
Abstract
Background:
Strategies to maintain prosthesis users’ daily limb volume are needed.
Objectives:
Test how intermittent incremental socket volume adjustments affect limb fluid volume and limb-socket distance.
Study design:
Repeated measures.
Methods:
People with transtibial limb loss walked on an outdoor trail wearing a motor-driven adjustable socket that they adjusted a small amount, approximately 0.3% socket volume, every 2 min using a mobile phone app. Limb fluid volume and sensed distance between the socket and a target in their elastomeric liner were monitored. A gradual socket enlargement phase was followed by a gradual socket reduction phase.
Results:
An incremental socket enlargement significantly increased limb fluid volume (p < 0.001) but not sensed distance (p = 0.063). An incremental socket reduction significantly decreased both limb fluid volume (p < 0.001) and sensed distance (p < 0.001).
Conclusion:
Participants’ residual limb fluid volume increases during ambulation compensated for incremental socket volume increases. For incremental socket volume decreases, residual limb fluid volume decreases did not compensate and the socket fit became tighter.
Clinical relevance
Results support the hypothesis that for people without co-morbidities, intermittent incremental socket volume enlargements are an effective accommodation strategy to increase limb fluid volume while maintaining socket fit. Intermittent incremental socket volume reductions decreased limb fluid volume but also made the socket fit tighter.
Keywords
Background
Socket fit is the most important challenge faced by people with limb amputation.1–3 Adjustable prosthetic sockets are a convenient means to manage socket fit. Unlike adding or removing prosthetic socks, adjustable sockets do not require users to doff their prosthesis, but instead to manipulate a knob on the socket or use a handheld remote-control unit to make adjustments. In commercial adjustable-volume sockets, a Boa™ ratcheting dial is used to adjust the length of a cable that runs through panels in the socket wall (RevoFit™) or around struts on the outside of the socket (Infinite Socket™).4,5 A cabled-buckle socket that adjusts distance across a gap in the socket was also recently introduced (iFIT™). 6 Prosthesis users manipulate the knob or buckle to move the panels, struts, or sides of the socket radially inward or outward according to their need. Elevated vacuum sockets (e.g. LimbLogic™, Harmony E2™, SmartPuck™) operate using a different strategy. They adjust voltage to a pump to maintain a vacuum pressure selected by the user. 7 The vacuum is thought to draw fluid into the residual limb during ambulation.8–11 While volume-adjustable sockets and elevated vacuum sockets improve convenience, prosthesis users must still initiate and specify the appropriate change in setting. Users with adequate protective sensation usually maintain a comfortable fit, though may need to make frequent adjustments.
In a recent investigation, the possibility was investigated that adjustable sockets can further be used to manage limb fluid volume. 12 On a group of participants with limb amputation resulting from traumatic injury, socket volume adjustments were made within prosthesis users’ acceptable socket volume range. Results showed that a socket enlargement ⩾0.7% socket volume caused rapid limb fluid volume increase, and a socket reduction ⩾0.7% socket volume caused rapid limb fluid volume decrease. However, during the 2–3 min after socket reduction, limb fluid volume increased and distance to the socket reduced, suggesting the fit became even tighter well after reduction was completed. This response may have been due to partial venous occlusion induced by the amount of socket reduction (0.7%–1.9% socket volume). Possibly, if smaller socket adjustments were conducted intermittently, allowing the prosthesis user’s residual limb time to recover from each incremental socket volume change, then fluid volume and distance to the socket after adjustment would be better maintained, and a consistent socket fit would be achieved.
In this study, on a group of people with transtibial amputation, we tested the hypothesis that intermittent incremental increases in socket volume increased limb fluid volume and maintained distance between the limb and socket, and that intermittent incremental decreases in socket volume decreased limb fluid volume and maintained distance between the limb and socket. We also tested if the most stable limb fluid volume and most stable distance were at the user’s self-selected optimum socket volume.
Methods
Participants
Participants were included in this study if they were at least 18 years of age, had an amputation at least 18 months prior, were currently using a definitive prosthesis, and were capable of walking without aides for bouts of at least 20 min. Participants were excluded if they had open sores on their residual limb or did not have adequate protective sensation in their residual limb (measured by Semmes-Weinstein 5.07 monofilament). Institutional review board (IRB) approval and written informed consent were obtained from participants before any study procedures were initiated.
Instrumented test sockets
Motor driven adjustable sockets were fabricated with inductive sensors embedded within the socket wall (Appendix 1). The sockets were duplicate in shape to participants’ normally used sockets and were similar in design to those used in a previous study, 12 in that the radial positions of three panels (anterior medial, anterior lateral, and posterior) were adjusted using a motor-driven cable. Each panel was covered with a 3/16″-thick piece of Nickelplast™, rounded at the edges. The motor assembly, which weighed 648 g, was positioned beneath the socket (Figure 1(a) and (b)). Inductive sensors were placed within the socket wall at mid-limb posterior medial and mid-limb posterior lateral locations. Participants wore liners of the same volume as their normal liner, but the liners used in testing, purchased from a commercial liner manufacturer (Willow Wood, Mt. Sterling, Ohio), included a thin layer of ferrous material within the elastomer outer layer. The ferrous material acted as a target for the inductive sensors. The inductive sensors were calibrated to monitor distance between the ferrous layer in the liner and the inside surface of the socket, termed “sensed distance” in this study. 13 Because there was a thin elastic element between the ferrous material and the socket, sensed distance decreased when the liner was pushed up against the socket (Appendix 1). A phone app 14 was operated by the participant to adjust socket volume. The researcher verbally directed the participant when to tighten or loosen the socket. Socket volume was adjusted in one-step increments only, where each step was a 4.75 mm cable length change, which corresponded to a socket volume change between 0.27% and 0.37% in this study. All participants started their test session at the neutral setting, that is, socket panels flush with the socket wall. Socket volume adjustments were made only during walking except for one participant (participant 2) who did not feel comfortable making adjustments while walking, so made them during standing.
