
Abstract
Background:
The role of the clinical prosthetist in healthcare has evolved substantially, and it is likely that expectations of the role have changed in recent times. Organisational Role Theory provides a framework for considering the expectations and behaviours of health professionals regarding their functions and roles.
Objectives:
The main objective of this study is to explore stakeholder consensus in role expectations of the clinical prosthetist in an Australian healthcare setting.
Study design:
Cross-sectional survey.
Methods:
The Prosthetist Role Expectations Scale was used to measure expectations and views of the roles of clinical prosthetists. The Prosthetist Role Expectations Scale has 72 items that form 11 subscales that describe prosthetist behaviour. It was distributed to six key stakeholder groups which included: prosthetists, prosthetic technicians, physiotherapists, medical rehabilitation specialists, orthotists and clients with limb loss.
Results:
Of the 1064 surveys distributed, 275 were returned. An additional 35 electronic responses were received, resulting in 299 complete data sets. A high level of consensus across the different stakeholder groups was found for 10 of the 11 subscales. In contrast, there were significant differences between groups for the ‘Independent Prescription’ subscale (p ⩽ .05). Differences in expectations, as noted by individual Prosthetist Role Expectations Scale subscale items (7 of 72) may indicate that stakeholders perceive a prosthetist’s role differently in select areas.
Conclusion:
There was broad agreement in expectations from stakeholders regarding the role of prosthetists in interdisciplinary functioning, research and communication related to prosthetic device provision and function. There were more varied expectations regarding prescription decisions, referral practices and clinician–client communication regarding emotional issues.
Clinical relevance
It is important to understand the expectations that stakeholder groups have regarding the clinical prosthetist role in healthcare settings. Such information can guide health professional education and interprofessional practice and may reduce interpersonal and interprofessional conflict.
Background
The clinical prosthetist is the primary allied health professional responsible for provision of prosthetic devices to clients who experience limb loss. 1 The prosthetic profession originated from trades (e.g. leather and metal) that undertook on-the-job training (i.e. an apprenticeship model of education). This model of prosthetics education was established in Australia until the 1960s, when it transitioned from an apprenticeship model to a tertiary-education model. 2 , 3 Since then, the level of entry-level education has progressively increased from a Diploma to a Bachelor to a Master’s degree. 2 , 3 The level of education has both changed and been changed by the professional expectations of prosthetists among other rehabilitation stakeholders.
Organisational Role Theory 4 provides a framework for considering the expectations and behaviours of health professionals regarding their functions. This theory poses that an individual’s chosen behaviour in the execution of their duties can be influenced by the expectations of that role held by the people they work with, who are known as ‘role-senders’. 4 , 5 For clinical prosthetists, role-senders may include stakeholders such as prosthetic clients, professional colleagues and other medical, nursing and allied health personnel. Official documentation describing a role, such as job descriptions, can be a key source of information informing expectations. However, the process of forming an expectation is subjective and typically filtered through the lens of education and experience. 5 According to Katz and Kahn, 5 problems can arise if role expectations are ambiguous or unclear. This can escalate into direct conflicts concerning a role. Differences in role expectations can also be associated with tension within an organisation and between co-workers or clients. 4 , 5
Little is known about the opinions of different role-sender groups regarding the role of clinical prosthetists. Indentification and comparison of role expectations across stakeholders could reveal any ambiguity concerning the contemporary role of prosthetists. The Prosthetist Role Expectations Scale (PRES) 6 was developed in accordance with the Organisational Role Theory framework. This scale was designed to assess expectations about prosthetics from a wide range of role-senders and to enable comparison of expectations between groups. 6 The purpose of this study was to use the PRES to explore the extent of agreement among stakeholder groups regarding their expectations of the role of the clinical prosthetist. It was hypothesised that views would vary according to the respondent’s professional backgrounds and their experiences with prosthetic services.
Methods
Ethics approval was obtained from the Human Ethics Committee of La Trobe University, Australia, prior to start of the study (FHEC05/161). The PRES scale 6 was chosen and used in this study for examining the opinions of six role-sender groups. These were prosthetists, orthotists, prosthetic technicians, physiotherapists, medical specialists (rehabilitation) and prosthetic clients. These groups were considered to represent health professionals and others who work most frequently with clinical prosthetists. 6 In Australia, medical rehabilitation specialists are doctors who have additional advanced training in the field of rehabilitation. They are the main medical pracitioners for amputees and other rehabilitation clients who require prosthetics.
