
Abstract
Background:
An inverted pendulum model represents the mechanical function of able-bodied individuals walking accurately, with centre of mass height and forward velocity data plotting as sinusoidal curves, 180° out of phase.
Objectives:
This study investigated whether the inverted pendulum model represented level gait in individuals with a unilateral transfemoral amputation.
Study Design:
Controlled trial.
Methods:
Kinematic and kinetic data from 10 individuals with unilateral transfemoral amputation and 15 able-bodied participants were recorded during level walking.
Results:
During level walking, the inverted pendulum model described able-bodied gait well throughout the gait cycle, with median relative time shifts between centre of mass height and velocity maxima and minima between 1.2% and 1.8% of gait cycle. In the group with unilateral transfemoral amputation, the relative time shift was significantly increased during the prosthetic-limb initial double-limb support phase by 6.3%.
Conclusion:
The gait of individuals with unilateral transfemoral amputation shows deviation from a synchronous inverted pendulum model during prosthetic-limb stance. The reported divergence may help explain such individuals’ increased metabolic cost of gait. Temporal divergence of inverted pendulum behaviour could potentially be utilised as a tool to assess the efficacy of prosthetic device prescription.
Clinical relevance
The size of the relative time shifts between centre of mass height and velocity maxima and minima could potentially be used as a tool to quantify the efficacy of innovative prosthetic device design features aimed at reducing the metabolic cost of walking and improving gait efficiency in individuals with amputation.
Background
Researchers have previously used an inverted pendulum model to represent the mechanical functioning of normal, bipedal overground walking.1–5 The inverted pendulum model is, by intention, simplistic. It represents each of the lower limbs as a single rigid segment, capable of rotation about the ankle during stance, with the whole-body centre of mass (CoM) located at its superior end. This model sits comfortably with the mechanical reality of walking, as the vertical trajectory of the CoM and its forward velocity vary during the gait cycle in a similar manner to that of the bob of an oscillating pendulum. The CoM is higher and slower during single-limb support (SS) and lower and faster during double-limb support (DS). When plotted graphically, CoM height and CoM forward velocity appear as sinusoidal curves, 180° out of phase, with CoM peak forward velocity coinciding with the lowest CoM height and CoM minimum forward velocity coinciding with maximum CoM height.
Individuals with a unilateral lower-limb amputation are mechanically constrained during walking by the prosthetic device used. 6 As a result, they, for example, walk more slowly, 7 fall more often 8 and have a higher metabolic cost of walking9–11 when compared to able-bodied (AB) individuals. Multiple issues may affect the gait pattern of any given population of individuals with lower-limb amputation, such as the ability of the prosthetic ankle and/or knee joint to allow flexion during stance. It is not well understood if the mechanical constraints imposed by prosthetic devices mean a mechanical model of walking could be applicable to individuals with a lower-limb amputation. It has been demonstrated not to be the case in individuals with a unilateral transtibial (UTT) amputation, where peak CoM forward velocity and minimum CoM height did not coincide during prosthetic-limb initial DS. 12 In such individuals, the CoM accelerates forward to peak velocity after the minimum CoM height occurs, therefore, while the CoM is being elevated.
Specific gait characteristics have been reported for individuals with unilateral transfemoral (UTF) amputation. For example, those with UTF are likely to retain a more vertical projection of the CoM at prosthetic-limb toe-off 13 and commonly use a vaulting mechanism, for example, via increased plantar flexion, during the intact-limb stance phase. This vaulting strategy supports the elevation of the CoM and hence allows for sufficient prosthetic-limb toe clearance during swing. 14 Also, during the prosthetic-limb stance phase, prosthetic knee flexion is restricted in order to prevent the prosthetic knee from unlocking and collapsing during weight bearing. 15 Both aspects could affect the efficacy of applying the inverted pendulum model to UTF gait, as the model does not include varying pendulum lengths (as induced by the vaulting mechanism) and restrained knee flexion. In addition, the mechanical constraint to rotate around the flexion/extension axis of the ankle might affect the synchrony of the inverted pendulum model. To date, the possibilities of applying the inverted pendulum model to the gait of individuals with an UTF has not been established, and it remains unclear to what extent their specific gait characteristics influence the efficacy of applying this model. Given the importance of step-to-step transitions in determining the metabolic cost of walking5,11 and that disruptions of energy transformations associated with the inverted pendulum mechanism can lead to increased energy expenditure, 16 any breakdown of compliance with the inverted pendulum model may partially explain the higher metabolic cost of walking for those with a lower-limb amputation as demonstrated by Houdijk et al. 11 for individuals with UTT.
