
Abstract
Background:
Immobilization, using a shoulder abduction brace, may be important after rotator cuff repair to achieve successful tendon-to-bone healing. Compliance with wear time is a concern.
Objectives:
Therefore, the abduction brace wearing time was assessed with temperature-sensitive sensors to objectively measure the abduction brace wearing compliance rate.
Study design:
Level of evidence I, prospective observational study.
Methods:
A temperature sensor was implanted into 54 standard shoulder abduction braces, worn by 50 patients (27 women; mean age, 56 years). At 6 weeks post-surgery, patients reported the number of hours they had worn the brace. The patient-reported and sensor data were compared, and the compliance rate (relative to the recommended wearing time) was determined, with compliance being the primary end-point and the discrepancy between the measured and patient-reported wear time being the secondary end-point.
Results:
Compliance was ⩾80% in 24 (48%) patients. Sensor-based compliance was lower than self-reported compliance (75% versus 96%, p ⩽ 0.001). Compliance was not predicted by age, sex, smoking, educational, employment, living status, or handedness.
Conclusions:
Roughly 50% of patients did not wear the brace at least 80% of the recommended time. Self-reported compliance is significantly lower than sensor-based compliance. Compliance was not predicted by measured demographic variables.
Clinical relevance
This is the first study in which the abduction brace adherence of patients after rotator cuff repair was assessed by the use of a temperature-sensitive sensor. The postoperative use of these braces is questionable as the patient’s abduction brace adherence is low. The self-reported wearing compliance is unreliable.
Background
Absence of healing and/or re-tearing after open or arthroscopic rotator cuff tendon repair occurs in more than 20%1,2 of the patients and presents a major challenge in shoulder surgery. In addition to technological and surgical improvements, 3 different postoperative rehabilitation protocols have been studied to increase the rate of tendon healing and improve clinical outcome. 4 Different shoulder immobilization tools are used for various amounts of time following a reconstructive procedure.4–6 Abduction braces are commonly used supports, which cause passive glenohumeral abduction and are thought to decrease the tension of the repaired posterosuperior rotator cuff in the early postoperative period.4,7,8 The positive effect of a postoperative shoulder immobilization has been questioned and could not be proven in a number of controlled trials.9–12 None of these studies, however, objectively assessed the wearing compliance of immobilization devices but used self-reported wearing compliance so that the true effect of immobilization devices on tendon healing cannot be concluded reliably. Silverio and Cheung 13 assessed the abduction brace wearing compliance of patients after rotator cuff repair and could not find any correlation between self-reported wearing compliance and functional outcomes. From other orthopedic subspecialties as spine or foot and ankle surgery, it is known that patient’s wearing compliance is low.14–18 Alternatively to patient’s self-declaration of wearing behavior, objective compliance assessment using thermo-sensitive sensors measuring body temperature can be used.14,16,17 The purpose of this study was to objectively analyze the abduction brace wearing behavior by the use of such a sensor in patients who underwent arthroscopic rotator cuff surgery.
Methods
Our single-center, single-blind, prospective prognosis study was approved by the local ethical committee of Zurich, Switzerland (Cantonal Ethical Commission number 2016-01089) and registered at clinicaltrials.gov (NCT03054753).
Consecutive series of patients with a primary full thickness, superior rotator cuff tendon tear who were scheduled for arthroscopic rotator cuff repair (ARCR) with postoperative immobilization in an abduction shoulder brace (ASB), were prospectively invited for the study. Patients presenting with a repeat tear were excluded.
All patients who signed both parts of the study consent form were included into the study. The first part of the consent form informed the patients before the ARCR about the intention of a compliance study without mentioning the use of an electronic sensor. A sensor (Orthotimer®, Rollerwerk Medical Engineering, Balingen, Germany; Figure 1) was placed without information and invisibly for the patient prior to the surgery so that the individual wearing behavior was not influenced by the patients’ cognition. At the routine 6-week follow-up visit, the patients first self-reported their wearing compliance, were then informed about the use of the hidden sensor, and, if they agreed, then signed the second consent form. Exclusion criteria are that patients with re-tears of the rotator cuff were excluded from the study before the re-reconstruction was performed and no sensor was implanted. Patients in whom no ASB was administered postoperatively and patients who denied participating in the study were also excluded from the study.

