
Abstract
Abstract
Purpose
To evaluate the efficacy of ankle foot orthoses (AFOs) prescribed in the community for children with cerebral palsy (CP).
Methods
Fifty-six children (32 boys and 24 girls, mean age 8.9 years, range 4–17) who were diagnosed as having CP were enrolled. They were grouped according to the type of CP, diplegic (n = 38) and hemiplegic (n = 18). Three-dimensional gait analyses while patient were barefoot and with AFOs were obtained and analyzed.
Results
The spatio-temporal findings were the most significantly changed as a result of AFO use. In the hemiplegic group, stride length was 11.7% (p = 0.001) longer with AFOs in both affected (10.2%) and non-affected (12.4%) legs, and cadence was reduced by 9.7%; walking speed was not affected. In the diplegic group, stride length with AFOs was 17.4% longer compared to barefoot (p < 0.001) and walking velocity improved by 17.8% (p < 0.001); cadence was unchanged. AFOs also increased ankle dorsiflexion at initial contact in both groups. In the hemiplegic group, AFOs produced an average 9.4° increase of dorsiflexion at initial contact (IC) on the affected side (p < 0.001) and 5.87° on the unaffected side (p = 0.007), and an increase of 9.9° (p < 0.001) dorsiflexion at swing, on the affected side. In the diplegic group, dorsiflexion at IC was increased by 13.4° on the right side and 7.8° on the left side (p = 0.05; p > 0.001, respectively) and an increase of 6° (p = 0.005) at swing. In the hemiplegic group of patients, knee flexion at initial contact on the affected side was reduced by 8.5° (p = 0.032) while in the diplegic group we found no influence. The number of patients that reached symmetry at initial double support tripled (from 5.6 to 16.7%) with the use of AFOs.
Conclusions
Our results showed that the use of AFOs improves spatio-temporal gait parameters and gait stability in children with spastic cerebral palsy. It has a lesser effect on proximal joint kinematics. Children with spastic hemiplegia display greater improvement than those with spastic diplegia.
Introduction
Equinus gait, the most common deformity in children with cerebral palsy (CP), is usually accompanied by additional abnormalities at the upper segments of the lower extremities [1, 2]. The use of ankle–foot orthoses (AFOs) is widely recommended to prevent the development or progression of this deformity and to improve the dynamic efficiency of the child's gait [3].
Physicians usually prescribe AFOs following clinical examinations and observation of the child's walking patterns [4]. In an epidemiological survey of two adjacent health districts, Morris et al. [4] found that most clinicians were uncertain about the indications for prescribing orthoses, and whether or not they did so was largely determined by personal preference. The proposed effects associated with AFOs include assistance in foot clearance at swing, correction of foot pre-positioning at initial contact, stability in stance phase and reduction of energy expenditure [3, 5, 6].
Most of the children referred to our gait analysis laboratory were using an AFO that had been prescribed for them by various health care practitioners. The purpose of the current study was to evaluate the efficacy of AFOs prescribed in the community to children with CP. It should be mentioned that our patient have been using AFOs on a regular basis; they then removed them temporarily and then underwent the gait study. We assessed the AFOs’ contribution to these children in our gait laboratory, using the parameters of time–distance, stride analysis, foot pre-positioning, and response to loading.
Patients and methods
This retrospective study was designed to evaluate CP children who were referred to our laboratory for three-dimensional (3D) gait analysis. The referring physicians were pediatric orthopedic surgeons, pediatric neurologists, and rehabilitation specialists. Inclusion criteria were current habitual use of AFOs and capability of independent walking. The gait analysis included conditions of barefoot and use of AFOs at the same session. The orthoses were divided into two main types, rigid and articulated, and gait performance was compared between them.
Study cohort
Fifty-six children with cerebral palsy (32 boys and 24 girls, mean age 8.9 (3.5) years, range 4–17) took part in the study. They were grouped according to CP type, diplegic (n = 38) and hemiplegic (n = 18). All parents gave their signed informed consent for the children to participate.