Therefore, the objective of this study was to investigate whether the level ground gait of individuals with UTF is represented by an inverted pendulum model. It was hypothesised that the model would, during intact-limb stance, perform similar for individuals with UTF compared to AB individuals, but different during prosthetic-limb stance.
Methods
Study design
As study design, a controlled trial was chosen, comparing AB individuals with individuals with an UTF amputation.
Participants
The UTF group consisted of 10 participants, all using the same prosthetic foot (Esprit; Chas. A. Blatchford & Sons, Basingstoke, UK). Data from eight (mean (standard deviation (SD)) age: 42 (14.8) years, mass: 86.3 (15.3) kg, height: 1.74 (0.06) m.) walking over level ground, previously published by De Asha et al., 12 were re-analysed. Data from two further individuals with UTF (mean (SD) age: 53 (2.8) years, mass: 74.1 (14.9) kg, height: 1.81 (0.11) m) and 15 AB male individuals (mean (SD) age: 27 (5) years, mass: 75.1 (9.1) kg, height: 1.81 (0.05) m) were collected at the University of Salzburg. All UTF participants had undergone amputation at least 2 years prior to participation, were free from neurological, musculoskeletal (other than limb amputation) or cardiovascular disorders, and had used their current prostheses for at least 6 months. All were classed as being at least K3 on the Medicare scale by their prescribing clinician, and all used their habitual knee component (1× Orion, 1× EUK SAKL, 2× KX06: all Chas A Blatchford & Sons, Basingstoke; 1× C-leg, 1× 3R45: both Otto Bock, Duderstadt, Germany; and 3× Total Knee: Ossur, Reykjavik, Iceland). Institutional bioethics committee approval was obtained at both locations, and written informed consent was provided by all participants prior to data collection.
Data acquisition
In addition to the data from De Asha et al., 12 kinematic and kinetic data were collected at 250 Hz and 1000 Hz, respectively using an eight camera motion capture system (Vicon, Oxford, UK) and two force plates (AMTI, Watertown, MA, USA). Participants walked at their self-selected walking speed on an 8-m (8 TF, 12) and 6-m (2 TF all AB, Salzburg) walkway with the two force platforms embedded in the middle of the walkways.
Reflective markers were attached to participants according to the Cleveland Clinic Marker Set (Motion Analysis Corp, Santa Rosa, USA), which uses an anatomical landmark calibration technique. 17 Markers on the prosthetic knee were placed medially and laterally of the rotational or approximated (for polycentric knee components) joint centre. At the prosthetic ankle and foot, the markers were placed to correspond with those on the intact side. For all UTF participants the mean of six trials at self-selected walking speed were analysed, while for the AB group one representative trial was analysed for each participant.