A green colored temperature sensitive Orthotimer® sensor. The correlation of size is demonstrated with the 1 Cent € coin.
Intervention
The rotator cuff tear was confirmed by an MR arthrogram in all patients. If clinically indicated, the ARCR was programmed. Preoperatively, the optimal size and position of the ASB was determined by an experienced orthopedic technician. The temperature sensor was invisibly placed into the foam of the abdominal belt of the ASB without the patient’s knowledge. The procedure was performed in regional anesthesia in the beach chair position using a usual arthroscopic suture anchor reconstruction technique. Immediately postoperatively the sensor-loaded abduction shoulder brace (Type Comfort, Pompa AG, 5212 Hausen/Brugg, Switzerland) (Figure 2) was fitted in the patient’s axillary pit. This allowed for close contact with the patient’s lateral waist detecting the patient’s body temperature (Figure 3). The temperature detected from the ASB belt well corresponded to the core body temperature measured with a clinical thermometer in the axilla or in the ear. Several temperature tests were performed in a pilot study in three different test persons at different interphase locations to define the best sensor placement for reliable measurement of the body core temperature. The sensor monitors the surrounding temperature in a 15-min interval. Similar sensors have been used to investigate wearing compliance of corsets in scoliosis therapy 17 and wearing behavior of compressive stockings after hind foot surgery. 16 If the measured temperature exceeded the threshold value of 35° Celsius, the sensor registered the measurement episode as “brace wearing time.” The asked ASB wearing time was 23 h/day 6 weeks postoperatively, which equals a mean of 966 h. For body hygiene, patients were allowed to remove the monitoring ASB and wear a shower compatible abduction splint in which no sensor was implanted. This is why the asked wearing time was 23 instead of 24 h/day. At the routine 6 weeks postoperative outpatient visit, all patients were asked to retrospectively report their average wearing compliance per day in percent from 0% to 100%. The read out of the sensor was only performed if the patient signed the second part of the study agreement. In case of denial, the sensor was deleted.

Test person with abduction shoulder brace “Comfort” (Pompa AG, Hausen/Brugg, Switzerland). The area of implantation is highlighted with the red circle.

Sensor implantation site on the abduction brace.
The read out of the sensors was performed with the Orthotimer computer software (Rollerwerk Medical Engineering, Balingen, Germany), which indicated the total wearing time of each day since the sensor was activated (= day of surgery). The total objective wearing time over the 6-week period was cumulated. This cumulated time was then divided by the cumulated recommended wearing time of ±966 h (23 h × ±42 days). The resulting quotient was defined as the compliance rate in percentage. Compliance rates were categorized in two groups: (1) high compliance rate group with patients with a wearing compliance rate of ⩾80% and (2) low compliance rate group with <80% of the asked wearing time. In addition, the patients’ compliance rate profiles were subcategorized into quintiles (quintile 1 = compliance rate of 0%–19%, quintile 2 = 20%–39%, quintile 3 = 40%–59%, quintile 4 = 60%–79%, quintile 5 = 80%–100%). The compliance profiles of non-compliant patients (<80%) were further analyzed to detect if non-compliance occurred at the beginning, at the end of the 6-week period, or continuously during a certain time of the day.
Apart from objectively measured and self-declared wearing times, parameters including age, gender, smoking, handedness, employment status, and educational and living status (living with family/alone) were assessed.
Outcome measures
The primary endpoint of the study was the proportion of patients in the high- and low compliance groups. The second endpoint was the difference between the self-reported and sensor-based compliance rate. The correlation between demographic variables and sensor-based compliance rate was calculated.
Statistics
The Shapiro-Wilk test was used to test the data for normal distribution. Differences in the wear rate between the high- and low compliance groups were evaluated using the Mann–Whitney U test. The correlation between demographic variables and sensor-based compliance rate was evaluated using a univariate linear regression model. Differences in demographic variables between the high- and low compliance groups were evaluated using the Mann–Whitney U Test. Significance was set as p < 0.05 and all p values were two-tailed. Analyses were performed using IBM SPSS Statistics for Windows (Version 22.0; IBM Corporation, Armonk, NY, USA) and power analysis was performed using Stata (StataCorp LLC, College Station, TX, USA).
