
Abstract
Background:
Maintaining an optimal rolling of the foot over the ground is thought to increase the stability and efficiency of pathologic gait. Ankle-foot orthoses are often prescribed to improve gait mechanics in individuals with lower extremity injuries; however, their design may compromise how the foot rolls over the ground.
Objectives:
The aim of this study was to investigate the effects of the sagittal plane ankle-foot orthosis alignment on roll-over shape and center of pressure velocity in individuals with lower limb reconstructions.
Study design:
Randomized cross-over study with a control group comparison.
Methods:
In total, 12 individuals with lower limb reconstruction who used a custom carbon ankle-foot orthosis and 12 uninjured controls underwent gait analysis. Ankle-foot orthosis users were tested in their clinically-provided ankle-foot orthosis alignment, with an alignment that was 3° more plantarflexed, and with an alignment that was 3° more dorsiflexed. Components of roll-over shape and center of pressure velocity were calculated from heel strike on the ankle-foot orthosis limb to contralateral heel strike.
Results:
Roll-over shape radius was not affected by 3° changes to alignment and was not significantly different from controls. Aligning the ankle-foot orthosis in more dorsiflexion than clinically provided resulted in a smaller peak center of pressure velocity that occurred later in stance.
Conclusion:
Individuals using custom carbon ankle-foot orthoses can accommodate 3° alterations in the dorsiflexion or plantarflexion alignment.
Background
The foot-ankle system has been described as functioning like a wheel 1 that rolls over three sequential rockers: first the heel, then the ankle, and finally the forefoot. 2 The integrated effects of these three rockers during single limb support represent the ankle-foot roll-over shape (ROS). 3 ROS is calculated using the path of the center of pressure (COP) under the foot relative to a fixed lower leg coordinate system. 4 Some of the original purposes of evaluating ROS were to characterize different prosthetic feet, 5 to understand the reasoning behind clinical fitting decisions, and to guide the design and alignment of device components.3,4,6,7 In addition to providing an additional means for objectively characterizing limb motion and loading, ROS-related parameters can provide mechanistic insight into how and why device design changes alter limb function.8–10 By investigating human movement using ROS, we can determine situations, conditions, or alignments that best emulate normative motion and loading.10,11
One variable that can help quantify how the foot rolls over the ground is the velocity of the center of pressure (vCOP). 12 Within the context of ROS, vCOP can increase by one of the two methods. First, a more rapid forward progression of the tibia results in a more rapid progression of the COP anteriorly toward the end of the foot. Second, a flatter region on the ROS path can result in a more rapid COP progression anteriorly under the foot at the same rate of tibial progression due to a more abrupt transition from heel to forefoot loading. Therefore, vCOP is a measure that has been used to evaluate the “dead spot” phenomenon perceived by patients in the clinical fitting of prosthetic feet. 13 The “dead spot” is where forward progression is disrupted and vCOP rapidly decreases. 13 However, it is important to note that vCOP is not constant throughout stance phase and has a characteristic triple peak pattern during (1) loading response, between 0%–20% of stance phase, (2) early, mid-stance, about 35% of stance phase, and (3) late stance/push-off, at about 92% of stance phase. 12 vCOP has been used in a variety of applications to evaluate the effects of design modifications in ankle-foot orthoses (AFOs). 8
AFOs are often prescribed to restore some lost ankle function, provide support to limbs, and facilitate energy storage and return.14–16 The literature characterizing the ROS with AFOs is limited to only a few human subject studies. Fatone and Hansen 9 found that thermoplastic articulated AFOs improved ROS in stroke patients such that those ROS radii were not significantly different from unaffected controls. For individuals with a variety of lower limb impairments (e.g. stroke, nerve injury, etc.), AFOs improved (increased) the radius of curvature compared to walking without an AFO, but deficiencies still remained, relative to controls. 17 Custom carbon AFOs that offer energy-storing-and-returning properties are now often used for patients with lower limb reconstruction.18,19 Ikeda et al. 8 found that altering the height and durometer of heel wedges used with these custom carbon AFOs significantly altered the ROS and vCOP properties. The altered limb loading may be due to the effect of the wedges and durometers on alignment, and evaluating the effect of alignment changes on of ROS may help interpret those findings.
