
Abstract
Background:
Individuals with severe lower extremity injuries often require ankle–foot orthoses to return to normal activities. Ankle–foot orthoses alignment is a key consideration during the clinical fitting process and may be particularly important during dynamic activities such as running.
Objective:
To investigate how 3° changes in sagittal plane ankle–foot orthoses alignment affect running mechanics.
Study design:
Controlled laboratory study.
Methods:
Twelve participants with unilateral lower limb injury ran overground and lower extremity running mechanics were assessed. Participants wore their passive-dynamic ankle–foot orthoses in three alignments: clinically fit neutral, 3° plantarflexed from clinically fit neutral, and 3° dorsiflexed from clinically fit neutral.
Results:
The 3° changes in sagittal alignment significantly influenced ankle mechanics during running. The plantarflexed alignment significantly decreased the peak ankle plantarflexor moment, peak knee extensor moment, and peak ankle and knee power absorption and generation compared to more dorsiflexed alignments. Alignment also altered footstrike angle, with dorsiflexed alignments associated with a more dorsiflexed footstrike pattern and plantarflexed alignments toward a more plantarflexed footstrike pattern. However, alignment did not influence loading rate.
Conclusion:
Small changes in ankle–foot orthoses alignment significantly altered running mechanics, including footstrike angle, and knee extensor moments. Understanding how ankle–foot orthoses design parameters affect running mechanics may aid the development of evidence-based prescription guidelines and improve function for ankle–foot orthoses users who perform high-impact activities.
Clinical relevance
Understanding how ankle–foot orthoses alignment impacts biomechanics should be a consideration when fitting passive-dynamic devices for higher impact activities, such as running. Individual running styles, including footstrike patterns, may be affected by small changes in alignment.
Keywords
Background
Surgical advances now allow the preservation of limbs that may have been previously amputated after severe lower extremity trauma. 1 However, patients may be left with functional deficits including musculoskeletal weakness and gait compensations. Ankle–foot orthoses (AFOs) can be an important part of rehabilitation and may be prescribed to improve gait in individuals with lower extremity neuromuscular dysfunction. 2 AFOs can be used to improve functional characteristics of the ankle–foot complex in an injured limb by controlling range of motion, optimally positioning the limb for the desired activity, and allowing energy storage and return.3–5
Optimizing AFO design criteria is a complex and multifactorial process. The majority of clinically prescribed AFOs are passive devices that rely on material properties, thickness and shape,6–8 and spring-like mechanisms 9 to provide energy storage and return during walking.6,10,11 AFO alignment is a key factor of proper fit, and small changes in alignment can induce important alterations in walking mechanics. Altering sagittal plane AFO alignment to a more plantarflexed (PF) alignment decreases peak knee flexion, the peak internal knee extensor moment,12–14 and quadriceps activity 13 during walking. AFO alignment is important to maximize comfort, function, and a pain-free range of motion at the ankle, although the criteria for “optimal” alignment are not well defined. Prosthetics literature indicates that different prosthetists will recommend different alignments for the same individual, indicating that a range of alignments could be considered clinically acceptable 15 ; the same is likely true for AFOs. However, the specific criteria a clinician needs to consider for optimizing function when determining alignment are not always known or agreed upon.14,16
The design of an AFO should account for many of the activities in which an individual participates. AFOs are typically designed to improve walking, but new approaches, including passive-dynamic AFOs, have enabled individuals to participate in high-impact activities, such as running.2,17–20 Previous work has shown that self-selected running speeds with a passive-dynamic AFO can be equivalent to able-bodied individuals; however, gait asymmetries still exist and higher loading rates are present on the unaffected side. 21 Relatively little information is available to guide the clinician’s decision-making process when preparing an AFO for high-impact activities, such as running. Sagittal AFO alignment is one key design parameter that can be readily modified and may have a direct effect on running mechanics. Given the larger demands, AFO design parameters are likely even more important during dynamic activities than during walking.
Aligning an AFO in either plantarflexion or dorsiflexion has the potential to impact how the foot strikes the ground during running, and there may also be subsequent effects on more proximal joints. A PF footstrike angle at initial contact is associated with a forefoot strike pattern and dorsiflexed (DF) footstrike angle is associated with a rearfoot strike pattern. 22 The majority of able-bodied runners use a rearfoot strike pattern, 23 which is usually associated with the presence of an impact peak and higher loading rates.24,25 While the literature is inconclusive, 26 some studies have shown that increased loading has been linked to overuse injuries.24,27–29 Previous literature has shown that moving from a rearfoot strike pattern to a midfoot or forefoot strike pattern may decrease loading rates and reduce the magnitude of impact peaks in the vertical ground reaction force.23,30 Higher loading rates may be of even greater concern in individuals who have experienced limb threatening injuries due to the injured tissues, as well as more frequent presence of pain in the limb.31,32
The alignment of an AFO is an important consideration, because how an individual loads the device can affect how the device stores and returns mechanical energy, affecting overall mechanics. Therefore, the purpose of this study was to investigate how 3° changes in sagittal plane AFO alignment affected lower extremity running mechanics in patients with plantarflexor weakness.
