
Abstract
Background and Purpose:
Passive dynamic ankle-foot orthoses have potential to facilitate return to running after a lower limb trauma. However, transitioning patients to new movement patterns that enhance passive dynamic ankle-foot orthoses benefits can pose a challenge. The purpose of this case study was to report biomechanical and functional outcomes for a patient utilizing a passive dynamic ankle-foot orthoses following completion of a session-based, midfoot strike run training program.
Case Description and Methods:
A patient using a passive dynamic ankle-foot orthoses to run due to surgically reconstructed tibia\fibula fracture underwent eight treadmill running sessions over 2 weeks while viewing continuous visual feedback on measured foot strike.
Findings and Outcomes:
After treatment, foot strike was changed from rearfoot to midfoot on the affected limb along with an 18% increase in mechanical work ratio of the ankle-foot-brace complex. Similar improvements were retained at one and five months following treatment.
Conclusion:
This report provides preliminary evidence that biofeedback-based foot strike training can enhance ankle-foot mechanical performance of patients using a passive dynamic ankle-foot orthoses to run.
Clinical relevance
For patients using a passive dynamic ankle-foot orthoses to run following lower limb trauma, supplementing standard rehabilitation programs with biofeedback-based footstrike training may improve biomechanical performance and running capability.
Keywords
Background
Returning to high-level function following severe lower limb trauma poses significant challenges for patients and their healthcare providers. Passive dynamic ankle-foot orthoses (PD-AFO) such as the intrepid dynamic exoskeletal orthosis (IDEO) pose one option to address these challenges and quickly return patients to physical activity and military duty.1,2 The IDEO is a custom-manufactured carbon fiber PD-AFO originally designed to facilitate running when prescribed in combination with the Return To Run clinical pathway - a program focused on plyometrics, strength, agility, and verbal run form coaching. 1
Run form coaching places particular focus on striking with the midfoot. As opposed to rearfoot, a midfoot strike theoretically maximizes PD-AFO mechanical leverage on posterior, elastic struts during loading response for energy return at push off. In contrast, a forefoot strike may cause excessive force through the rigid footplate and accelerate device failure. Switching foot strike from rear to midfoot has additionally been shown to alter knee joint net mechanical demands in able-bodied runners. 3 Thus, detailed study of changes in PD-AFO energetics and knee mechanical demands coinciding with footstrike manipulation could inform further development of training programs for IDEO users.
From a learning perspective, self-assessment of true foot strike is challenging. In a prior study of 46 experienced able-bodied runners, only 43%–56% of participants were able to accurately self-report their foot strike relative to gold standard high-speed video. 4 For PD-AFO users, impaired ankle-foot proprioception due to prior limb trauma and the mechanical constraints of a PD-AFO likely make footstrike perception even more difficult. To address this, session-based movement training programs supplemented with biofeedback on measured mechanics may be useful. In a prior study, eight sessions of run training over 2 weeks viewing real-time feedback on hip adduction kinematics proved effective in reducing pain and improving function for patients with patellofemoral pain for up to 1 month following treatment.5–7 Although promising, this style of program has not yet been evaluated for feasibility with complicating factors of low baseline endurance, limb trauma reconstruction, and orthotic devices.
The purpose of this case study was to report biomechanical and functional outcomes for a patient utilizing a PD-AFO due to prior limb trauma, following completion of a session-based, midfoot strike run training program.
Case description and methods
The patient was a male, U.S. Marine Corps Veteran who suffered an open, comminuted left tibia/fibula fracture due to a gunshot wound (27 years old at injury; Figure 1(a) and (b)). Over 27 surgeries were required to structurally preserve the left lower limb. Three years after injury, the patient was re-evaluated by a multidisciplinary team of providers at Naval Medical Center San Diego, including a physical therapist, certified prosthetist/orthotist, orthopedic surgeon, and physical medicine and rehabilitation physician. The IDEO, a PD-AFO, was prescribed and custom manufactured by the certified prosthetist/orthotist (Figure 1(c)). The patient then participated in the Return to Run clinical pathway, 1 completing 14 sessions over 3 months. Reporting of this case was approved by the Institutional Review Board at Naval Medical Center San Diego and written patient consent for use of medical information was obtained.