Aligning an AFO to mimic the COP characteristics of an intact limb appears desirable, but information regarding the importance of alignment on factors influencing ROS remains limited. To the best of our knowledge, it is currently unknown how AFO alignment affects COP characteristics during walking in individuals with lower limb trauma and if the ROS and/or vCOP are affected by changes in alignment. Knowing this information may better help orthotists align an AFO for a given individual. Therefore, the purpose of this study was to determine how the sagittal plane AFO alignment influences the characteristics of ROS and vCOP during walking. A secondary aim was to compare ROS and vCOP between AFO users and uninjured subjects. We hypothesized that the clinically-provided (CP) AFO alignment would achieve ROS characteristics more similar to uninjured individuals than a more dorsiflexed or plantarflexed alignment.
Methods
Inclusion criteria consisted of age 18–50 years, lower limb injury requiring surgical reconstruction procedures, clinically documented plantar flexion weakness and use of a custom carbon fiber AFO (Intrepid Dynamic Exoskeletal Orthosis—IDEO, Figure 1), walking and resting pain less than 4/10, and ability to comply with study procedures. Subjects were excluded if they had moderate or severe traumatic brain injury. The IDEO is a passive-dynamic AFO with a rigid footplate and a tibial cuff which are connected by an energy-storing-and-returning posterior strut. More information on the device can be found in prior publications.18–20 An overview of the surgical management of this patient population is described by Shawen et al., 21 and the rehabilitation program completed by the subjects is described by Owens et al. 22 This study was approved by the Brooke Army Medical Center IRB, and all subjects read and signed informed consent forms.

Intrepid Dynamic Exoskeletal Orthosis (IDEO) alignment was modified to achieve a more dorsiflexed (left) or plantarflexed (right) position relative to the CP alignment using a 3° wedge attached to the posterior strut.
Subject characteristics.
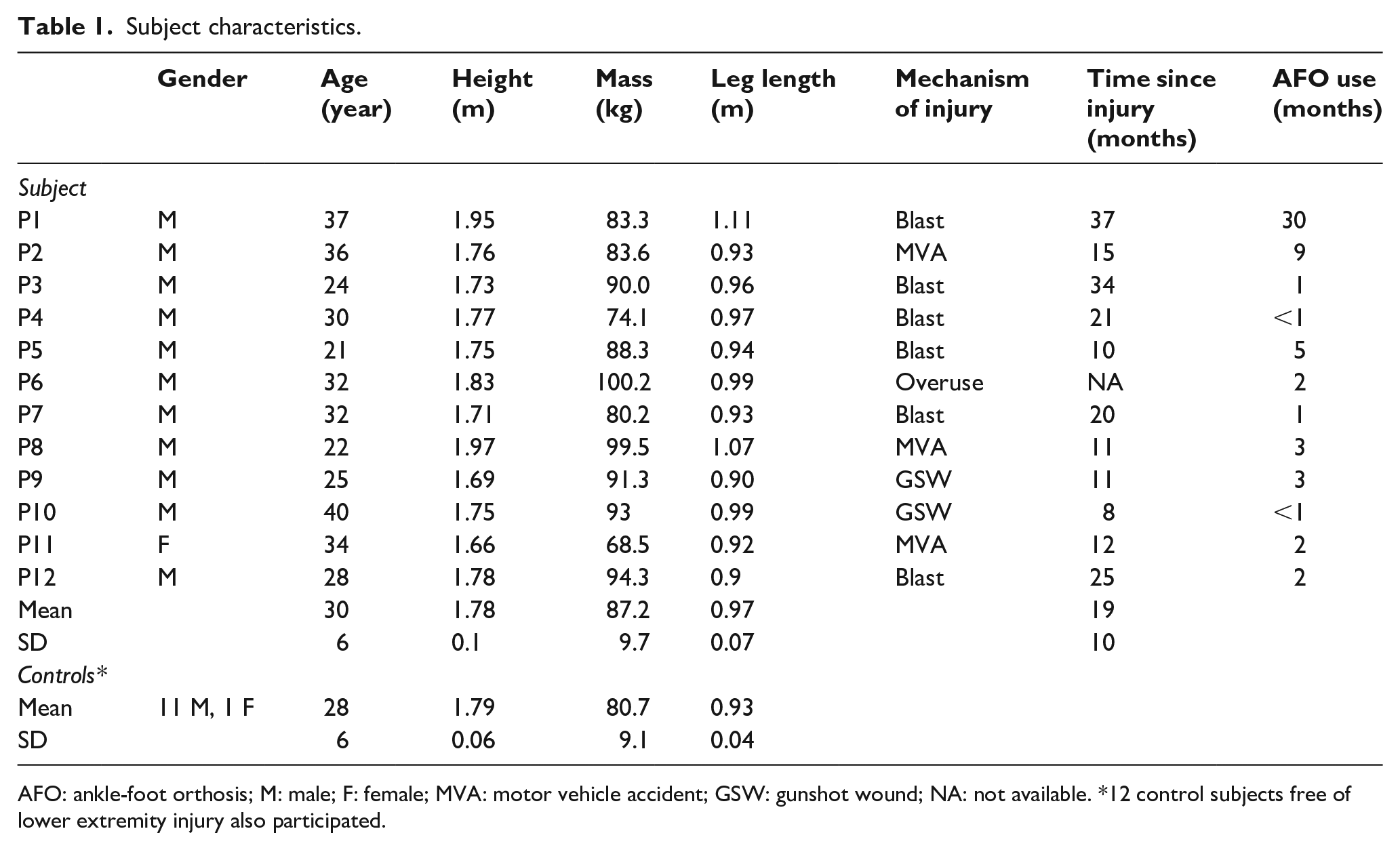
AFO: ankle-foot orthosis; M: male; F: female; MVA: motor vehicle accident; GSW: gunshot wound; NA: not available. *12 control subjects free of lower extremity injury also participated.