Results
A post hoc power analysis based on the observed compliance rate of 48% and the expected compliance rate of 67% based on previous data revealed that a total of 50 patients were sufficient to provide an acceptable power of 78%. 16
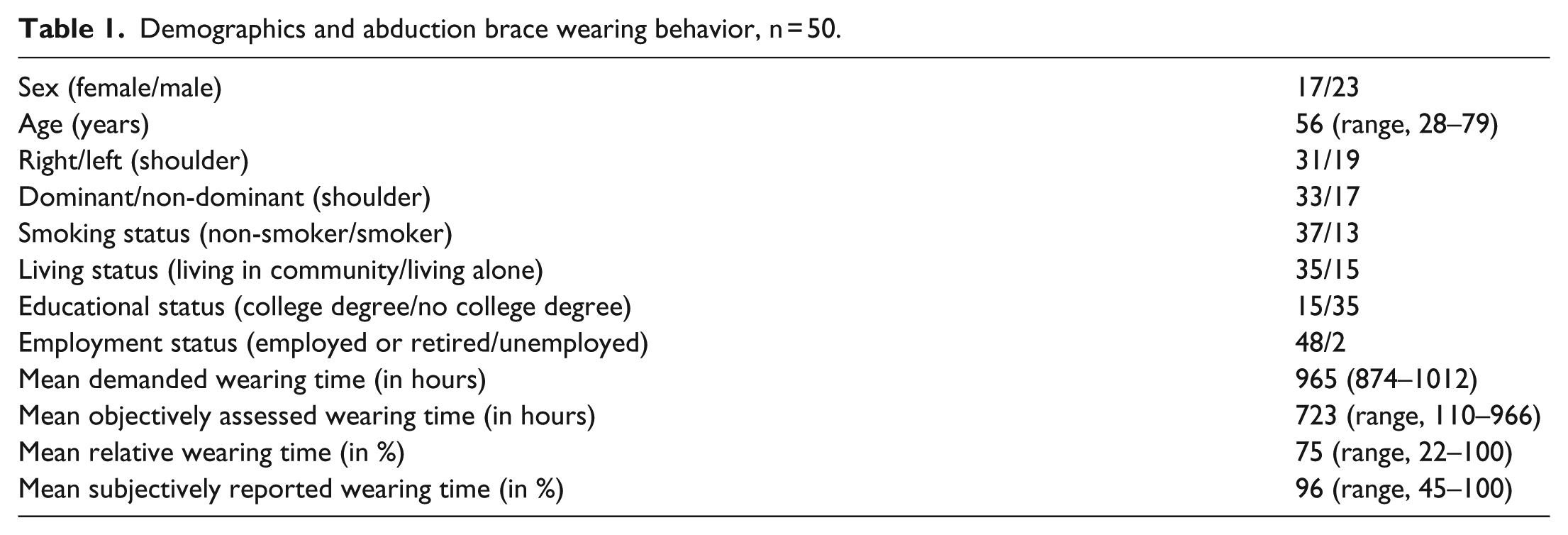
Of the 54 initial patients, 4 (7%) had to be excluded: 2 patients denied the read-out of the sensor, 1 patient carried only the water-proof ASB without sensor, and in 1 patient the sensor was lost before read out. The ASB compliance was therefore analyzed in 50 patients including 17 women and 33 men (34%/66%) with a mean age of 56 years (range 28–79) who had signed both parts of the consent form. From the 31 right and 19 left shoulders (62%/38%), 33 were dominant and 17 non dominant shoulders (66%/34%). In all, 37 patients were non-smokers and 13 were smokers (74%/26%). 35 patients declared to live with family members or in a living community, and 15 patients lived on their own (70%/30%). A total of 47 patients were employed and 3 patients were unemployed (94%/6%) during the time of observation. While 15 patients declared to have a degree from university, 35 had no university degree (30%/70%). Six different shoulder surgeons performed the index surgery.