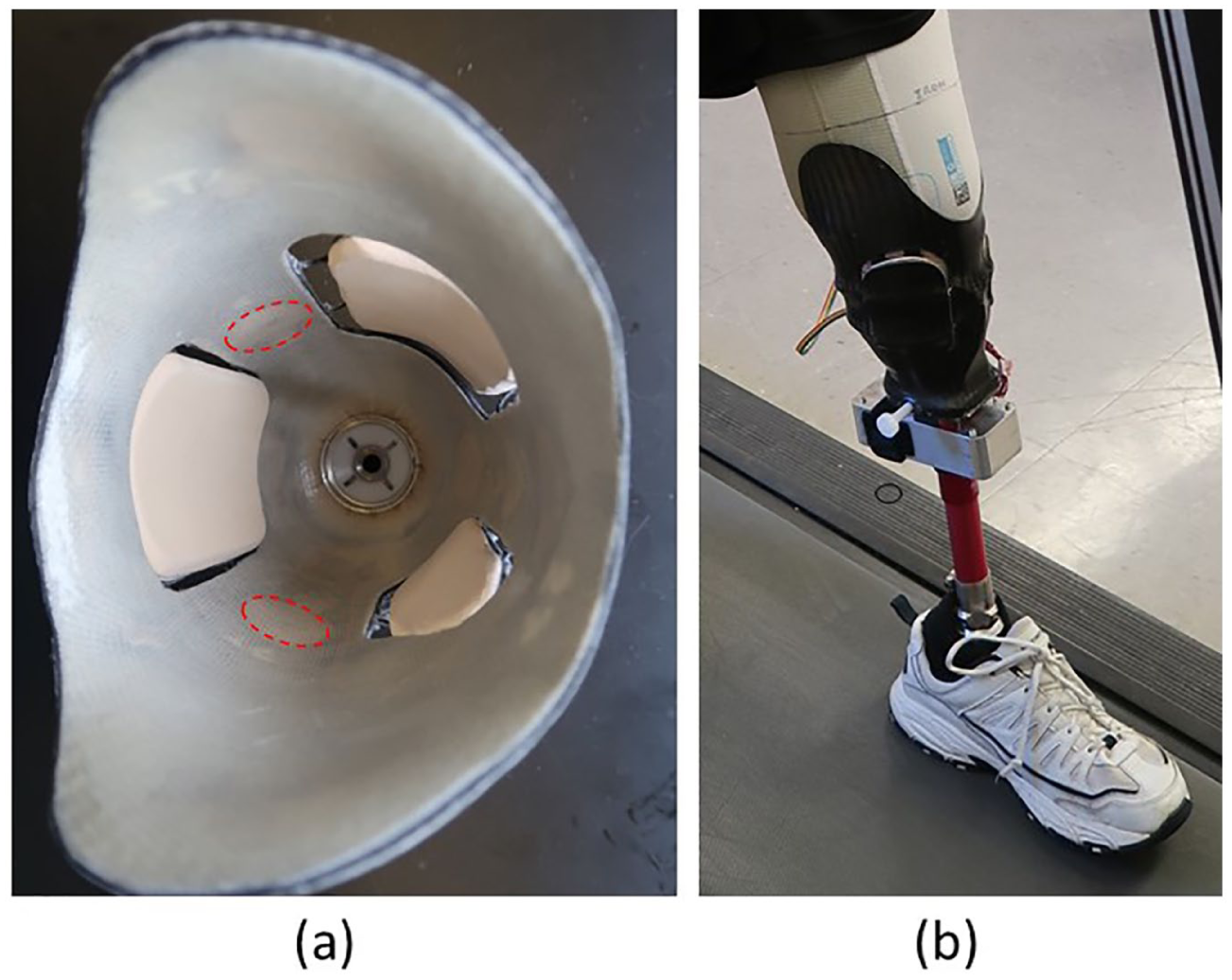
Test prosthesis. (a) Adjustable socket panels were positioned anterior medial, anterior lateral, and posterior; inductive sensors to measure distance to the target in the liner were positioned at posterior medial mid-limb and posterior lateral mid-limb locations (dashed red circles). (b) The motor to adjust length of the cable through the socket panels was positioned beneath the socket.
Testing protocol
The testing protocol is summarized in Appendix 2. Upon arriving at the lab for testing, participants sat for 10 min with their prosthesis donned to achieve a homeostatic condition. Participants’ age, time since amputation, weight, residual limb length from the mid-patellar-tendon to the distal end of the limb, mid-limb circumference, and presence or absence of peripheral vascular disease and/or diabetes were recorded. Participants then doffed their prosthesis and their residual limb was instrumented with thin-tape electrodes for bioimpedance analysis to monitor fluid volume in the posterior region. 15 Participants walked in the instrumented socket with the panels in the neutral (flush) position. If the socket was uncomfortably large, sock ply was adjusted to achieve a comfortable setting. Participants donned the instrumented prosthesis and left the lab accompanied by the researcher. As they walked to the start of the testing path (~10 min), participants were permitted to adjust the socket panels and select an optimum socket volume. After a 5 min sit, participants walked continuously along a level asphalt trail while they adjusted socket volume using a mobile phone app to control the motor-driven, cabled-panel, adjustable socket. Participants increased socket volume one motor-step increment every 2 min, upon cuing by the researcher. The process was continued until participants indicated that their socket fit was unacceptable, that is, participants would normally add a sock. Participants then sat on a nearby bench for 5 min. Before starting the next phase, participants were asked to adjust their socket volume to be acceptable for walking. Several participants reduced the socket volume to their initial setting while others only reduced the socket volume by a one motor-step increment. The protocol was continued, socket volume was reduced one motor-step increment every 2 min until participants indicated that their socket fit was unacceptable, that is, participants would normally remove a sock. Participants then adjusted the socket to a comfortable setting and returned to the lab.
