
Abstract
Introduction:
In trans-tibial prosthetics, shape-capture methods are employed to create a representation of the residuum. Shape-capture methods can be grouped into the categories of ‘hands-on’, ‘hands-off’ and computer-aided design.
Objective:
This review examines the influences and trends of shape-capture methods on the outcomes of quality, comfort of user and clinical efficiency, in the population of trans-tibial prosthesis users.
Study Design:
Systematic Review
Method:
Databases and relevant journals were searched. Participants included trans-tibial prosthetics users/limb models. Interventions included shape-capture methods. Outcomes included quality, comfort of user and clinical efficiency.
Results:
Overall, 22 papers were evaluated; 8 papers evaluated hands-on and hands-off methods, 2 evaluated computer-aided design and 12 evaluated measurement systems used with shape capture. No papers relating to clinical efficiency were found.
Conclusion:
Overall evidence was weak in suggesting that effects on outcomes were due to the sole influences of shape capture. However, studies suggest that hands-on methods are dependent on a prosthetist’s skill. Hands-off methods, although repeatable, might still require experience to attain a good fit. Computer-aided design studies were mostly done on theoretical models. Shape-capture measurements require more consistent ‘gold standards’. The relation between socket fit and comfort is still unclear. Overall, more research is required in each area.
Clinical relevance
A good fitting prosthetic socket is crucial for efficient and comfortable use of a prosthesis. To attain the best chances of a good fit, it is important that the characteristics of the residuum are captured as accurately as possible during the initial “shape capture” stage. This paper attempts to categorize and evaluate the existing shape capture methods on their influence and trends on various outcomes - Quality of shape capture, comfort of user and clinical efficiency.
Keywords
Introduction
Background
In a trans-tibial prosthesis, the socket works as a mechanical coupling between the human body and the prosthetic limb. To allow for efficient and comfortable use of the prosthesis, it is crucial to attain a good fit of the socket. The production and fitting of a socket occur over four main stages – shape capture, modification, fabrication and alignment. The stages are intimately linked, with the previous stage influencing subsequent ones. Due to this close relation, errors made in the overall process could be cumulative. Hence, it is important that the shape of the residuum is captured as accurately as possible to obtain the best chance of a good fit.1–5
Optimal socket fit
In 1995, Klasson 6 mentioned three criteria for a good fitting socket:
The mechanical coupling between the skeleton and the prosthesis is to be as stiff as possible;
No tissue damage;
Minimum discomfort to the user.
A stiff mechanical coupling would allow for minimal residuum displacement and effective transfer of forces during weight bearing. This was acknowledged by Lilja and Oberg, 7 who stated that high stiffness improves proprioception and prosthetic function. To attain a stiff coupling, skeletal structures in the residuum would need to be stabilised within compressed soft tissue. Soft tissue compression should occur naturally under load and not through manual deformation in specific areas. This would aim to provide a uniform pressure distribution around the residuum, which would minimise tissue damage and discomfort. 6 Klasson’s opinions resonated with those of Kahle, 8 who agreed that a uniform pressure distribution would minimise skin breakdown.
Klasson also suggested that modification of the captured shape should be kept to a minimum as it is an unquantifiable and unreproducible process1,9–11 which could introduce discrepancies in socket fit. 12 Holmgren was cited, stating that shaping for an even pressure distribution should be done at the shape-capture process. 6
The three criteria could be obtained through a socket that matches either the surface or the volume of the loaded residuum. 6 Surface matching is difficult to achieve and errors could create peak loading pressures in other areas. Volume matching applies the principle of hydrostatic load transfer, which assumes that soft tissues behave uniformly when loaded and should the socket be a closed system of fixed volume, there would be equal pressure distribution over the residuum. However, soft tissues are not uniform and the socket is an open system. Therefore, volume matching sockets can only be described as a quasi-hydrostatic system.
Socket design
Presently, there are two existing socket designs used in trans-tibial prosthetics. Specific surface bearing design suggests that weight is borne mostly on specific load tolerant surfaces of the residuum. 13 This design requires manual manipulation of soft tissues to pre-shape the negative cast, which is followed by modification that shapes the socket contours to anticipate contact forces of gait.
Total surface bearing design suggests that equal load should be distributed over all surfaces of the residuum. It aims to create a quasi-hydrostatic system, which redistributes socket pressures in gait. 9 It is sometimes referred to as a hydrostatic socket. 14 This design utilises pressurised casting to load the residuum and usually no further modifications are required.
Although the two socket designs are radically different, they are both prescribed clinically, depending on the indications of the prosthetic user.14,15
Shape capture
‘Shape capture’ is the term loosely used to define the process where a representation of the residuum is created via either a physical cast or virtual scan. It provides the prosthetist with a starting point to design and fabricate the eventual socket. Thus, it is essential that shape capture represents the residuum as accurately as possible, to minimise cumulative error. 16
Conventionally, shape capture is done via plaster-of-Paris (POP) bandages, where it is wrapped and hand shaped by the prosthetist to produce a negative cast. 17 However, with different socket designs and advancements in technology, new methods of shape capture have emerged.
Categorising shape capture
In prosthetics, the terminologies and classifications used for shape capture are still inconsistent. Safari et al. 18 used the term ‘hands-on’ for a conventional wrap cast and ‘hands-off’ for shaping with pneumatic pressure, while Manucharian 19 referred to the hydrocast as ‘hands-off’.
For clarity, this article would refer to ‘hands-on’ as any shape-capture technique that requires manual shaping. ‘Hands-off’ techniques would not require manual dexterity in shaping. Computer-aided design (CAD) would refer to digital shape-capture methods. These methods are categorised in Figure 1.