Gait analysis
The children underwent gross motor function classification scale (GMFCS) [7] assessment as well as a thorough physical assessment consisting of manual muscle testing, joint range of motion, joint and muscle stiffness testing. 3D gait analysis was performed using an 8-camera system. (VICON 612 motion analysis system Oxford Metrics, UK). Retro-reflective markers were applied on anatomical landmarks to capture gait performance. Kinetic data were collected using four AMTI force plates (Advanced Mechanical Technology Inc., Watertown, MA, USA). The children were asked to walk along a 12-m walkway at self-selected velocity, first barefoot and then with their AFOs. Data on five trials were collected for each mode to check for reproducibility, and one was chosen as the most representative performance for further analysis. Stride analysis was based on the force plate signal output, i.e., ground reaction force.
Index of symmetry
The index of symmetry is a parameter that compares the performance of one limb to the other during the gait cycle. If both limbs perform in exactly the same manner, their index of symmetry is scored 100%. The index is calculated by dividing right side data by left side data for each subject multiplied by 100. Patients that meet the criteria of being within 10 of 100% symmetry are considered to have a positive index of symmetry [8].
Statistical analysis
SPSS 11.5 for Windows (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses, which included the paired t-test, scatter plots and Person's correlation coefficient or Spearman's rank order, according to the distribution of the variables (symmetric quantitative variables, gauss curve or ordered categories). One-way analysis of variance was applied to examine the effectiveness of AFOs vis-à-vis the children's diagnoses and the types of orthoses they used. All affected feet were referred to as the “right” side and the unaffected as the “left” side in the hemiplegic groups for statistical purposes.
Results
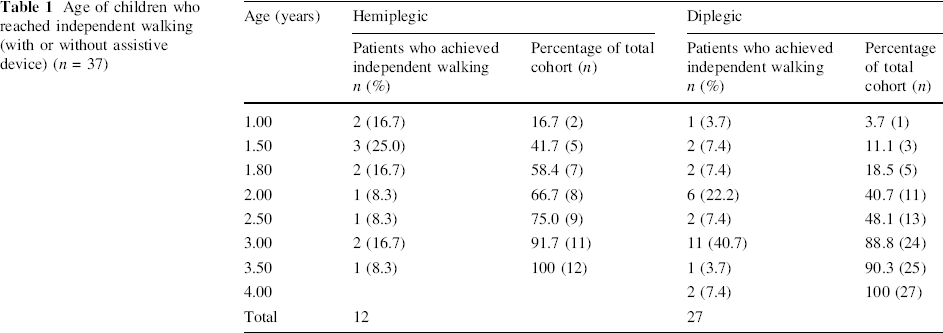
In the hemiplegic group, 7/12 (58.3%) children reached independent walking at the age of 18 months and 11/12 (91.7%) at the age of 3 years (median 1.8 years, Table 1). They were all classified as being at gross motor function classification system (GMFCS) level I [7]. In the diplegic group, only 5/27 (18.5%) children acquired independent walking by the age of 18 months, and 24/27 (88.8%) at the age of 3 years, (Table 1). Fifteen of the diplegic children were classified as being in GMFCS level I and 23 in level II. An additional four patients that were classified as GMFCS level III, were omitted from the study.
Age of children who reached independent walking (with or without assistive device) (n = 37)
The effect of AFOs on time–distance parameters
Table 2 summarizes the comparative spatial–temporal parameters while walking with AFOs and barefoot. Stride length was significantly increased (11.7 cm, p < 0.001) with the use of AFOs. The increases were recorded for both the rigid and articulated AFOs (p < .001 and p < .001, respectively), and there was no significant difference between the two types (F = .439; p = 0.511). In the hemiplegic group, stride length and step lengths of the affected and unaffected sides were significantly increased (p = 0.01, p = 0.026, and p = 0.01 respectively); specifically, the group's stride length increased by 11.2% (11.4 cm). In the diplegic group, stride length and step lengths (right and left) increased significantly as well (p < 0.001), with stride length increasing by 17.6% (12.3 cm).