Data analysis
Participants’ socket volume was expressed as a percent change relative to the participant’s self-selected optimum socket volume at the start of walking on the trail. Participants’ maximum-tolerated percent socket volume for the enlargement phase of the protocol and minimal-tolerated percent socket volume for the reduction phase of the protocol were tabulated. Limb fluid volume data were expressed as a percent change from a reference value, the mean of the minimum fluid volume during each of the first 10 steps at the outset of the protocol after the participant arrived at the trail.
Each of the two bouts of walking for each participant (enlargement, reduction) was segmented into steps as described previously. 12 The minimum percent limb fluid volume and the time during stance phase it occurred was calculated for each step, and the mean of the posterior medial mid-limb sensed distance and posterior lateral mid-limb sensed distance at the same time point was also calculated. We used minima during stance phase of each step as our metric because, in prior studies, it was shown to well-correlate with socket volume.12,13 It was therefore a strong candidate as a socket fit metric for use in automatically adjusting sockets. Using these data, we calculated the percent limb fluid volume change and sensed distance change from an adjustment, limb fluid volumetotal change and sensed distancetotal change, respectively, as listed in Figure 2. We also calculated subsets of these variables—the immediate rapid change upon adjustment and the gradual change over 2 min after an adjustment was completed.
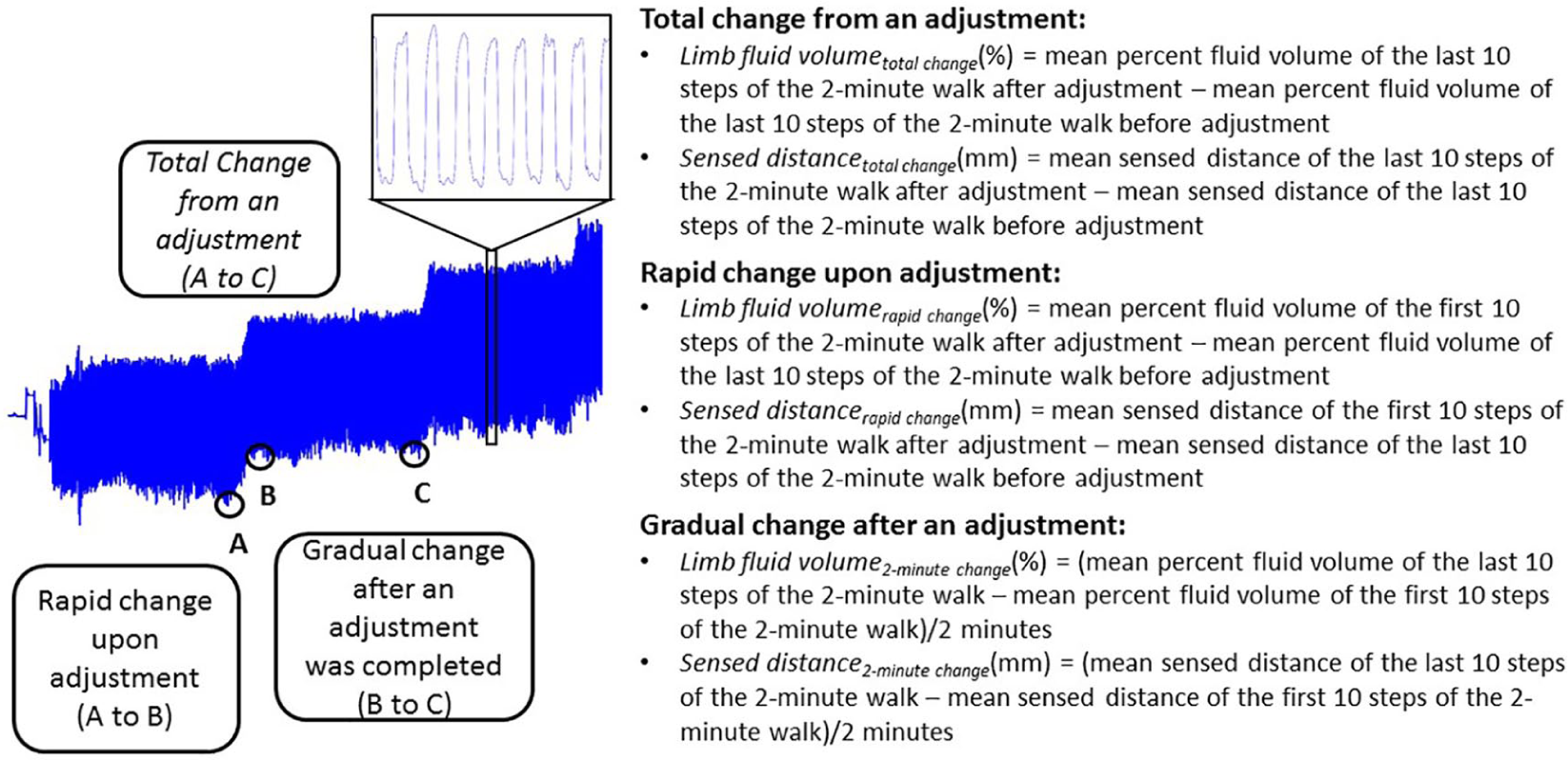
Limb fluid volume versus time results from a test session illustrating calculations executed on the data. Comparable calculations were conducted on sensed distance data at the same time points.