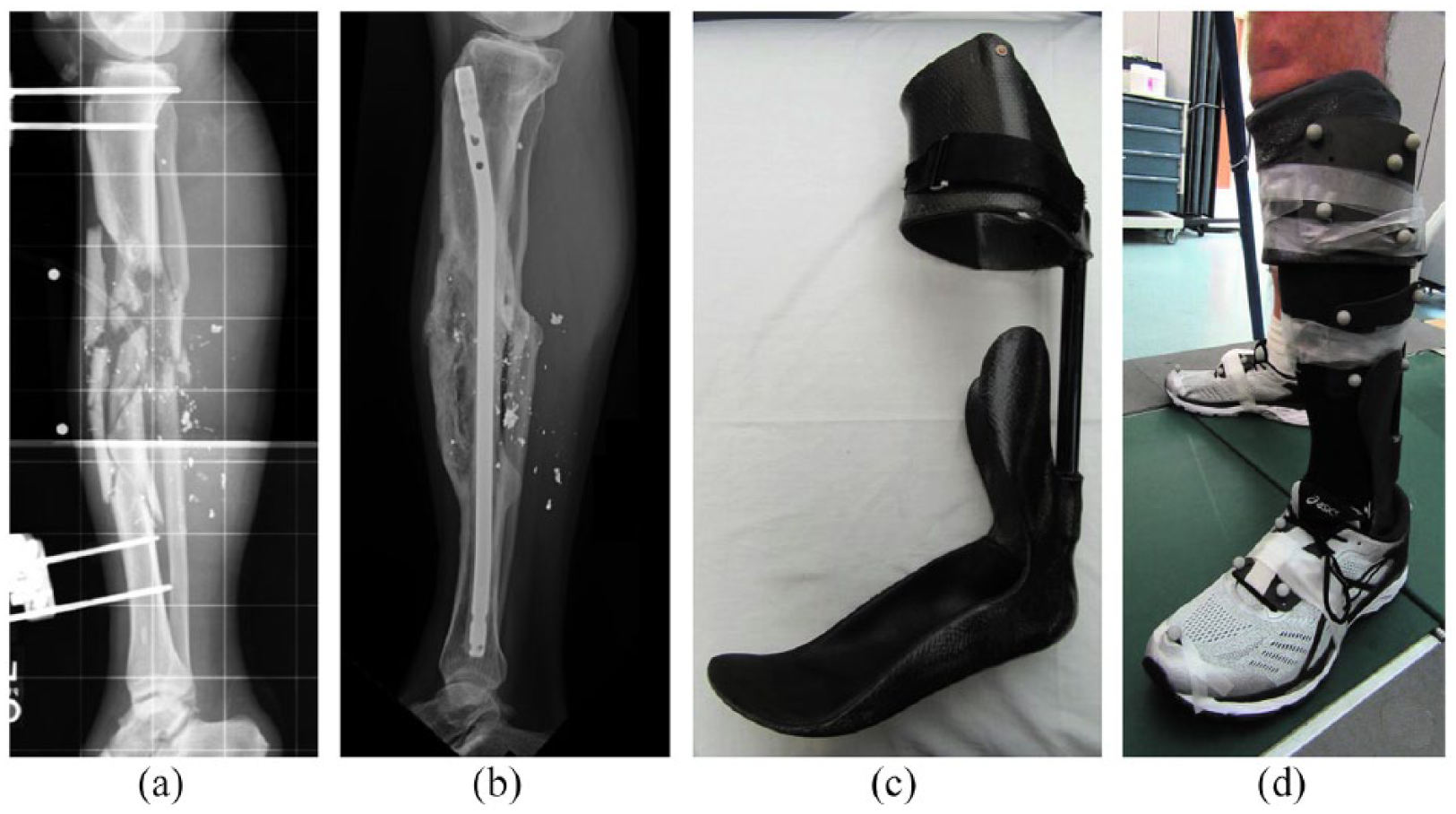
Left tibia/fibula fracture due to gunshot wound (a) prior to and (b) following surgical reconstruction. (c) Intrepid dynamic exoskeleton orthosis (IDEO) custom made at the Naval Medical Center San Diego incorporating two, circular cross-section energy storage and return carbon fiber posterior struts (Medi Clever Bone). (d) Configuration of rigid, cluster motion capture markers on the patient’s limb and IDEO.
