visual 3D motion analysis software (C-Motion Inc., Rockville, MD, USA) was used to filter marker position data (using a fourth-order, zero-lag, Butterworth low-pass filter with a cutoff of 6 Hz), build link-segment models, label heel strike and toe-off events, and compute spatiotemporal outcomes.
Walking speed, step width, and step time asymmetry were selected as primary outcomes. Walking speed was calculated for each stride as the distance between heel strikes on the same side divided by the time between heel strikes. Step width was calculated as the mediolateral distance between the estimated ankle joint centers at one heel strike and the next heel strike on the opposite side. Step time asymmetry was calculated as the absolute value of the difference between the right and left step times. Other spatiotemporal gait characteristics used to further characterize participants’ gait pattern included stride length (distance between one heel strike to the next on the same side), cadence (number of steps per minute), and step time (described above). Two additional measures of step time variability were explored to assess participants’ gait quality. The first, step time coefficient of variation (COV) has been assessed previously in dual-task research in people with TFA. 4 The second measure of step time variability, based on work by Galna et al., 10 is meant to isolate the construct of variability from associated asymmetry and preserve the original units to improve interpretability.
Statistical analysis
Descriptive analyses were performed for all variables (IBM SPSS Statistics version 19.0, Armonk, NY, USA). Potential differences between groups with respect to participant characteristics (e.g. age and cognitive function) were assessed using paired t-tests. The effect of dual-task performance was examined for each walking and cognitive outcome using a repeated-measures analysis of variance (ANOVA) with one within-subject factor (task: single-task, dual-task) and one between-subject factor (group: TFA, control). The level of significance for all tests was set at α = 0.05.