For each participant, we calculated the “most stable” socket volumes during each socket adjustment phase (enlargement, reduction). The most stable socket volume was defined as that at which limb fluid volume and sensed distance experienced their lowest rates of change (closest to zero) over the 2 min after an adjustment was made (B to C in Figure 2). Rate of change was calculated as the slope of a least-squares best-fit line to the data. We tested the hypothesis: the most stable socket volume was the user’s optimum socket volume (set at the outset of walking on the trail) for both socket enlargement and socket reduction.
Testing for normality using a Shapiro–Wilk test demonstrated that some of the variables were not normally distributed. A Wilcoxon Signed Rank test with a test statistic of 0.05 was used for all comparisons.
Results
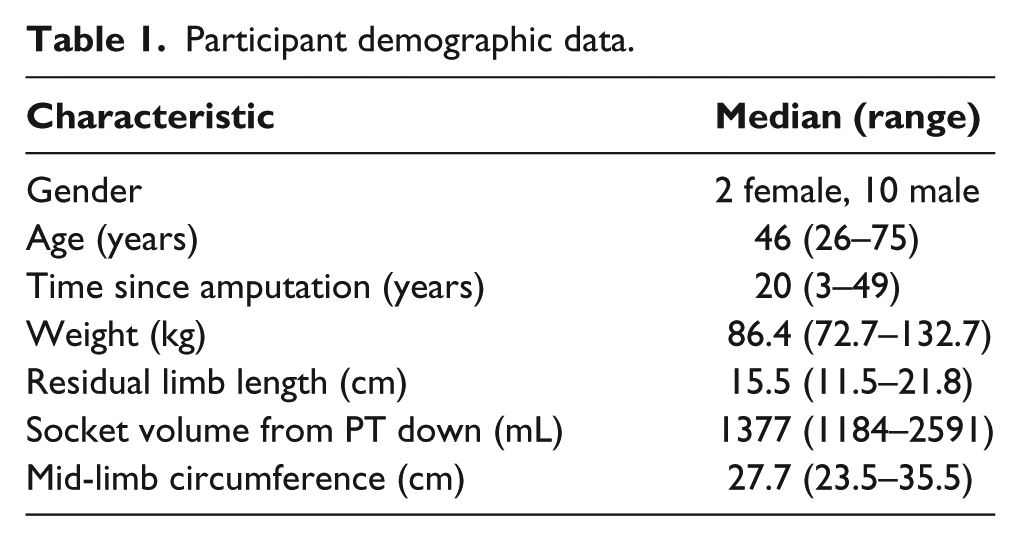
A total of 12 people with transtibial limb amputation participated in this study. All participants had their amputation as a result of trauma and were K-3 or K-4 level 16 ambulators. Participant demographic data are summarized in Table. 1. None of the participants had been diagnosed with peripheral vascular disease or diabetes. All participants used locking pin suspension and energy storage and return feet in their normal prosthesis, and in their test prosthesis. Nine participants did not wear socks, and three participants did wear socks (participants 2, 3, and 4).