Three years after receiving the IDEO, the patient returned for follow-up (height = 182 cm, weight = 89 kg). He reported he had begun to run twice a week for 3–4 miles at a time, but desired to further advance overall running performance and address secondary left knee pain (inferior patella/tibial plateau) that arose with prolonged running. A referral to the Movement Retraining Clinic was issued where a physical exam and treadmill running evaluation revealed bilateral rearfoot initial contact.
Eight sessions of movement training, 5 completed over 18 days were prescribed to transition to bilateral midfoot strike (Table 1). While running on a treadmill at a self-selected speed, the patient viewed real time, graphical feedback on bilateral foot relative to ground inclination angle with green and red coloring differentiating mid- and rearfoot strikes, respectively (Figure 2). 9 To achieve midfoot contact, the patient was verbally cued to create green peaks closely under the threshold without seeing red. To enforce autonomy-supportive learning, 6 no other verbal cues were given, as self-guided problem-solving has been suggested to strengthen motor learning outcomes. Visual feedback was used, as an external attentional focus has been shown to speed the learning process and result in enhanced accuracy and consistency of the learned strategy. 6
Treatment schedule and outcomes across training (S1–8) and evaluation visits at pretraining (PRE), posttraining (POST), one month follow-up (FU1), and five month follow-up (FU5).
