
Abstract
Background:
Using mechanical orthoses have some limitations for walking in paraplegic patients. The development of powered orthoses could potentially overcome some of the limitations of those currently available.
Objectives:
The aim of this review was to compare the evidence of the effect of powered gait orthoses (PGOs) when compared to reciprocating gait orthoses (RGOs) and also hip guidance orthoses (HGOs) in improving gait parameters and the energy efficiency of walking by spinal cord injury (SCI) patients.
Study Design:
Literature review.
Methods:
Using the PRISMA method, and based on selected keywords and their composition, a search was performed in PubMed, Science Direct, and ISI Web of Knowledge databases. Eight articles were selected for final evaluation.
Results:
The results of the analysis demonstrated that there is lack of evidence to show that currently-developed powered orthoses improve the walking parameters of SCI patients when compared to RGOs and HGOs.
Conclusions:
The changes offered by PGOs are not substantial enough for such orthoses to be currently considered preferable by SCI subjects for ambulatory purposes.
Clinical relevance
The development of powered orthoses is still in its infancy and progress needs to be made to improve their functionality and performance envelopes.
Background
An inability to walk, the most important outcome after spinal cord injury (SCI), has been associated with risks of osteoporosis, cardiovascular disease, pressure ulcers, circulatory problems, muscular spasticity and contractures.1-5 Consequently, the ability to stand and walk using an orthosis has been stated as an important goal for SCI patients to achieve. 6
Various assistive devices, including orthoses, have been introduced to aid in improving the walking parameters of SCI patients. Orthoses currently used to aid walking include hip-knee ankle-foot orthoses (HKAFOs), the Walkabout orthosis (WO), hip guidance orthoses (HGOs) such as the Parawalker, and examples of reciprocating gait orthoses (RGOs) such as the isocentric reciprocating gait orthosis (IRGO) and the advanced reciprocating gait orthosis (ARGO).7-13 Studies have demonstrated that the gait parameters of SCI patients may be improved with these types of orthoses compared to when walking with conventional devices such as bilateral knee ankle foot orthoses (KAFOs), but factors such as low levels of energy efficiency and the lack of cosmesis has still limited patient use.5,14-18
The adverse energy costs associated with ambulating with these devices is a major impediment to long-term use.14,19 One alternative treatment option could be the use of functional electrical stimulation (FES) in conjunction with RGOs, but energy expenditure has been shown to remain high with associated rapid onset of muscle fatigue when utilizing FES.6,8 Existing options for orthotic intervention are therefore currently inadequate. PGOs could potentially offer a better or alternate solution by the prudent application of power to targeted joints and thereby potentially reducing the energy demand from lower limb muscle groups during ambulation for this patient group.
In order to help alleviate this, powered gait orthoses (PGOs) were initially developed in the 1970s to improve the energy efficiency of walking by SCI subjects and also to improve their gait when compared to that achieved when walking with non-powered orthotic devices. The aim was to add power to mechanical joints positioned adjacent to the anatomical hips, knees or ankles to produce an increase in the speed and the total distance walked (endurance) as well as an improvement in the energy efficiency of such patients during ambulation. The use of the forces produced by actuators was hypothesized to be an effective way to overcome the problem of the considerable effort required to ambulate in reciprocal walking orthoses. 20
PGOs described in the literature have typically utilized pneumatic muscle actuators (pMAs), hydraulic actuators or direct current (DC) electric motors to apply power to specific joints in their designs. However, the addition of power units can lead to additional weight of the orthosis as well as reduced cosmesis. 21 The weight differential between powered and equivalent non-powered orthoses has not been accurately quoted in previous studies; nor does the literature offer conclusive evidence as to the percentage increase in metabolic cost which may be expected in line with the added weight of adding power to an RGO for SCI subjects. Ohta utilized a knee and hip direct current (DC) powered mechanism which weighed 2.2 kg. 20 One recent development (Arazpour 22 ), has quoted the additional weight added by providing DC power to orthotic hip joints in an IRGO as being 2.8 kg (a 66% increase); however, how this would translate into the potential increase in metabolic energy expenditure is unknown. A reduction in the metabolic energy expenditure while ambulating and reduction of the power requirement of the actuators used in PGOs has been stated to be advantageous for subjects with SCI. 23
Studies which have measured energy efficiency of walking, have cited various outcome measures such as energy expenditure, the physiological cost of walking (PCI), the O2 cost of walking, or energy consumption when comparing different orthotic interventions. Gait parameters analyzed have typically included speed, cadence and stride length (which are all intimately related). However, the effects of PGOs on these parameters were not clear when compared to RGOs and HGOs, and therefore needs further clarification. The aim of this review was therefore to assess the evidence of PGOs compared to RGOs and other more conventional orthoses in improving specific gait parameters when worn by SCI patients.
