
Abstract
Background:
Severe facial hypertrophic scars are known to severely impact emotional well-being. Pressure therapy by means of transparent face masks has been used for almost 40 years, but evidence about the clinical effects remains sparse.
Objectives:
To provide a summary on the efficacy of transparent face masks in the treatment of facial hypertrophic scars.
Methods:
A literature search was conducted in PubMed, MEDLINE, and Cochrane databases through 1 January 2018. Articles describing the clinical effects of facial pressure therapy for remodeling the face after trauma or surgery with a validated tool were included. This review included studies of participants treated with facial hypertrophic scars, both minors and adults.
Results:
Three articles involving 33 patients were selected for inclusion. Two studies described statistically significant improvement in facial scars measured by durometer, ultrasound, and the Patient and Observer Scar Assessment Scale (POSAS).
Conclusions:
Facial pressure masks have been shown to deliver significant improvement in facial scars, measured by both subjective and objective tools. However, only three studies could be included in this literature review. Also, because of considerable limitations of the studies, it remains difficult to draw substantial conclusions about the efficacy of transparent face masks.
Clinical relevance
This literature review provides a summary of the current evidence on the subjectively and objectively measured clinical effects of transparent face masks in the treatment of facial scars, highlighting the need for further research on this topic.
Background
Hypertrophic scars caused by facial burns can have a detrimental effect on patient’s mental well-being. The cornerstone in treating hypertrophic scars in the face consists of exerting mechanical pressure. Early treatment options consisted of hoods that were made of elastic fiber. However, due to the irregular shape of the face, the amount of pressure they delivered was often insufficient, especially over concave sites of the face. In the 1980s, rigid transparent plastic face masks were introduced and they have become a widely accepted treatment method for hypertrophic facial scars.1–4 Although pressure therapy is widely used and accepted as the standard conservative therapy for treating hypertrophic facial scars, the exact working mechanism is not yet elucidated. Meanwhile, varying fabrication methods and different types of facial orthoses have been described.5,6
The conventional method of fabricating a custom transparent face mask requires an experienced orthotist/prosthetist. The fabrication process includes the formation of a negative and positive plaster mold, respectively, after which a transparent thermoplastic sheet is heated and molded over the positive plaster mold.2,7
In recent years, however, non-contact scanning of the face and three-dimensional (3D) printing of the mask have been developed and have become more attractive, as it is, in particular, more convenient and less burdensome for children.5,8–10 With the help of specialized software, the model obtained by 3D scanning can be adjusted, and a mask can be printed by a 3D printing machine.
Although fabrication methods for face masks are still developing, robust evidence about their clinical effects is limited. Wearing a full-face pressure mask for a prolonged period may have a negative impact on emotional well-being as it can be demanding and uncomfortable. However, the psychological impact of wearing a face mask is not well-documented. In addition, there is doubt about the intervention as an evidence-based strategy.
A literature review addressing clinical and adverse effects of pressure therapy by means of facial pressure mask therapy may be helpful. Hence, the aim of this literature review was to provide an overview of the effectiveness of facial pressure therapy by means of transparent face masks in the treatment of facial hypertrophic scars as well as the side effects of this therapy.
Methods
A computerized search was conducted in PubMed, MEDLINE, and Cochrane databases through 1 January 2018. The search query used in PubMed was (((“facial pressure mask” OR “face mask” OR “face mask” OR “facial orthoses”) AND (“scars” OR “hypertrophic scars” OR “burns”))). In addition, references were screened for other relevant articles.
Eligibility criteria
Inclusion criteria required articles to assess the clinical effects of facial pressure therapy for remodeling the face after trauma or surgery with a validated tool. This review included studies of both minors and adults treated for facial hypertrophic scars and protruding facial flaps after facial flap surgery.
Studies lacking actual data on the treatment outcome of the therapy were excluded, as well as studies that only described the formation process of a face mask and studies that were written in a language other than English. Primary outcome measurements were data obtained from tools for evaluating facial scars and adverse effects such as pain, pruritus, and psychological distress.
Randomized controlled trials, controlled trials, and in absence of these designs, observational studies (cohort studies, case-control studies, and case series) were also eligible for inclusion.