Methods
Subjects
Twelve individuals who had sustained unilateral lower limb injuries resulting in clinically documented plantarflexor weakness participated in this study (Table 1). Injuries were often complex and surgical procedures multifactorial, but the patients can be generally classified as having their primary deficits due to fracture or nerve injury, with many experiencing soft tissue injury and loss. An overview of the surgical management of this patient population is described by Shawen et al. 1 The nature of the injuries and associated loss of function resulted in the clinical prescription of a passive-dynamic AFO. All participants read and signed informed consent in accordance with policies set forth by the Brooke Army Medical Center Institutional Review Board.
Subject characteristics.
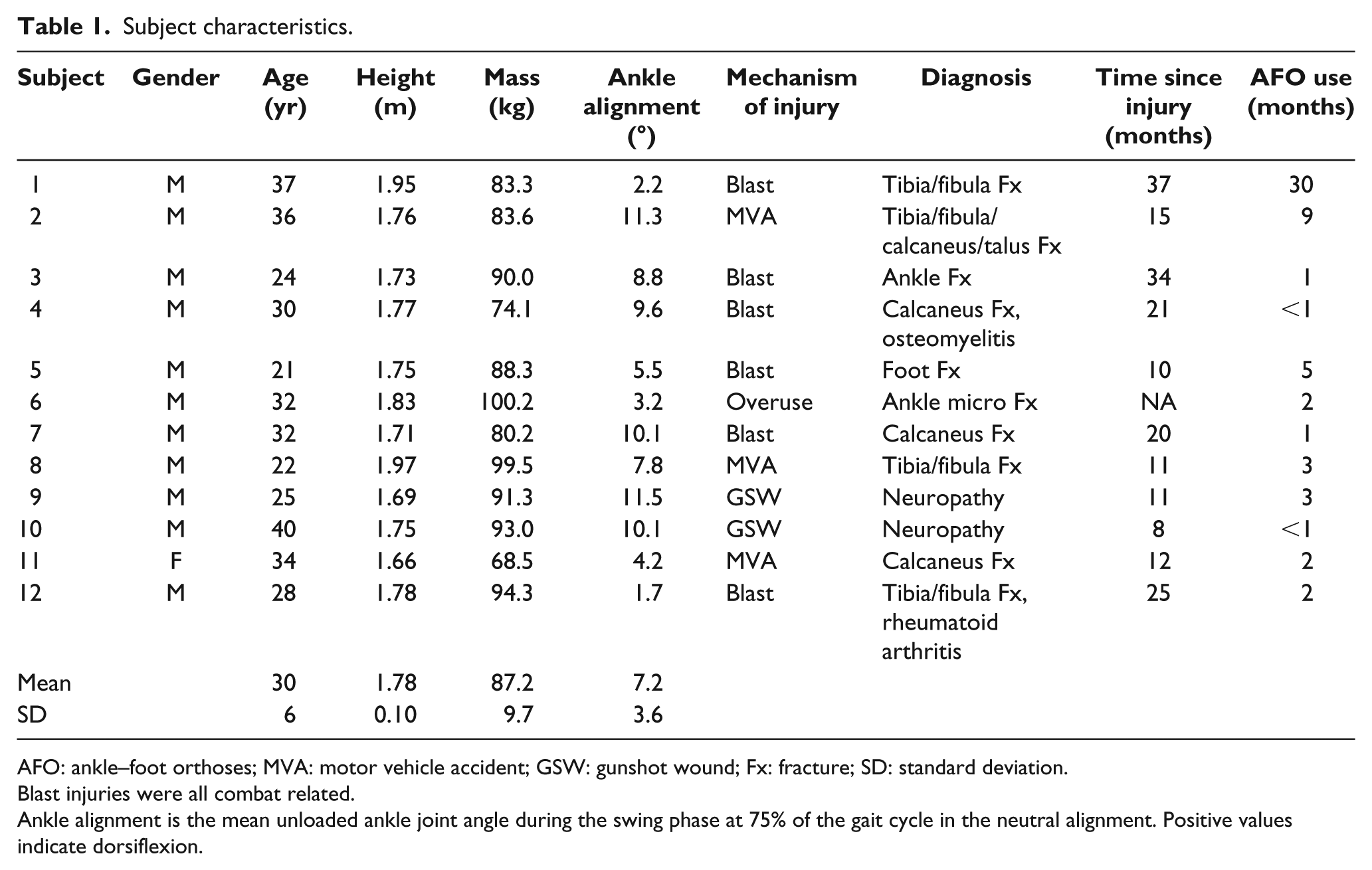
AFO: ankle–foot orthoses; MVA: motor vehicle accident; GSW: gunshot wound; Fx: fracture; SD: standard deviation.