Results
Participants
Participants with TFA (n = 14) and matched controls (n = 14) were similar with respect to age (p = 1.0), height (p = 0.61), weight (p = 0.71), and number of co-morbid conditions (p = 1.0). People with LLL had significantly lower MoCA (t(26) = −3.31, p = 0.006) and ABC scores (t(26) = −3.72, p = 0.003) and significantly more falls per year (t(26) = 3.07, p = 0.009) (Table 1). All 14 participants with TFA reported the need to pay attention to walking. The most common situations or activities that required attention included walking on icy or slippery surfaces (n = 14, 100%), over uneven terrain (n = 13, 92.9%), down stairs (n = 12, 85.7%), and walking in sand or snow (n = 12, 85.7%).
Participant demographics/characteristics.
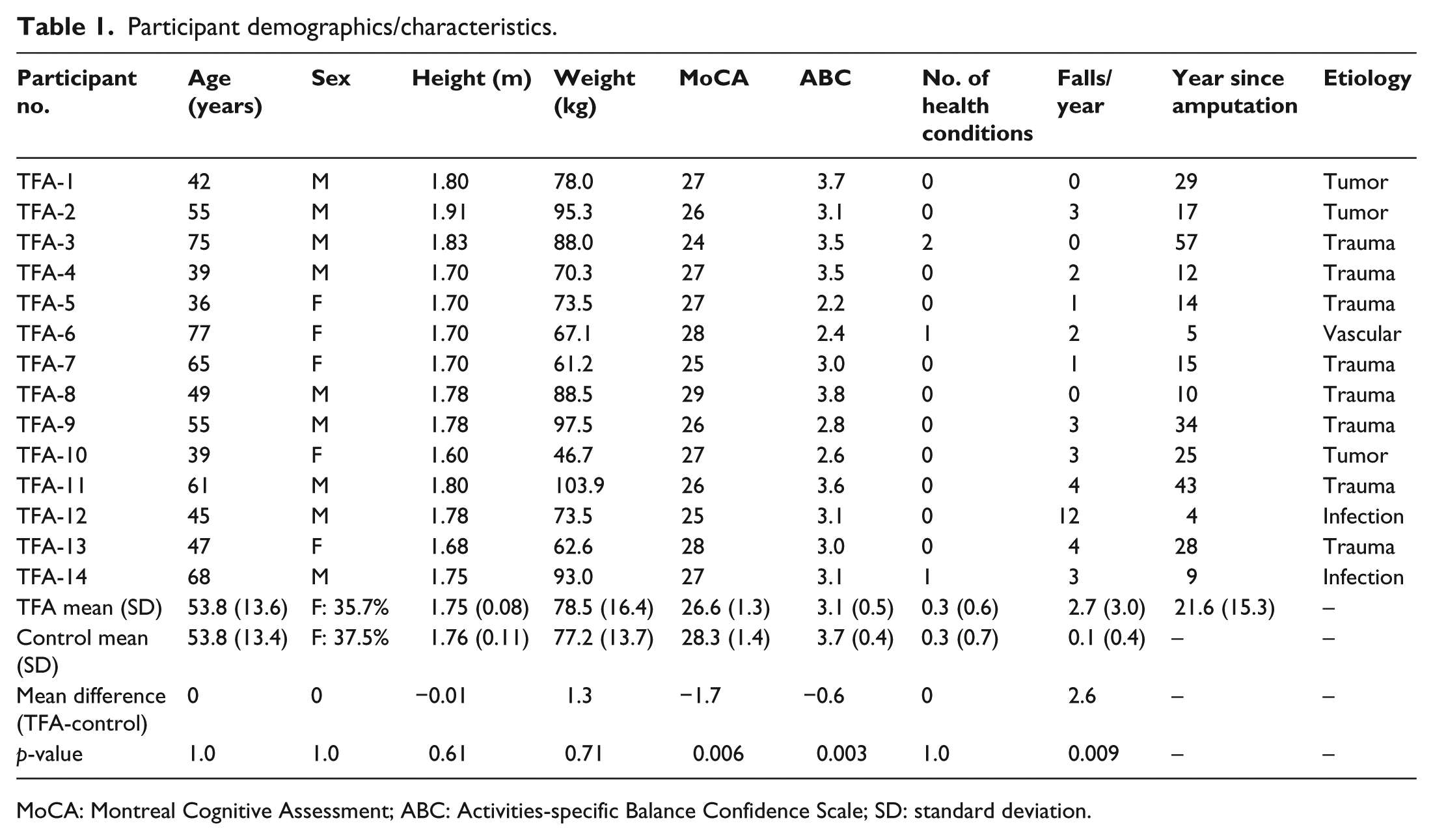
MoCA: Montreal Cognitive Assessment; ABC: Activities-specific Balance Confidence Scale; SD: standard deviation.
All participants with TFA wore an Ottobock MPK (Duderstadt, Germany) with stance and swing control (i.e. C-Leg, Genium, or X2). Participants used suction, seal-in, and pin-locking liners. At the time of the study, participants had used their MPKs for at least 2 years (range 2–9 years). All participants reported that their sockets were well-fitting and that their prostheses were unchanged for the prior 3 months. Fit and alignment of prostheses were optimized by the participants’ individual prosthetists and were not changed for this study.
Cognitive task performance
A significant main effect of task (F(1, 26) = 8.24, p = 0.008) for response latency indicated that both groups had longer response latencies in dual-task compared to single-task conditions. No other significant main effects or interactions were observed for either response latency or response accuracy (all p > 0.05, Table 2).
Mean results and p-values for walking and cognitive measures.