The initial AFO alignment for each subject had been established by his or her orthotist as part of standard clinical care, and hereafter is referred to as the CP alignment. This alignment was subject-specific and took into account the subject’s available and pain-free range of motion. Changes to the sagittal plane alignment were made relative to the CP position by inserting a small wedge at the distal portion of the strut interface with the footplate to allow for 3° changes in more dorsiflexion (DF) or plantarflexion (PF) from the CP setting, depending on how the wedge was positioned (Figure 1). The 3° alignment change was chosen because it represents the largest adjustment typically made during the clinical fitting of the IDEO. At least 10 min wear time was given prior to testing in each alignment condition. The control group did not wear AFOs.
Marker trajectory data were captured with 26 motion capture cameras (120 Hz, Cortex, Motion Analysis Corp., Santa Rosa, CA). Subject motion was tracked using 57 reflective markers according to the procedures described by Wilken et al. 23 Kinetic data were captured using a series of five centrally located force platforms in tandem (1200 Hz, AMTI, Inc., Watertown, MA).
AFO users and able-bodied control subjects visited the laboratory for a single session. Each subject performed over ground walking trials while kinematic and kinetic data were recorded. Subjects walked at a standardized speed based on leg length and a Froude number of 0.16. 24 In this cross-over study design, three alignment conditions (CP, PF, and DF) were tested in a randomized order and subjects were not informed of which alignment condition they wore. Five strides in which the affected limb (AFO users) and right limb (control group) made full contact with the force platform were collected. After the completion of the walking trials, subjects ranked their preference for the three AFO alignment conditions.
Kinematic data were first processed using Cortex 3.3 (Motion Analysis, Santa Rosa, CA), then exported to Visual3D (C-Motion, Inc, Germantown, MD) for further processing. The kinematic data were interpolated using a cubic spline and filtered using a fourth-order Butterworth low-pass filter with 6 Hz cutoff frequency; kinetic data were filtered using a 50 Hz cutoff frequency. Temporo-spatial variables were calculated across the gait cycle.