Twenty four (48%) patients wore the abduction brace ⩾80% (mean objective compliance rate of 92%) (Figure 4) and 26 (52%) patients wore the abduction brace <80% (mean objective compliance rate of 55%) of the asked total wearing time (Figure 5). A total of 12 (24% patients of the high compliance (⩾80%) groups showed a compliance rate of 100%. In the low compliance group, 13 patients had a compliance rate between 60% and 79% (= quintile 4), 8 patients between 40% and 59% (quintile 3), 4 patients between 20% and 39% (= quintile 2), and 1 patient showed a compliance rate of <20% of the recommended wearing time (quintile 19) (Figure 6).
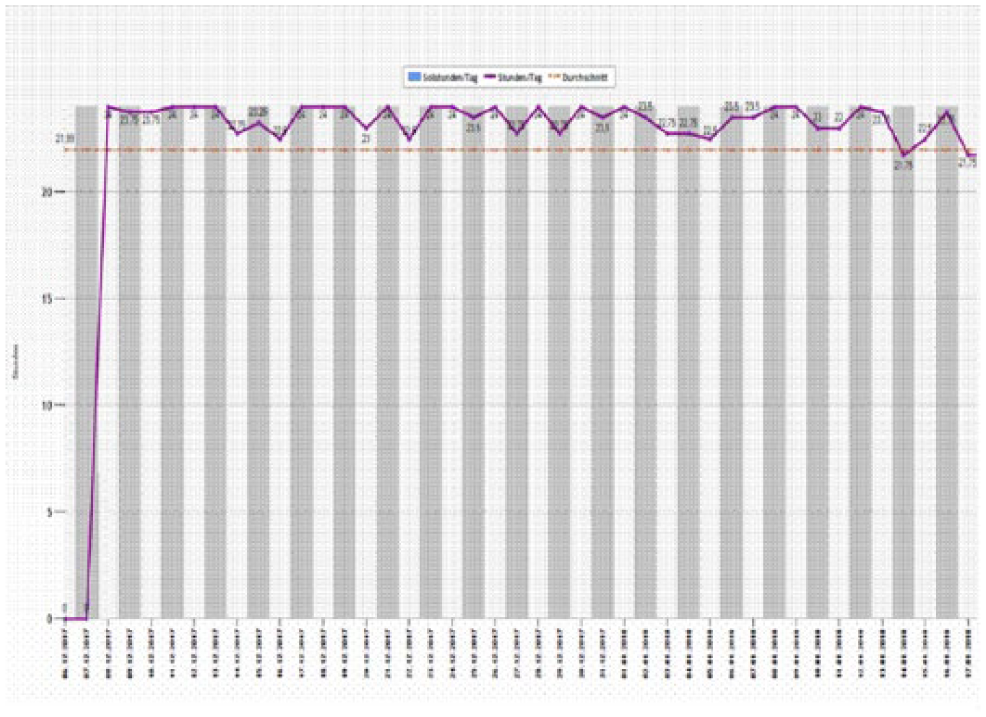
Computer read out of a high compliant patient with ⩾80% compliance rate.