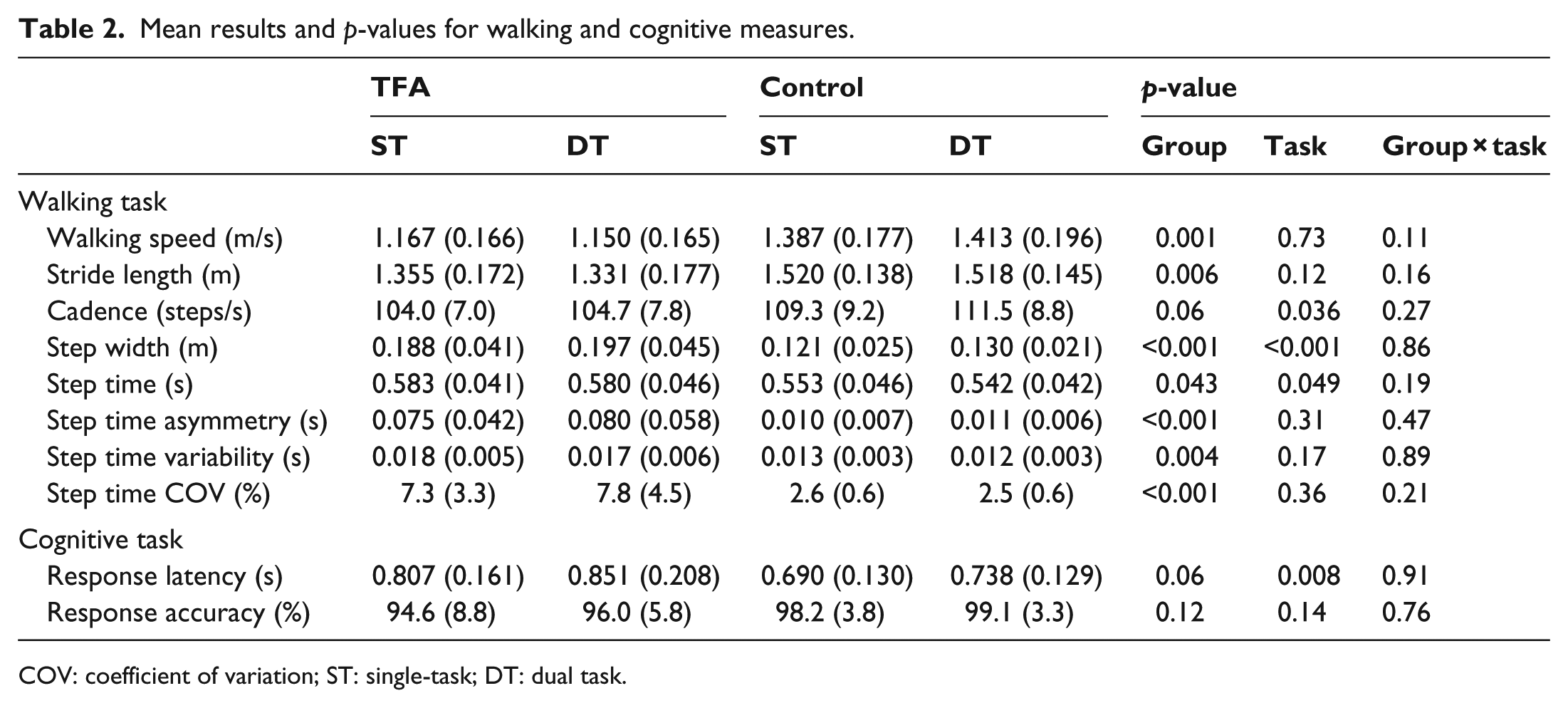
COV: coefficient of variation; ST: single-task; DT: dual task.
Walking performance
An average of 23.1 steps per condition was analyzed for each participant. The number of steps per participant did not significantly differ by group (p = 0.45) or task (p = 0.08). A main effect of group was observed for walking speed (F(1, 26) = 13.65, p = 0.001), step width (F(1, 26) = 27.37, p < 0.001), and step time asymmetry (F(1, 26) = 24.89, p < 0.001), indicating that participants with TFA walked more slowly, with wider steps, and with more asymmetry than control participants under both single- and dual-task conditions. A main effect of task was observed for step width (F(1, 26) = 19.09, p < 0.001), indicating that both groups adopted wider step widths when performing a concurrent task. No significant interactions were observed (all p > 0.11), indicating that the addition of a concurrent cognitive task did not differentially affect walking speed, step width, or step time asymmetry in participants with TFA compared to controls (Table 2; Figure 1).
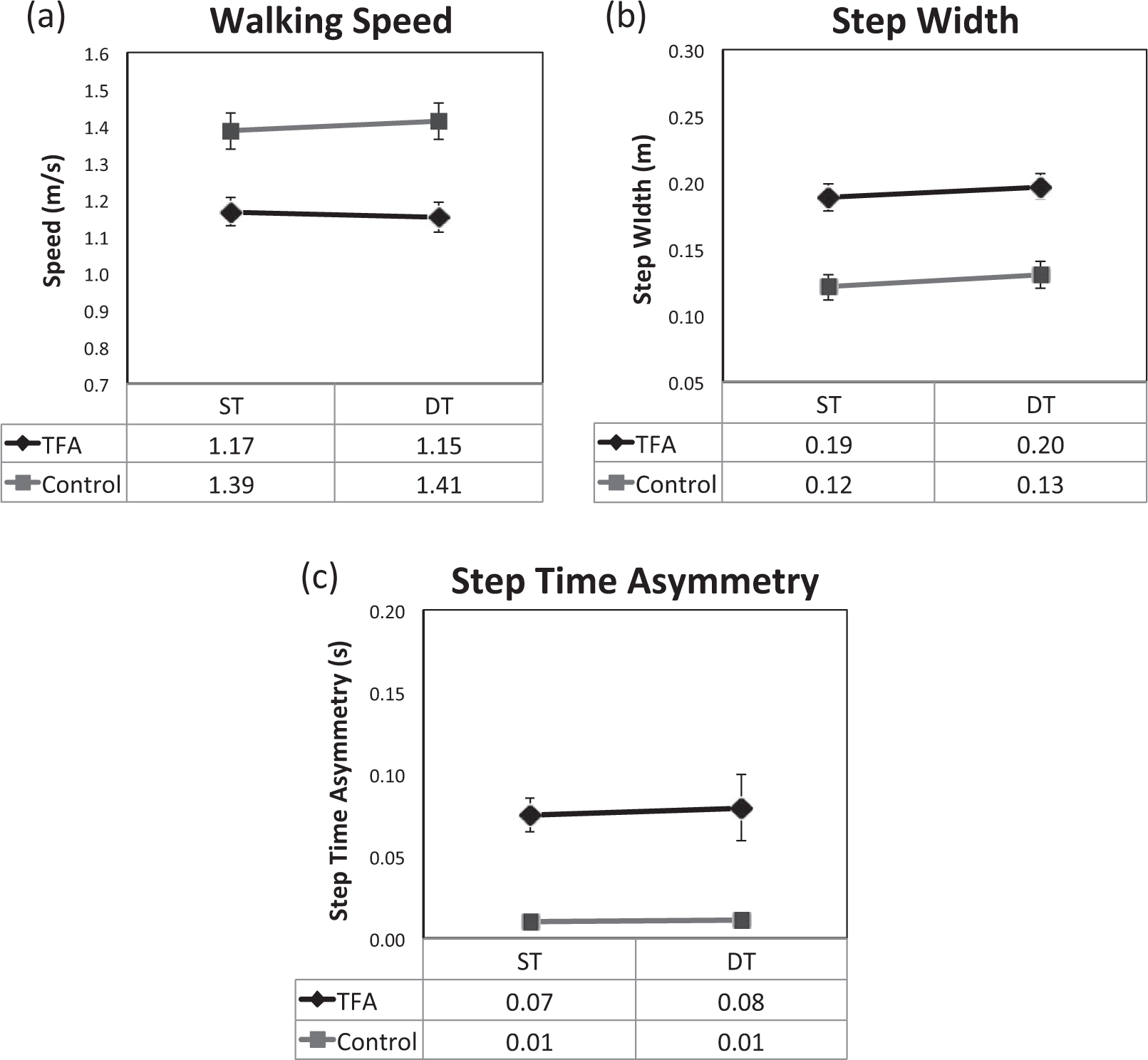
Single- and dual-task (a) walking speed, (b) step width, and (c) step time asymmetry results for both groups. Gray squares represent data for the control group, and black diamonds represent data for the TFA group. Error bars represent standard error.
Secondary walking measures
A main effect of group was observed for most secondary outcomes, including stride length (F(1, 26) = 8.77, p = 0.006), step time (F(1, 26) = 4.52, p < 0.043), step time COV (F(1, 26) = 22.74, p < 0.001), and step time variability (F(1, 26) = 9.77, p = 0.004) indicating that, under both single- and dual-task conditions, participants with TFA walked with shorter stride lengths, shorter step times, and greater variability than controls. In addition, a main effect of task was found for step time (F(1, 26) = 4.26, p = 0.049) and cadence (F(1, 26) = 4.91, p = 0.036) indicating that both groups