Participant demographic data.
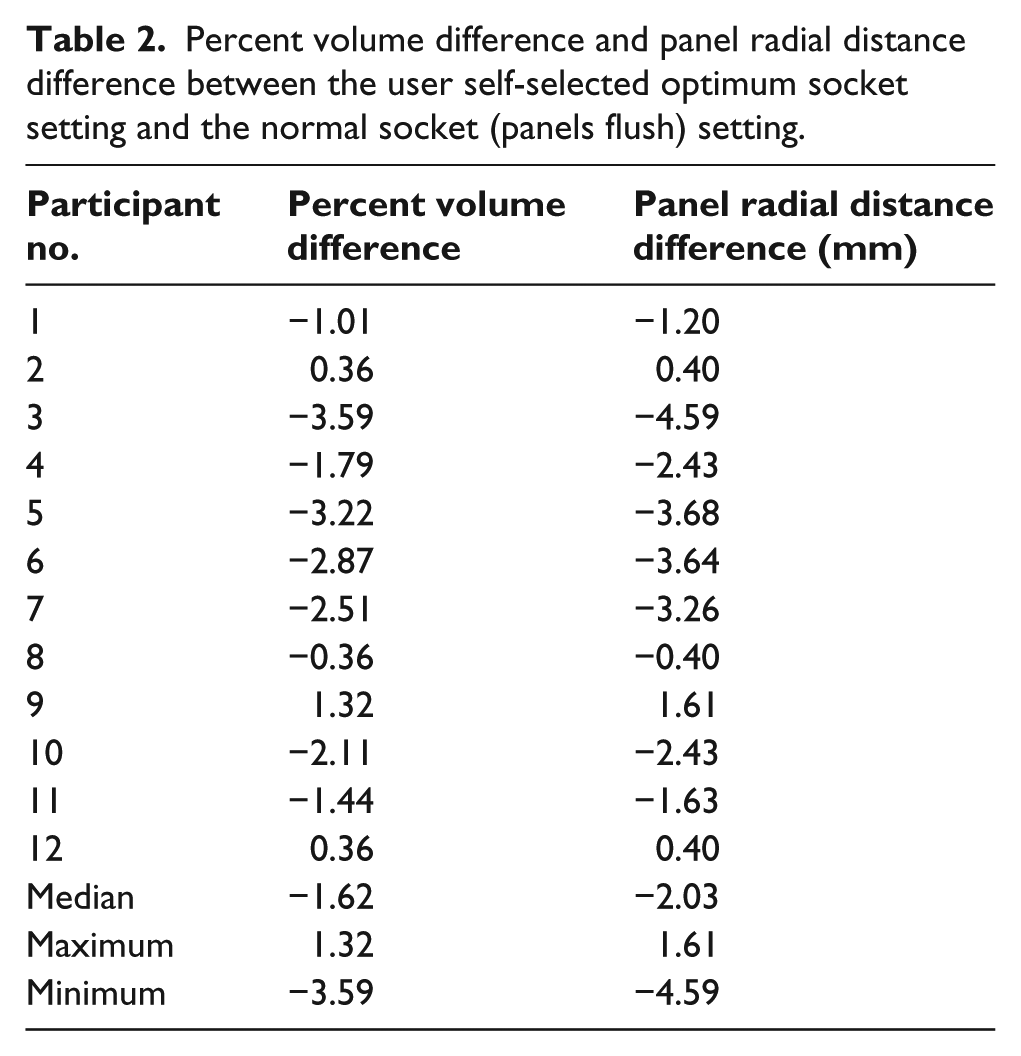
Nine of the 12 participants reduced their normal socket volume to achieve an optimal fit (Table 2). The median volume difference between the participants’ self-selected optimum socket and the normal socket was −1.62% of the self-selected optimum socket volume (range = −3.59% to 1.32%).
Percent volume difference and panel radial distance difference between the user self-selected optimum socket setting and the normal socket (panels flush) setting.
The median of the maximum percent socket volume tolerated by participants during the enlargement phase was 1.44% (range = 0.37% to 3.95%) relative to participants’ self-selected optimum socket volume, and the median of the minimum socket volume tolerated during the reduction phase was −1.26% (range = −3.94% to 0.35%) relative to participants’ self-selected optimum socket volume. Socket volume ranges selected by each participant are included as colored line segments in Figure 3(a) and (b).
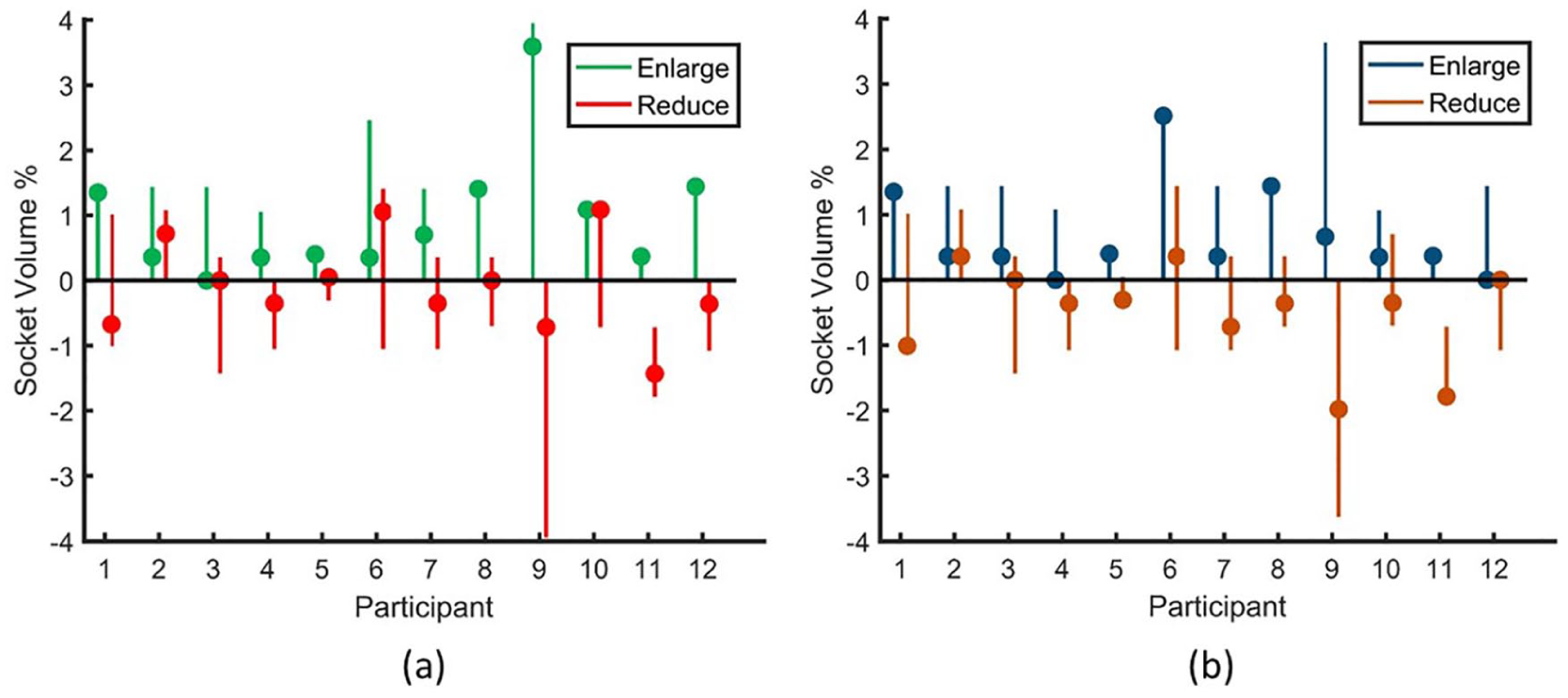
Most stable socket volume. (a): percent socket volume relative to user self-selected optimum at which rate of percent limb fluid volume change was closest to zero. (b): percent socket volume relative to user self-selected optimum at which rate of sensed distance change was closest to zero. The dots represent the most stable socket volume. The line segments indicate the range of socket volume during testing.