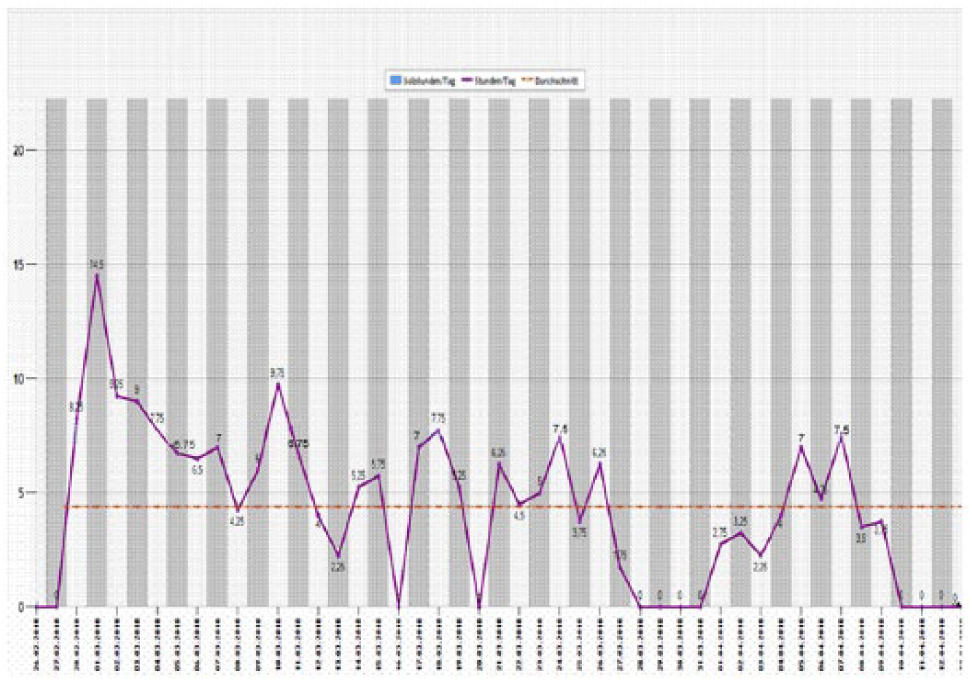
Computer read out of a low compliant patient with <80% compliance rate and a low compliance profile in the second half of the declared wearing time.
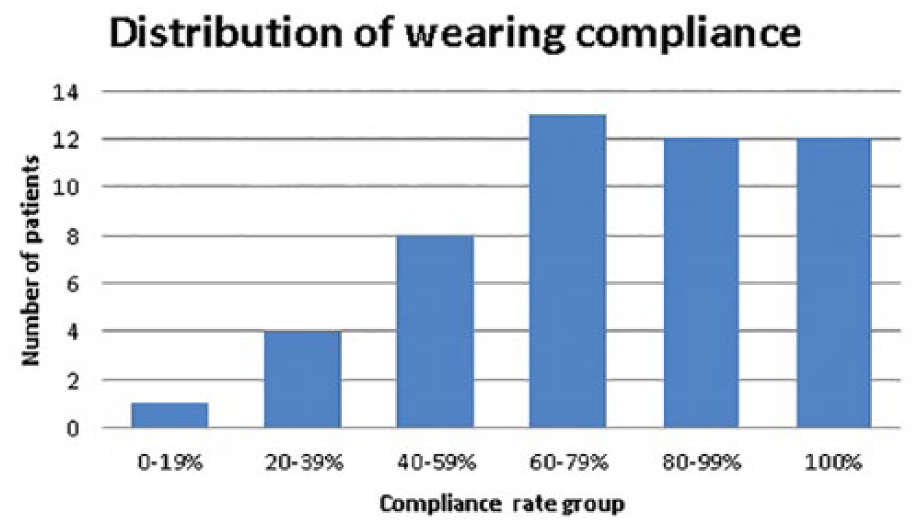
Diagram showing dispersion of patient compliance.
The mean absolute objective wearing time of all patients was 723 h (range, 110–966), and the mean recommended wearing time was 965 h (874–1012), resulting in a mean objective compliance rate of 75% (range, 55%–100%). The patient’s self-declared mean wearing time was 96% (range, 45%–100%), leading to a discrepancy of 21% between patient’s self-declared and objectively measured compliance values of all patients (p < .001)—see also Table 1.
Demographics and abduction brace wearing behavior, n = 50.
The mean measured compliance rate of the low compliant patients group was 55% (range, 11%–78%). The self-reported mean compliance rate of the same group was 93% (range, 50%–100%). The mean discrepancy between self-reported and measured compliance rates was 38% (range, 5%–78%) in the low compliant group.
The mean measured compliance rate of the high compliant group was 93% (range, 80%–100%). The mean self-reported compliance rate was 98% (range, 80%–100%), resulting in a mean discrepancy rate of 5% (range, 0%–20%) was significantly smaller than in the low compliance group (p < 0.001).