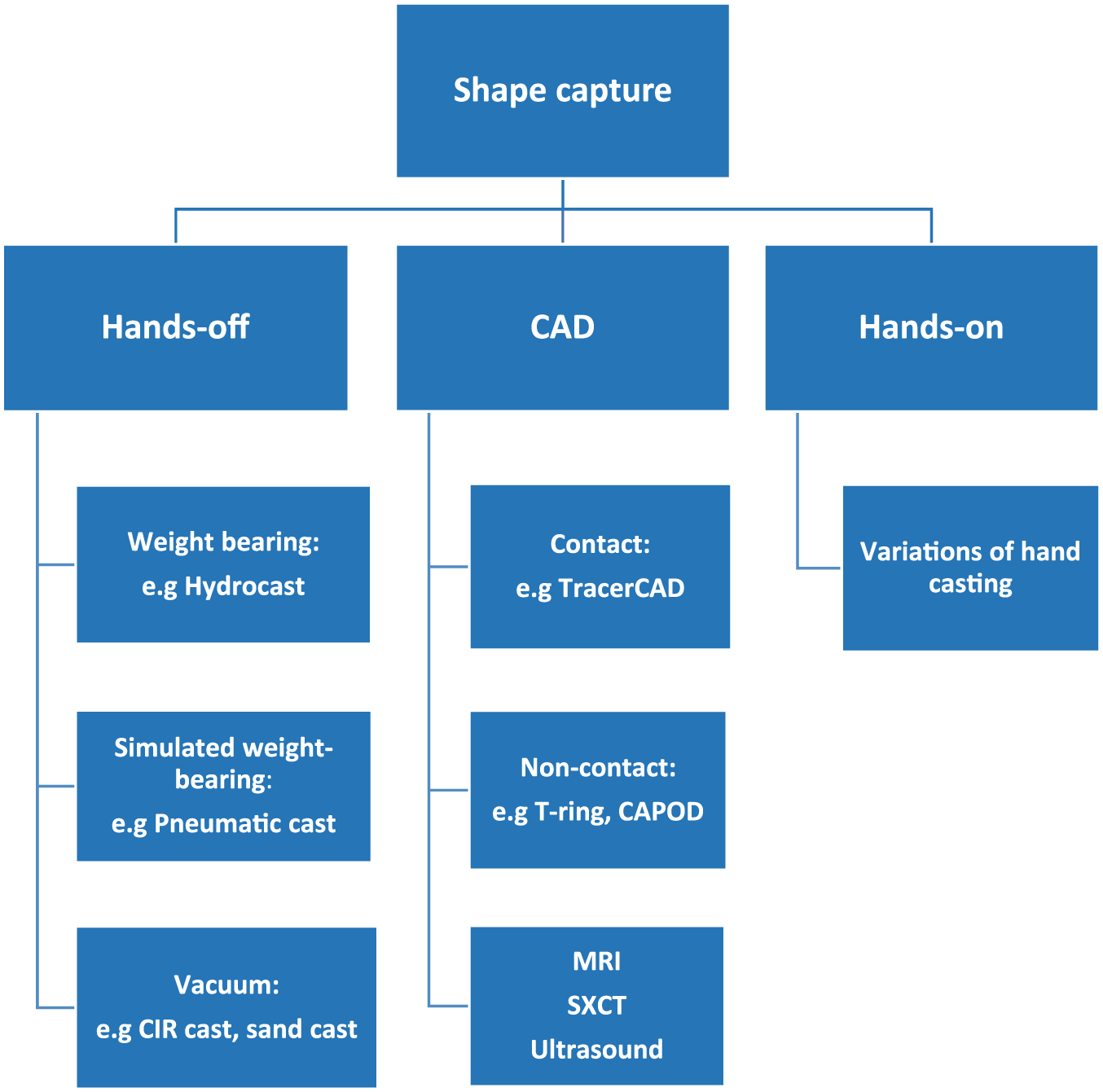
Shape-capture methods.
CAD (contact)12,20,21 methods require contact between the digitizer and the surfaces of the subject, in order to capture its shape. CAD (non-contact)12,22–27 are optical scanners that utilise laser, 28 fringe projection 29 and silhouetting30,31 technology to capture shape. Ultrasound, 32 magnetic resonance imaging (MRI)18,33 and spiral X-ray computed tomography (SXCT)30,34 are systems that can capture both external and internal structures of the residuum. These methods are also non-contact; however, due to their added capabilities, they are classed under a separate sub-group. CAD methods do not load the limb, thus requiring modification to the captured shape.
Hands-off, weight-bearing (HOFF(WB)) methods 35 capture shape under load-bearing conditions with the casting equipment supporting the prosthesis user. This attempts to replicate socket loading pressures experienced in standing, which help to shape the negative cast. Minimal or no modification is required.6,16,35
Hands-off, simulated weight-bearing (HOFF(SWB)) methods also attempt to replicate weight-bearing pressures. However, these casts are taken in a non weight-bearing state, with appliances exerting external pressures to shape the negative cast. Some modification might still be required. 9
Hands-off, vacuum (HOFF(V))36,37 methods apply the ‘principle of dilatancy’ to capture shape through vacuum suction. Depending on the technique utilised, these casts can be performed in a weight-bearing state. Modification might be required.38,39
It is difficult to distinctly categorise shape-capture methods due to the multiple overlaps in characteristics; however, these categories would be used in this review for clarity.
There are suggested advantages and disadvantages of different shape-capture methods, which are listed in Table 1.
Shape-capture methods: perceived advantages and disadvantages.
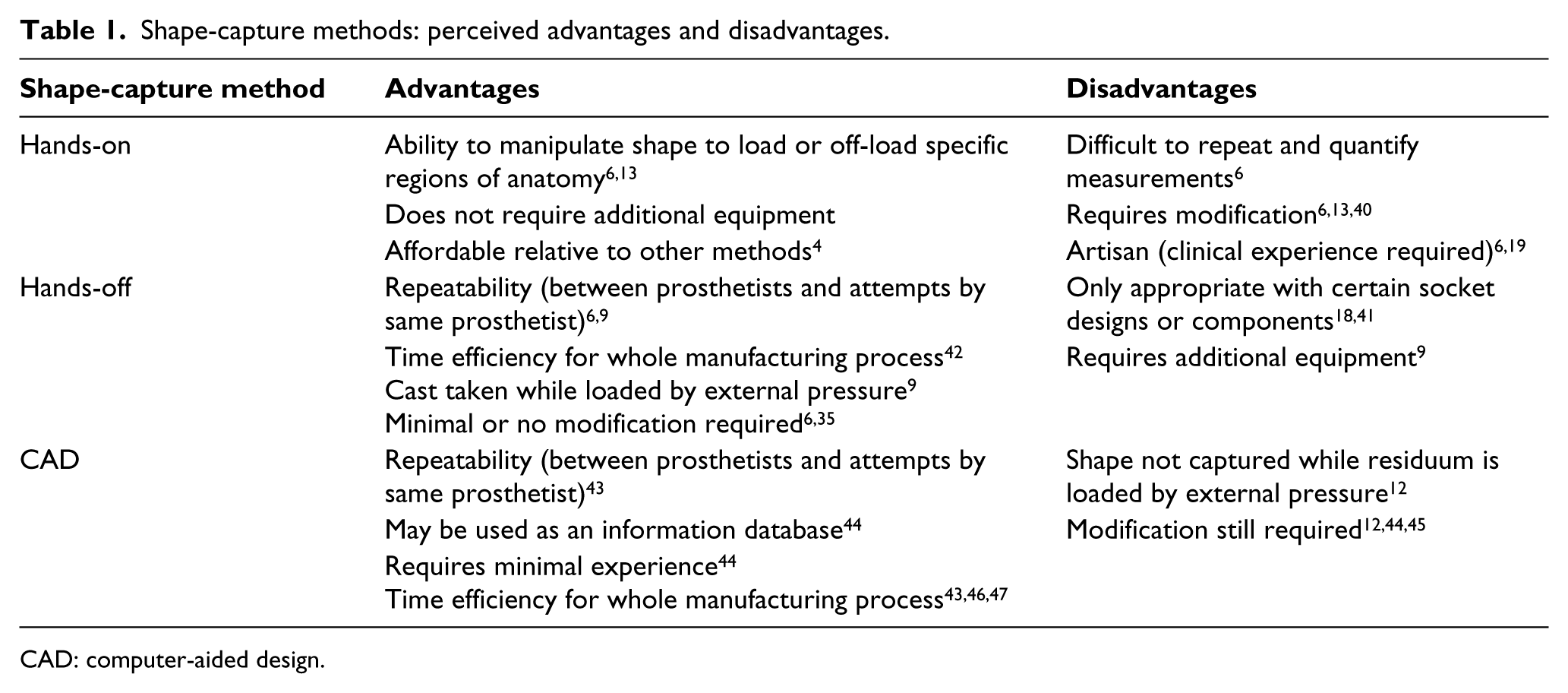
CAD: computer-aided design.