Data processing
Labelling of marker trajectories was undertaken in Workstation and Nexus software (Vicon) before all data were exported to Visual3D (C-Motion, Germantown, USA) from which point on the processing was identical for all participants. Kinematic and kinetic data were filtered using a fourth-order, zero-lag Butterworth filter with a 6 Hz cut-off. A nine-segment model (head, trunk, pelvis, thighs, shanks and feet) of each participant was constructed. Initial contact (IC) and toe off (TO) were defined as the instants the vertical component of the ground reaction force first went above or below 20 N, respectively. The gait cycle was defined from IC of the prosthetic (UTF) or right (AB) limb to the consecutive IC of the ipsilateral limb and normalised to 100%. In instances where no kinetic data were available (i.e. a missed or incomplete force platform contact), IC and TO were defined using kinematic data.18,19 From these events, phases of SS and DS were defined. The position of the whole-model CoM was calculated as the weighted average of the model’s segmental CoMs.20–22 Forward velocity of the CoM was defined as the first derivation of the CoM position in the walking direction, which was in line with the global coordinate system of the respective laboratory. The height of the CoM was defined as the instantaneous vertical distance between the CoM and the walking surface. For the UTF group timings, normalised to the gait cycle, of the minimum and maximum CoM height and forward velocity were identified in the following four phases: (1) prosthetic initial double-support (IDS_P); (2) prosthetic single-support (SS_P); (3) prosthetic terminal double-support (TDS_P); (4) intact single-support (SS_I) (Figure 1). For the AB group, these timings were identical, only the analysed gait cycle started with the right foot always, resulting in prosthetic phases corresponding to the right side and SS_I corresponding to the left side (Figure 1).
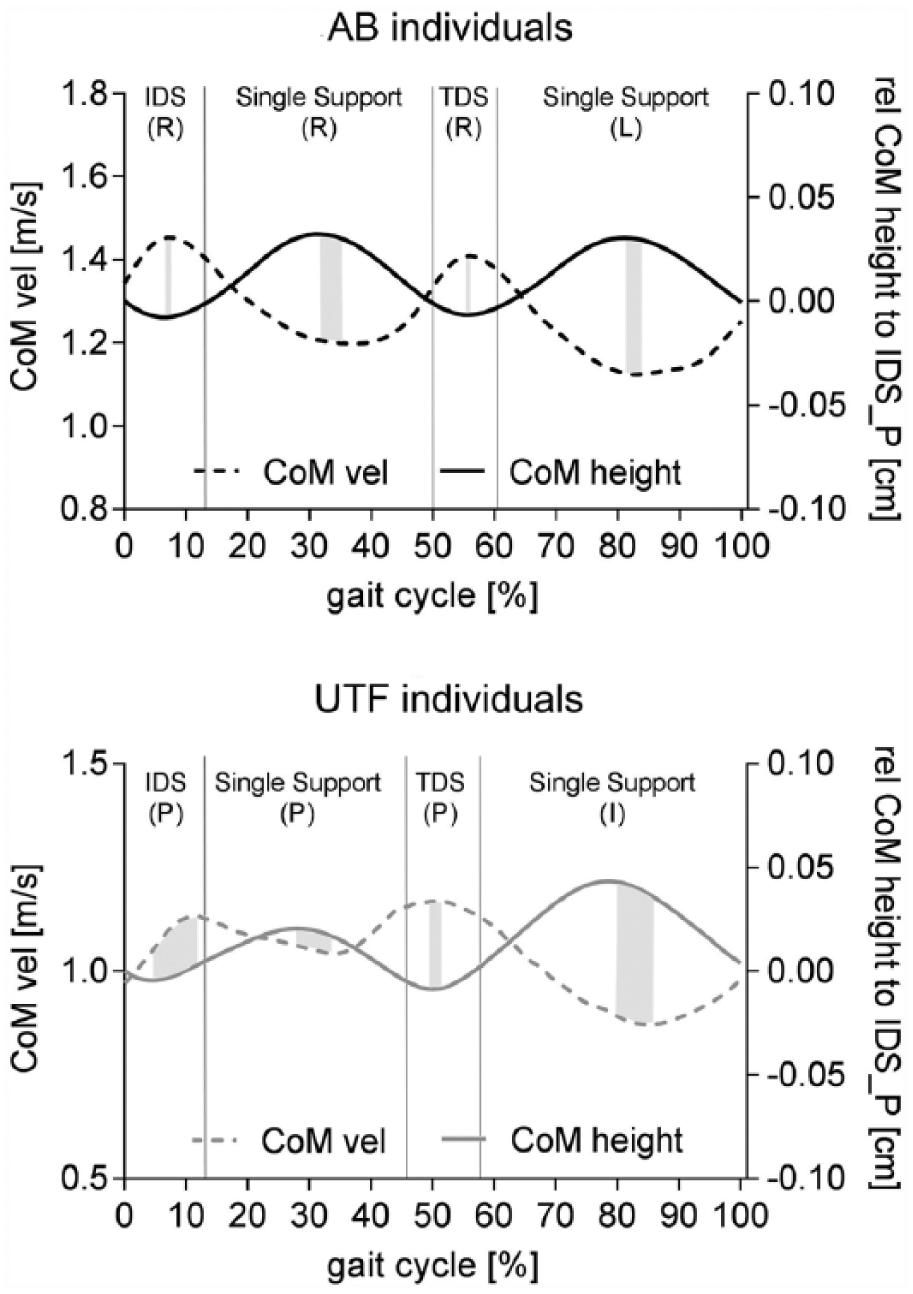
Mean forward CoM velocity (dotted lines) and CoM height relative to the CoM position at initial contact (solid lines) for all AB (black lines) and UTF (grey lines) participants throughout a normalised gait cycle during level walking. Initial and terminal double-limb support (IDS, TDS) and single-limb support (SS) phases are indicated by solid vertical lines, the relative time shift between maximum and minimum positions is shown as shaded areas.