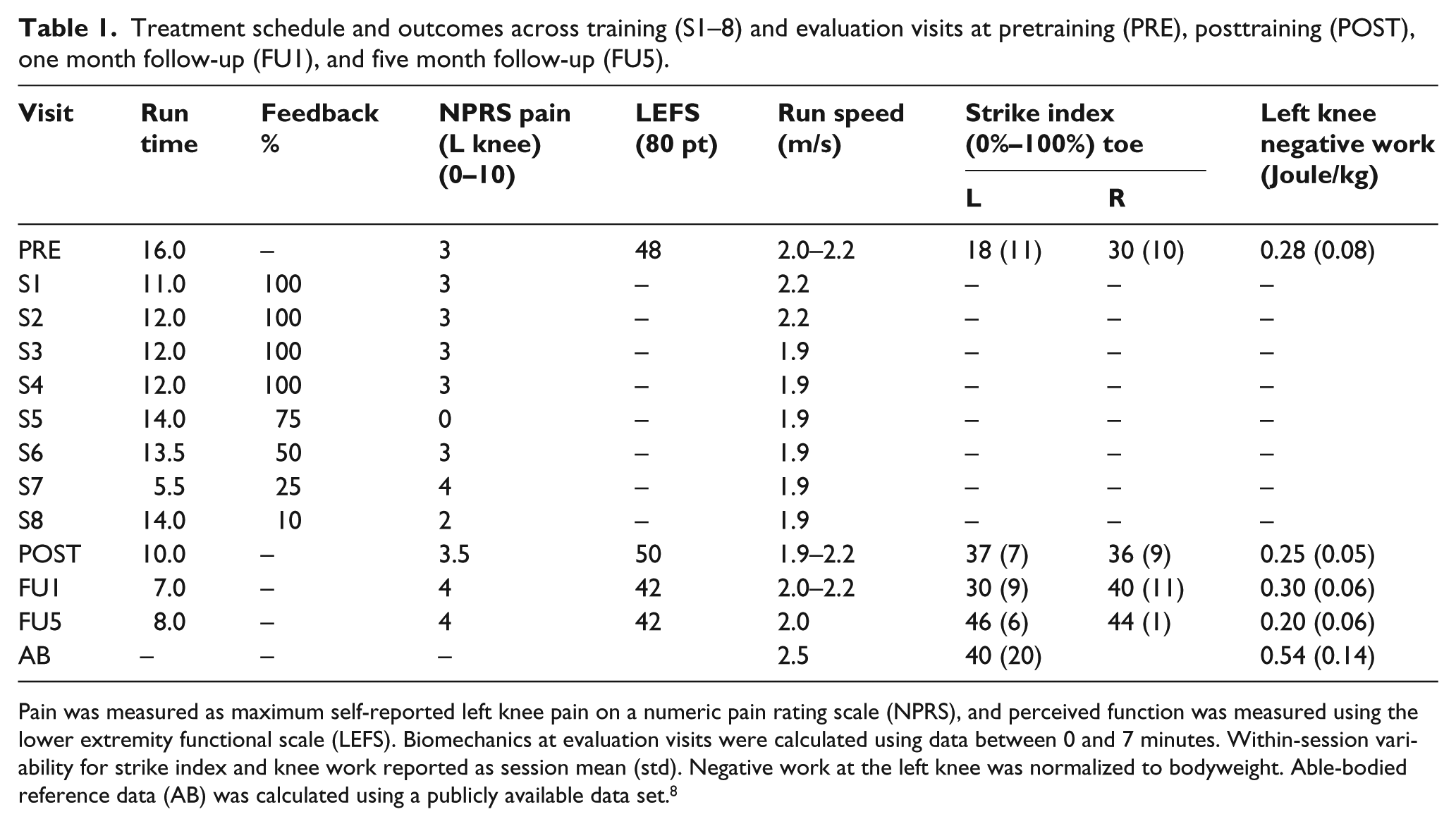
Pain was measured as maximum self-reported left knee pain on a numeric pain rating scale (NPRS), and perceived function was measured using the lower extremity functional scale (LEFS). Biomechanics at evaluation visits were calculated using data between 0 and 7 minutes. Within-session variability for strike index and knee work reported as session mean (std). Negative work at the left knee was normalized to bodyweight. Able-bodied reference data (AB) was calculated using a publicly available data set. 8
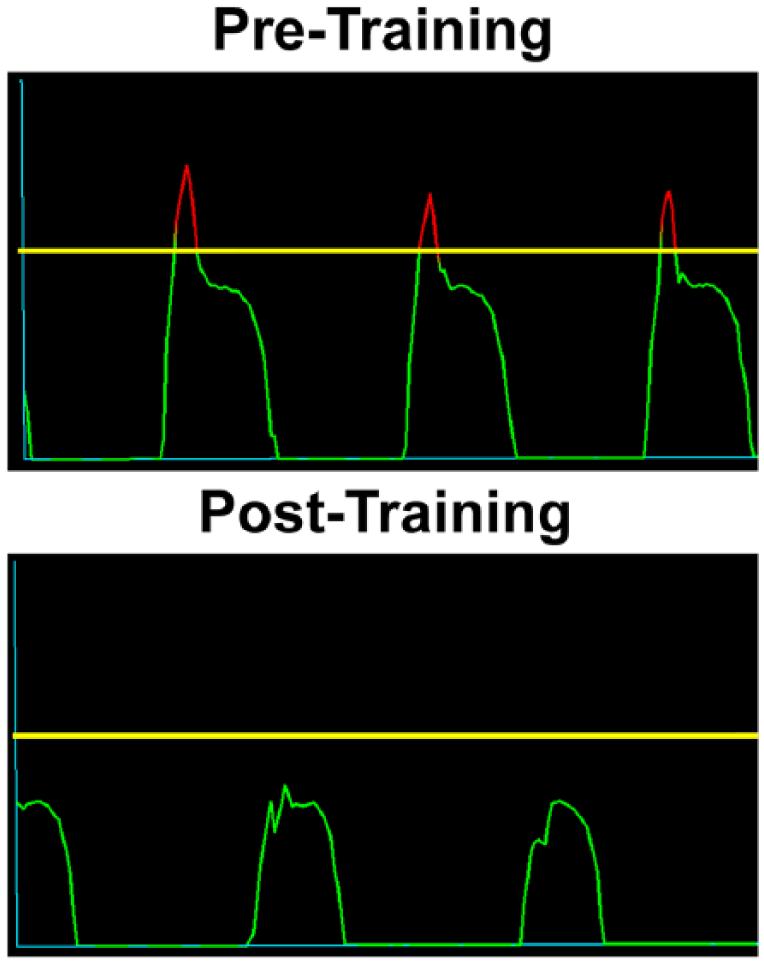
Visual feedback on sagittal foot inclination angle for a single limb displayed to patient on television screen during running PRE (top) and POST (bottom) training. Feedback was displayed bilaterally. A threshold horizontal line (yellow) was set for each foot with patient standing in foot flat, such that peaks above the yellow line (red coloration) signaled increasing rearfoot contact, and below the yellow line (green coloration) signaled increasingly forefoot contact. The patient was instructed to aim for green peaks closely under the threshold, without crossing above into red, thereby achieving contact with foot approximately level to the ground. Graphs displayed the most recent 100 motion frames (~0.8 s) where each peak indicated a separate foot strike (~3–4 strikes).