Methods
Inclusion and exclusion criteria
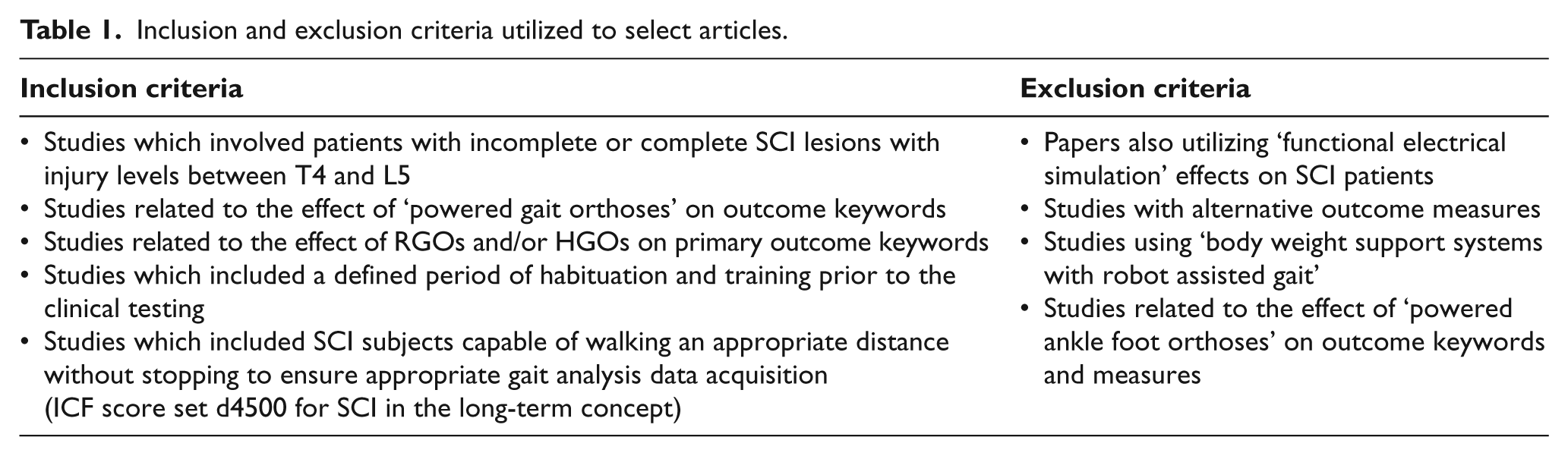
The search was designed to include all studies utilizing HGOs, RGOs, WOs or PGOs, which were either investigated separately or in combination with other devices such as KAFOs in the same study, with the primary goal of investigating their effect on gait parameters and/or energy efficiency when worn by SCI subjects. Studies which involved use of other interventions simultaneously (such as FES) were excluded; as were single case studies and those which compared the primary outcome measures between patients with different disabilities. Those studies which tested orthoses with healthy volunteer subjects (even though the orthoses of interest were utilized in the study) were also excluded. The population of interest was subjects who had sustained a SCI and used one or more of the orthotic devices listed above following a suitable training period.
Only those studies written in English which were published in peer-reviewed journals with full text available were included in the review. Table 1 gives further details of the inclusion and exclusion criteria. The ethics committee of University of Social Welfare and Rehabilitation Science approved this study.
Inclusion and exclusion criteria utilized to select articles.