The COP trajectory in the lower leg coordinate system 25 was calculated in Visual3D from ipsilateral heel strike through contralateral heel strike 3 and then exported to a custom MATLAB program (The MathWorks, Inc., Natick, MA). Data were cropped to include only forward progression of the ROS curve, defined as a positive horizontal displacement in the direction of motion. Cropping was performed to remove variable COP estimates associated with low loads immediately following initial contact. 3 The ROS radius of curvature and the anterior–posterior position of its center were determined by fitting a best-fit circular arc to the transformed COP data. 26 The circle fitting algorithm failed for three subjects whose data did not follow an arc shape, and their data were excluded from the ROS analysis. The vCOP was calculated by taking the first derivative of the COP position data, and the peak value was identified within 5%–85% of stance phase.
Normality was assessed using a Shapiro–Wilk test (SPSS, IBM Corporation, Armonk, NY). Non-normally distributed data were transformed using a logarithmic base 10 transformation and re-tested for normality. A repeated measures analysis of variance (ANOVA) determined a significant effect of alignment within the AFO user group. Significant main effects were separated with post hoc paired t-tests with sequentially rejective Bonferroni–Holm corrections to identify significant differences among alignments. A univariate ANOVA determined significant main effects between AFO user and control data, and a Dunnett’s post hoc test separated significant main effects. Significance was set at p < 0.05.
Results
In total, 12 Service members with severe unilateral lower limb injuries and 12 Service members free of injury (control group) participated in and completed this study (Table 1). There were no significant differences between groups for age, height, and mass (p > 0.05). Functional deficits in the AFO user group resulted from fractures of the tibia, fibula, calcaneus, talus, ankle fusion, osteomyelitis, and/or neuropathy. Time of IDEO use is included in Table 1. The average standing alignment of the shank segment was 10.4 (3.8)° from vertical. The data from all 12 participants in each group were analyzed. Table 2 presents mean (standard deviation) results. There was no significant main effect of AFO alignment on ROS radius (Figure 2). Radius values were also not significantly different between AFO users in any alignment condition compared to uninjured controls. However, there was a significant main effect of AFO alignment on ROS position such that ROS center of curvature (Figure 3) was shifted more posteriorly in the DF alignment compared to the PF and CP alignments (p < 0.001). The between-group analysis indicated that the position of the center of the ROS radius was not significantly different from uninjured controls with the PF or CP alignments.
Dependent measures presented as mean (standard deviation).
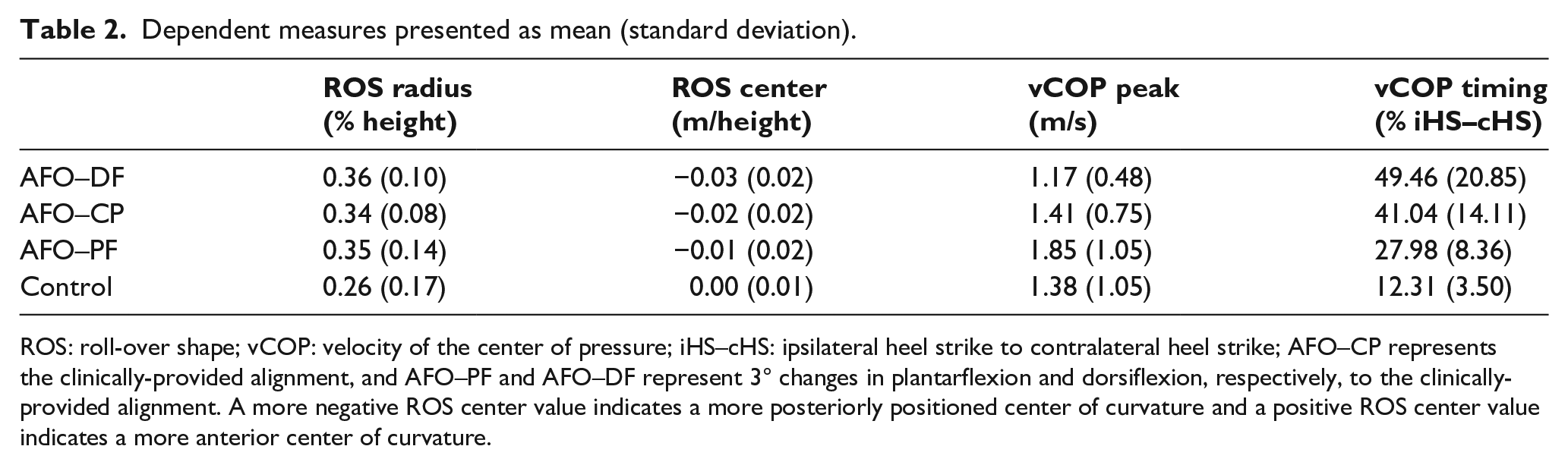
ROS: roll-over shape; vCOP: velocity of the center of pressure; iHS–cHS: ipsilateral heel strike to contralateral heel strike; AFO–CP represents the clinically-provided alignment, and AFO–PF and AFO–DF represent 3° changes in plantarflexion and dorsiflexion, respectively, to the clinically-provided alignment. A more negative ROS center value indicates a more posteriorly positioned center of curvature and a positive ROS center value indicates a more anterior center of curvature.