The time–distance parameters of the hemiplegic and diplegic subgroups
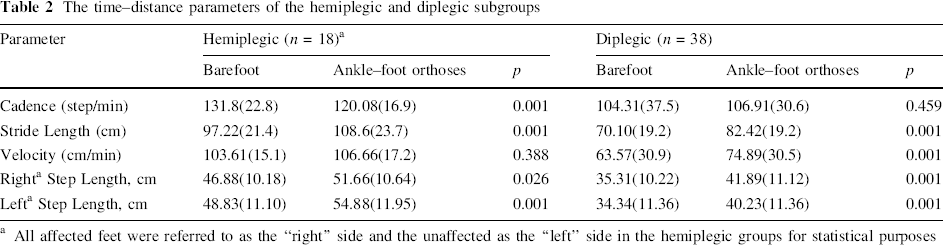
All affected feet were referred to as the “right” side and the unaffected as the “left” side in the hemiplegic groups for statistical purposes
Cadence in the hemiplegic group was a significantly (p < 0.0010) reduced by 9.7% 11 steps per minute. It underwent no change in the diplegic group (p = 0.459).
Walking velocity increased in both groups (Table 2). It increased by 17% in the diplegic group (10.5 cm/min, p < 0.001), but only marginally in the hemiplegic group (p = 0.388).
Stride analysis included the following temporal parameters: stride time, step time, stance period, single support and double support, the latter as percentage of gait cycle.
Table 3 represents selected temporal parameters. No significant changes in stride analysis were observed in the diplegic group, except for left double support (p = 0.041) whereas in the hemiplegic subjects stride time and step time (for both limbs) and stance phase for the affected side increased significantly (p < 0.001, p = 0.003, p = 0.009, and p = 0.012 respectively).
Stride analysis including the temporal parameters stride time, step time, stance period, single support and double support periods
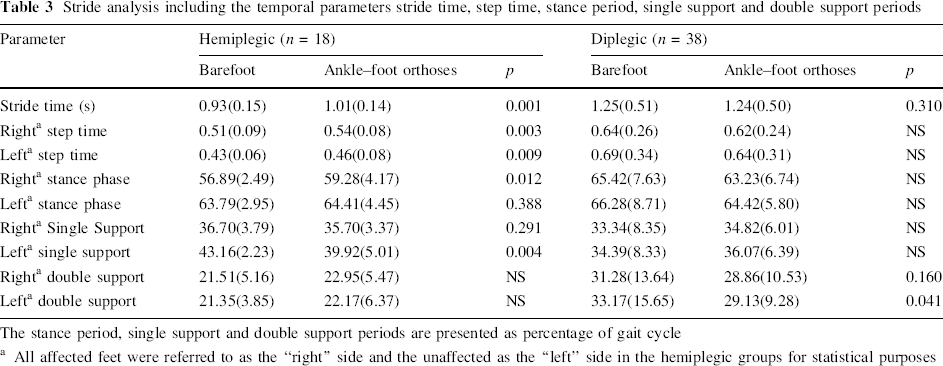
The stance period, single support and double support periods are presented as percentage of gait cycle
All affected feet were referred to as the “right” side and the unaffected as the “left” side in the hemiplegic groups for statistical purposes
The efficacy of AFOs at stance phase
AFO produced an averaged increase of 8.5° in ankle dorsiflexion at initial contact compared to walking barefoot (p < 0.001). The change was 11.4° on the affected side for the hemiplegic children (p < 0.001) and 5.9 on their unaffected side (p = 0.007). Ankle dorsiflexion of the diplegic children was significantly improved by 13.5(19.8)° on the right side (p = 0.56) and 7.8 (10.8)° on the left side, (p < 0.001) (Table 4). The type of AFO was of borderline significance: the articulated type increased ankle dorsiflexion by 4.3 (p = 0.060) and the rigid type by 2.2 (p = NS). Knee flexion at initial contact with the use of AFOs was reduced by 7.4° (p = 0.032) in the hemiplegic group, while no significant reduction of knee flexion was observed in the diplegic group. Neither the knee nor the ankle were significantly affected by the use of AFOs during loading response. The knee was not affected in single support, neither by rigid nor by articulated AFOs (Figs. 1, 2).