The PRES scale was developed to assess and characterise the expectations of prosthetists in a clinical environment. It is comprised of a pool of 72 items with 11 behavioural subscales, describing a range of behaviours that could be expected of prosthetist in the context of providing care for clients with limb loss. 6 Response to each item is rated on a 6-point Likert-type scale ranging from ‘very strongly agree’ to ‘very strongly disagree’. There is emerging evidence that the PRES has good content and construct validity, test–retest and inter-rater reliability. 6
Recruitment
Recruitment procedures varied slightly according to each role-sender group and their workplaces. Prosthetic facilities had direct contact with prosthetists, orthotists, technicians and prosthetic clients. Managers of hospital departments and private facilities were also invited to participate, and if they consented, were asked to distribute the survey packages to participants.
Prosthetic clients were recruited via two Australian support groups (‘Limbs4Life’ and The Amputee Association of New South Wales). Limbs4Life mailed hardcopy surveys to people on their mailing list. The Amputee Association of New South Wales advertised the project with an electronic link to the survey via their website. Recruitment of medical rehabilitation specialists and physiotherapists occurred via a public forum and special interest groups such as AUSTPAR. All completed surveys were returned to the research team via a provided paid envelope, facsimile or electronic submission, linked to an electronic version. All participants were informed about the study in an information statement that was included with the survey. They were also advised that return of the survey would be deemed as their consent to participate in the study.
Survey data