Shape-capture measurements
Clinically, measurements at anatomical landmarks on the residuum are usually taken together with shape capture. A variety of measurement equipment exist, ranging from rudimentary hand tools to advanced CAD systems, possessing resolutions capable of measuring changes in one-tenth of a millimetre in geometry or percentage volume. 48 To assess for shape-capture accuracy, equipment precision is required.
Evaluating shape capture
Quality of shape capture
To have the best chance of obtaining a good socket fit, shape capture should be repeatable, reliable and accurate. However, as the dimensions of a residuum under optimal socket fit conditions are still unknown, ‘true’ accuracy is undefined. Some studies utilised ‘gold standard’ measurements to determine the dimensions of an unloaded residuum as a reference standard for accuracy. 12 However, this ‘gold standard’ varies across literature.
A ‘clinically acceptable’ socket fit was suggested to allow for 1–2 socks to be worn over the residuum.7,40 The exact measurements of this fit differ across studies, but it was suggested that volumetric differences are within 5%–9% of the residuum’s volume.7,18,31,40 Sanders et al. 42 mentioned that a 5% volumetric change in a uniformly expanding residuum with a diameter of 90 mm would correspond to a radial difference of 1 mm. However, it was unclear how this value was obtained.
In this article, quality of shape capture will be determined by the reliability and accuracy of different methods. Accuracy would be measured according to the values of the clinically acceptable fit.
Comfort of user
A prosthetic socket needs to fit comfortably. Having an ill-fitting socket would result in gait deviations, skin breakdown and even rejection of prosthesis. 3 Comfort can be quantified using internally valid scales such as the Socket Comfort Score (SCS). 41
Clinical efficiency
Some shape-capture methods are suggested to improve clinical efficiency through minimisation of cost and time. 36 Hence, different shape-capture methods could be employed for centres with varying budgets and clinician experience.
Objectives
Shape capture is the first step of every socket production process. However, it is unclear which shape-capture methods provide the best chances of attaining a good fit, under certain conditions. Therefore, outcomes relating shape capture to socket fit need to be evaluated.
The purpose of this review is to examine the influences and trends of shape-capture methods on the outcomes of quality, comfort of user and clinical efficiency, in the population of trans-tibial prosthesis users. This review also hopes to suggest direction for future research.
Method
Protocol
The methodology of this review was documented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 43 Studies were graded according to the American Academy of Orthotists and Prosthetists (AAOP) guidelines. 44
Studies were selected based on the criteria in Table 2. Studies that used models as subjects were also included, as quality was evaluated as an outcome. Quality of shape capture determines the margin of error for measured dimensions of any object.
Study selection.
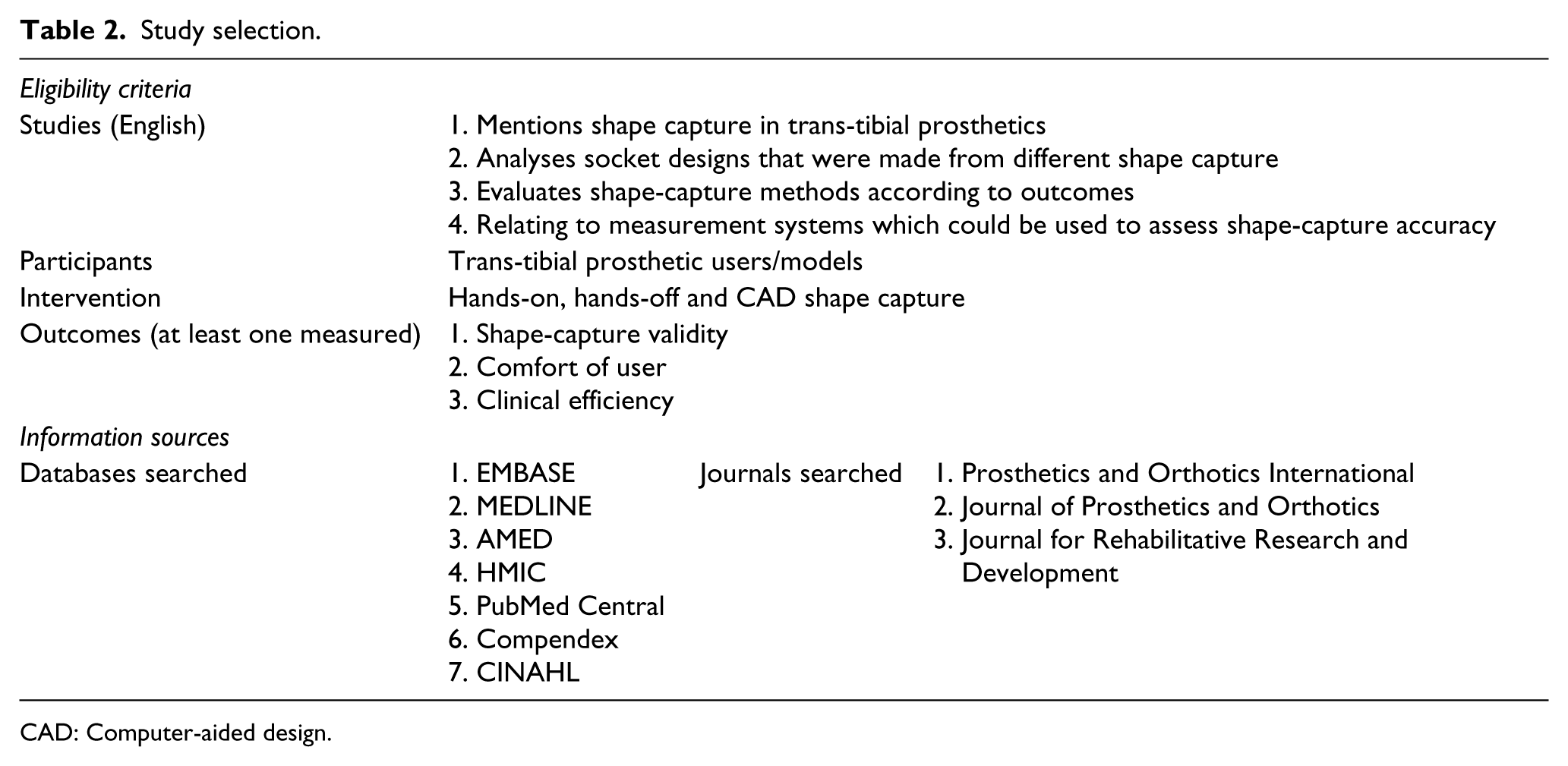
CAD: Computer-aided design.