The patient was given goal run durations, although sessions were ended early if excessive fatigue was observed or a score on the numeric pain rating scale (NPRS, 0–10) increased by two or more points. Across the final four treatment sessions, percentage of total time viewing feedback was gradually decreased in a faded schedule to facilitate internalization of the strategy (75%, 50%, 25%, 10%). 7 Follow-up evaluations with no visual feedback were completed immediately after the final treatment session (POST), and at one and five months following his final training session (FU1, FU5). At all evaluations, perceived function was measured using the lower extremity functional scale (LEFS, 80-point maximum = no limitation). 10 Three-dimensional ground forces were measured via instrumented treadmill (1200 Hz, AMTI, Watertown, MA), and kinematics were measured using a 14-camera, passive optical system (120 Hz, Motion Analysis Corporation, Santa Rosa, CA). A modified six-degree-of-freedom marker set was applied using rigid clusters of four reflective markers affixed to the midfoot, proximal shank, and distal thigh (Figure 1(d)). Foot strike was classified post hoc using a center of pressure-based strike index (SI), where 0%–33%, 33%–67%, and 67%–100% indicate rear-, mid- and forefoot strikes. 9 To account for treadmill inaccuracies at low force magnitudes, SI value was extracted at 10% stance, where initial contact and toeoff were defined using a 25 Newton vertical force threshold. Motion and analog data were lowpass filtered at 15 Hz prior to inverse dynamic calculations.