Blast injuries were all combat related.
Ankle alignment is the mean unloaded ankle joint angle during the swing phase at 75% of the gait cycle in the neutral alignment. Positive values indicate dorsiflexion.
Experimental setup
A 6-degree-of-freedom marker set with 57 retro-reflective markers was used to capture subject motion. A 26-camera motion capture system (120 Hz, Motion Analysis Corp., Santa Rosa, CA, USA) tracked marker trajectories, and kinetic data were captured using three AMTI force platforms embedded in the center of a 20 m runway (1200 Hz, AMTI, Inc., Watertown, MA, USA.). A detailed overview of the marker set, equipment setup, and data collection procedures can be found in Wilken et al. 33
Each subject had been clinically prescribed the Intrepid Dynamic Exoskeletal Orthosis (IDEO), a custom, passive-dynamic AFO that has been described previously.2,18,20,34 Different IDEO design components have been investigated to improve the customization process,13,17,35,36 and efforts are underway to increase its availability to a broader population through civilian providers. Subjects wore this AFO for both walking and running, among other activities. The IDEO was designed to intentionally mimic some of the properties of a prosthetic running foot, specifically that the posterior strut deflects to store and return energy. Clinical fit of the AFO, including neutral alignment, was determined by a certified prosthetist/orthotist with extensive IDEO fitting experience. Neutral alignment was based on the experience of the clinician, patient preference, and pain-free range of motion. The shape of the footplate, tibial cuff, and positioning of the posterior strut are all involved in the overall alignment of the AFO. However, in this study, only the positioning of the posterior strut was experimentally modified relative to the neutral fit using a 3° wedge (polyurethane alignment wedge, Össur, Reykjavik, Iceland) inserted at the distal portion of the strut-footplate interface, to re-align the AFO in a more PF or DF position relative to the neutral alignment (Figure 1). The 3° alignment change from neutral alignment was selected to represent changes implemented clinically and within the range of variability in alignment of different prosthetists and orthotists.15,37 A repeated measures study design was used to compare each subject across three alignment conditions, rather than defining a priori a neutral alignment to be used by all subjects, which would not be clinically appropriate for patients using AFOs. All participants underwent the same therapeutic and rehabilitation program during recovery from their injuries; this program incorporated running rehabilitation and encouraged a midfoot or forefoot strike pattern on the AFO limb. 18
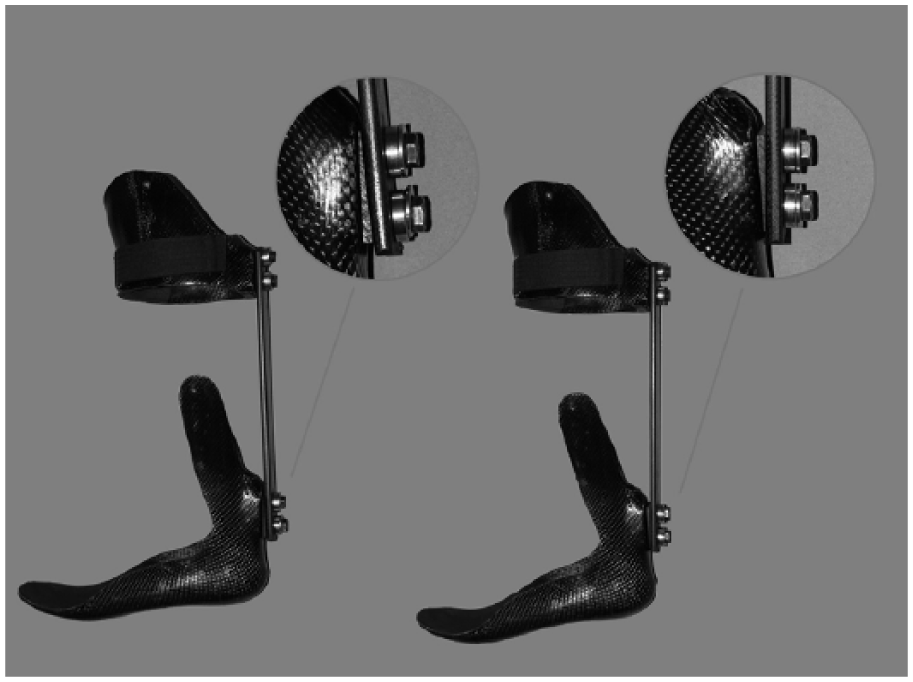
The intrepid dynamic exoskeletal orthosis (IDEO). A 3° wedge was inserted between the distal portion of the strut and footplate to align the AFO in dorsiflexion (left) or plantarflexion (right).