Search strategy
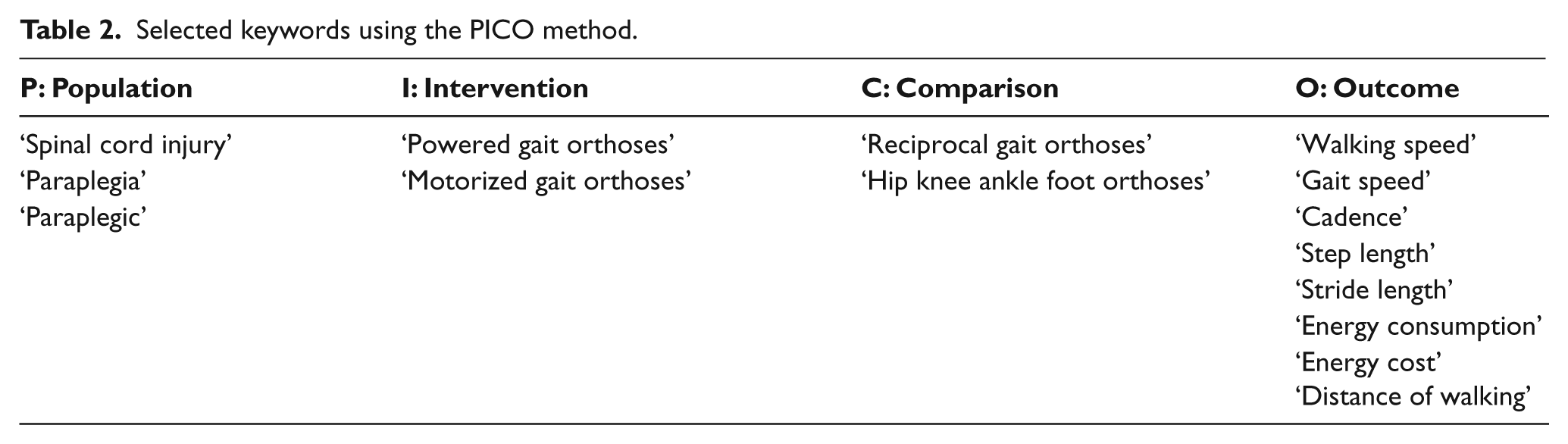
Using the Population Intervention Comparison Outcome (PICO) method, and based on selected keywords and their composition (Table 2), a search was performed in PubMed, Science Direct, ISI Web of Knowledge databases. By using ‘OR’, ‘AND’, ‘NOT’ words as Boolean operators between the selected keywords, relevant articles published in this field were identified. Identified articles were published in English language up to and including the year 2010. The inclusion and exclusion criteria are shown in (Table 1). Finally, eight articles were selected for final evaluation.
Selected keywords using the PICO method.
The procedure was followed using the PRISMA method (see Figure 1).
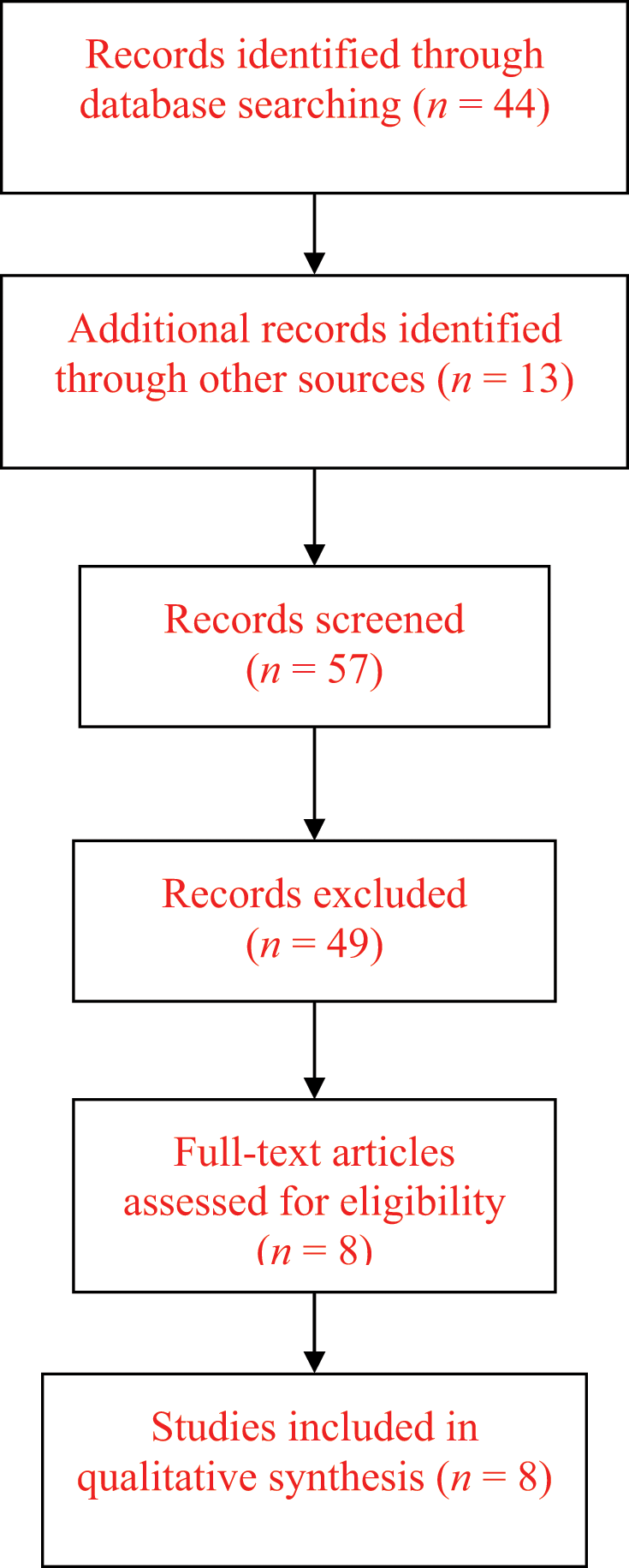
The procedure was followed using the PRISMA method.
Number of references identified, screened, excluded
In total, 57 references which could potentially meet the inclusion criteria were found. The Science Direct search identified 27 articles for further review, and a further 30 additional articles were identified in the other databases (Table 3).Two independent authors then screened each publication to determine whether the inclusion criteria were fully met, and agreed via discussion on the final articles to be selected. Finally, eight articles were selected for final evaluation. Primary outcome measures (keywords) selected for comparison were walking speed, endurance and energy efficiency.
Number of articles selected for potential review according to each database.

Results
The following text summarizes the results demonstrated by studies investigating the comparative effects on parameters demonstrated by SCI subjects walking with non-powered orthotic devices.