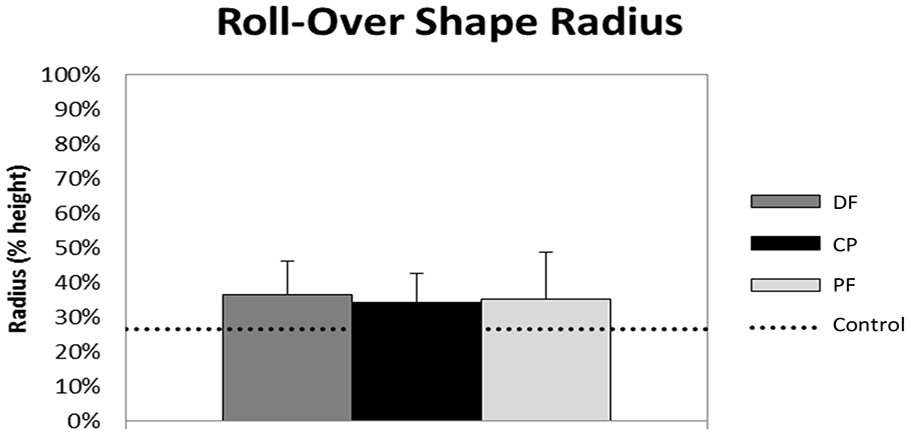
Mean and standard deviation of the roll-over shape (ROS) radius of curvature.
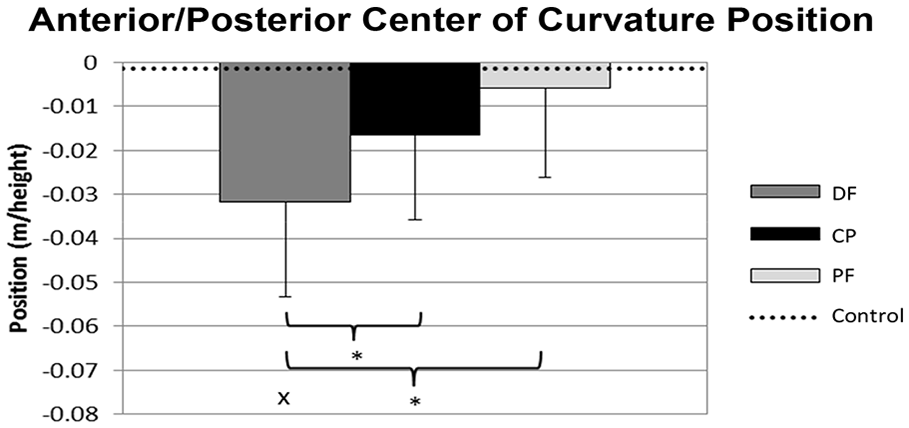
Mean and standard deviation of the roll-over shape (ROS) anterior/posterior center of curvature position. A more negative value indicates a more posteriorly positioned center of curvature.