had shorter step times and higher cadence in dual-task relative to single-task conditions. No other main effects or significant interactions were observed (all p > 0.05), indicating that the addition of a concurrent cognitive task did not differentially affect step length, cadence, step time, or variability measures in participants with TFA compared to controls.
Discussion
The purpose of this study was to compare single-task and dual-task walking between people with TFA using MPKs and controls. We assessed three primary walking outcomes: walking speed, step width, and step time asymmetry. Walking speed is a valid, reliable, and sensitive measure of gait 11 and has been noted to decrease in people with LLL under dual-task conditions. 4 Step width is associated with postural stability in older adults 12 and people with LLL have shown increased step width in response to challenging walking conditions. 13 Step time asymmetry has been used to assess temporal differences between the prosthetic and non-prosthetic sides in people with LLL. 14 Step time asymmetry is often higher in people with TFA compared to non-amputees, 14 and increased asymmetry may reflect, in part, worsening of gait compensations common to prosthesis users (e.g. vaulting and lateral trunk lean). Results suggest that people with TFA walk slower, with larger step widths and greater temporal asymmetry than people without LLL, regardless of whether a concurrent cognitive task is performed. These deficits reflect a gap in walking performance between controls and people with LLL, even those using state-of-the-art prosthetic technology. Differences in performance between groups observed in this study are similar to those reported between people with TFA who use non-microprocessor knee (NMPK) technologies and controls.5,14–18 Contrary to our hypothesis, the addition of a concurrent cognitive task did not differentially impact participants with and without TFA when walking over a firm, level surface.