Leung 24 in an intra-group study of SCI subjects (n = 6) with complete lesions at levels T12–L1, compared the effects of walking with IRGOs compared to KAFOs on their PCI, walking speed and endurance. With IRGOs rather than bilateral HKAFOs the walking speed increased (10.46 ± 2.00 versus 5.51 ± 4.30 m/min), and the PCI (2.85 ± 0.77 versus 6.77 ± 3.28 beats/m) was more than halved. The averaged total distance walked (endurance) was almost doubled (62.5 m versus 33.16 m) when walking in the IRGO.
In a study of SCI subjects (n = 6) with a wide range of lesion level (complete – T3–T12), Massucci 15 demonstrated that after a six- to eight-week period of walking training with an ARGO, patients achieved a walking speed of between 7.8 and 16 metres per minute with the orthoses. However, the energy cost of walking was eight times higher (1.28 versus 0.16 mlO2/kg/m) after this period of training.
In a randomized cross-over design with a wash-out period, Harvey 25 demonstrated that walking speed in IRGOs was greater than with the Walkabout orthosis in nine SCI patients with complete lesions between levels T9–T12. The average PCI in the WO condition (8.4–10.3 beats/m) was greater than in the IRGO condition (4.3–7.0 beats/m).
In a comparative study between SCI subjects (two with complete and two incomplete between levels T5 and T10), Winchester 26 compared the IRGO to the RGO when measuring walking speed and cadence. Walking speed with the RGO was shown to be 12/7 ± 1/9 and with the IRGO 13/5 ± 2/1 m/s. Cadence with RGOs was 30/3 ± 6/2 and with the IRGOs 31/3 ± 7/9 steps in a minute.
Whittle 27 in a randomized crossover design with no wash-out period, found no differences between walking speed, stride length and cadence in 22 SCI patients with lesion levels between T3 and T12 when walking with either an HGO + Crutch or an RGO + walker. The average speed with the orthoses was 0/24 m/s.
Table 4 shows the outcomes of selected studies which demonstrate the effect of PGOs when compared to RGOs on specific outcome measures.
Main characteristics and methodological scores on studies between PGOs and RGOs.