All data received from the survey were de-identified in order to preserve the anonymity of participants. Raw data for each participant’s Likert-type scores on each item were recorded in an Excel data spreadsheet. Likert-type scores were assigned a numerical value ranging from one (indicating very strong agreement) to six (indicating very strong disagreement). As per the PRES development study, a mean Likert-type score for each subscale and item was calculated for each role-sender group. 7
Statistical analysis
Each classification on the Likert-type scale was assigned a numeric value (very strongly agree ranked 1, to very strongly disagree ranked 6). Descriptive statistics for each subscale and item were calculated for the different role-sender groups. Categorical data from a Likert-type scale are often analysed using non-parametric tests; however, our data were normallly distributed and suitable for parametric testing. A midline boundary between ‘agree’ and ‘disagree’ on the Likert-type scale was set at 3.5, 6 considering the numerical value of the first Likert-type category was set at one. Mean scores of less than 3.5 were considered to reflect general agreement with item content, whereas scores of 3.5 or greater were considered to reflect general disagreement.
Items or subscales that showed a categorical difference between groups (shown by group mean score on opposing sides of the midline boundary of 3.5) were further analysed for any statistically significant differences. One-way analysis of variance (ANOVA) was applied to determine any significant between-group differences (p ⩽ .05). 8 Subsequently, Tukey’s post hoc tests were performed to examine the separate results for each group. Welch ANOVA was used for analysis of items that violated the assumption of homogeneity of variance. 9
Results