Excluded studies
Studies that used direct socket production were excluded. In direct socket production, the socket is formed on the user’s limb via a lamination process. It is a method of socket fabrication rather than a different shape-capture method. 45
Studies that reported on CAD scanning of negative hand casts in their methodology were also excluded. This is essentially using CAD for modification, rather than the actual shape capture. 46
Studies that reported on post amputation temporary prostheses or included subjects who were inexperienced prosthetic users were also excluded. This is to limit the differences in outcome measures due to volume fluctuations as well as comfort where new users are not yet accustomed to a prosthesis.31,48,47,49
Papers that only presented technical instructions were also excluded as they do not evaluate any outcomes.
Information sources
Studies were found via searching of electronic databases and bibliographies of included studies. To ensure a thorough search process, journals where included studies were most commonly published in were hand searched to obtain other relevant studies. These are listed in Table 2. The last updated search was done on 25 April 2018. The full search strategy and search terms are shown in Appendix 1.
Study selection
The author assessed the eligibility of studies independently. Studies which were found to be ambiguous in inclusion or exclusion criteria were discussed with the co-authors.
Data collection process
A template was created for the data extraction process. This is detailed in Appendix 1. Extracted data are presented in Tables 3 and 4.
Studies evaluating hands-on, hands-off and CAD.
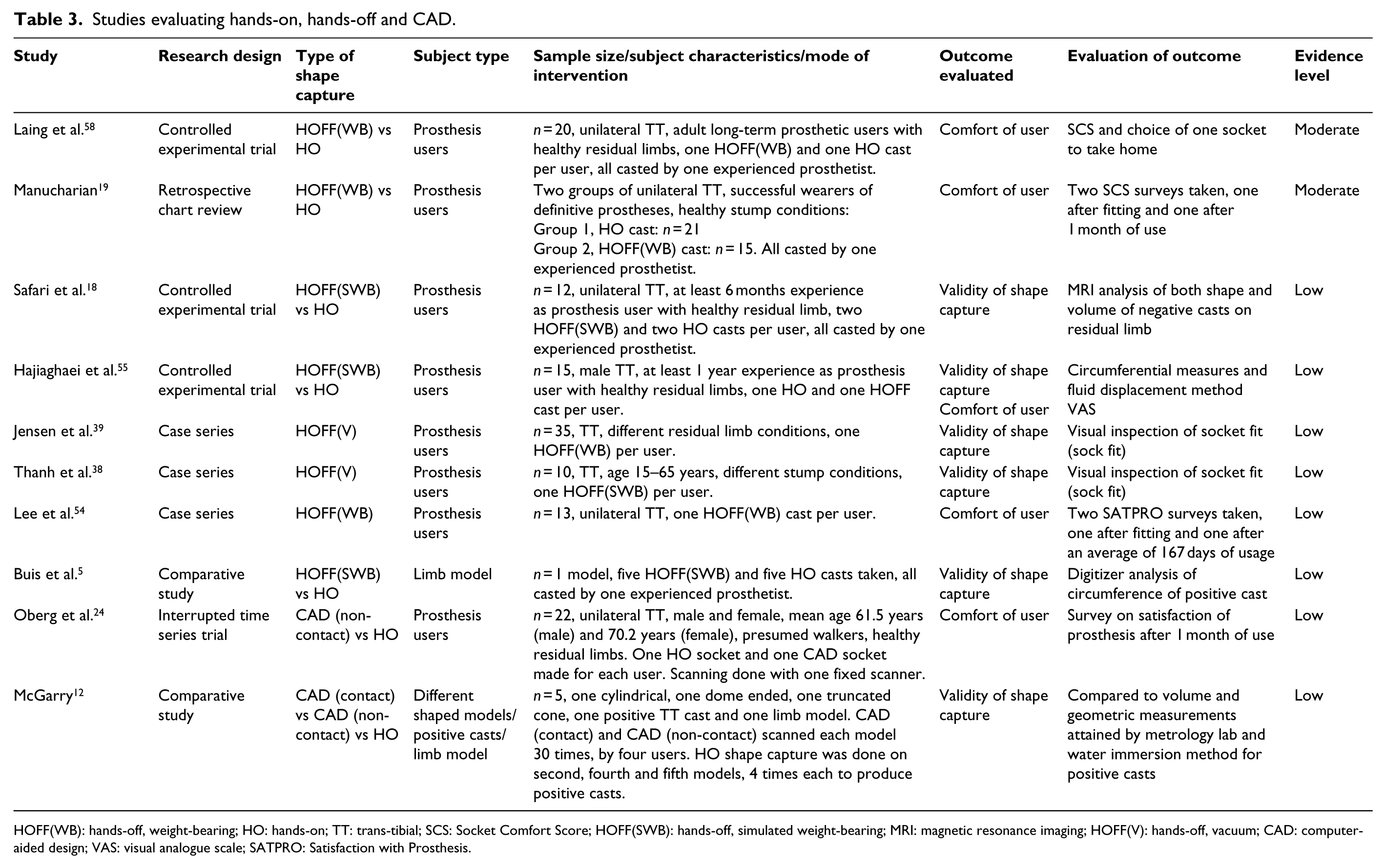
HOFF(WB): hands-off, weight-bearing; HO: hands-on; TT: trans-tibial; SCS: Socket Comfort Score; HOFF(SWB): hands-off, simulated weight-bearing; MRI: magnetic resonance imaging; HOFF(V): hands-off, vacuum; CAD: computer-aided design; VAS: visual analogue scale; SATPRO: Satisfaction with Prosthesis.
Studies evaluating measurement systems.