Protocol
Participants visited the laboratory for one data collection session in which all three alignment conditions were tested in a randomized order. Subjects had approximately 30 min accommodation time in each alignment condition prior to participating in the running collection. Kinematic and kinetic data were recorded as subjects ran overground at a self-selected speed. Five strides with full foot contact on one of the force platforms were collected on each limb. Ground reaction force data were used to determine heel strike and toe-off. After completing all conditions, subjects ranked their preference for each of the three AFO alignments. No instructions were given on the criteria to use to rank preference.
Data analysis
Data were initially processed using Cortex (Motion Analysis Corp., Santa Rosa, CA, USA), then exported to Visual3D (C-Motion, Inc., Germantown, MD, USA) for further analysis. Kinematic and kinetic data were interpolated using a cubic spline and filtered using a fourth-order Butterworth low-pass filter with cutoff frequencies of 6 and 50 Hz, respectively. A 13 segment full body model was created for each subject and was scaled by subject mass (inclusive of IDEO mass) and height. The approximate mass of the AFO was 2 kg. Joint angles were calculated using Cardan rotation sequences, and inverse dynamics were used to calculate joint moments and powers.38,39 Experimental AFO alignment was determined by the ankle angle at 75% of the gait cycle, when the device was unloaded during swing. Ankle range of motion was calculated by taking the maximum and minimum ankle angle over the gait cycle. Footstrike angle was calculated as the angle of the foot in the sagittal plane at heel strike subtracted from the static foot angle while standing with the foot flat on the floor. 22 Continuous data were time-normalized to 100% gait cycle. Joint moments and powers were scaled to body mass and ground reaction forces were scaled to body weight. Peak joint angles, moments, and powers were identified from individual trials and used for further analysis. Impact peaks were identified as the peak vertical ground reaction force preceding a local minimum. 24 If that first initial peak in the vertical force, commonly designated as the impact peak, was not present, the first peak in the vertical ground reaction force was identified. Loading rate was calculated between 20% and 80% of the period between footstrike and the identified vertical ground reaction force peak.
Statistical analysis
A two-way repeated measures analysis of variance (2 limbs × 3 alignment conditions) was performed in SPSS (IBM Corporation, Armonk, NY, USA) to identify significant main effects and interactions among the dependent variables. Post hoc paired t-tests identified differences among alignment conditions and between limbs. Sequentially rejective Bonferroni–Holm corrections were used for multiple comparisons (unadjusted α = 0.05).
Results
Running speeds were not significantly different among alignment conditions (P = 0.146) and were 3.1 (0.4), 3.0 (0.4), and 3.1 (0.4) m/s for the DF, neutral, and PF alignment conditions, respectively (mean (SD)). Overall, eight participants ranked PF as their preferred alignment, three chose DF as their preferred alignment, and only one participant preferred the neutral alignment. Unless specifically noted, only statistically significant interactions, main effects, and pair-wise comparisons are reported. Mean (SD) and ranges for peak joint angles, moments, and powers are presented in Table 2 and mean profiles across the gait cycle are shown in Figure 2.
Mean (SD) and (range) peak data for all three AFO alignment conditions and the neutral condition on the unaffected limb.