Data extraction
One researcher was involved in selection of articles matching the inclusion criteria and also in data extraction. A second researcher evaluated outcome measures and performed quality assessment of the included studies according to Oxford Centre for Evidence-Based Medicine guidelines. 11 Both researchers reviewed each article separately. Eleven study characteristics were extracted: lead author name (and publication year); study design; study population (age, nationality, scar type, and cause for mask therapy); mask materials; fabrication method; therapy details (daily hours of wearing, mean applied pressure, and time between injury and start of therapy); outcome measures (validated subjective and objective assessment tools); follow-up details; control groups; results; and adverse effects.
Results
The literature search identified 102 articles, of which 3 articles met the inclusion criteria (Figure 1: PRISMA flow chart). Articles included were studies based on the clinical effects of a transparent face mask on facial scars or on facial scars after facial flap surgery with protruding flaps, measured by a validated tool. Excluded articles consisted of articles that described other types of masks (such as laryngeal masks and respiratory masks). Furthermore, 25 articles that described the use of a face mask were excluded because they did not use any validated measurement tool or because they solely described the fabrication process. Study characteristics are summarized in Table 1.
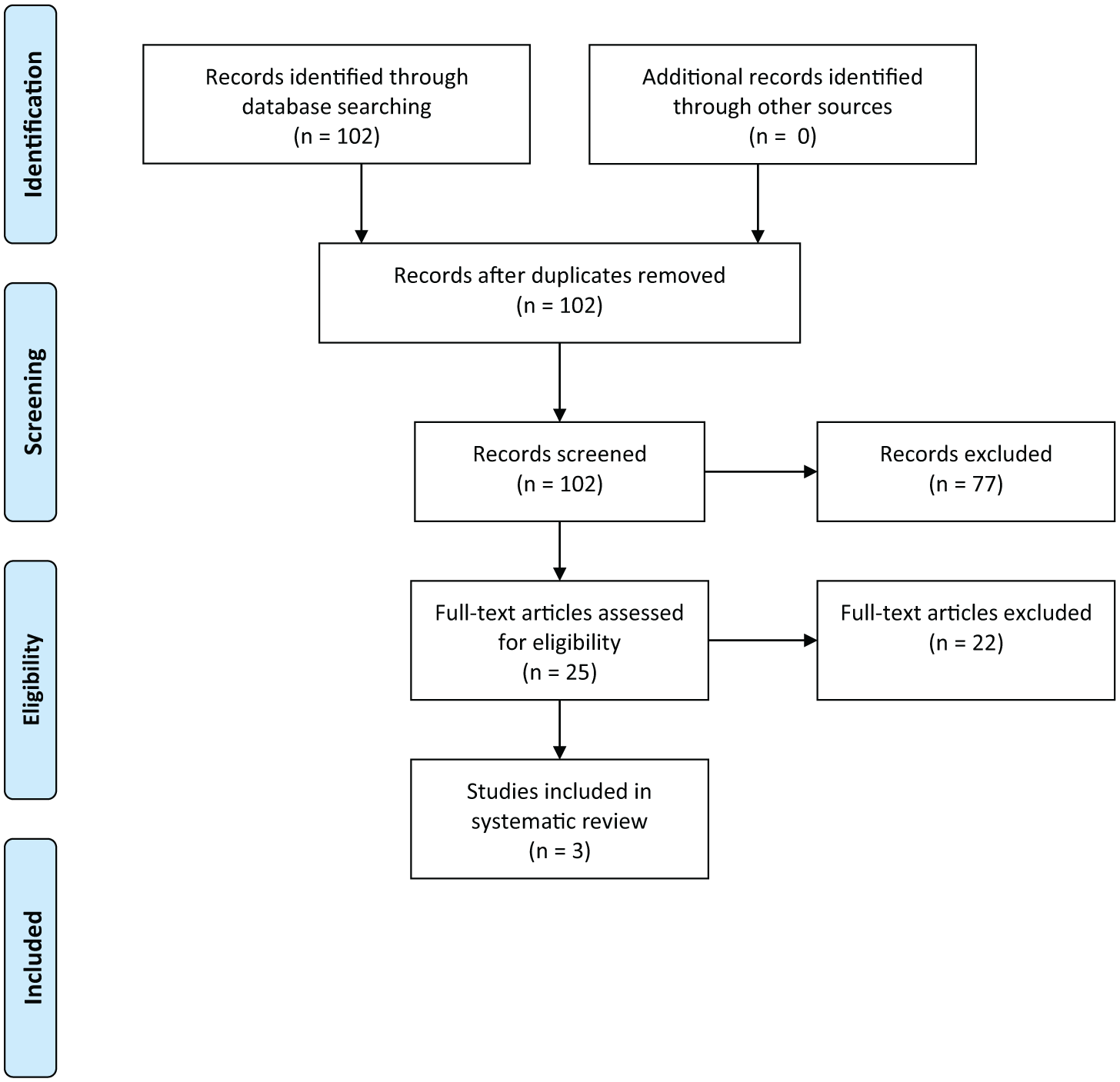
PRISMA 2009 flow diagram.