Among the non-compliant patients, 17 (34%) patients showed a constant, low-compliance profile with an average wearing time of 11 h/day (range, 5–17) instead of the recommended 23 h/day. Seven patients (14%) wore the ASB during the first 3 weeks with high compliance (⩾23 h/day) and changed their behavior to a low compliance pattern for the second half of the recommended wearing period like seen in Figure 5.
Two patients wore the ASB for the first two weeks only and then autonomously abandoned the ASB. No correlation between demographic variables and compliance rates was visible (Figure 7).
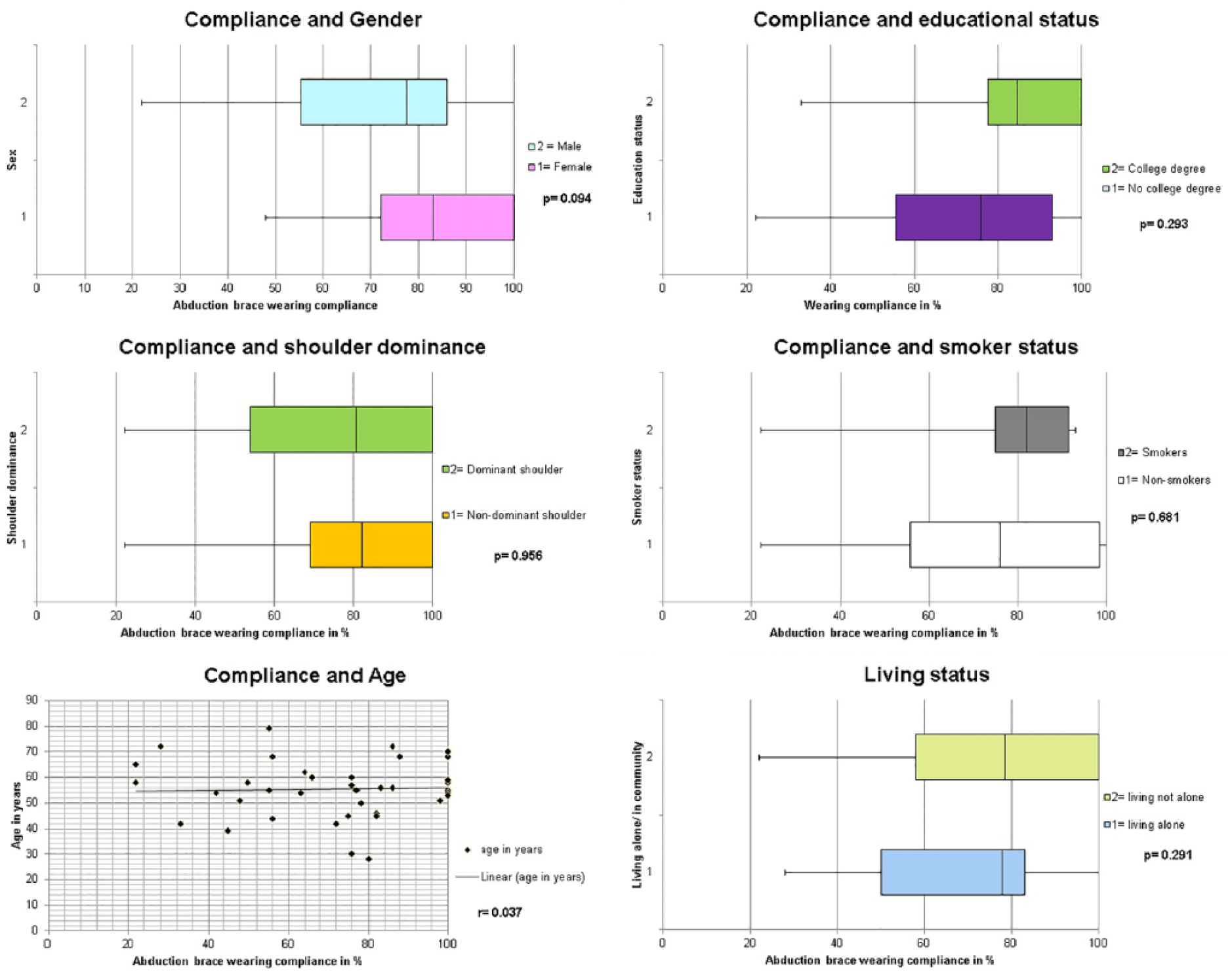
Box plots representing compliance rates depending on sex, educational status, shoulder dominance = handedness, smoker status, and living status. Compliance in correlation with age is demonstrated.