Total change from an adjustment
Intermittent incremental socket volume enlargements significantly increased limb fluid volumetotal change (p < 0.001), but did not significantly affect sensed distancetotal change (p = 0.063). Intermittent incremental socket volume reductions significantly decreased both limb fluid volumetotal change and sensed distancetotal change (p < 0.001). Limb fluid volumetotal change and sensed distancetotal change were significantly greater for enlargement than reduction (p < 0.001) (Figure 4).
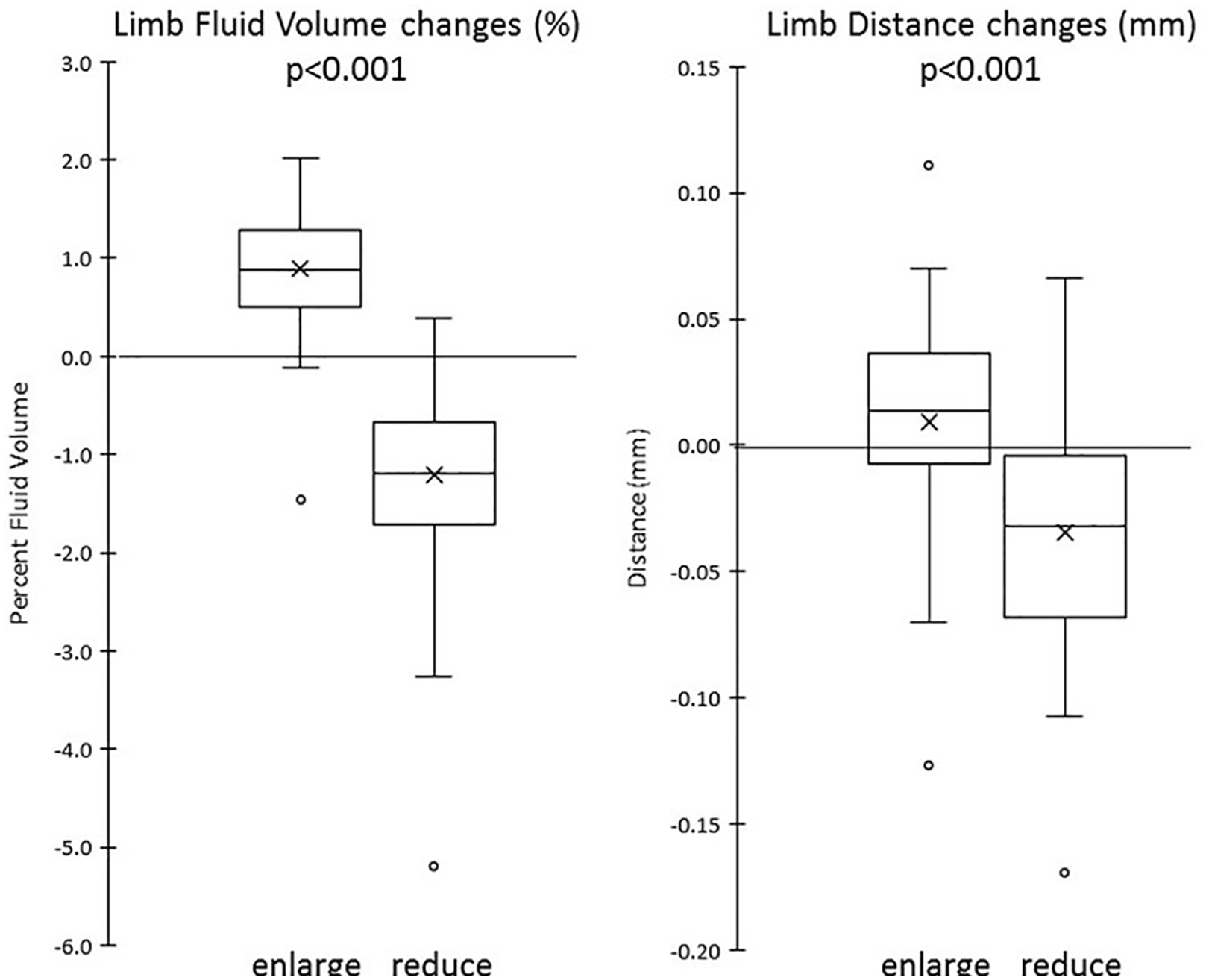
Total change from an adjustment. Left panel: percent limb fluid volume; right panel: sensed distance.