Study characteristics.
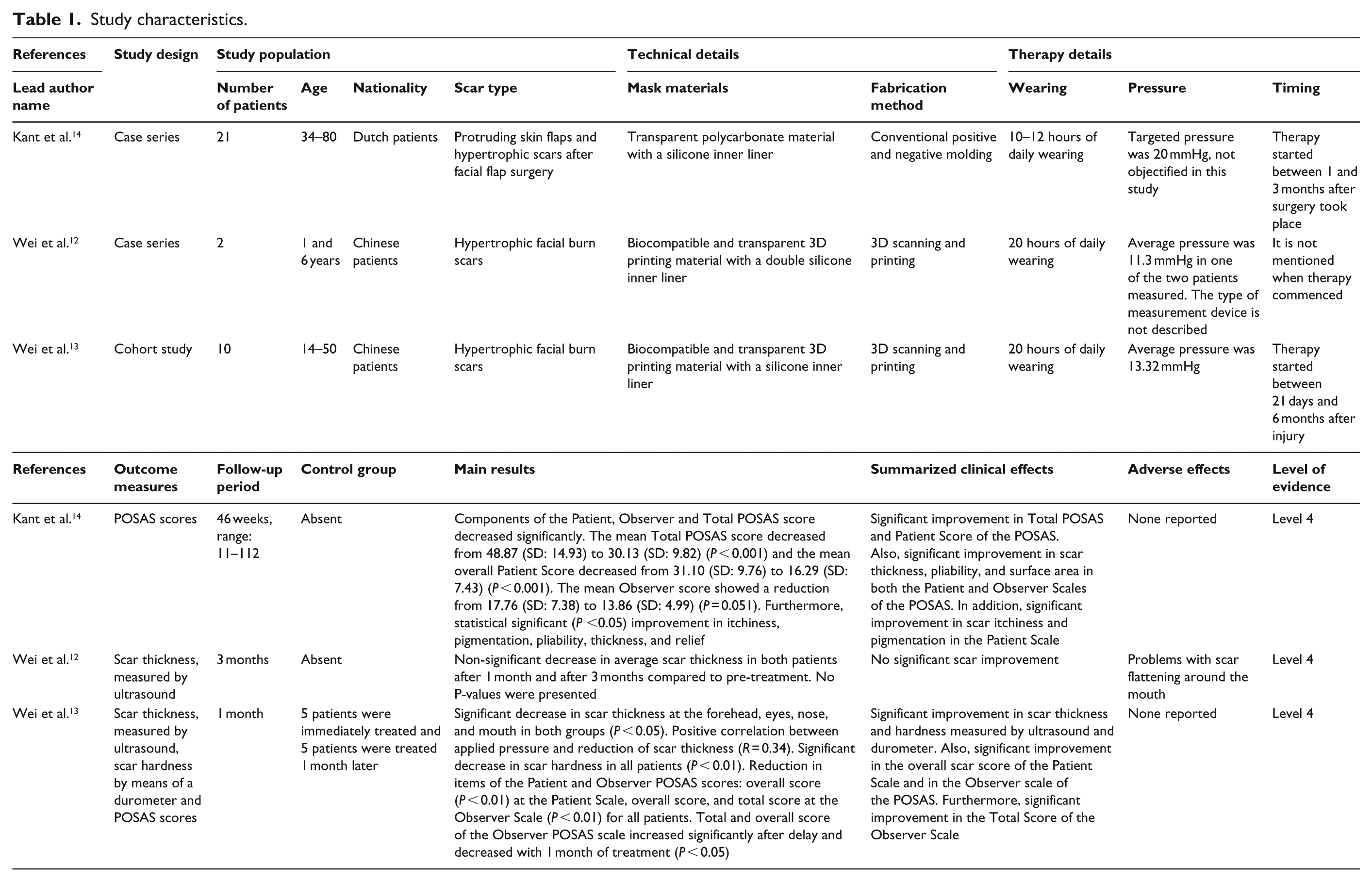
All studies were performed in vivo. In total, 33 patients (both children and adults, age ranging from 1 to 80 years old) with hypertrophic scars or unsatisfying results after facial flap surgery (patients with facial hypertrophic scars and protruding skin flaps) were treated with transparent facial pressure masks. Study populations size ranged from 2 to 21 patients. All of the studies were observational studies and evidence was rated as Level 4 according to the Oxford Centre for Evidence-Based Medicine guidelines. No controlled trials were identified. The included articles originated from China (two) and the Netherlands (one) and were published in 2016 and 2017. Two articles described patients with hypertrophic scars caused by thermal or chemical burns12,13 and one study 14 included patients with hypertrophic scars and protruding skin flaps after facial flap surgery.