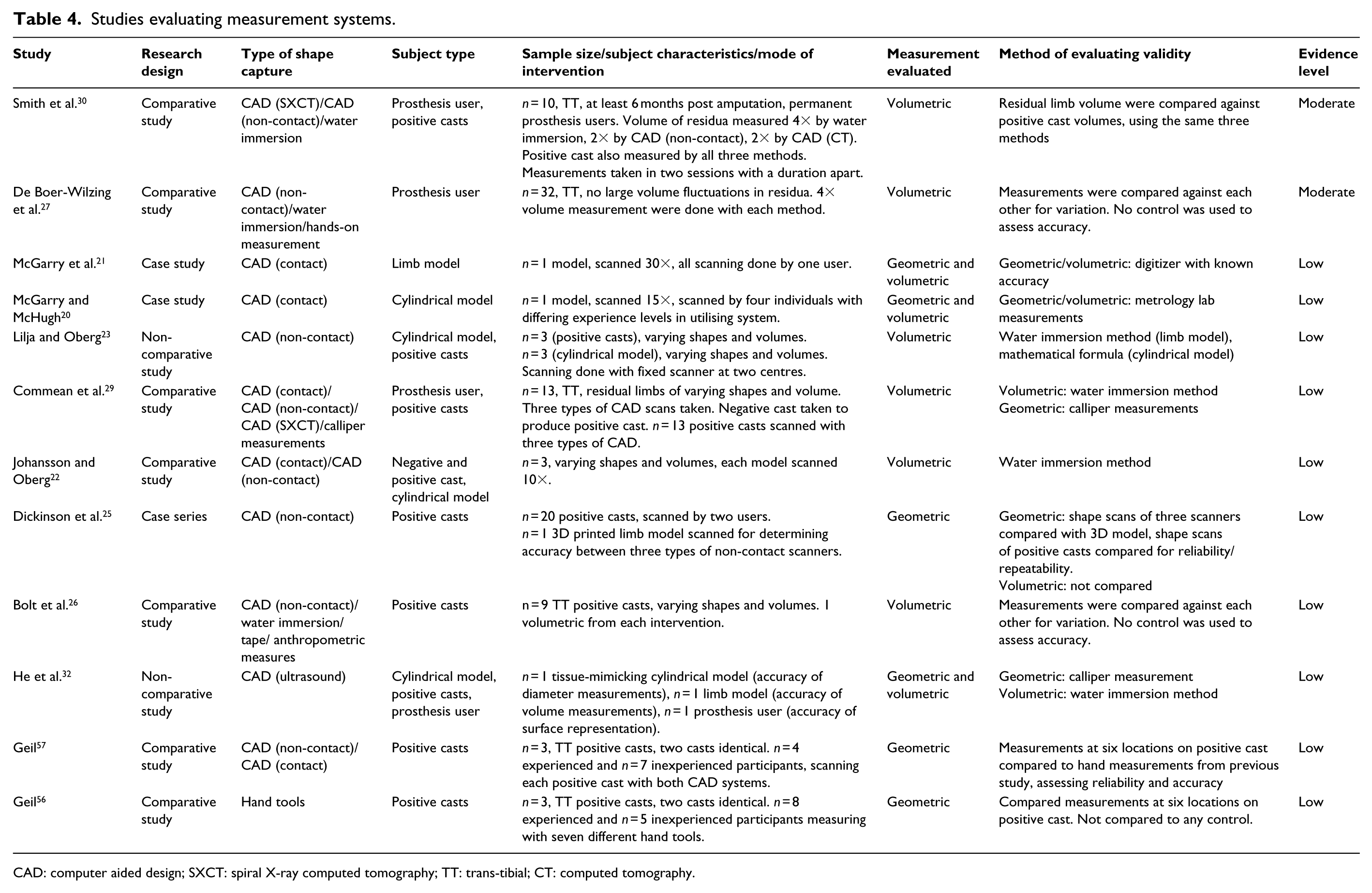
CAD: computer aided design; SXCT: spiral X-ray computed tomography; TT: trans-tibial; CT: computed tomography.
Risk of bias
Risk of bias was evaluated via the AAOP State-of-the-Science Evidence Report. 44 Studies were classified according to their design; however, not all fulfilled the categories provided. Studies with experimental designs were graded higher than those without. The checklist determined the level of bias by assessing the study’s internal validity (IV) and external validity (EV). Overall grades of ‘low’, ‘moderate’ and ‘high’ are given, according to the level of bias and study design.
Results
Study selection
A total of 22 eligible studies were identified in this review. The selection process is detailed in Figure 2, and the extracted data are presented in Tables 3 and 4. No studies evaluating clinical efficiency were found, which led to the outcome measure being removed.
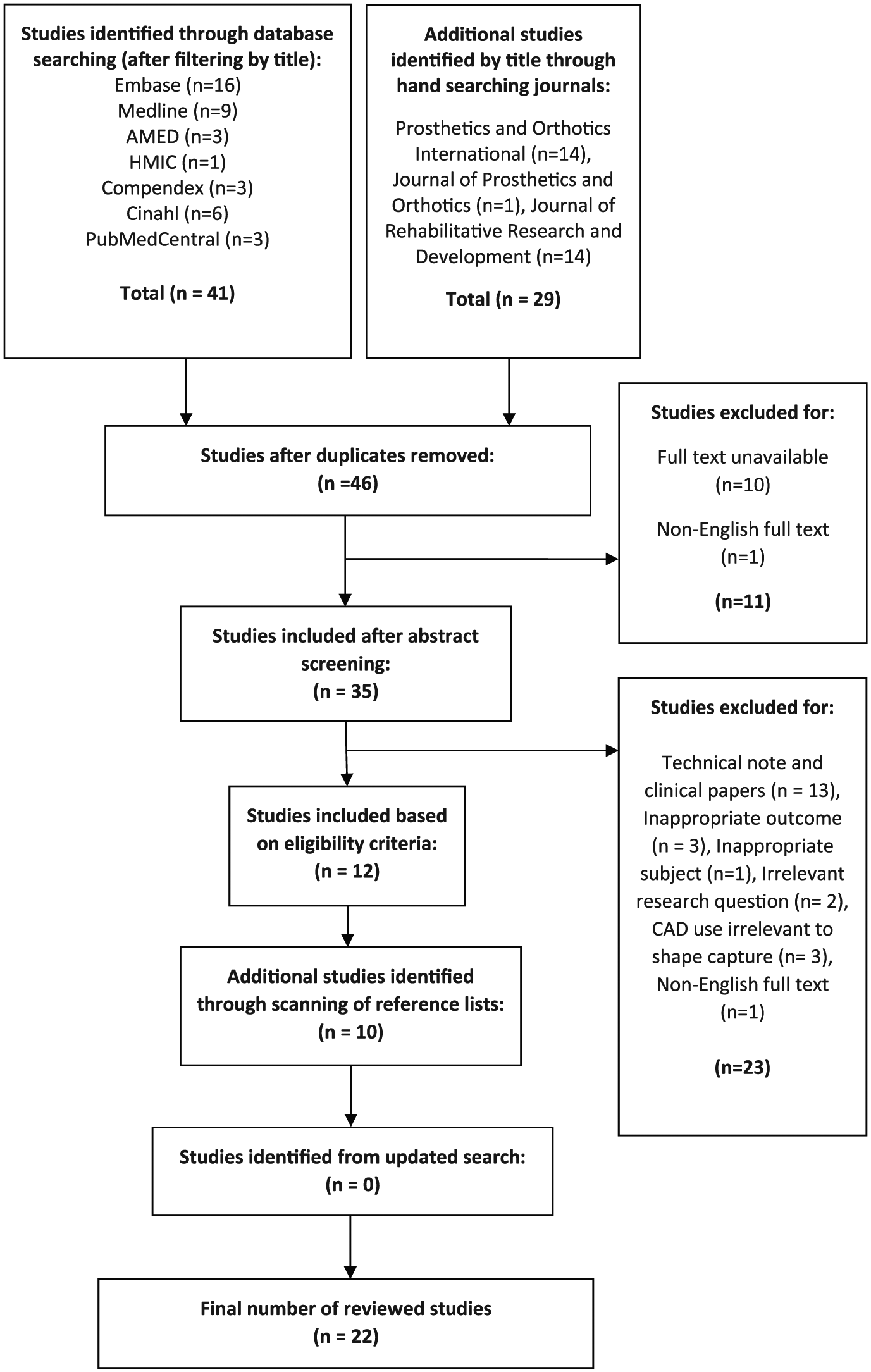
PRISMA flow diagram.