A total of 1064 hardcopy surveys were sent, and 275 returned to researchers within the return date deadline. Of these, 11 were incomplete and not included in further data analysis. Therefore, 264 surveys with complete responses were considered for data analysis, resulting in a 25% response rate from the hardcopy surveys. An additional 35 electronic responses were received, resulting in a total of 299 surveys utilised for data analysis. Response rate according to role-sender grouping is presented in Figure 1.
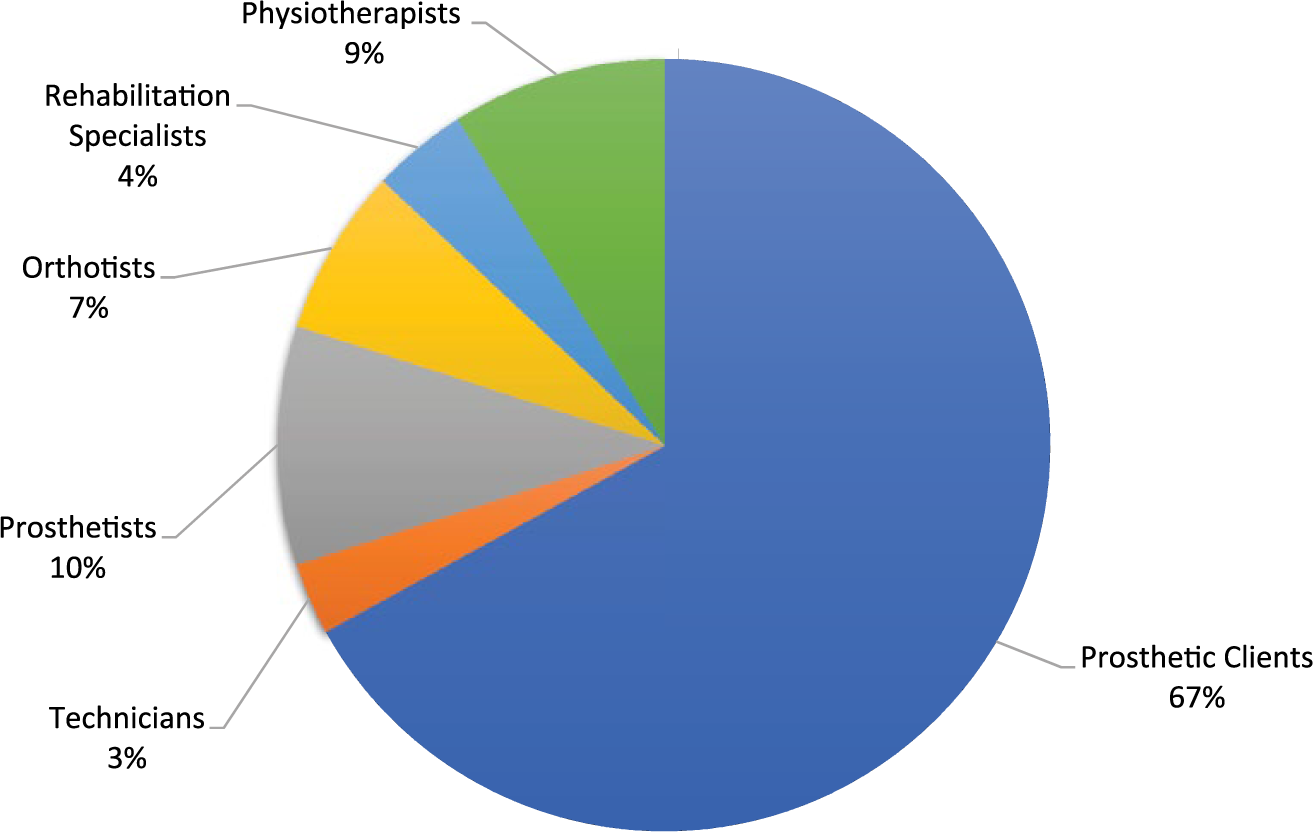
Response rate according to the six role-sender groups.
Descriptive statistics for each subscale of the PRES are presented in Table 1. Ten of the 11 subscales demonstrated mean scores in the ‘agreement zone’. The only exception was for the ‘Independent Prescription’ subscale of the PRES. The medical rehabilitation specialist group showed a mean score of 3.6 for this particular scale, whereas the remaining groups had mean scores of less than 3.5. Further analysis of the ‘Independent Prescription’ subscale showed a statistically significant difference (p ⩽ .05) between the medical rehabilitation specialists and other groups, excepting physiotherapists (Table 2).
Descriptive statistics for each PRES subscale.
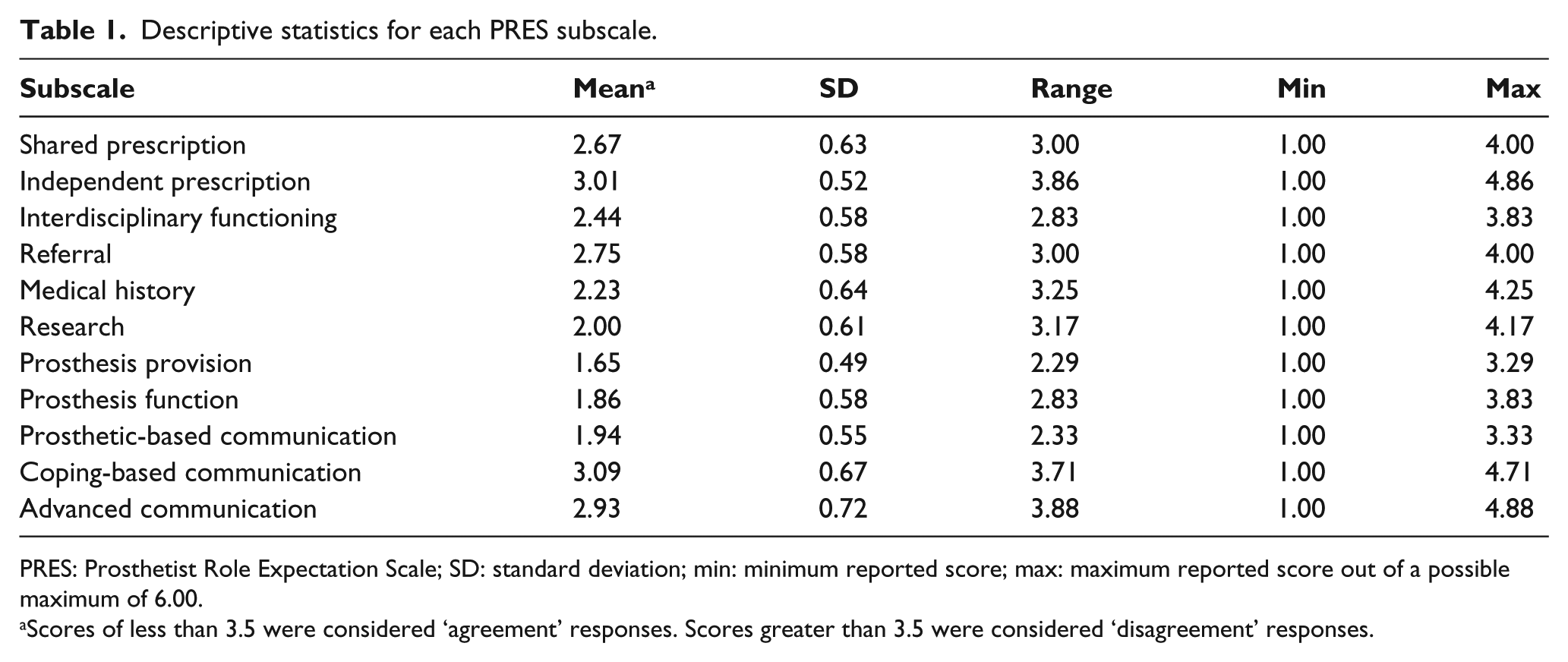
PRES: Prosthetist Role Expectation Scale; SD: standard deviation; min: minimum reported score; max: maximum reported score out of a possible maximum of 6.00.
Scores of less than 3.5 were considered ‘agreement’ responses. Scores greater than 3.5 were considered ‘disagreement’ responses.
ANOVA results and Tukey’s post hoc testing for differences between role-sender groups for the ‘independent prescription’ PRES subscale.
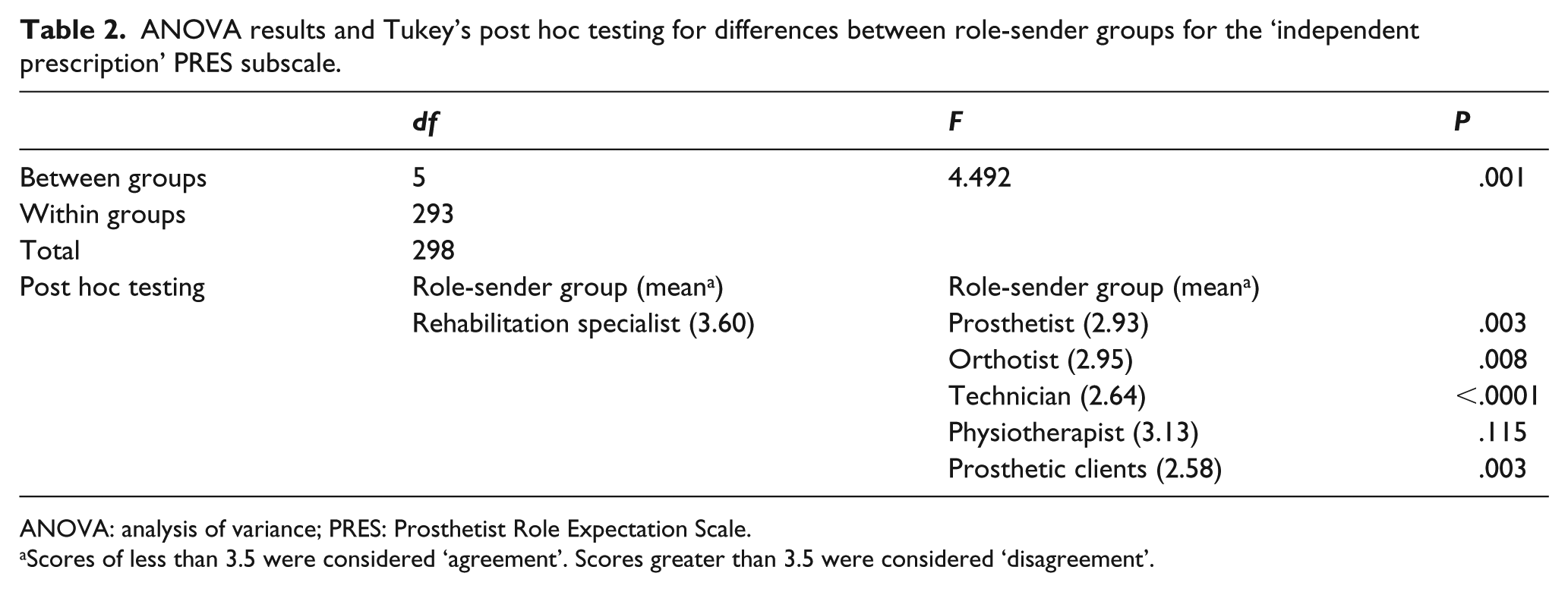
ANOVA: analysis of variance; PRES: Prosthetist Role Expectation Scale.