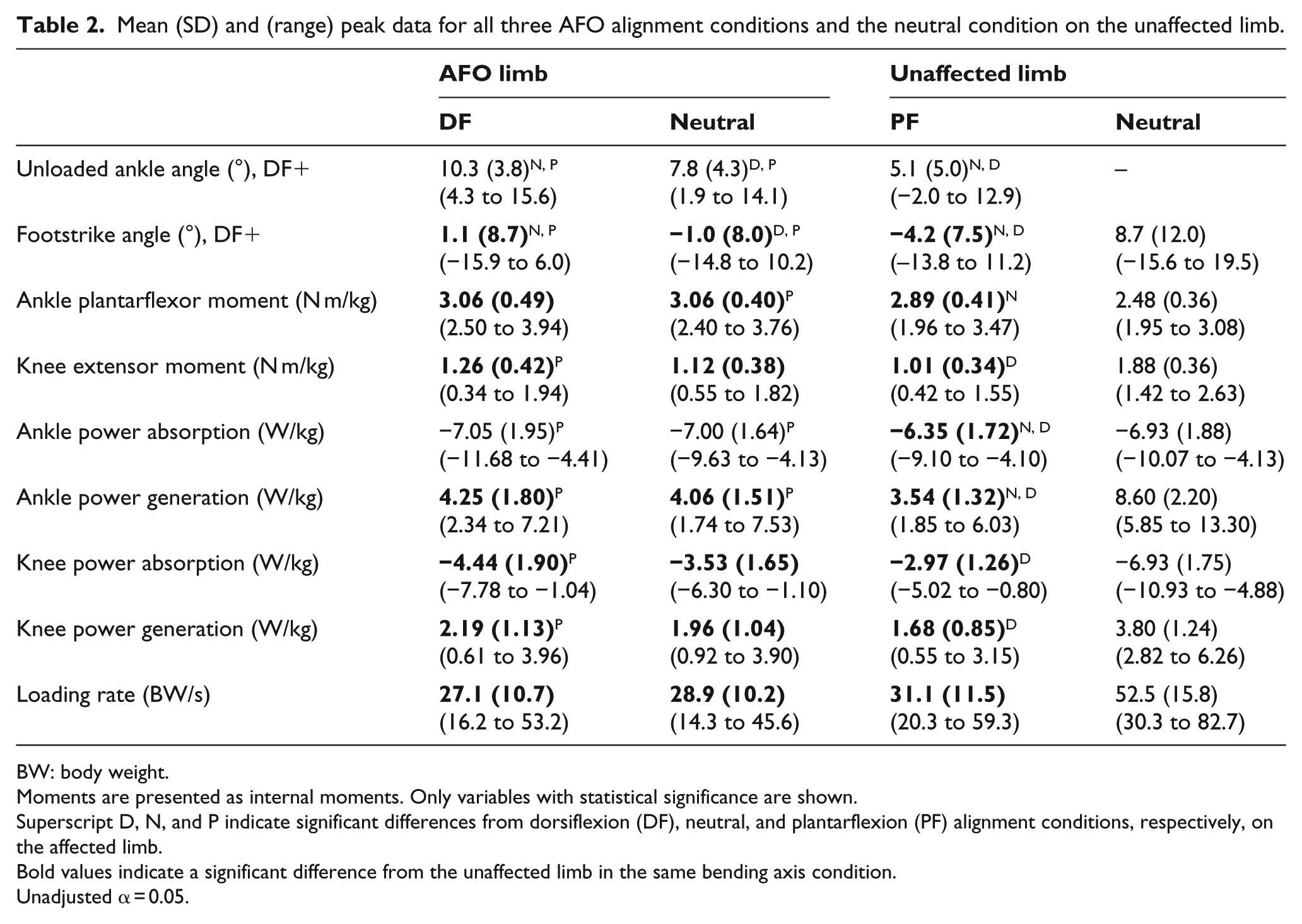
BW: body weight.
Moments are presented as internal moments. Only variables with statistical significance are shown.
Superscript D, N, and P indicate significant differences from dorsiflexion (DF), neutral, and plantarflexion (PF) alignment conditions, respectively, on the affected limb.
Bold values indicate a significant difference from the unaffected limb in the same bending axis condition.
Unadjusted α = 0.05.
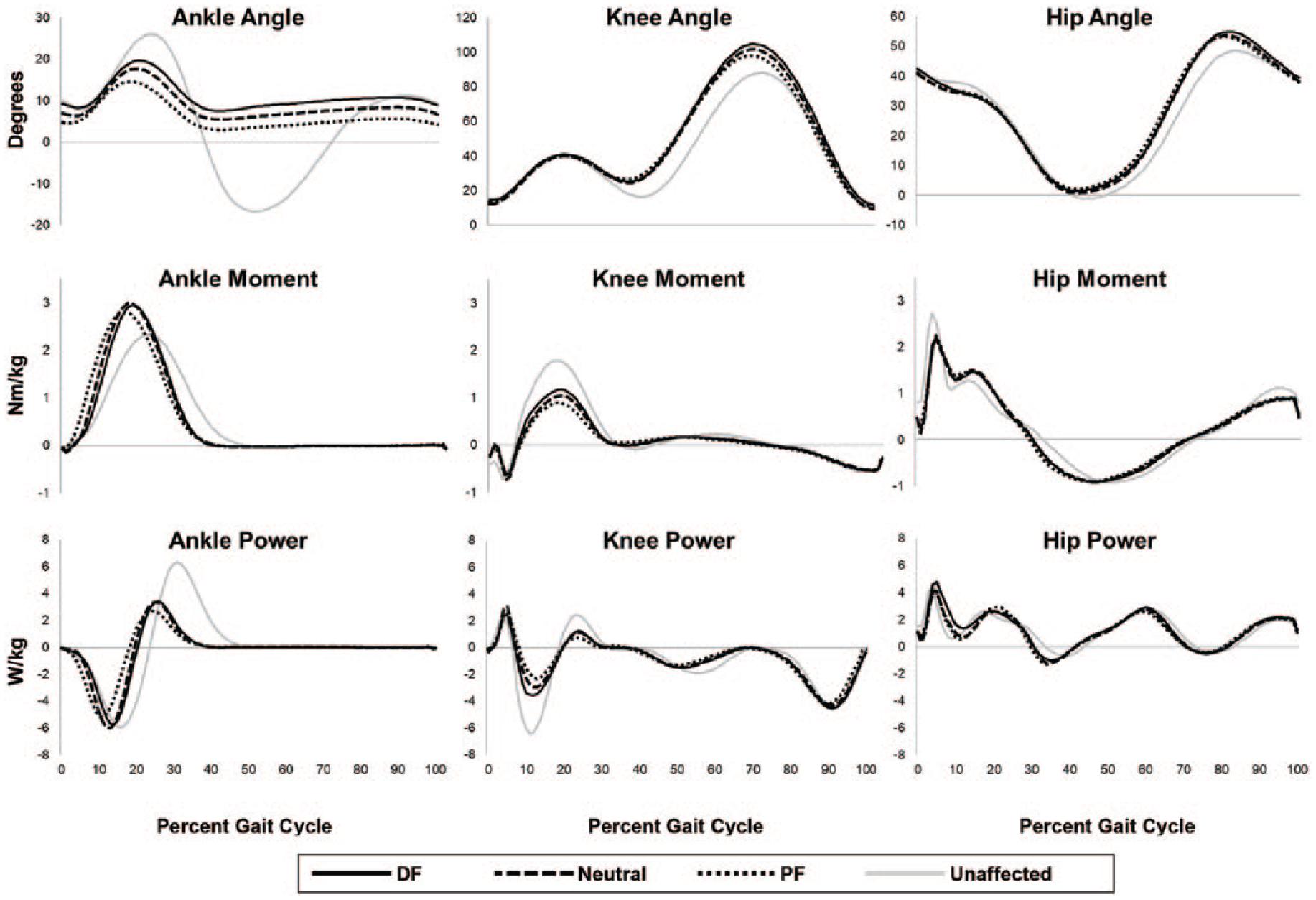
Mean angles, internal moments, and powers for the ankle, knee, and hip joints across the gait cycle. Joint angles are presented as flexion/dorsiflexion (+) and extension/plantarflexion (–), joint moments are extensor/plantarflexor (+) and flexor/dorsiflexor negative (–), and joint powers are generation (+) and absorption (–). Gray lines indicate unaffected limb data in the neutral condition.
Joint angles
Although variation in clinical alignment resulted in between subject variability, the 3° wedge significantly changed the neutral ankle angle (P < 0.001). Specifically, the 3° wedge caused a net change in the unloaded ankle angle (during swing) 2.74° (1.20°) in the PF condition and 2.27° (1.13°) in the DF condition. AFO alignment did not significantly affect peak knee flexion during stance or peak hip angles. There was a significant main effect of limb (P < 0.001), such that in comparison to the unaffected limb, the AFO limb had significantly less ankle range of motion during walking for all conditions (P < 0.001).
Footstrike angles