vCOP and timing of the peak were not normally distributed, and log transforms were applied. There was a significant main effect of AFO alignment such that the peak vCOP was significantly greater in the PF alignment than in the CP (p = 0.004) and DF (p = 0.002) alignments (Figures 4 and 5). In the PF alignment, the peak vCOP occurred significantly earlier than in the CP (p < 0.001) and DF (p = 0.002) alignments and the CP alignment’s peak vCOP occurred significantly earlier than the DF alignment (p = 0.013). The between-group analysis indicated that across all alignments, the timing of the vCOP peaks (Figure 5) occurred significantly later in stance than the controls (p ⩽ 0.002).
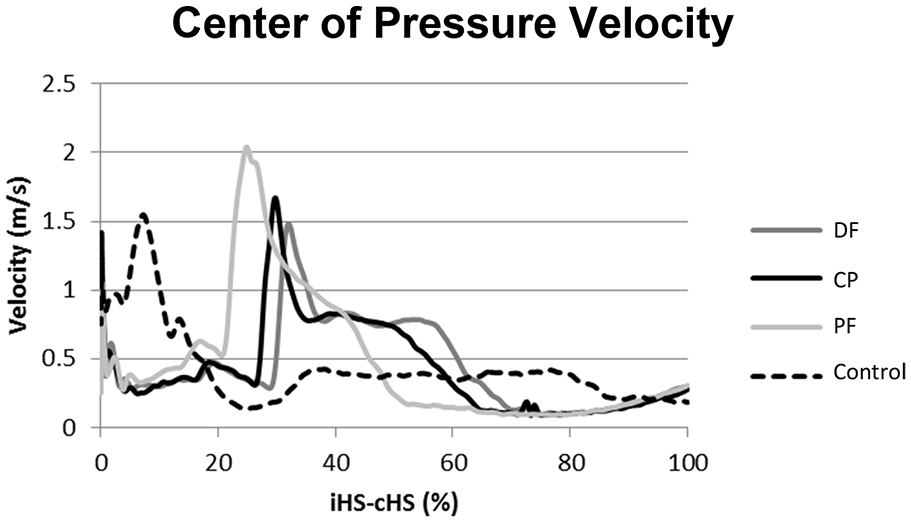
Plot of the velocity of the center of pressure (vCOP) for representative subject and control.
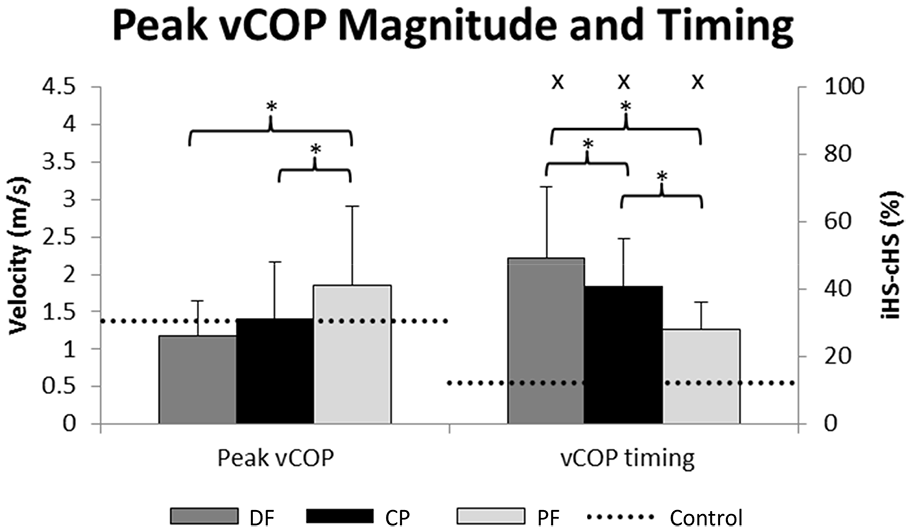
Mean and standard deviation of the velocity of the center of pressure (vCOP) peak magnitudes (left) and timing (right) for the affected limb.