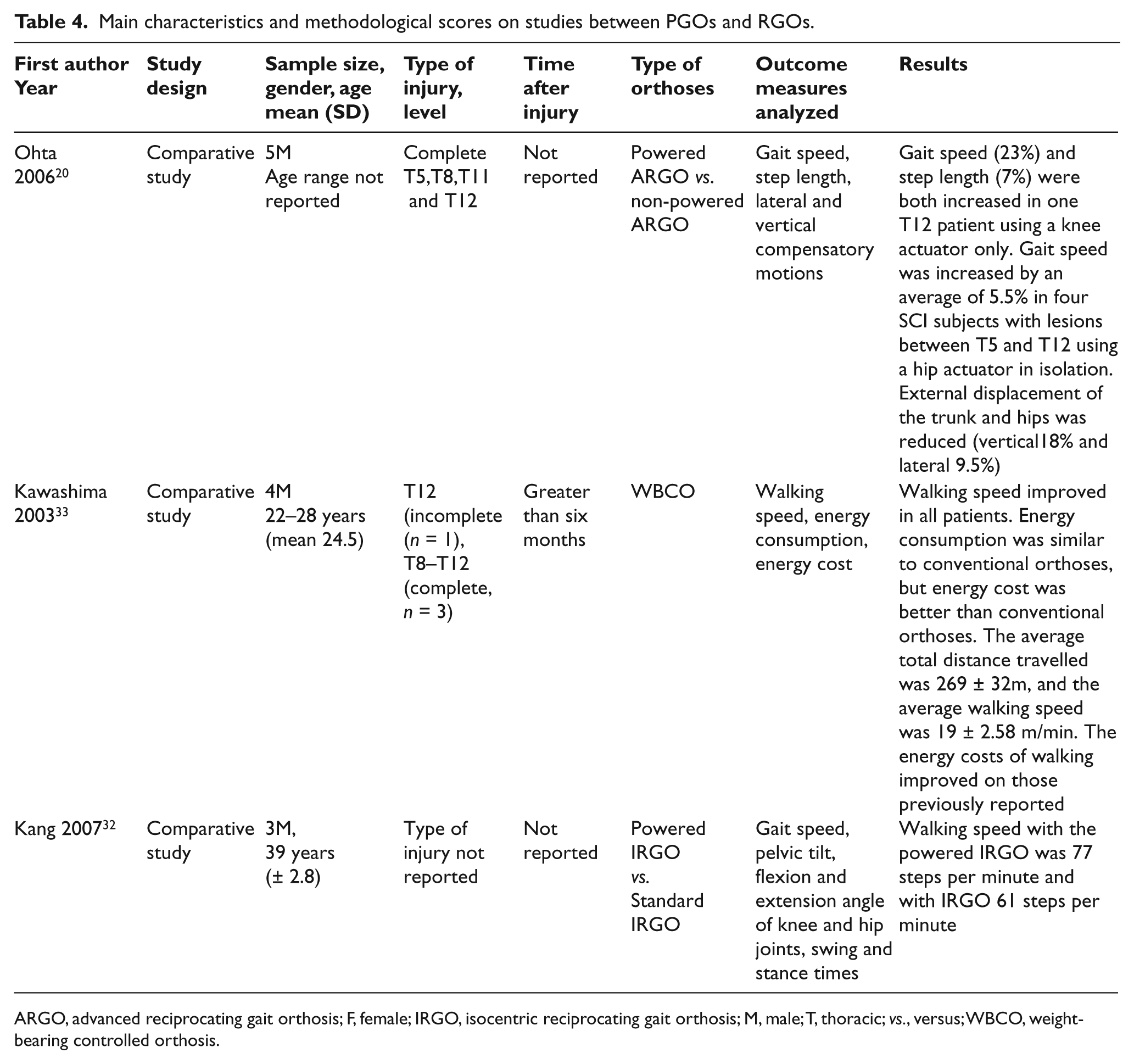
ARGO, advanced reciprocating gait orthosis; F, female; IRGO, isocentric reciprocating gait orthosis; M, male; T, thoracic; vs., versus; WBCO, weight-bearing controlled orthosis.