Fabrication process and materials used
All three studies varied concerning the process and materials used to fabricate the face masks. The two studies by Wei et al.12,13 used non-contact scanning of the face followed by 3D printing for fabrication. In these studies, 3D scanning and adjusting took place by use of a computerized software model, after which masks were directly printed by means of biocompatible medical 3D printing materials.
In the study by Kant et al., 14 the face mask was fully custom fabricated by an experienced prosthetist using a plaster imprint (negative model) and molding (positive model) technique. All masks were reported to have an adequate pressure distribution between the mask and the face, regardless of the fabrication technique.
In all studies, a silicone inner liner was added to the mask.
Exerted pressure underneath the mask was monitored in the two Chinese studies12,13 by means of validated pressure sensors. The average pressure ranged from 9.34 mmHg to 22.62 mmHg. Mask therapy commenced between 3 weeks and 6 months after injury or surgery. In one study, this period was not described. 13
Follow-up information
Follow-up ranged from 1 to 25.7 months. Daily therapy duration aimed at between 10 and 20 hours. However, patient compliance to daily therapy was not objectively evaluated in any of the studies.
In one study consisting of 10 patients with active hypertrophic scars caused by extensive facial burns (>2.5% of the total body surface area), a control group was formed. 12 The treatment group consisted of five patients who were immediately treated and the control group consisted of five patients who were observed for 1 month before commencement of therapy.
Clinical effects
One study 14 reported outcomes solely by means of a validated scar assessment scale, the Patient and Observer Scar Assessment Scale (POSAS). This scale is designed for assessment of scars by both patient and clinician. It consists of two scales (the Patient and Observer Scale), each rating scars on six items and at an overall opinion from the clinician and patient between 1 and 10. The Total POSAS Score is the sum of the total Patient and Observer Scores.
The study by Wei et al. 13 only used an objective measurement for measuring scar thickness by means of an ultrasound instrument. The article by Wei et al. 12 also reported scar thickness measurements by means of ultrasound, scar hardness by means of a durometer and the POSAS.
Concerning the two studies that used ultrasound for scar measurements, the study by Wei et al. 12 measured scar thickness in six facial zones (forehead, eyes, nose, mouth, cheek, and chin). This study contained a 1-month delayed treatment group. In the delayed treatment group, scars thickness increased significantly during delay. After 1-month treatment, scar thickness decreased significantly in this group. Statistically significant improvement in scar thickness was found on the forehead, eyes, nose, and mouth after 1 month of treatment in both groups. The study also reported significant decrease in scar hardness after 1 month of follow-up in both groups.
In the study by Wei et al., 12 one item of both the Patient and Observer Scale (the overall assessment of the scar) decreased significantly for all patients after 1 month of treatment. For the Observer Scale, the overall score decreased significantly in all patients. In the delayed treatment group, the overall scar assessment item and the total score of the Observer Scale significantly increased after delay and decreased after 1 month of treatment.
Finally, this study showed a positive linear relationship between changes for scar thickness and the pressure applied locally (Pearson correlation coefficient r = 0.34).