Scores of less than 3.5 were considered ‘agreement’. Scores greater than 3.5 were considered ‘disagreement’.
Seven items from the independent prescription, shared prescription, referral, adjustment and advanced communication subscales showed mean Likert-type scores that indicated opposing opinions between groups. Four of these items were statistically significant between-group differences (Table 3). Further examination of the mean scores and post hoc tests revealed that the magnitude of differences between the groups varied for each item (Table 4). Descriptive summaries of the four subscales with differences in agreement are presented in the following section.
ANOVA and Welch ANOVA PRES results for individual items indicating a difference in agreement between role-sender groups.
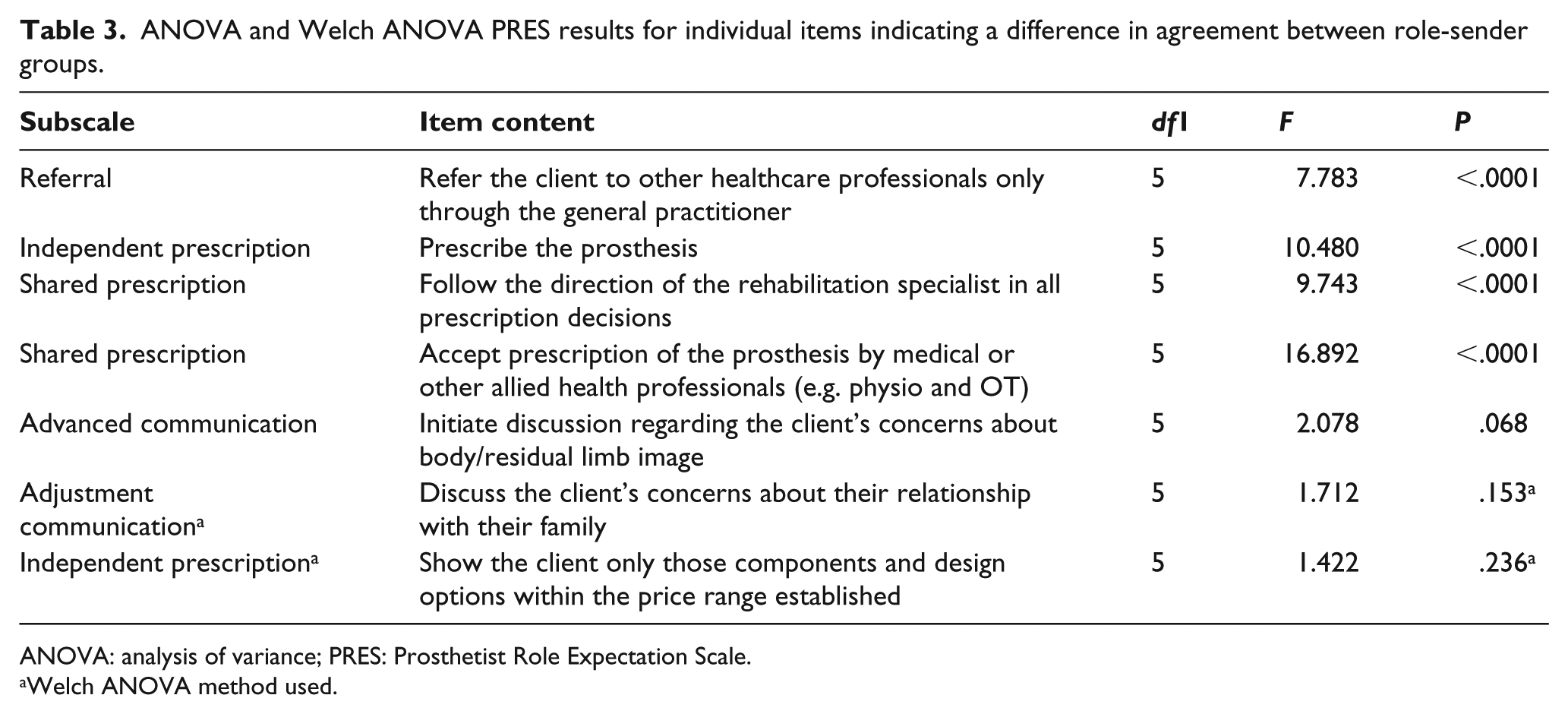
ANOVA: analysis of variance; PRES: Prosthetist Role Expectation Scale.