Effect on walking speed
Reciprocal walking has been shown to be more efficient than when using a swing-through pattern. 28 However, slow walking speeds have been reported with RGOs.21,29-31 The effect of different types of RGO in providing adequate gait speed in SCI patients has demonstrated that it is highest when using the IRGO. However, one study showed no significant difference between an IRGO and an RGO. 25 No significant differences were found when comparing an HGO to an RGO. 26
Cadence
When comparing ARGOs and HGOs, no significant difference in cadence has been reported. 26 However, when comparing an IRGO with an ARGO, it has been demonstrated that cadence was significantly higher when walking in the IRGO. 26 IRGOs have therefore proven to be more effective in increasing cadence than other mechanical non-powered orthoses. A low-friction connection link between the hip joints in this type of orthosis and the effect of this relationship in creating symmetrical movements in both lower extremities may cause this improvement in cadence and, as also stated, an increased walking speed.
Step length
One paper compared this parameter between two orthoses. However, when comparing ARGOs and HGOs, no significant difference in step length between the two orthoses was detected. 27
Energy consumption
The evidence in the literature shows that energy consumption is reported to be less in RGOs than when wearing HKAFOs.14,15,24 In addition, IRGOs use less energy during ambulation than other RGOs25,26; but RGOs, like other mechanical orthoses, cannot be a totally appropriate replacement for wheelchairs in SCI patients. 15
Endurance
Only one paper was found which detailed the maximum walking distance facilitated when SCI subjects walked with an RGO-type orthosis, which quoted the mean walking distance within six minutes as being 75.3±8.4 m. 32
Studies comparing RGOs to PGOs or PGOs in isolation
With regard to gait parameters, only three studies have compared RGOs with electrically or pneumatically actuated PGOs when worn by SCI patients.
In 2003 Kawashima and colleagues evaluated the effects of a ‘weight-bearing controlled orthosis’ on gait velocity, energy consumption and energy cost when worn by four paraplegic patients. These results were compared with results of previous studies with conventional orthoses. 33 In 2007, Ohta et al. evaluated a motorized ARGO with an un-powered version, in terms of walking speed, stride length and lateral sway on five SCI patients. 20 Finally, in 2007, Kang et al. evaluated a powered IRGO via pneumatic actuators with a mechanical IRGO as post test, in terms of walking speed, pelvic tilt, flexion and extension angle of the knee and hip joints and stance and swing phase times on three SCI patients. 32 From the literature review, the three main variables assessed in the articles reviewed were walking speed, energy efficiency, and endurance as measured by total distance walked. However, the evidence of the effect of walking with PGOs on these specific parameters is limited.
Walking speed
Kawashima demonstrated that the average walking speed with the WBCO was 19 m/min in SCI subjects (n = 3), which was faster when compared to a previous study (11.8 m/min), 24 due to the ability to alter the ankle angle during gait.
Ohta and colleagues when using an orthosis with DC motor power to knee actuators demonstrated that a 23% increase in walking speed (from 0.43 to 0.53 m/s) was attainable. 20 This is slower than that achievable in an IRGO. Perhaps, it is possible to have a more efficient externally applied force to orthotic knee joints in mechanical orthoses via a power source, to enable an appreciable increase in gait speed in SCI patients to be achieved, although one study found that activated hip actuators produced slower speeds.
Energy efficiency
With regards to energy consumption, Kawashima and colleagues reported that WBCOs produced no significant change in energy consumption in SCI patients, but the energy cost did decrease to 17/12 (J/kg/m). 27
Endurance
With regards to endurance (one of the most critical parameters enabling SCI patient use), no evidence was found relating to the endurance attainable in PGOs. Stride length and cadence have also been analyzed when investigating the gait parameters produced when walking with PGOs.
Ohta and colleagues reported an average stride length of 101 cm when ambulating with non-powered ARGOs in four subjects, but demonstrated a 7% increase in this variable with a powered ARGO. The hip joint actuator increased the amount of stride length in all the four SCI subjects. 20 One paper reported, cadence rates of 77 steps per minute with a powered IRGO and 61 steps per minute with an IRGO without power. 32
Discussion
Most studies selected for this review had a low number of subjects with a wide range of lesion level which made it impossible to prove efficacy of the test interventions used. Most papers reported means for a small n without SD or 95% confidence interval, which means that they did not provide a complete picture and may have led to a misinterpretation of the findings. Also, a non-significant decrease means that any observed decrease could not be considered anything more than a random finding such as those demonstrated when comparing walking speed.25,26 Studies should include an adequate number of SCI subjects to enable meaningful statistical analysis to be performed.