Quality appraisal
Overall, 19 studies5,12,18,20–26,29,32,38,39,54–57 were rated to have low evidences due to high risk of bias, 3 had moderate evidences19,27,30,58 with moderate risk of bias and no studies with very low risk of bias were found. These are presented in Tables 3 and 4.
Hands-on and hands-off
Eight studies evaluated HO and HOFF methods; 5,18,19,38,39,54,55,58 four studies reported on quality,5,18,38,39 three reported on comfort19,54,58 and one reported on both outcomes. 55
Comfort was evaluated in two studies comparing HOFF(WB) against HO,19,58 as reported in Table 5. Both studies used the SCS as their outcome measure. However, one study 19 took SCS surveys on two separate occasions, one after initial fitting and the other after a month of use. In both surveys, results for HO were better. The other study 58 took surveys after initial fitting and found no significant differences between HO and HOFF(WB) sockets.
Results for hands-on, hands-off and CAD.
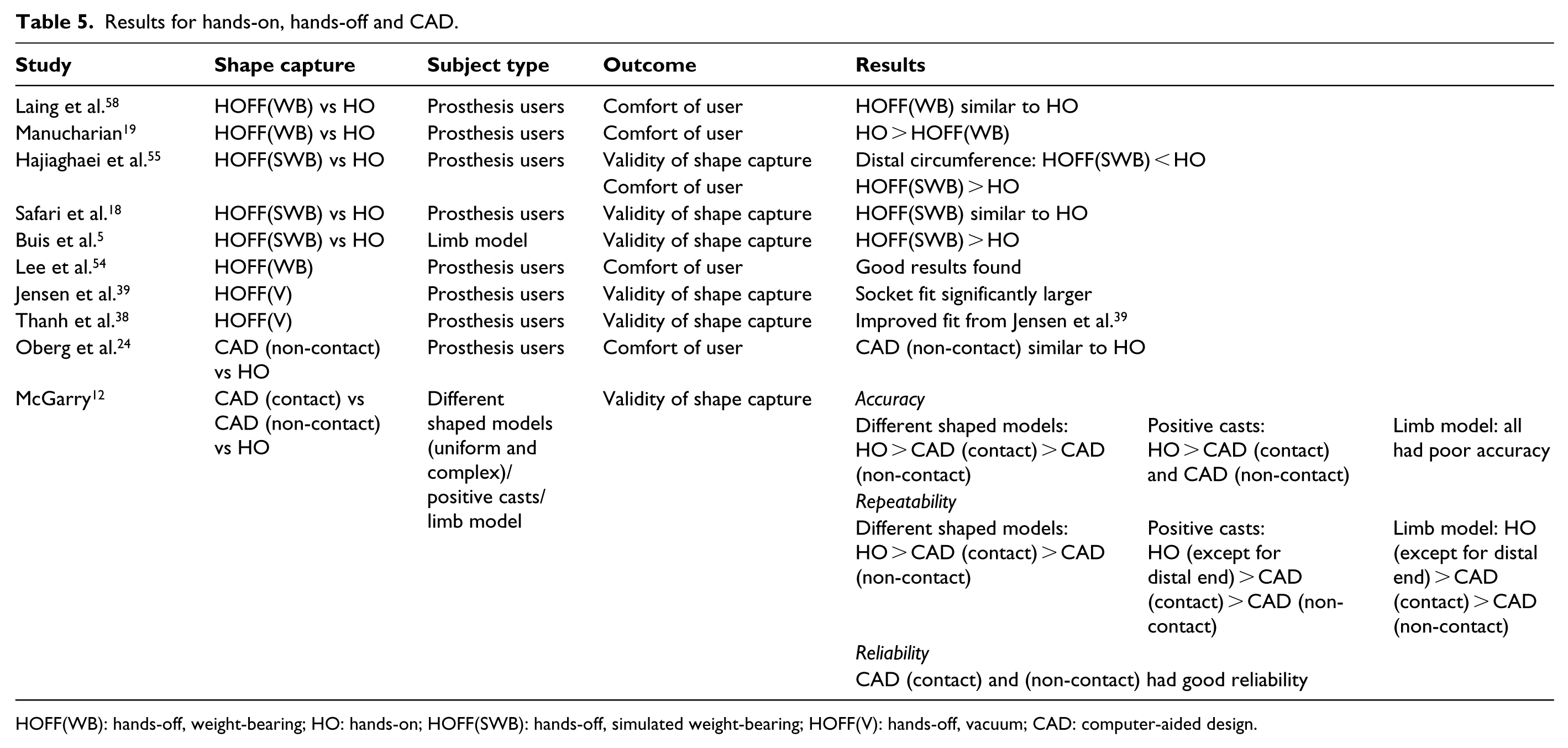
HOFF(WB): hands-off, weight-bearing; HO: hands-on; HOFF(SWB): hands-off, simulated weight-bearing; HOFF(V): hands-off, vacuum; CAD: computer-aided design.
Quality was evaluated in two studies comparing HOFF(SWB) against HO.5,18 Both studies had different subject groups and outcome measures, as evident in Table 5. One was done on residual limbs, while the other was done on a single limb model. Both studies compared cast repeatability. The first study used MRI to evaluate negative cast dimensions on the residual limb. 18 The other used a digitizer to analyse circumferences of positive casts. 5 The first study 18 found that both HO and HOFF(SWB) produced repeatable and clinically acceptable volumes, but lacked shape repeatability. When expressed in percentage volume for clinical significance, HO shape differences equated to a ‘1 sock fit’, while HOFF(SWB) did not require a sock. The other study 5 found that HO lacked repeatability where variations in circumferential measurements ranged from 2.4 to 5 mm. HOFF(SWB) was more repeatable and had a maximum variation of 1.4 mm.
CAD
Two studies evaluated CAD shape capture.12,24 As presented in Table 5, one study reported on comfort of user, 24 where satisfaction of socket was measured after a month of use. The study compared CAD (non-contact) to HO sockets on group of prosthesis users. No significant differences were found. The other study compared HO, CAD (contact) and CAD (non-contact) 12 on various theoretical models. Accuracy of volumetric and geometric dimensions obtained was evaluated against metrology laboratory measurements to determine clinical significance. CAD (contact) had good accuracy for uniformly shaped models, but was inaccurate on complex shapes and the limb model. HO was found to be inaccurate on the limb model and CAD (non-contact) was found to be largely inaccurate across all models. Reliability of HO was not evaluated but CAD (contact) and CAD (non-contact) were found to be reliable. Both CAD systems had good repeatability on uniform shapes, but performed poorly on complex shapes and the limb model. HO had better repeatability when compared to CAD, except for distal end volumes in more complex shapes and the limb model. Generally, all methods lacked repeatability at measuring distal end volumes in complex shapes and CAD (non-contact) was the least repeatable method.
No study was found evaluating CAD against HOFF.