Welch ANOVA method used.
Tukey’s post hoc results for individual items indicating a difference in agreement between role-sender groups.
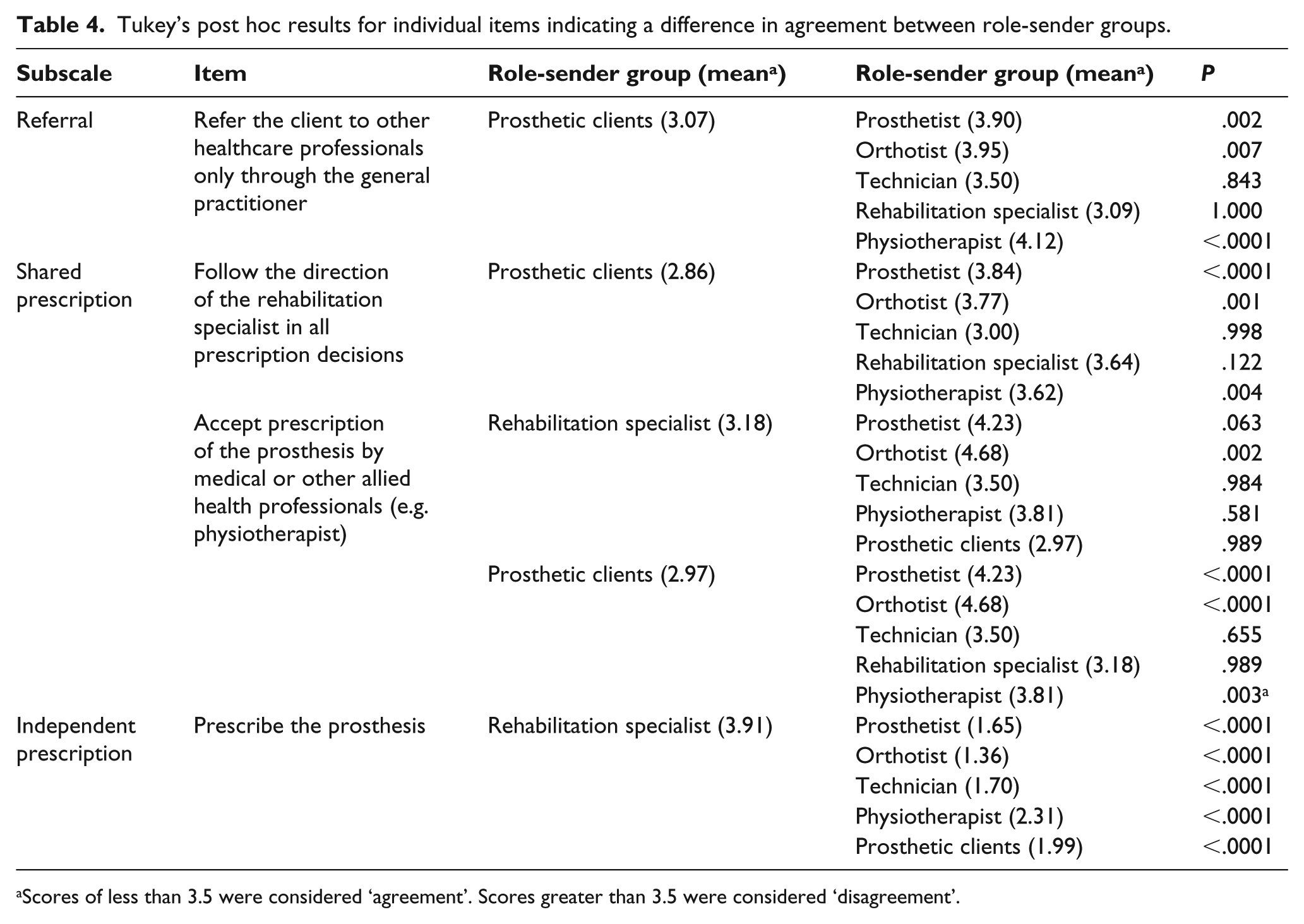
Scores of less than 3.5 were considered ‘agreement’. Scores greater than 3.5 were considered ‘disagreement’.