A mechanical work analysis was used to estimate the combined, energetic performance of the PD-AFO in combination with the patient’s affected limb. The ankle and knee joints were modeled with three rotational and three translational degrees of freedom. 11 The distal foot was modeled as a deformable body, capable of storing/returning energy. 12 Positive/negative instantaneous powers over the stance phase were separately integrated to yield positive/negative mechanical work for the distal foot, ankle, and knee. Positive work estimates the energy added to the body from all collective active and passive structures spanning a joint/segment (i.e. PD-AFO components + muscles + ligaments + cartilage), while negative work estimates energy stored or dissipated. A ratio of total positive over negative work was calculated where 100% indicates net zero energy addition/subtraction. Ratios were calculated for ankle work (WRA), and also for summed ankle plus foot work (WRAF). Ankle kinematics and kinetics were additionally extracted and are provided in Supplementary Material (Table S.1—range of motion, peak angular velocity, peak moment). The patient’s achieved run durations varied across evaluation visits due to low baseline endurance (Table 1). For analytical consistency, only data between 0 and 7 min were used for the biomechanical analysis. All biomechanical metrics were computed per stance phase and then compiled into a session average/standard deviation to measure within-session variability. Able-bodied reference data were generated using a publicly available data set of 28 males running at 2.50 m/s on an instrumented treadmill 8 (age = 34.8 ± 6.7 year, mass = 69.6 ± 7.7 kg).
Findings and Outcomes
The patient successfully completed all eight training sessions (Table 1). Left knee pain measured by NPRS remained consistent across visits, with a maximum of 4/10. Perceived lower limb function measured by LEFS was low at PRE and did not change at POST or at follow-up visits relative to a 9-point threshold for clinically meaningful change 10 (Table 1). Anecdotally at FU5, the patient reported high satisfaction with the program and noted that his recreational running capacity had increased to a maximum of 11 miles at a time.
Results for biomechanical parameters across evaluation visits are presented in Table 1 and Figure 3. Foot strike index for the left PD-AFO changed from rearfoot (18% PRE) to midfoot (37% POST) immediately after training, with retention at long-term follow-up (30% FU1, 46% FU5). Alongside foot strike change, ankle WRA for the PD-AFO limb increased from 91% PRE to 124% POST, with retention at long-term follow-ups (105% FU1, 109% FU5). A substantial decrease in WRA within-session variability was also measured (46% PRE, 7% POST). Combined ankle-foot WRAF increased immediately after training (57% PRE, 76% POST), with retention at long-term follow-up (72% FU1, 73% FU5). In contrast, left knee negative joint work did not notably change between evaluations, but was consistently below able-bodied persons running at a similar speed.