Rapid change upon adjustment
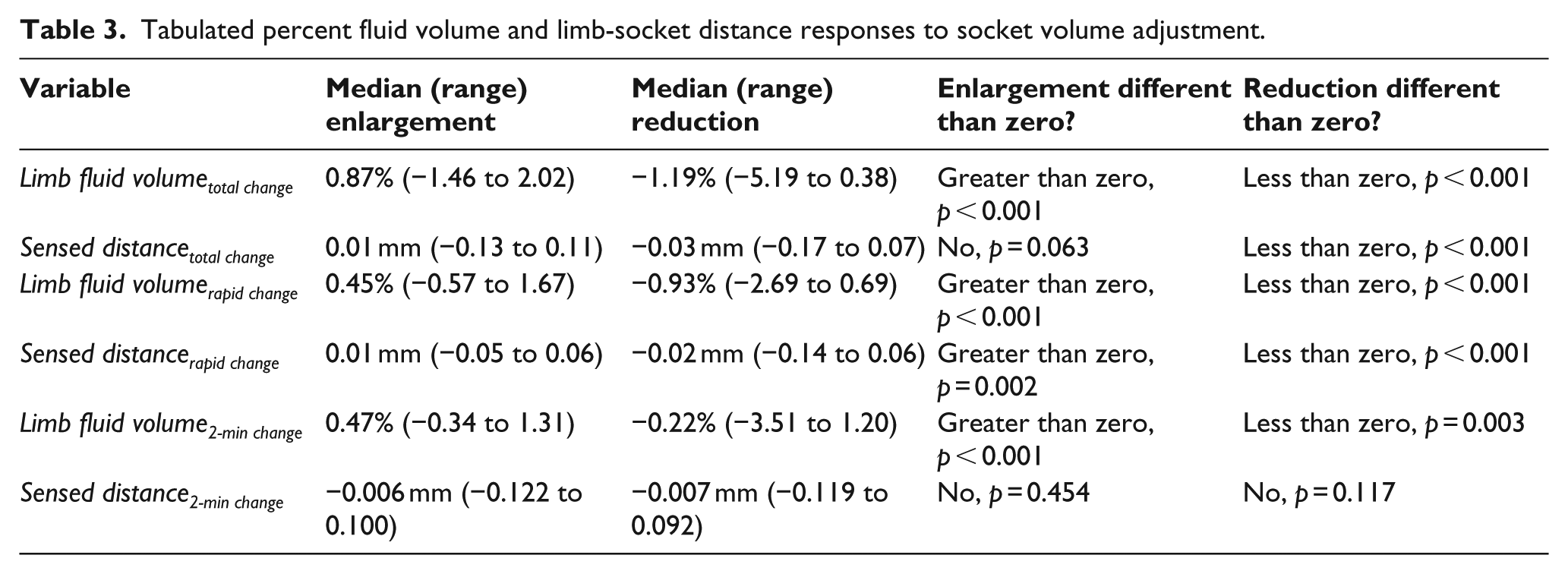
Upon socket enlargement, both limb fluid volumerapid change and sensed distancerapid change were significantly greater than zero (p < 0.001 and p = 0.002, respectively; Table 3). Upon socket reduction, both were significantly less than zero (p < 0.001). Both limb fluid volumerapid change and sensed distancerapid change were significantly greater for enlargement than reduction (p < 0.001).
Tabulated percent fluid volume and limb-socket distance responses to socket volume adjustment.
Gradual change over 2 min after an adjustment was completed
During the 2 min after socket enlargement was completed, limb fluid volume2-min change was significantly greater than zero (p < 0.001), and sensed distance2-min change was not significantly different than zero (p = 0.454) (Table 3). During the 2 min after socket reduction, limb fluid volume2-min change was significantly less than zero (p = 0.003), and sensed distance2-min change was not significantly different than zero (p = 0.117). During the 2 min after adjustment, limb fluid volume2-min change was significantly greater for enlargement than reduction (p < 0.001), and sensed distance2-min change was not significantly different for enlargement compared with reduction (p = 0.958).
Most stable socket volume
The null hypothesis that the most stable limb fluid volume was at the user’s optimum socket volume was rejected (p = 0.035). Ad hoc analysis considering enlargement and reduction separately showed that after socket enlargement the true median of the percent socket volume that induced the most stable limb fluid volume (0.55%, range = 0.00% to 3.59%) was significantly different than the user’s optimum socket volume (p = 0.003), and that after socket reduction (−0.18%, range = −1.43% to 1.08%) was not significantly different than the user’s optimum socket volume (p = 0.759) (Figure 3(a) and (b)).
The null hypothesis that the most stable sensed distance was at the participant’s self-selected optimal socket volume at the start of the protocol was not rejected (p = 0.420). The median percent socket volume that induced the most stable sensed distance after socket enlargement was 0.36% (range = 0.00% to 2.51%) relative to the participant’s self-selected optimal socket volume, and that after socket reduction was −0.35% (range = −1.98% to 0.36%) relative to the participant’s self-selected optimal socket volume.
Discussion
The purpose of this study was to determine if small intermittent changes in socket volume could be used to manipulate transtibial prosthesis users’ residual limb fluid volume during ambulation without detrimentally affecting socket fit. This effort is relevant toward the development of sockets that automatically adjust volume, a goal pursued by a number of researchers.17–22 Typically, automatically adjusting sockets are equipped with sensors that monitor socket fit, and a control system and actuator adjust the socket to maintain fit based on sensor data. For example, for the inductive sensors used here, the control system might adjust socket size during walking to maintain the fit metric (minimum sensed distance within a step) at a value set by the user and prosthetist in the clinic. When the sensed distance decreased the socket would enlarge, and when it increased the socket would reduce. Although such an automatically adjusting socket is “reactive” instead of “anticipatory,” it may be effective in clinical practice because it senses a change in fit far sooner than the user 13 and makes small adjustments accordingly. Results from this study support the hypothesis that intermittent incremental increases in socket volume during walking, near prosthesis users’ preferred socket volume, increase limb fluid volume and maintain sensed distance. Percent limb fluid volume significantly increased from before adjustment to 2 min after adjustment was completed, while sensed distance was not significantly different (Table 3). We expect this happened because residual limb fluid volume continued to increase after socket enlargement was completed, resulting in a sensed distance from the socket 2 min later near its previous value before socket enlargement was initiated. This capability to adapt to a small socket enlargement by increasing limb fluid volume is expected to be clinically beneficial and may be an effective volume accommodation strategy for prosthesis users to implement during walking, provided adjustments are executed near their preferred socket volume.