Similar to these findings, Lamoth et al. 4 demonstrated that addition of a concurrent cognitive task did not differentially affect walking speed, stride time, or spatiotemporal variability in eight people with TFA using various prosthetic knees compared to matched controls. This study aimed to build on this previous research by increasing the sample size and limiting participation to persons using MPKs. MPKs have the potential to improve walking stability through continuous modification of hydraulic knee flexion resistance in stance phase to prevent or ameliorate falls. 19 Previous research suggests that use of MPKs may improve dual-task walking compared to non-MPKs in persons with TFA who are limited community ambulators. 20 In this study, MPK use may have reduced participants’ reliance on cognitive resources when walking over a firm, predictable surface such that the effects of the concurrent task on walking were similar between people with TFA and controls.
People with TFA and matched controls demonstrated similar walking changes when a concurrent task was added. While this might suggest that use of MPKs substantially decreased reliance on cognitive resources, it is important to note that a statistically significant main effect of group was observed for all primary and most secondary gait measures. Differences between groups were observed in both single-task and dual-task conditions, as participants with TFA walked at least 0.2 m/s slower and with steps that were approximately 7 cm wider than controls. Thus, even with use of MPK technology, participants with TFA in our study walked with slow, wide steps, which are indicative of a conservative gait pattern. 21 This pattern may have been adopted by people with TFA as a conscious or unconscious strategy to reduce reliance on cognitive resources when walking, even under single-task conditions. In other words, participants with TFA may preemptively use a conservative walking pattern that reduces postural control demands and minimizes reliance on cognitive resources at the expense of walking performance.
The supposition that groups were differentially impacted by the addition of a concurrent task is supported by participants’ self-report data in this study. All participants with TFA reported that they “pay more attention to walking than those without amputation,” with walking on slippery surfaces, uneven terrain, stairs, sand, and snow most often requiring extra attention. Compared to walking on firm, level surfaces, these walking tasks likely require increased reliance on sensory feedback to maintain stability while walking. In the absence of sensory inputs from the peripheral limb, persons with LLL may need to allocate increased cognitive resources to these walking tasks. Future studies should explore the effect of a concurrent task on challenging walking situations, such as uneven surfaces, that require reactive postural responses to unanticipated perturbations. 22
The results of this study should be considered in the context of the high incidence of people with TFA who report the need to “concentrate on every step.”1,3 In a previous survey study by Gauthier-Gagnon et al., 1 approximately 60% of people with TFA reported “concentrating on every step,” while the remaining 40% reported that “walking has become automatic.” It is possible that eligibility criteria used in this study, such as “ability to walk for 15 min without assistive devices,” may have resulted in a more physically capable sample than those in previous studies. Indeed, Gauthier-Gagnon et al. 1 reported that over 70% of people with TFA in their survey study used canes, crutches, or a walker for locomotion indoors. This suggests a high reliance on such devices in people with TFA, though the use of assistive devices may be less common among people using MPK technology. Thus, our study may have disproportionately represented more functional individuals who are less reliant on cognition for walking over level surfaces.
Limitations
One limitation of this research was that it was conducted in a laboratory, which may not accurately reflect the requirements of mobility in the home or community. In addition, methodological choices such as providing instructions for focus or the choice of cognitive task may also limit generalizability to situations presented in daily life. Further, as noted above, it is possible that participants in this study had higher physical abilities than most people with TFA due to certain eligibility criteria (e.g. ability to walk without assistive devices). Thus, our sample may not reflect the full spectrum of the population of people with TFA.
Conclusion
This study suggests that performance of a concurrent cognitive task affects walking similarly in people with TFA using MPKs and age- and sex-matched controls. However, people with TFA walked more slowly than controls with a wider base of support and greater asymmetry, even under single-task conditions. This gait pattern may reflect a conservative walking strategy that minimizes postural stability demands and the use of cognitive resources to monitor and control walking.
Footnotes
Acknowledgements
The authors would like to thank the following individuals for their assistance with this research: Rebecca Archer for assistance with data collection and processing, Robert Price for engineering support, Dr Marcia Ciol for statistical guidance, Lisa Flexner for providing the cognitive task stimuli, and Drs Deborah Kartin, David Morgenroth, and Patricia Kramer for scientific guidance.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by a Center for Sensorimotor Neural Engineering Seed Grant, a subaward of award number EEC-1028725 from the National Science Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Science Foundation.