Measurements
A total of 12 studies compared measurement systems;20–23,25–27,29,30,32,56,57 11 compared CAD systems20–23,25–27,29,30,32,57 and 1 compared hand tools. 56 With reference to Table 4, studies compared geometric and volumetric measurements on a variety of subject groups. Studies had small sample sizes and mostly compared models of different shapes and volumes. Only four studies27,29,30,32 included measurements carried out on a residuum. Studies suggest that the different systems were generally repeatable and reliable. However, results varied according to shape, compressibility of surfaces, study design and statistical analysis.
Discussion
The purpose of this review was to report on the influences and trends that shape-capture methods had on certain outcomes in trans-tibial prosthetics. With the paucity of literature on shape capture, along with a specific focus on certain outcomes, only a few eligible studies were identified from the search. Of the literature identified, there were many variations in study characteristics. This made inter-study comparisons difficult. Many studies also involved different forms of bias, which affected overall validity.
Shape-capture methods
In the study by Safari et al., 18 repeatability was compared between HOFF(SWB) and HO. Both methods utilised POP bandages but differ in the shaping process. For HOFF(SWB), POP bandage was applied over a silicon liner worn on the residuum. For HO, wrap casting was done directly onto the residuum. This difference in interface could affect cast deformability which would affect the evaluated dimensions. ‘8 layers of stockinet’ were also worn on the residuum before either HO or HOFF(SWB) casts were taken. This was to improve boundary visibility in the MRI scan. However, this is not a normal clinical practice and it was unclear if measurements took into account the diameters and volumes of the stockinet. Hajiaghaei et al. 55 compared between HOFF(SWB) and HO. The HO method used was atypical of the conventional wrap cast but was similar to the ‘Precision Plaster Casting’ detailed by Staats, 59 which was used to develop the UCLA TSB socket. 60 Although this method required hand shaping and modification, however, it utilises weight bearing, which might not permit comparisons with other HO studies.
In studies by Laing et al. 58 and Manucharian, 19 SCS was used to evaluate socket comfort at initial fitting. Manucharian 19 assessed comfort immediately after the alignment stage, without any mention of acclimatisation. On the contrary, Laing et al. 58 assessed comfort as the last outcome after a series of measurements for various gait tests, where the user could have already been acclimatised to the socket. Lee et al. 54 utilised the Satisfaction with Prosthesis (SATPRO) to assess post-fitting and post-usage satisfaction, while Hajiaghaei et al. 55 used a visual analogue scale (VAS) to determine socket comfort. Along with different outcome measures of comfort, different socket suspensions, interfaces and prosthetic feet were also used in each study. These could have affected comfort scores, which made inter-study comparison unsuitable.
Buis et al. 5 compared the consistencies of HOFF(SWB) and HO on a single limb model. As the limb model is not able to replicate tissue behaviour, results might differ if the study was done on a residuum. Furthermore, use of a single model with no variations in dimensions might not be able to fully assess the repeatability of both methods. In the study by McGarry, 12 HO was compared against CAD (contact) and CAD (non-contact), assessing for quality. Theoretical models, positive casts and a manikin model were used as subjects. Similarly, these subject types are not representative of the residuum. However, the results suggested that the quality of CAD systems with regard to more complex shapes and compressible models was poor. This might also suggest that poor results would be obtained on a residuum. However, more CAD studies involving prosthesis users and updated systems are required to draw a conclusion.
Jensen et al. 39 investigated the effects of a HOFF(V) on socket fit. This method captured the shape of the residuum via vacuum suction, with the user bearing weight on a sand-filled container. 36 The method was later on improved by replacing sand with micro-polystyrene beads and the weight-bearing element of the cast was omitted. 37 Both methods required cast modification. The new method was evaluated by Thanh et al., 38 who reported an improved one sock fit from 2–5 socks required to obtain total contact in the original sand cast. However, these assessments were done on sockets manufactured from modified casts. Shape capture in both studies was also done by the same prosthetist which could affect its reliability. Both of these factors would have affected the assessment of shape-capture quality.
Safari et al. 18 found that HO produced acceptable volume but poor shape repeatability when applied on residual limbs. McGarry 12 reported that HO had poor repeatability in distal end volumes but acceptable repeatability in diameter measurements when done on a limb model. Each study assessed repeatability with one prosthetist applying the intervention. These differences in results could be due to variations in plaster wrapping techniques, study designs and subject types.
HOFF methods were developed to minimise the influences of a prosthetist’s casting and modification skills on the resultant socket fit.9,16 This would possibly indicate that HOFF would be suitable for clinics that lacked experienced practitioners. 58 As shown in Tables 3 and 5, HOFF methods were applied in developing countries and were suggested to produce promising results.38,39,54,58 However, these findings should be interpreted with caution. Jensen et al. 39 and Thanh et al. 38 mentioned that experienced prosthetist inputs were still required for the casting and modification process. Laing et al. 58 attempted to minimise inter-rater error by having the same experienced prosthetist casting for both HO and HOFF(WB). Only Lee et al. 54 evaluated comfort of HOFF(WB) sockets casted by less-experienced clinicians.
Measurements
Most of the findings reflected those reported by Sanders et al., 48 in their systematic review of measurement systems for volume change in the residuum. With variations in system and study characteristics, differences in results were expected. However, due to the focus of this review, differences were not covered in detail. Instead, general findings were discussed.
There was a lack of reference standard which systems could be compared to. Geil 56 compared the repeatability and accuracy of hand tools against each other. McGarry and McHugh 20 referred to measurements obtained from a metrology laboratory as the ‘gold standard’. Some studies12,22,23,32 compared volumetric measurements to that of a water immersion method. However, Bolt et al. 28 and De Boer-Wilzing et al. 27 evaluated water immersion against CAD and found that there were systematic errors. Studies were also inconsistent in the indices used for analysis of repeatability and reliability.
It was found that all systems evaluated had acceptable reliability and repeatability while measuring theoretical models. However, evidence is weak in suggesting the results would be achieved on a residuum. Studies that measured a residuum show that results vary according to marker positioning, movement and residuum characteristics.27,29,30,32 Systems capable of visualising internal structures have potential to assess socket fit with reference to tibial position within the residuum.18,29 However, due to high costs, inaccessibility and duration of scan time, these systems are not implemented in clinical use. 48
Accuracy of shape capture
Accuracy could be assessed by comparing shape to either the unloaded residuum or to a loaded residuum with dimensions of an optimal fit. Due to the lack of ‘optimal fit dimensions’ for each limb, ‘true’ accuracy of shape could be difficult to quantify.
Klasson 6 suggested that the optimal socket fit would stabilise the tibia through soft-tissue compression when the residuum’s volume equilibrium is reached. Fluid in the residuum would be drained out proximally as it compresses, till the limit of compressibility is reached. This rate of proximal fluid transfer would be pressure and time dependent due to the viscosity of flow, where time taken for volume change and pressure exerted are inversely related. The geometric and volumetric dimensions measured under this condition could perhaps be considered as the ‘optimal fit dimensions’ for that particular residuum. However, Klasson also mentioned that there is no knowing if such a condition can be reached, and if so, the amount of pressure and time required and the corresponding limb dimensions are unknown. At present, no study has quantified these dimensions.