Kinematic data comparing the angles of each joint for the different gait events
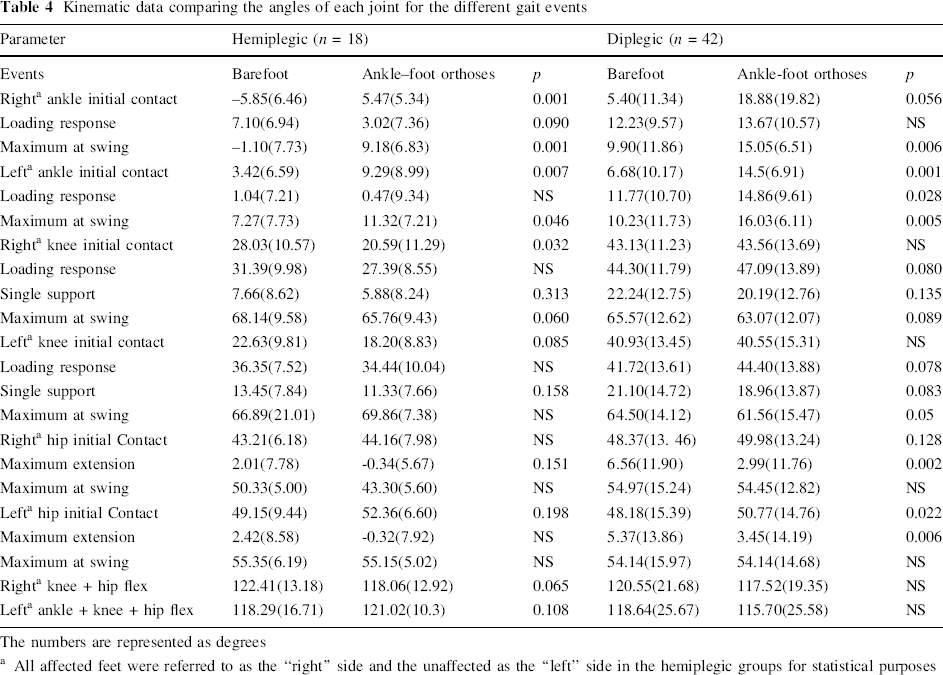
The numbers are represented as degrees
All affected feet were referred to as the “right” side and the unaffected as the “left” side in the hemiplegic groups for statistical purposes
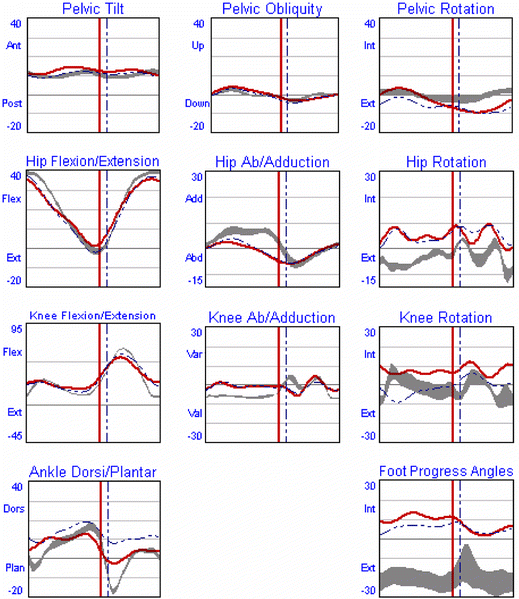
Kinematic results of the affected side of a left hemiplegic patient. The red (solid) line represents the barefoot mode the dotted line represents the braced mode
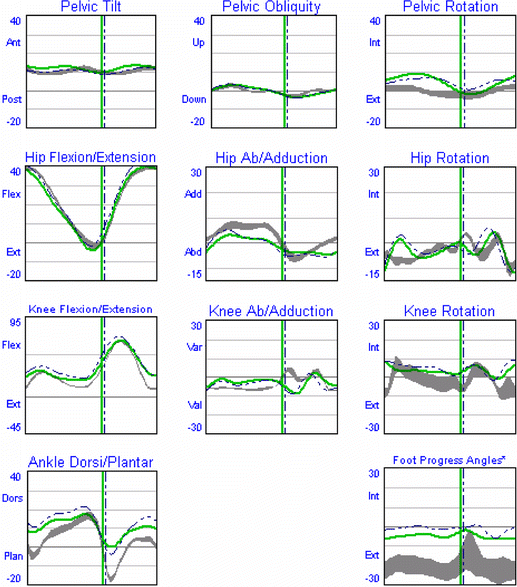
Kinematic results of the unaffected side a left hemiplegic patient. The green (solid) line represents the barefoot mode the dotted line represents the braced mode
The effect of AFOs on the swing phase
To assess the effect of AFOs on the swing phase, we looked at the maximal knee flexion in mid-swing, maximal hip flexion at terminal swing and maximal ankle dorsiflexion during swing phase. Ankle dorsiflexion was significantly increased by the use of AFOs in both groups (p = .046 to <0.001). Knee flexion and hip flexion were not significantly reduced by the use of AFOs (Table 4).