Surface area demonstrated a statistically significant improvement between start and end of therapy in the Patient Scale of the POSAS in patients with hypertrophic scars and protruding flaps after facial flap surgery. 14 Furthermore, this study reported a statistically significant improvement in scar itchiness, pigmentation, pliability, and thickness. Concerning the Observer Scale, thickness, pliability, and surface area improved significantly. Furthermore, this study showed a significant decrease in the mean Patient Scale and Total POSAS Score between start and end of therapy. The mean Observer Scale did not show a statistically significant decrease.
The other study by Wei et al. 13 showed a decrease in average scar thickness after 1 month and after 3 months of treatment by ultrasound measurements compared to baseline in both patients. However, these differences in thickness were not reported as statistically significant.
Adverse effects and complications
Wei et al. 13 reported problems with scar flattening around the mouth, an area where the child moved a lot for speaking, which negatively affected the pressure around the mouth of the mask. No complications were reported in any study.
Discussion
This literature review aimed at outlining and critically evaluating the available evidence concerning the clinical effects of facial pressure masks in the treatment of hypertrophic scars.
With respect to these clinical effects, two of the three studies reported significant improvement on scars and facial flaps assessed by means of both subjective and objective measurements: ultrasound, durometer, and POSAS. The third study showed a reduction in scar thickness after 1 and 3 months; however, this difference was not statistically significant. No severe adverse effects were reported in the studies.
Evidence that was reviewed was limited to observational studies (one cohort study and two case series). Furthermore, patient populations were small, follow-up periods were short, and only study included a control group. Because of these limitations, it remains difficult to draw a substantial conclusion regarding clinical effectiveness of transparent facial masks.
Transparent facial pressure masks have been used for over three decades predominantly for the treatment of hypertrophic scars after burns. 1 Patients who are eligible for face mask therapy are required to be mentally stable enough to wear a face mask for several months and in some cases for over 2 years. Therefore, it is considered to be an extraordinarily demanding therapy and known to challenge patients’ compliance.15–17 Therefore, the scarcity of clinical evidence about the effects of face masks is understandable. However, a recent study about patients’ satisfaction with their facial appearance after finishing face mask therapy described that esthetic results to remain stable in a 5-year follow-up period with a study population of 87 patients. 18 However, this study did not describe the clinical effects of face masks.
Although the existing evidence about the clinical effects is limited, transparent facial pressure masks are the only modality for treating severe burn-related hypertrophic facial scars using mechanical pressure. Accordingly, face mask therapy is still the main treatment for severe facial scars. However, other modalities including microneedling, (sub)dermabrasion and fractioned laser therapy are also used for improving (less severe) hypertrophic facial scars in current clinical practice.19–23
In contrast, the use of mechanical pressure therapy on anatomic locations other than the face is well-documented.24–27 It has been shown to be an effective modality, hypothesized to work by decreasing blood flow and reducing collagen synthesis as a result. Another suggested effect caused by pressure therapy is hypoxia, resulting in fibroblast degeneration and loosening of collagen fibrils.28,29
The suggested scar enhancing effects of facial pressure therapy are based on exerting a certain amount of pressure. There is no consensus about the exact amount of needed pressure. In an article by Candy et al., 32 it is stated that applied pressure needs to be at least 24–25 mmHg to overcome capillary pressure in scar tissue. In other studies, lower pressure dosages also seemed acceptable and effective.24,31 Also, the suggested duration the mask should be worn daily varies in literature.2,32,33
In the studies included in this review, all face masks contained an inner layer of silicone gel. The rationale behind this was to add or optimize pressure in certain facial areas. Silicones are a well-known modality used in the treatment of scars.30,34 Silicone gel sheet therapy has been suggested to be effective in reducing scar thickness and improving pliability by its proposed occlusive effects on scars, affecting skin hydration and decreasing capillary activity, and thereby reducing collagen deposition.35–40
However, available evidence about the combined effect of both pressure garments and silicones on hypertrophic scars is still inconclusive.30,39,40
Conclusion
This review provides an overview of the current evidence for the clinical effects of transparent facial pressure masks in the treatment of hypertrophic facial scars and protruding flaps. Two of the three studies described statistically significant improvement in facial scars and facial skin flaps, both subjectively and objectively measured. However, these studies had substantial limitations. Therefore, further clinical research with larger study populations and including control groups is necessary to confirm the suggested clinical beneficial effects of face masks on hypertrophic facial scars and protruding skin flaps.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.