There were no significant differences in walking speed between groups. Anecdotally, all patients could perceive a difference when alignment was changed. When ranking preference, 8/12 subjects preferred the PF alignment over the DF and CP alignments.
Discussion
This biomechanical study examined how 3° changes in the sagittal plane alignment of an IDEO-AFO affected the characteristics of ROS and vCOP during walking. There currently exists no standard as to how to align custom carbon AFOs, and different orthotists may employ different techniques due to training, experience, and trial and error. This study provides information on how changes in alignment, relative to the initial alignment selected by the clinician, affect how the foot rolls over the ground and the body progresses over its base of support. Based on these findings, clinicians can alter alignments to best-fit individuals’ needs.
Based on our results, changing alignment in a relatively stiff AFO like the IDEO significantly altered the ROS center of curvature position. The DF-aligned IDEO had a more posterior center of curvature than more plantarflexed alignments. The nearly rigid foot plate, constructed from greater than 3 mm of carbon fiber thickness and with high trimlines, limits deflection. Without foot plate deflection, the ROS attributed to the forefoot rocker would be flattened with a more PF alignment. Lowering the forefoot into a more PF position moves the nadir of the best-fit circle anteriorly, also moving the center of curvature anteriorly. With a more PF alignment, the COP moves anteriorly earlier and more rapidly, and with an excessively plantarflexed alignment, an AFO user may perceive greater difficulty progressing over the foot, similar to walking uphill. In contrast, a more DF alignment results in persistent loading of the heel with a slower progression to forefoot loading as seen here. Preference and biomechanical data from this study suggest that the CP alignment was excessively dorsiflexed, resulting in the PF condition providing more normal limb mechanics and being rated as most preferred.
Knowledge of how alignment changes affect the ROS center of curvature can be utilized by clinicians in this way to enhance smooth roll-over throughout stance. Although a trend was observed across the three conditions with more DF resulting in a more posterior center of rotation, the DF alignment was the only alignment with the center of curvature significantly more posterior than the control data. Consistent with the results presented here, Hansen’s 6 testing of prosthetic foot alignment revealed that the relative position of the center of curvature shifted forward as the foot was aligned in more PF. Unlike the AFOs tested here, which have a nearly rigid foot plate and demonstrated no change in ROS radius with altered alignment, the distal aspect of carbon fiber prosthetic feet is designed to deflect when loaded. As a result, Hansen et al.’s findings that a more PF prosthetic foot resulted in a smaller radius of curvature are likely due to greater deflection of the foot, resulting from earlier toe loading.
Changing AFO alignment significantly altered the relative timing and magnitude of the peak vCOP. The altered magnitude and timing of vCOP is intuitive, given the limited displacement provided by relatively stiff AFOs like the IDEO and a limited ability to alter tibial orientation during gait. A more PF position resulted in less time spent on the heel, with the relatively lower forefoot position, resulting in earlier and more rapid forefoot loading and a corresponding forward motion of the COP. These results are consistent with prior research where different height and durometer wedges used under the heel of the IDEO effectively created a more DF or more PF positioning, and thus altered vCOP timing. 8 The vCOP magnitude was not significantly different from controls, but the timing was significantly later in stance. Although many potential explanations are possible for these contrasting findings, it is likely that clinical providers first seek to avoid an abrupt transition from heel to forefoot loading associated with a large vCOP magnitude. In contrast, the IDEO’s reliance on a heel cushion rather than actual ankle motion to attenuate impact and lower the forefoot to the floor during loading response results in delayed forefoot loading and a difference from controls. Delayed forefoot loading in the IDEO results in both a prolonged ankle DF moment and significantly delayed vCOP peak.8,27
The vCOP and ROS center of curvature positions can provide insight into further changes the AFO alignment has on the knee kinematics and kinetics and electromyographic (EMG) activity of the lower limb. The DF alignment had a significantly more posterior ROS center of curvature than the other alignments and the control data. Additionally, the DF alignment had the lowest vCOP peak of the 3° alignments and occurred significantly later than the other alignments and the control data. This indicates that the ground reaction force vector stays more posterior on the foot during early stance. In a more DF AFO alignment, a delayed timing of the peak vCOP and posteriorly-positioned center of the radius of curvature are associated with a later transition to a PF moment, as has been shown experimentally. 27 This DF alignment thus provides less control of tibial forward progression, requiring greater activation of quadriceps muscles and a greater internal knee extensor moment. 27 Conversely, the higher peak vCOP and earlier timing in the PF alignment indicate a rapid transition of the COP under the foot. With this rapid transition, it would be expected that the ground reaction force vector would transition forward more quickly in the PF alignment than the CP and DF alignments. This has been shown experimentally to result in a more rapid transition from an ankle DF moment to a PF moment and decreased quadriceps activity. 27 Clinicians can utilize these findings to effectively control the vCOP with sagittal plane AFO alignment changes and to meet the unique needs of individual patients. For example, those with quadriceps weakness may require a more PF alignment to move the COP anterior earlier in stance for improved knee stability. This finding may have also contributed to 8/12 participants preferring the PF alignment.