Footstrike angles were significantly altered by AFO alignment (P = 0.024). On average, participants landed in greater degrees of PF in the PF alignment and in greater degrees of DF in the DF alignment. The changes in alignment only affected the positioning of the foot as tibial angles at initial contact were not significantly different among alignment conditions (P = 0.378) and there were no kinematic differences across other joints.
Joint moments
There was a significant interaction in the peak ankle plantarflexor moment in late stance (P = 0.002) such that the AFO limb had lesser peak ankle moments with the PF alignment than the neutral alignment (P = 0.003), although neither were significantly different from DF. The unaffected limb’s peak ankle moments were significantly lower than the AFO limb’s (P ⩽ 0.004), but were not influenced by the contralateral changes in alignment. At the knee, there was a significant interaction in the peak internal extensor moment during stance (P = 0.002) such that PF alignment resulted in significantly lesser moments in the AFO limb than the DF alignment (P = 0.002). Comparisons between neutral and PF (P = 0.015, adjusted α = 0.010) and neutral and DF (P = 0.123) were not significantly different. Alignment on the AFO limb did not significantly alter knee moments on the unaffected limb. Comparisons between limbs showed that the unaffected knee had greater knee extensor moments (P ⩽ 0.005) than the AFO limb. Hip moments were not significantly altered by alignment condition.