We evaluated foot clearance by calculating the combined maximal flexion of the two joints. Combined flexion at the knee and hip joints underwent a significant reduction in lower extremity, declining on both sides (p = 0.028 and 0.041) for the entire sample, but not significantly for the groups in isolation. However, within the hemiplegic group we found a borderline reduction in the combined flexion on the affected side.
Index of symmetry
The main effect of AFOs on the symmetry of gait was observed in the hemiplegic group.
The number of patients that achieved symmetry at the initial double support period of the gait cycle increased from 5.6 to 16.7% with the use of AFOs. Additionally, the percentage of these cases rose by approximately 22.3% when we measured total double support time (Table 5). Stance period rose from 38.9 to 66.7%. In the hemiplegic group, the symmetry in step length was reduced with the use of braces; this change, however, was not significant (p = 0.069). We applied the paired t-test to see if the use of AFOs made any of the gait parameters shift towards a more symmetric pattern and found no significant change in either group (p = 0.127).
Index of symmetry
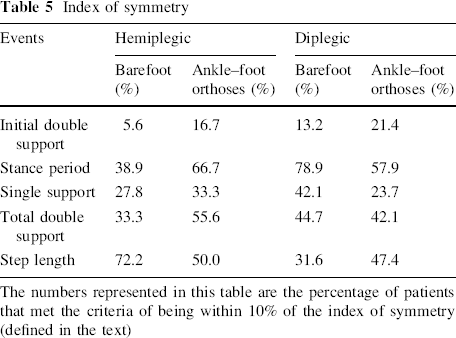
The numbers represented in this table are the percentage of patients that met the criteria of being within 10% of the index of symmetry (defined in the text)
Discussion
The aim of this study was to retrospectively assess whether AFOs prescribed in the community health care environment are effective in improving the gait of children with two types of spastic CP, hemiplegic and diplegic. We measured the spatio-temporal parameters and gait kinematics of children who were using AFOs prescribed by their treating physicians, and compared the available data of various gait parameters in order to measure the benefits of using AFOs. In our study design, the patients that were using AFO's on a regular basis had them removed for the purpose of the study at the same session. We should take into consideration that different results might have been obtained if these patients had been out of their AFOs for several weeks. Since our clinical practice is to perform gait analysis of patients that use AFOs regularly in and out of their braces in a single session, it was impractical to take off the AFOs for a longer period of time. This point should therefore be considered in future studies on this subject.
The division of braces into rigid and articulated types was done according to function and not definition, since they were prescribed by a number of physicians and produced by different manufacturers. It should be mentioned that the majority of the AFOs were the flexible type; different orthoses are prescribed, with there being no general consent on which type is preferable for improving gait velocity [9], energy expenditure [10] or other functions [11, 12]. Patients who have a tendency to crouch could benefit from a solid type AFO that induces knee extension or a ground reaction type AFO that prevents excessive foreword movement of the tibia and keeps the ground reaction force anterior to the knee. Patients with adequate knee extension and excessive equines will benefit from a hinged type AFO that allows dorsiflexion in the stance phase. Posterior leaf AFOs possess the advantage of conserving the energy during midstance, to be used for push-off in cases of a weak gastro soleus mechanism.