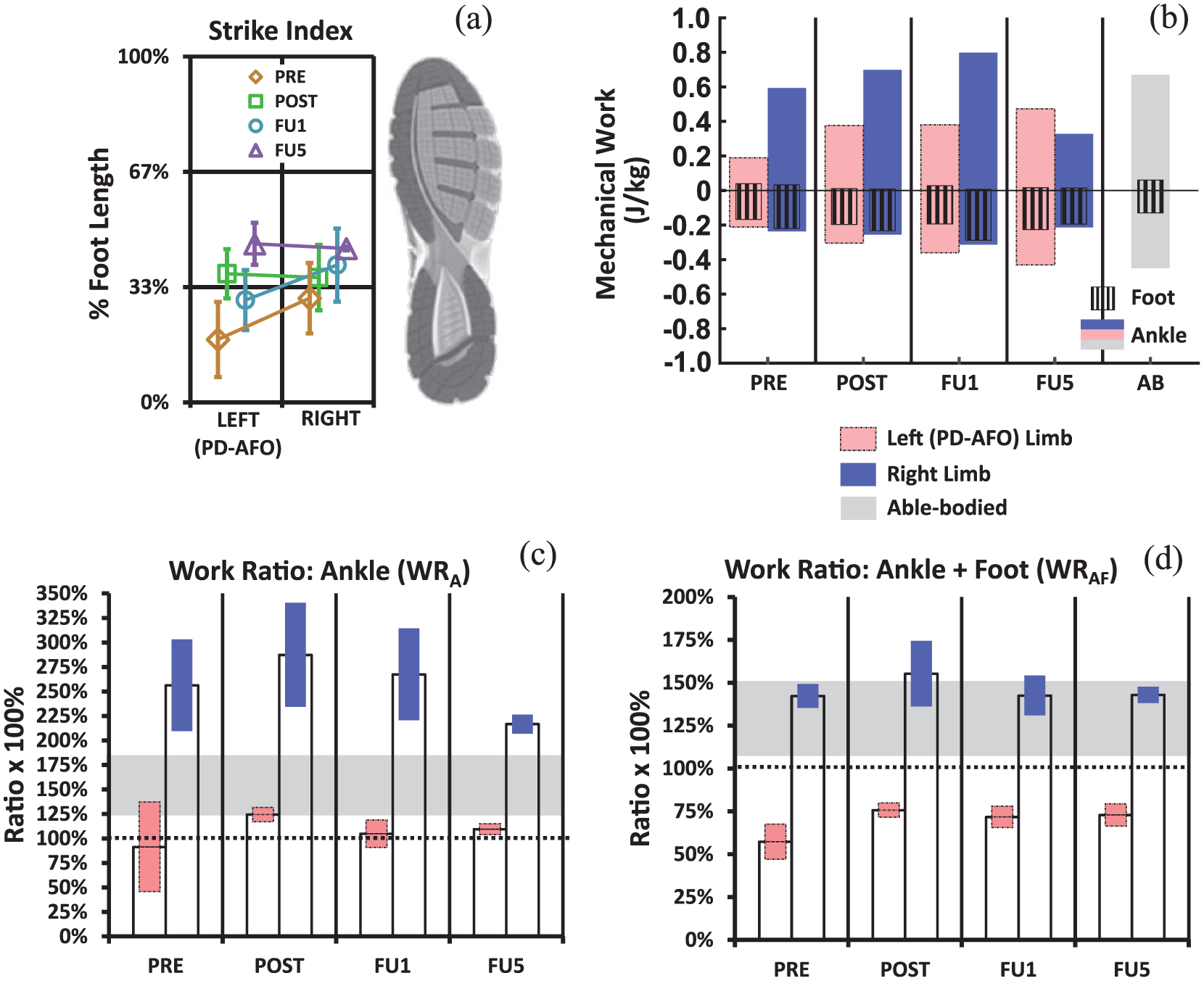
Biomechanical outcomes before and after footstrike training. (a) Strike index at 10% stance measuring rear-mid-forefoot classification. (b) Mechanical work done at the ankle and by the distal foot during stance normalized to bodyweight. (c, d) Ratio of positive to absolute negative work for the ankle and for the combined ankle-foot. The 100% dotted reference line indicates a level at which the same amount of energy was returned and/or generated as was stored and/or dissipated by the combination of anatomic and PD-AFO structures. Bar height indicates session average and colored range indicates magnitude of within-session variability over 7 min (± one standard deviation).
Discussion and Conclusion
The purpose of this case study was to report outcomes for a patient utilizing a PD-AFO due to severe prior limb trauma, following completion of a session-based, midfoot strike run training program. In this preliminary case, the patient successfully transitioned from a rearfoot to midfoot strike on the PD-AFO limb and retained these mechanics up to 5 months following treatment. Energetic performance of the patient’s ankle-foot complex combined with the PD-AFO also improved following training. At PRE, work ratio about the ankle WRA averaged low at 93%—below a 100% reference indicating net energetic loss, and further below the able-bodied range (Figure 3). In addition, within-session variability of WRA over the 7 min of continuous running was large at PRE, highlighting that while the patient achieved a high WRA of 148% at an SI of 33%, he was unable to maintain and WRA fell to 45% at the lowest SI of 7% after 7 minutes (Supplementary Material - Table S.2). Versus mid- to forefoot, a rearfoot strike produces less mechanical leverage about the ankle in early stance necessary to passively load PD-AFO struts (low PRE left ankle moment, Supplementary Material—Table S.1). Theoretically, this may shift late stance propulsive demands to the plantarflexors, leading to variability from neuromuscular sources and fatigue across extended runs. However, a more detailed model and simulation is required to estimate relative contributions from biologic versus passive PD-AFO structures. 13
After treatment, WRA on the PD-AFO limb increased to 124% POST with an SI of 37%, with retention 5 months later at 109% and an SI of 46%, each with greatly reduced within-session variability. The further 16% SI increase on the PD-AFO limb between FU1 and FU5 appeared to correspond with reduced, overcompensation in positive ankle work and WRA on the right, unaffected limb (Figure 3(b) and (c)). These added improvements may represent long-term effects over the course of five months as the patient gradually gained trust of the strategy and the PD-AFO limb. The patient may also have continued to internally optimize how mechanical energy added to the body from the ankle-foot was used at the task level (e.g. for body forward propulsion versus support), which could further lessen demand on the unaffected limb.