Joint powers
There was a significant interaction between alignment and limb for ankle joint power (P < 0.001) such that the AFO limb had significantly less peak ankle power absorption and generation in the PF alignment condition compared to the neutral (P ⩽ 0.005) and DF (P ⩽ 0.004) alignments. The unaffected limb was not influenced by alignment changes. All alignment conditions had significantly greater power generation in the affected limb (P < 0.001). There was also a significant interaction between alignment and limb for peak knee power absorption (P = 0.003) and subsequent power generation (P = 0.002). In the AFO limb, participants experienced significantly less knee power absorption (P = 0.004) and generation (P < 0.001) in the PF than the DF alignment, and alignment did not influence power of the unaffected knee. Knee power absorption and generation were consistently greater in the unaffected limb than in the AFO limb (P ⩽ 0.022). Hip power absorption and generation were not significantly affected by alignment condition.
Loading rates
Loading rates were not significantly different between alignment conditions and there were no significant interactions. Loading rates on the AFO limb were 91%, 82%, and 64% less than the unaffected limb in the DF, neutral, and PF alignments, respectively (P < 0.001), due largely to the consistent presence of an initial impact peak in the unaffected limb’s vertical ground reaction force (Figure 3).
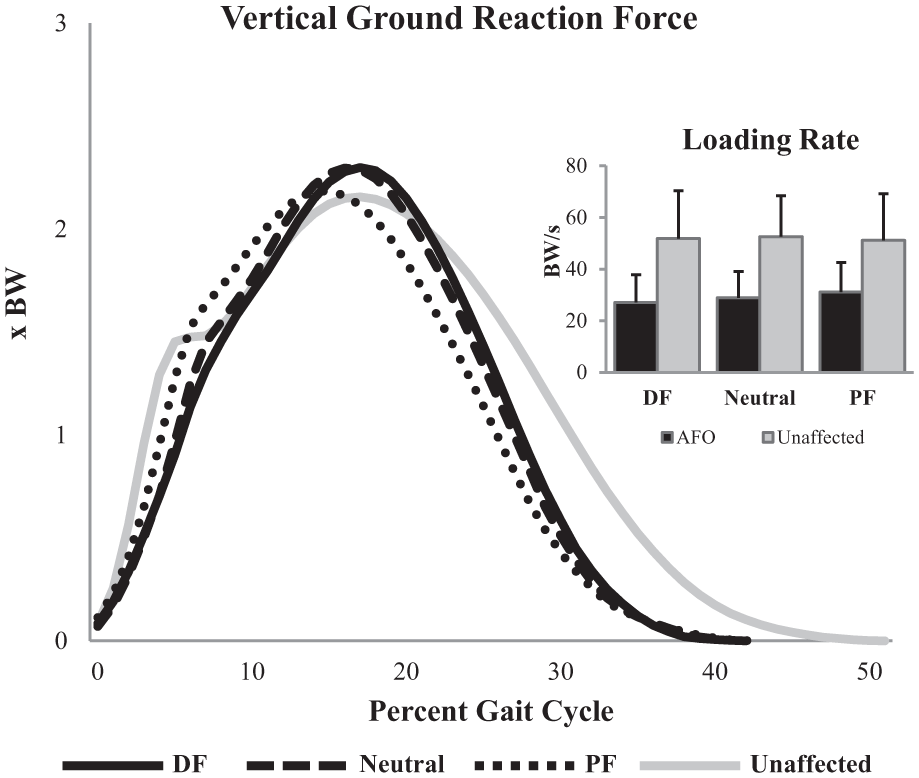
Mean vertical ground reaction force for the three alignment conditions and the neutral condition on the unaffected limb across the stance phase of the gait cycle. Also displayed are the average loading rates (SD bars) for each condition, on both the AFO and unaffected limbs.
Discussion
The purpose of this study was to investigate how 3° changes in sagittal plane AFO alignment affected running mechanics. AFO alignment significantly affected footstrike angles, as well as knee and ankle moments and powers. Few kinetic differences were observed between the DF and neutral alignments, while aligning the ankle in greater PF produced more consistent effects.
Specifically, the PF alignment resulted in approximately 15% less peak ankle power absorption and generation than the neutral and DF alignments. This was unexpected, as a more PF foot contact (mid or forefoot) is encouraged during rehabilitation with this AFO 18 with the intent of increasing mechanical energy storage and return in the posterior strut. Numerous research efforts are aimed at improving ankle power generation in populations with ankle plantarflexor weakness,10,40,41 but a more PF alignment appears to negatively affect energy storage and is not a recommended strategy. It is possible that the effects of a more PF position on proximal joints or increased difficulty controlling the device altered how individuals loaded the device, yielding the observed effects.
While the PF alignment did not provide ankle power benefits, it did reduce the internal knee extensor moments compared to more DF alignments. Similar decreases in the internal knee extensor moment12–14 and in the demands placed on the quadriceps musculature 13 with more PF AFO alignments have been reported during walking. These results may have important implications for individuals with quadriceps weakness or for delaying quadriceps fatigue during running. The reduced demand placed on the knee extensors also may have contributed to the majority (8/12) of individuals preferring the PF alignment overall.