Due to the lack of a ‘true’ accuracy, authors in the literature have defined volumetric and geometric values of a ‘clinically acceptable fit’ which correspond to a 1–2 sock fit over the residuum.7,18,40 Most studies that evaluated quality of shape-capture systems used these values to determine their clinical significance. However, it was found that there was a lack of consensus between studies defining these values.7,18,31,40,42 This inconsistency could likely affect the quality of systems with regard to clinical significance.
Literature for measurement systems mostly focused on the need for equipment precision and resolution in measuring an unloaded residuum. Although they are important, it was found that different conditions could have a significant effect on a residuum’s volume and geometry, possibly larger than the precision gained from using a sophisticated system. Lilja et al. 61 found that residual limb volume increased with muscle activity during casting, up to 5.8%. Zachariah et al. 31 found that the residuum’s volume change ranged from 0.2% to 17% within 5 min of doffing and it was inconsistent between subjects and conditions. These significant values might possibly suggest that perhaps more attention should be directed towards assessing socket fit or captured shape of a loaded residuum, rather than surface and volume measurements in an unloaded residuum. These could be achieved with systems that can assess internal limb structures.
Comfort of user
Comfort is subjective and difficult to quantify.47,49 Surveys such as the SCS 41 provides a numerical result for ease of statistical analysis. However, opinions towards socket comfort still vary between individuals and it can be influenced by different factors.
Experienced prosthesis users might prefer a socket design due to familiarity. This was reflected in the study by Manucharian, 19 where it was found that initial and final SCSs were higher for subjects whose socket designs were unchanged.
Comfort is also an outcome which is measured at the end of the socket production process. This occurs after the stages of shape capture, modification, manufacturing and alignment. Changes made in any of the stages could have an effect on the overall outcome.52,62,63 Influence from components such as suspension, prosthetic foot, 51 socket materials and interfaces 64 might have an effect on overall comfort score. Therefore, it is difficult to ascertain if the effects on comfort are due to the sole influence from shape capture, unless inconsistencies are removed with more robust research methodologies.
Summary
In summary, as presented in Tables 3 and 4, all studies had small sample sizes and were inconsistent in characteristics and outcome measures. This limited the potential for inter-study comparisons, which subsequently affected the confidence of trends identified. Evidence was also weak in suggesting that effects on outcomes were due to the sole influence of shape-capture methods. However, from the limited evidence, some insights could still be drawn.
Generally, HO was found to have poor shape repeatability.5,18 This was likely due to the deforming nature of the HO method, where indentations are made to pre-shape the cast for modification. Some results reported that HO is repeatable in volume, where differences are within the clinically acceptable ranges. 18 This was not found across all studies. 12 Irrespective of study design, this likely corresponds with suggestions in literature that a good fitting HO cast is still largely dependent on a prosthetist’s skill. 6
Safari et al. 18 reported that although HOFF(SWB) produced repeatable volumes, it had poor shape repeatability. The author suggested that the poor repeatability could be caused by factors such as setting of bladder pressure and proximal force application during casting. Other HOFF studies were found to also utilise input from experienced prosthetists during the casting process.19,38,39,58 These similarities could perhaps suggest that although HOFF methods aim to minimise the reliance on a prosthetist’s technical skills, some degree of experience in apparatus usage is still required to attain a good fit.
There were a lack of studies that compared CAD to other shape-capture methods. Most studies involving CAD evaluated the quality of systems on theoretical models. More CAD studies evaluating socket fit on residual limbs are required.
No particular ‘gold standard’ measurement for residual limbs has been established in the literature, and it is still unclear as to what the dimensions of an optimal socket fit are. 48 Also, there was no robust evidence to suggest that the criteria of a ‘clinically acceptable fit’ was accurate due to variations found in literature.7,18,31,40,42 More research is required in establishing reference standards to which quality of shape capture could be compared to.
Comfort was found to be subjective in nature and differed across studies and individuals. HOFF methods encourage an even pressure distribution over the residuum6,9,16 and in theory would be expected to produce better results in comfort as compared to HO with load-specific surfaces. Interestingly, no distinct trends in comfort were identified between sockets produced from HOFF or HO methods. This agrees with findings from Cavenett et al., 15 where no differences were identified for comfort, between TSB and PTB socket designs. This suggested that although scales could be used to quantify comfort, 41 the exact mechanisms of socket fit relating to comfort are still unclear 47 and more research is required on the topic.
Limitations
This systematic search and review was done by one author, only considering literature that was written in English. This may have resulted in possible oversight of other research in foreign languages. The nature of the topic being studied contains multiple variables that are intertwined and only studies with experienced prosthesis users were included. Hence, findings obtained might not be fully representative of the trans-tibial prosthesis user population. Attempts at organising the literature into sub-groups for the context of this review might have discounted some details that each shape-capture method presents.
Recommendations for future work
To obtain an optimal fit, the socket needs to be either surface- or volume matching. 6 However, surface matching is difficult to attain and present shape-capture methods that can only create quasi-hydrostatic systems through attempted volume matching. These methods also only represent a static situation. Goss et al. 53 reported on redesigning a hydraulic rig initially used by Isherwood in attempting to attain a surface-matching socket. 6 Although uncompleted and untested, this rig allowed for real-time pressure measurements and was proposed to be able to cast the residuum in a dynamic situation with the use of polyester tape. More research in this direction is required to possibly design a shape-capture method that could also incorporate the dynamic nature of gait.
The exact relations between socket fit and comfort are still unclear. 47 However, future research can look at assessing the fit of a loaded limb within a socket. Most present systems are only able to evaluate the dimensions of an unloaded residuum, with the exception of SXCT.29,30 SXCT is capable of providing accurate representations of a limb within a socket, however, only in a static position. Papaioannou et al. 50 reported on a system that could assess socket fit in a dynamic situation. This could possibly open up new avenues for understanding socket comfort.
Conclusion
The purpose of this review was to examine the influences and trends that shape-capture methods would have on certain outcomes in trans-tibial prosthetics. However, it was found that study characteristics and outcome measures used were inconsistent. This made inter-study comparisons unsuitable, which limited trend identification. Overall evidence was weak in suggesting that effects on outcomes were due to the sole influences of shape capture. However, it was not unexpected that hands-on methods lacked shape repeatability.5,18,55 This was due to the manual cast deformation required of a specific surface bearing socket design. Volume repeatability differed between studies and is likely to be influenced by a prosthetist’s skill.12,18 Hands-off methods were found to be generally repeatable but some equipment usage experience was still required to attain good results.19,38,39,58 CAD (contact) methods had higher quality when compared to CAD (non-contact); however, these findings were obtained on theoretical models. 12 Measurement systems lacked a reference standard and ‘gold standards’ were inconsistent across studies. 48 Comfort was found to be subjective, and its relation to socket fit is still unclear. 47 Overall, more research is required in each area and future studies should have more robust methodologies to limit variabilities between studies. Future research should possibly look towards developing dynamic shape-capture methods 53 and utilising systems which are capable of assessing socket fit in dynamic situations. 50
Footnotes
Appendix 1
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.