The 3° changes in alignment did not significantly alter the radius of curvature of the ROS on the affected limb. A ROS similar to a healthy, able-bodied individual is thought to positively influence the stability and efficiency of pathological gait. 9 However, a number of other components are also important for stability and efficiency other than ROS. Mitchell et al. 28 and Hansen et al. 26 researched a link between ROS radii and metabolic rate. Both authors found ideal ROS radii in their subject populations based on their height that incurred the least metabolic cost. Although our study did not look to optimize metabolic rate, the control participants in this study had a ROS radii of 27% body height, while the affected limb ranged from 34% to 36% of body height. No significant differences were detected between AFO user and control data. Therefore, if the controls were walking at optimal metabolic ROS radii, it can be inferred that the AFO users were also walking at optimal ROS radii throughout the changes to the alignment of the AFO.
The primary limitation of this study is the inability to standardize alignment across AFO users or provide an “optimal” custom carbon AFO alignment to the clinical and scientific community. Providing a single alignment that should be used across individuals of varying pathologies may be viewed inappropriate for some individuals and would not have been feasible for many of the individuals enrolled in this study, who were a varied cohort in terms of initial injury and surgical procedures. Alignment is a component of many factors including a pain-free position that is patient-specific. An additional, and necessary, limitation of this study is the lack of a no-AFO condition for comparison purposes, which would identify the acute effects of the AFO on the rocker shape profile. However, many of the study participants could not tolerate the data collection protocol without the use of their AFO and, therefore, this condition was intentionally not tested.
Future work on individuals with pain-free ranges of motion could establish optimal alignment characteristics of dynamic AFOs. Although this study sought to determine if small changes in AFO alignment would yield significant biomechanical differences during walking, not to identify a single alignment that would be universally appropriate, standardized guidelines of how to optimally align dynamic AFOs would be a useful reference for this field.
Conclusion
Individuals using custom carbon AFOs can accommodate to 3° alterations in the DF or PF alignment such that ROS radius is not affected and is not significantly different from uninjured individuals not using AFOs. An alignment that is shifted more DF than CP has a smaller peak vCOP and a later timing, which when combined with the more posterior center of curvature indicates a later transition of weight-bearing forces. The PF alignment has a greater peak vCOP with an earlier timing and more anterior center of curvature, indicating a more rapid transition of weight-bearing forces. The changes seen in this study indicate that a custom carbon fiber AFO as aligned by clinicians has a small (6°) alignment range that subjects can tolerate without altering the ROS radius, giving clinicians a range of positions to work with to meet a person’s specific needs.
Footnotes
Authors’ Note
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army, the Department of the Air Force, or the Department of Defense or the US Government.
Author Contributions
ERE, MDR, AJI and JW - conceptualization, formal analysis, methodology, writing - review and editing.
MDR and ERE - investigation
JMW - funding acquisition
Declaration of Conflicting Interests
The author(s) disclosed no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by the Center for Rehabilitation Sciences Research, Department of Physical Medicine and Rehabilitation, and Uniformed Services University of Health Sciences, Bethesda, MD.