Independent Prescription Subscale
The respondents in all groups agreed that the prosthetist should advise on optimal length of the residual limb, approve a prosthetic device if another professional has constructed it and should prescribe adjustments to a device following a review appointment. All disagreed that the prosthetist should prescribe prostheses without input from clients or without consultation with other health professionals. All groups (with the exception of technicians) disagreed that the prosthetist should only show the client components and design options within their price range. All groups (with the exception of medical rehabilitation specialists) agreed that the prosthetist should be the main health professional to prescribe the prosthesis.
Shared Prescription Subscale
When making shared decisions, all groups agreed the prosthetist should consider the client’s views, seek input from the multidisciplinary team and prescribe the device following consultation with a medical rehabilitation specialist. Prosthetic clients and technicians agreed that the prosthetist should ‘follow the direction of the rehabilitation specialist in all prescription decisions’. The remaining role-sender groups disagreed. Likewise, the prosthetic client and medical rehabilitation specialist groups agreed that the prosthetist should ‘accept prescription of the prosthesis by medical or other allied health professionals’. All other respondent groups did not agree with this statement.
Referral Subscale
All groups agreed that the prosthetist should have the appropriate skill-set to determine when referral to mental-health services is indicated. They should also organise experienced clients to speak to individuals before amputation. All agreed that a prosthetist should ‘refer directly to a psychologist if a client presented as not coping following surgery’. Everyone agreed that prosthetists should refer the client to the community-based general medical practitioner for all non-prosthetic concerns. They also agreed that the prosthetist should refer directly to other health professionals for non-prosthetic concerns. The medical rehabilitation specialists and prosthetic clients concurred that referral to other professionals should ‘only take place through the general practitioner’, whereas the remaining groups disagreed with this statement.
Adjustment Communication Subscale
There was consensus that the prosthetist should discuss client-raised concerns regarding feelings of depression and not change the topic if a client-initiated conversation about emotional issues. They concurred that the prosthetist should discuss the client’s concerns regarding how they are coping following amputation in areas such as returning to work and the response of families and friends to amputation. The prosthetic clients, physiotherapists and medical specialists generally disagreed that prosthetists should extend discussion to their ‘client’s concerns regarding their relationship with their family’. The other role-sender groups agreed with this statement.
Advanced Communication Subscale
All groups reported that the prosthetist should competently use verbal and non-verbal communication techniques, active listening and empathy for a client’s expressed concerns. All agreed that prosthetists should ‘actively assist the client to identify issues in need of clinical assistance or discussion’. They also concurred that the prosthetist should ‘not initiate a discussion of deep emotional issues’, ‘explore the grief process with the client’ or ‘encourage a client to speak honestly about the impact of amputation on their sexuality’. There were divergent opinions regarding whether prosthetists should ‘initiate discussion regarding the client’s concerns about body image’. Medical rehabilitation specialists and physiotherapist groups disagreed, whereas the remaining groups agreed that the prosthetist should initiate discussion of this topic.
Discussion
This investigation showed that prosthetists, prosthetic technicians, physiotherapists, medical rehabilitation specialists, orthotists and prosthetic clients generally agreed on the roles and expectations of prosthetists in clinical practice. The PRES results also revealed broad agreement regarding the prosthest role in interdisciplinary functioning, research and activities related directly to device provision and function. This was consistent with the description of the role in the published literature. 1 ,10–12 There were a small number of areas of disagreement between groups in the role of prosthestists. These related to prescription decisions, referral practices and clinical communications concerning sensitive client issues.
The difference in opinion regarding prescription decisions might be related to the traditional use of the term ‘prescription’ in a health context, which has been historically linked to a medical practitioner’s direct instruction, usually provided in writing. This term can also be used more broadly as an action of directive or authoritative decision-making. 13 The term ‘prescription’ appears widely in literature regarding the role of prosthetist, with and without specific reference to a medical practitioner’s written instructions and involvement. 1 , 10 , 11 , 14 , 15 Internationally, the American Board for certification in Orthotics, Prosthetics and Pedorthics Inc. 16 recommended that a prosthetist ‘must receive a prescription from a physician before providing any orthosis, prosthesis or pedorthic device to a patient’. The International Society for Prosthetics and Orthotics (ISPO) 11 advised that the prosthetist ‘takes part’ in prescription, whereas the British Association of Prosthetists and Orthotists (BAPO) 17 identified the prosthetist’s role in the context of ‘design’ and ‘provision’, and also make recommendations for prescription in their the Prosthetic Best Practice Guidelines. 14
Broader use of terminology pertaining to prosthetics may be reflective of the evolution of the role 18 , 19 and subsequent expectations in this area. Nevertheless, the variation in terms and resultant interpretation of the terminology could be a challenge to role-senders when shaping their expectations of the role of the clinical prosthetist. Overall, the respondents advised that prescriptive decision-making should be a consultative process. In addition, the prosthetist has the broadest expertise when advising on prosthetic device design. This differs from the historical, medically led model for prosthetics prescription captured by Blocka: 19 In the past, the medical specialist (orthopaedic surgeon or medical rehabilitation specialist) was the main head of the rehabilitation team and prescribed the orthosis or prosthesis and was the main director of care over other professionals involved. 19
The PRES results indicated that allied health professionals (prosthetists, orthotists and physiotherapists) were supportive of the prosthetist exercising independent prescription decisions, whereas the medical specialists (and to a lesser extent, prosthetic clients) held more medically led expectations. 19 One of the limitations of this study was that the PRES was not able to determine if the variance in results was due to role ambiguity associated with the prescription language or differences in held views.