It is important to match subjects for age and injury level and severity of spinal injury (i.e. complete or incomplete injury) when comparing PGOs to RGO-type orthoses. One study attempted to alleviate this problem by pairing off subjects who had comparable lesion levels and matching their age in a crossover study, but did not include a washout phase between the test conditions.
The main variables which need to be measured in any future studies should be walking speed, energy efficiency and the total distance walked (endurance). These are the variables which need to be improved in order to eventually demonstrate efficacy of PGOs for providing the means of ambulation for SCI subjects in favor of RGO types. However, only one study 24 measured the endurance demonstrated when walking in an IRGO. No other studies measured this parameter.
The evidence suggested that the gait characteristics demonstrated by SCI subjects when walking in non-powered orthoses were not comparable to that of healthy subjects, and indicated the need for the addition of powered mechanical joints in the devices. Most SCI subjects manage well in a wheelchair as it is faster and more efficient than walking in reciprocal orthotic devices, which are also expensive in terms of time, money and effort. 25 When considering PGOs, the study by Ohta indicated that an average increase in gait speed (5.5%) may be achieved following the addition of power to the hip joints in an ARGO when worn by SCI subjects with injury levels between T5 and T12. However, the addition of power to the knee in one SCI subject with a lesion at T12 produced a much larger increase in gait speed of 23% and also increased the step length by 7%.
One parameter that has been largely overlooked in studies involving PGOs is the effect on the unacceptably high physiological cost index (PCI) of walking in current non-powered devices. This has been cited as one of the main reasons for discontinuation of use by SCI subjects. This could be due to the need to reach forward using crutches or other walking aids to give extrinsic stability and aid propulsion and the subsequent high use of the upper body and arm muscles. One study 24 demonstrated a reduction in PCI by SCI subjects when walking with an unpowered IRGO compared to bilateral locked KAFOs. The authors indicated that reduced use of the upper body and arms in the IRGO may have been a contributing factor. However, no powered RGO PCI studies were found in the literature.
Studies investigating the effect of orthotic intervention on PCI in less-disabled subjects have demonstrated varying results. One study investigated the effect on PCI in anterior poliomyelitis subjects when walking with bilateral stance control KAFOs (which allow knee flexion during swing, but a locked knee during stance) compared to locked KAFOs. 34 There was surprisingly no significant reduction in the PCI data acquired. It is therefore unclear as to the extent to which PGOs could offer a solution to reducing this parameter if both knees were able to flex via externally-applied power without also supplying power to the hips. The provision of cyclic power to both hip and knee joints simultaneously could reduce PCI values in SCI subjects and is a hypothesis which requires future investigation. Perhaps a multidimensional assessment of gait function other than speed and distance would be helpful in determining whether there is any functional gain other than ability to walk in a straight line without specific functional purpose can also be a future area of study. The excessive weight of current powered devices and the potential benefits of reducing weight in future designs also needs to be addressed.
Future studies should therefore include the following:
An investigation into the design and manufacture of more advanced powered orthoses with a view to further improving gait characteristics of SCI subjects. Simultaneous activation of hip and knee actuators should be available in future designs. While cosmesis was not investigated in the studies analyzed for this paper, consideration should be given to improve cosmesis and reduce noise levels produced by actuators in new designs. A comparison between the effects of novel powered orthoses with those of IRGOs should be performed, and all pertinent gait parameters plus PCI calculations compared. The effect of powered orthoses on gait parameters should be more widely determined over a longer period of time than currently performed. The effect of the powered orthoses on quality of life measures and social participation in SCI patients should be investigated. Interaction between PGOs and wheelchairs should be considered in new designs.
Conclusion
The limitations of this study include the low number of studies involving powered orthoses available in the literature and the low number of subjects participating in these studies, which negated the possibility of assessing the positive effects of this type of orthosis in SCI patients. Another limitation was a potential lack of reliability measures of the assessors. Although existing studies have had positive effects on certain parameters, variables such as cadence and walking distance have not been routinely measured in this type of orthosis.
Consequently there is not enough evidence to prove the efficacy of powered orthoses when used for walking by SCI patients and no conclusions can be derived from literature currently available. However, the development of powered orthoses is still in its infancy and progress needs to be made to improve their functionality and performance envelopes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.