White et al. [3] and Dursun et al. [13] reported that the use of AFOs significantly increased walking velocity and stride length, but did not alter cadence. On the other hand, Buckon et al. [14] found that the use of AFOs in CP children increased stride length, reduced cadence but did not significantly change walking velocity. Some authors reported that AFOs reduced exertion during standing [15] and walking [5], while others [14] demonstrated that it had no effect on exertion and did not change oxygen consumption at self-selected velocity. The authors noted that the increase in velocity that had been demonstrated in long-distance walking, however, does indicate a reduction in energy costs [5]. Maltais et al. [10] concluded that a hinged AFO reduces oxygen uptake and the ventilatory cost of walking [10], while Suzuki et al. [6] calculated the energy expenditure index and stated that ambulation with flexible plastic AFOs requires more energy than walking barefoot.
In our study, we could not establish statistical differences between types of braces within the groups, since the further division for articulated and solid AFO yielded groups too small to draw any statistically supported conclusions. Our results, therefore, represent both types.
Our CP study population consisted of 18 children who were spastic hemiplegic and 38 children who were spastic diplegic. The following discussion relates to each group separately.
The spatio-temporal parameters were most significantly changed in the hemiplegic group, in which stride length was significantly longer with the use of AFOs in both the affected and non-affected legs. Cadence was reduced, while the walking speed was not significantly changed. The latter may be explained as a result of the reduction in cadence, but it may also be due to a “ceiling effect”, since the velocity in this group was close to the normal range [16]. Ankle dorsiflexion increased, better foot position and heel strike in both affected and unaffected sides were achieved, and knee flexion was reduced at initial contact. However, midstance was not significantly affected. These results are in agreement with some previous studies [17–19], while on the other hand Buckon et al. [20] recently concluded that AFO use did not markedly alter joint kinematics in children with spastic hemiplegia. We demonstrated that the use of AFOs in spastic hemiplegic children improved gait symmetry mainly in time parameters such as double support time, thus minimizing limp and body sway.
The stride length in the diplegic group was significantly longer as a result of AFO use. Their cadence was not changed, but velocity improved. Our results are in agreement with those of previous studies that showed an increase in velocity due to an increase in stride length, with no change in cadence [4, 13, 14, 17]. An increase in stride length is a benefit for children with CP, because it reflects better stability during stance. The conclusion that braces improve stability is supported by Abel et al. [17] in their study on diplegic subjects. Gait cycle begins with weight acceptance comprised of plantar flexion of the foot (“the first foot rocker”) and knee flexion as a response to the loading mechanism [15]. To accomplish this task, the ankle should reach a neutral position and the knee should be at full extension at terminal swing. Buckon et al. [14] reported that AFOs enabled proper foot pre-positioning at initial contact. We found that AFOs increased ankle dorsiflexion at initial contact, but the changes in the more proximal joints were not markedly significant. Our results partially agree with a study on diplegic children by Buckon et al. [14], in which they found that AFOs increased stride length, decreased cadence without change in velocity, and had no effect on joint kinematics.
As expected, AFOs increase ankle dorsiflexion at swing phase and thereby improve foot clearance. There was no significant change in either knee or hip kinematics in either of the study groups during the swing phase, although the degree of combined knee and hip flexion was marginally reduced in the diplegic group. The rationale of using the combined flexion was to evaluate if the increased dorsiflexion of the ankle at swing phase caused less elevation of the lower extremity, which may suggest a lesser displacement of the center of mass during gait.
The index of symmetry compares the function of each leg during gait, reflecting the amount of symmetry measured for a given subject. The index did not shift towards improvement in either of our study groups, but the improvement seen in some parameters is encouraging. This index had not previously been reported in children with CP, and it should be further evaluated and matched with other parameters such as pelvic obliquity and center of mass shifts.
We agree with Flett [21] that children with spastic hemiplegia display the greatest improvements in gait and functional mobility when using AFOs. Children with spastic diplegia were found to derive less benefit from the use of AFOs. In conclusion, our current results showed that the use of AFOs, prescribed on a clinical basis by doctors in the community, improves gait patterns and gait stability in children with spastic cerebral palsy. Other issues such as the role of braces in preventing contractures, the role of gait analysis in selecting specific types of AFOs for specific gait patterns or the role of timing (night time versus day time or half day versus full day use of braces) were not within the scope of this study, and should be further investigated.