Regarding referral practices, clinicians agreed that one element of the prosthetist’s role should be to make independent referral to other health professionals. This reflects referral practice in the Australian Competency Standards, 10 which cite the importance of referral to a range of health professionals. In contrast, the prosthetic clients and medical rehabilitation specialists often expected a medical practitioner to be involved in referral. These expectations are more in keeping with the earlier editions of the Australian Competency Standards 10 , 12 which make specific mention of the general medical practitioner in referral. 12 Given the diversity of prosthetic work environments in Australia, variations in referral pathways are likely.
The different stakeholder groups had a range of opinions regarding how a prosthetist should communicate with the client regarding sensitive emotional issues. Adjustment to amputation is multifaceted and subjective. The literature indicates that many clients are likely to experience some emotional distress or strain, especially in the early stages. 20 Due to the long-term nature of prosthetic management, it is likely that prosthetists work and communicate with clients experiencing some psychosocial distress, with the potential for further referral for therapeutic support.
The PRES included two subscales designed to explore prosthetist’s behaviours related to a client’s psychosocial concerns. The role-senders agreed that prosthetists should competently engage in client-initiated, concern-specific discussion with a communication skill-set sophisticated enough to recognise when a client is in need of psychosocial assistance. The respondents also agreed that it was important for the prosthetist to sensitively discuss concerns with their client and refer accordingly.
Value statements from educational and professional organisations agreed with this description of the communication skill-set. 10 However, the PRES results showed that many respondents were uncertain where professional boundaries lie when discussing sensitive personal issues. This was shown by disagreement between groups for some items, such as body image, and variation for items with similar themes (interpersonal relationship concerns). Evidence of the complexity of this issue was also evident in two opposing statements from PRES prosthetic client respondents; ‘Social/ psychology issues should be left alone. The prosthetist’s role should be to ensure the best limb is supplied’ and ‘I can talk about anything with my prosthetist and generally do’.
Literature concerning client–clinician communication can be classified into two general areas. These are (1) demonstration of specific communication skills (e.g. active listening and body language) and (2) value statements describing communication as a lens by which the skills should be executed (e.g. ‘He or she shall provide services to patients in a professional manner’). The latter presents a challenge from the perspective of Organisational Role Theory 4 as value statements can be highly subjective in their interpretation by the individual. What might be considered ‘professional’ by one person may not be perceived as such by a client. The PRES results indicated that expectations of a clinical prosthetist’s communication skill varied among different role-senders and sometimes lacked clarity surrounding specific sensitive issues.
While this study can provide first insights into current expectations of the role of the clinical prosthetist in Australia, it has some limitations. The degree of representation of each group from each state within Australia was variable; therefore, it is not possible to generalise the results nationally or internationally. In addition, the inclusion of a wider range of role-senders may have resulted in a richer data-set and captured the expectations of those outside the intended six groups. Regular application (every 5–8 years), analysis and publication of the PRES would assist the professional community to better understand the current expectations of their role. Another limitation was that the categorisation of ‘agreement’ or ‘disagreement’ on the PRES was based on group average data, and not the opinions of individuals.
Conclusion
The first Australia-wide application of the PRES showed many areas of agreement between different stakeholder groups regarding the current expectations of the role of the clinical prosthetist. It was agreed that clinical prosthetists have major roles in interprofessional teamwork, research and communication associated with device provision and function. Differing expectations between groups were found for a small number of issues related to prescription decisions, referral practices and clinician–client communication concerning sensitive emotional issues.
Footnotes
Author contribution
RLM, GM and MEM conceptualised and designed the study. RLM and GM were involved in data colleciton and RLM conducted the data analysis. RLM and APB contributed to writing the first draft manuscript. All authors reviewed and contributed to revisions and approved the final manuscript.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. However, the authors are from the same institution as the Editor-in-Chief of the Prosthetics and Orthotics International journal.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.