Discussion
The potential benefit of postoperative shoulder protection with an abduction shoulder brace is extensively discussed. Yet we do not even know whether people wear them or not. This means that the true effect of brace protection is currently hypothetical, and the patient cannot be adequately informed about the potential benefits of wearing such a brace postoperatively. It was the aim of this study to objectively analyze ASB wearing compliance of patients after rotator cuff reconstruction.
Overall, the total wearing time was 75% of the desired and recommended wearing time. In contrast, the total self-reported wearing time was 96% (p < 0.001). The main finding of this study is the fact that only 48% of the patients showed a high rate (⩾80%) and 52% of the patients a low (<80%) compliance rate.
A total of 93% of the low compliance group reported to have worn the ASB as recommended. The high compliance group reported a mean wearing time of 98%. The overestimation of the self-reported wearing time was significantly higher in the low compliance group than in the high compliance group and corresponds to the observations from other studies which showed that compliance assessment by questionnaires is not reliable.14,15,17-19
Therefore, the use of a small, invisible temperature-sensitive sensor can be helpful to improve wearing compliance.17,19 A non-blinded implantation of a sensor might be helpful to improve wearing behavior in the future. 17
In the analysis of risk factors for incompliance with abduction brace wearing, no significant differences were detectable between men versus women, smokers versus non-smokers, dominant versus non-dominant shoulders, patients with university degree versus patients without university degrees, or patients living with family or in community compared with patients living on their own. Furthermore, the correlation between age and wearing compliance was very low.
One limitation of the study was the assessment of subjective wearing behavior by asking the patients during the outpatient visit to estimate the subjective wearing compliance rate in percentage. The use of a questionnaire would have provided a more anonymous situation for the patients and it is possible that they may have answered more precisely than in a conversation with the treating surgeon.20,21 Nonetheless, it was felt that too much attention to the wearing time would potentially influence natural wearing compliance.
Another limitation of the study was the definition of high (⩾80%) and low (<80%) wearing compliance. The definition was arbitrarily set by the authors and may not be the ideal value. Future analysis of the results of the repairs with regard to wearing times may allow us to identify a minimal optimal value. Currently, even the World Health Organization holds that there is no general gold bench mark of compliance rates which can separate noncompliant from compliant therapy behavior. 22 Unfortunately, the software program’s ability allowed only the read out of the total amount of worn hours per day, but it does not display at which time of the day the brace was worn or not, which might be helpful to distinguish at which time of the day or night the patients showed low or high compliance. One other limitation of the study is the fact that the patients were not asked regarding ASB wearing satisfaction, which might be an interesting factor. On the other hand, it is expectable that wearing any kind of a shoulder brace during night is not comfortable and it would be very likely that the majority of patients experienced the wearing of the ASB as uncomfortable.
In addition, it is obviously very unclear how individual patients use their arm in the non-compliant time.
Conclusion
One out of four patients who are instructed to wear an abduction brace after arthroscopic rotator cuff repair do wear the brace at least 23 h/day. About half of the patients comply with ⩾80% and half with ⩽80% recommended wearing time over a postoperative period of 6 weeks. The discrepancy between self-reported and objectively assessed wearing behavior was significant. Overall, patients overestimated their wearing time by 21% (p < 0.001). The difference of overestimation is significantly higher in noncompliant patients compared to compliant patients (38% versus 5%, p < 0.001)—compliant patients by 5% and noncompliant patients by 38% (p < 0.001). No significant differences in wearing behavior were identifiable regarding age, sex, handedness, educational status, smoker, and living status. The influence of wearing behavior on clinical and structural outcome will be analyzed in a further study.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Cantonal Ethical Commission number 2016-01089, Zurich, Switzerland.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.