Alignment systematically influenced the footstrike angle at initial ground contact on the AFO limb. The results do not imply that all subjects landed in a rearfoot strike pattern in the DF condition and in a forefoot strike pattern in the PF condition, but that the 3° changes in the AFO’s alignment corresponded to the change in angle of the foot at initial contact. The lack of significant changes to tibial angles at initial contact indicates that the changes in alignment drove the differences observed in footstrike angles on the AFO limb. On average, participants landed in a more PF position on the AFO limb than on the unaffected limb, creating inter-limb asymmetries that may have important implications if maintained long term. 27
Footstrike pattern is an important consideration for running and has received much attention due to its purported association with lower extremity overuse injuries,29,42 although imposing a change in footstrike pattern by adjusting AFO alignment should not be interpreted the same as freely modifying footstrike pattern. Runners who are taught to strike on their forefoot tend to have greater ankle power absorption and generation than those who rearfoot strike,43–45 while in the present study, aligning the AFO in PF decreased peak ankle power absorption and generation. At the knee, the decreases in power absorption 44 and internal extensor moment 45 were consistent with previous reports on forefoot strike patterns. In the present study, when the ankle was aligned in greater PF, subjects landed in greater degrees of foot plantarflexion, but these biomechanical changes did not affect the loading rate. However, unaffected limb loading rates were significantly greater than on the affected limb, which is consistent with research on individuals with other traumatic lower limb injuries, such as amputation. 46
The results of this study and others14,47 demonstrate that alignment changes of only a few degrees may produce significant changes in limb mechanics and muscle activation. These data can be used in conjunction with clinical evaluation and fitting procedures to guide care of individuals requiring a dynamic AFO. Although this study focused on running, patients wore the same AFO for a variety of other activities, and the optimal alignment of a single passive-dynamic AFO used for multiple activities is likely multifactorial.
Limitations
The primary limitation of this study was that all subjects were not prescribed the same neutral alignment, as custom alignments are the standard of care for this type of AFO. For individuals with lower extremity musculoskeletal injury, it is important to align each AFO to meet the specific needs of the individual, and therefore, it would not have been possible to achieve identical alignments for all participants. The second limitation is that many of the participants in this study cannot run pain-free without an AFO, so a no-AFO condition was not included. Third, the participants’ injuries were heterogeneous, although all exhibited similar musculoskeletal weaknesses and were prescribed this AFO to improve pain and function. Previous studies have shown that healthy controls walking in a carbon-fiber AFO 48 have almost identical gait mechanics to injured individuals walking in the AFO used in this study, 13 which suggests the mechanics observed are largely driven by the presence of an AFO regardless of the specific injury. Fourth, this study did not determine how a user’s experience with an AFO affected his or her gait mechanics. All participants in the present study had received more than eight rehabilitation sessions prior to participating in this study. Finally, this subject population consisted of Service Members with lower limb injuries who were otherwise in good physical health. This population may not be representative of all AFO users, but may better represent the AFO users who can participate in high-impact activities.
Conclusion
Altering the sagittal alignment of an AFO by 3° produced significant changes in lower extremity running mechanics. A more PF alignment reduces ankle power absorption and generation, but also reduces the knee extensor moment, which may have important implications for running as an endurance activity. Footstrike angles were also influenced by alignment, but these changes did not significantly affect loading rates, which are often linked to overuse running injuries. Overall, sagittal plane AFO alignment is an important design parameter that should be critically evaluated to meet patient needs when prescribing an AFO for running. A better understanding of how AFO alignment affects running mechanics and biomechanical risk factors for overuse injuries could contribute to the development of evidence-based prescription guidelines and improve rehabilitation outcomes for AFO users.
Footnotes
Acknowledgements
The authors acknowledge Andrea Ikeda, CP, for her contributions with device alignment and Jennifer Aldridge Whitehead, Derek Haight, Starr Brown, Paige Lane, Harmony Choi, and Dr Christopher Rábago for assistance with data collection and processing. Support for this study was provided by the Center for Rehabilitation Sciences Research, Department of Physical Medicine and Rehabilitation, Uniformed Services University of Health Sciences, Bethesda, MD. The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, Department of Defense or the U.S. Government.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K.A.S., E.R.E., and J.M.W. certify that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Ethical review
This study has been approved by the Brooke Army Medical Center Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by the Center for Rehabilitation Sciences Research, Department of Physical Medicine and Rehabilitation, Uniformed Services University of Health Sciences, Bethesda, MD.
Location
The experimental data collection and analysis were performed at the Center for the Intrepid at Brooke Army Medical Center, JBSA Ft. Sam Houston, TX 78234.