The summative ankle-foot work ratio WRAF also showed improvement but at a lower magnitude than WRA, rising from 57% PRE to 76% POST and retained at 73% at FU5. In contrast to WRA, within session variability of WRAF was minimal at PRE. Closer inspection of work composing WRAF revealed that an SI range from 7% to 33% during PRE corresponded with a low and high WRA of 43% and 147%, but yielded a relatively stable WRAF when combined with high and low distal foot WR of 69% and 4% (Supplementary Material—Table S.2). Regardless, WRAF magnitude was 15%–19% greater in all follow-up evaluations, highlighting that increasingly leveraging the ankle complex (ankle anatomy + PD-AFO strut) via a midfoot strike was more mechanically effective than relying partly on distal structures (foot anatomy + PD-AFO footplate + shoe). Damping components (shoe rubber, foam heel lift), shoe-ground friction, and multiplanar buckling of the footplate could contribute to lesser mechanical efficiencyof the distal complex.
The patient’s running associated knee pain was unchanged by midfoot strike training. Left knee negative work at PRE measured well below comparable able-bodied magnitudes, and did not decrease further with midfoot strike transition as reported for able-bodied runners. 3 This may indicate the patient had already employed a knee avoidance strategy to minimize mechanical demands about the left knee as a means to decrease movement associated pain. Orthotic adjustment of the PD-AFO proximal cuff to change how external loads transfer from the ground on to the tibia may also have been a useful supplemental intervention for knee pain given the patient’s specific reconstruction (Figure 1(b)).
Finally, before treatment, the patient scored a low 48 out of 80 on the LEFS indicating significant self-perceived impairment due to lower limb function, and no change was measured after foot strike training. Inspection showed the lowest rated questionnaire items were consistently “standing for one hour,” “running on uneven ground,” and “making sharp turns while running fast.” Augmented training to address these specific subtasks may be useful for future, similar patients.
Conclusion
In conclusion, midfoot strike training appreciably improved energetic performance of the patient’s ankle-foot complex aided by the PD-AFO. Self-reported knee pain and overall lower limb function were not changed, although recreational running frequency did increase substantially. This feasibility study demonstrates that movement training programs designed for able-bodied, experienced runners can be adapted to a clinical, orthotic, and limb trauma rehabilitation environment. Expanded work is needed to assess efficacy across a larger sample of PD-AFO users and injury types.
Supplemental Material
SupplementaryMaterial_v2 – Supplemental material for Biomechanical improvements following foot strike biofeedback training for a patient using a passive dynamic ankle-foot orthosis during running
Supplemental material, SupplementaryMaterial_v2 for Biomechanical improvements following foot strike biofeedback training for a patient using a passive dynamic ankle-foot orthosis during running by Adam J Yoder, Brittney N Mazzone, Richard S Miltenberger and Shawn Farrokhi in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors thank Anahid Ebrahimi for contributing to the code used in analysis. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government.
Author contributions
AY and BM collected experimental data. RM administered orthotic services. AY analyzed the data and wrote the manuscript. All authors provided revisions and approval of final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided in part by resources of the DoD-VA Extremity Trauma and Amputation Center of Excellence.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.