Results from this study support the hypothesis that intermittent incremental decreases in socket volume during walking decrease limb fluid volume, but do not support the hypothesis that intermittent incremental decreases maintain sensed distance. Instead, participant limbs were closer to the socket 2 min after adjustment was completed than before adjustment. This capability to avoid rapid fluid volume loss upon socket reduction is expected to be clinically beneficial. Reducing socket volume had the intended effect of making the socket tighter. The duration of this effect, however, that is, how long a closer distance to the socket is maintained, is unknown since each adjustment in socket size was maintained for only 2 min. Studies holding adjustments for longer durations would be needed to address this issue.
We suspect that part of the reason sensed socket distance was better maintained during enlargement than reduction has to do with health characteristics of the participants tested. All participants in this study had their limb amputation as a result of trauma and were active prosthesis users without peripheral arterial disease or diabetes. In previous studies, participants without these co-morbidities often demonstrated fluid volume gain and retention during high activity.23,24 In other words, their normal tendency was to gain fluid volume during ambulation. We propose that this quality in this study benefited and helped stabilize sensed distance during and after enlargement. During and after reduction it slowed fluid volume loss so that participants’ sockets stayed tight. Possibly, the three participants (participants 8, 11, and 12; Appendix 3) who instead followed the hypothesis of constant sensed distance during the socket reduction phase of the protocol had different physiologic response processes than the others. This is conjecture and the underlying physiologic basis would need to be identified through rigorous scientific analysis.
Participants preferred a socket size smaller than their normal socket size (panels flush; Table 2). We investigated if compression of the Nickelplast covering the panels contributed to this result (Appendix 4). The panel radial position difference between users’ self-selected optimum socket size and flush far exceeded Nickelplast compression for limb-socket pressure at comparable sites during walking reported in the literature. Thus, it is unlikely pad compression explains why participants preferred a socket size smaller than their normal socket size. We suspect participants preferred a smaller socket size because they preferred the sense of stability it induced during outdoor ambulation and because the test prosthesis was heavier than their normal prosthesis.
Unlike this study, results from a prior study where a single larger socket reduction was conducted (⩾ 0.7 percent socket volume) showed gradual fluid volume increases and gradual sensed distance decreases after reduction. 9 Possibly the larger socket reduction (median of 3.5× more than in this study) induced partial venous occlusion after adjustment, restricting venous outflow and causing fluid volume to increase. Whatever the reason, this difference in results between the two studies points to the importance of considering the magnitude of socket volume adjustment when the prosthesis user makes manual adjustments, and when designing computer-controlled sockets that adjust automatically. Small adjustments may be more favorable.
In this study, we do not know if and how much participant residual limbs displaced proximally or distally in the socket at different socket size settings. We suspect that the sensors positioned mid-limb on the side of the socket registered a sensed distance change before proximal or distal displacements occurred since they were extremely sensitive and the socket volume changes were small. However, a separate sensor to monitor limb distal position would need to be added to make this conclusion.
We observed that the three panels for the single cable adjustable sockets used in this study “floated” while the participant walked, even though cable length was constant. In other words, on occasion, one panel moved outward while another panel moved inward, which may have shifted the anterior-posterior position or medial-lateral position of the limb in the socket. Fluid volume data appeared relatively insensitive to floating panel movements, presumably because a large region of the residual limb was monitored using the sensing technology (bioimpedance analysis). Sensed distance data were more sensitive to this action presumably because it monitored from local positions. We suspect the floating panels may be a reason for the higher variability in sensed distance data than fluid volume data in this study (Appendix 3).
Results from this study demonstrated that the most stable limb fluid volume was not at the prosthesis user’s self-selected optimum volume. However, the socket volume that induced the most stable sensed distance was not different than the user’s self-selected optimum. Prosthesis users may sense distance to the socket better than fluid volume when selecting an optimum socket volume. However, this is conjecture and would need to undergo rigorous scientific testing to validate.
This study was conducted on participants who had their limb amputation as a result of trauma, thus it is unknown if findings apply to people with amputation from other etiologies. Similarly, participants did not have peripheral arterial disease or diabetes. Because the study was relatively short in duration, median time of 67 min from leaving the lab to returning to the lab, it is unknown how limb fluid volume will change in longer time frames.
Conclusion
The observation that participants in this study, all active prosthesis users without peripheral arterial disease or diabetes, increased limb fluid volume upon incremental socket enlargement and achieved a consistent distance to the socket 2 min later suggests that intermittent incremental socket volume increases during walking may be an effective accommodation strategy to counter limb fluid volume losses that may occur during other times of the day, for example, during standing or sitting.
Footnotes
Appendix 1
Appendix 3
Appendix 4
Author contribution
All authors contributed equally in the preparation of this manuscript.
Associate Editor: Nerrolyn Ramstrand
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was based on work supported by the US Army Medical Research Acquisition Activity (USAMRAA) under contract no. W81XWH-16-C-0020. Any opinions, findings and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the USAMRAA.