For each phase, the relative time shift was calculated as the time difference between the maxima and minima of CoM vertical position and forward velocity normalised to gait cycle duration. Assuming inter-limb symmetry in the AB group, the mean of both, left and right, limbs were calculated for the metric values. In case of perfect compliance with the inverted pendulum, a time shift of zero would be observed with increasing time shift magnitude indicating reduced adherence to the inverted pendulum model.
Statistical analysis
Statistical testing was performed using SPSS software (version 23, IBM, Armonk, NY, USA). UTF data were not normally distributed, thus a non-parametric statistical approach was adopted for all participants.
The data first was analysed to detect main effect of groups (UTF and AB) using a Friedman analysis of variances by ranks. A second Friedman analysis of variances by ranks was used to detect the main effect of phases (IDS_P, SS_P, TDS_P, SS_I). Post hoc tests were conducted, where significant main effects were identified using (1) for each phase the Mann–Whitney U-test to detect differences between groups (AB vs UTF) and (2) for each group the Wilcoxon signed-rank test to detect differences between the phases). For all statistical tests an alpha level of 5% (p < 0.05) was set. Post hoc test were conducted using a Bonferroni-corrected alpha of p = 0.008 for phase comparisons and p = 0.013 for group comparisons. Effect sizes were calculated as r with the boundaries of 0.1, 0.3 and 0.5 for small, medium and large. 23
Results
During level walking, there were significant effects of group (p = 0.004), gait cycle phase (p < 0.001) and a group by phase interaction (p < 0.001) on the relative timings of CoM height and velocity maxima and minima. Between gait phases, the AB group did not show significant differences in time shifts between CoM maxima and minima of height and forwards velocity, with median relative time shifts ranging between 1.2% and 1.8% of gait cycle duration (p > 0.087, Figures 1 and 2). For the UTF group, the median relative time shift was significantly increased during IDS_P phases compared to the TDS_P (p = 0.005, r = 0.89) and SS_I phase (p = 0.005, r = 0.89; Figure 1). Post hoc analysis of differences between the UTF and the AB group indicated the difference was only significant during the IDS_P phase, when the UTF group displayed increased relative time shifts compared to the AB group (IDS_P, p < 0.001, r = 0.79), indicating that maximum CoM velocity occurred after minimum CoM height. In the TDS_P DS phase, the maximum CoM velocity was almost synchronous with minimum CoM height (Table 1, Figure 2).
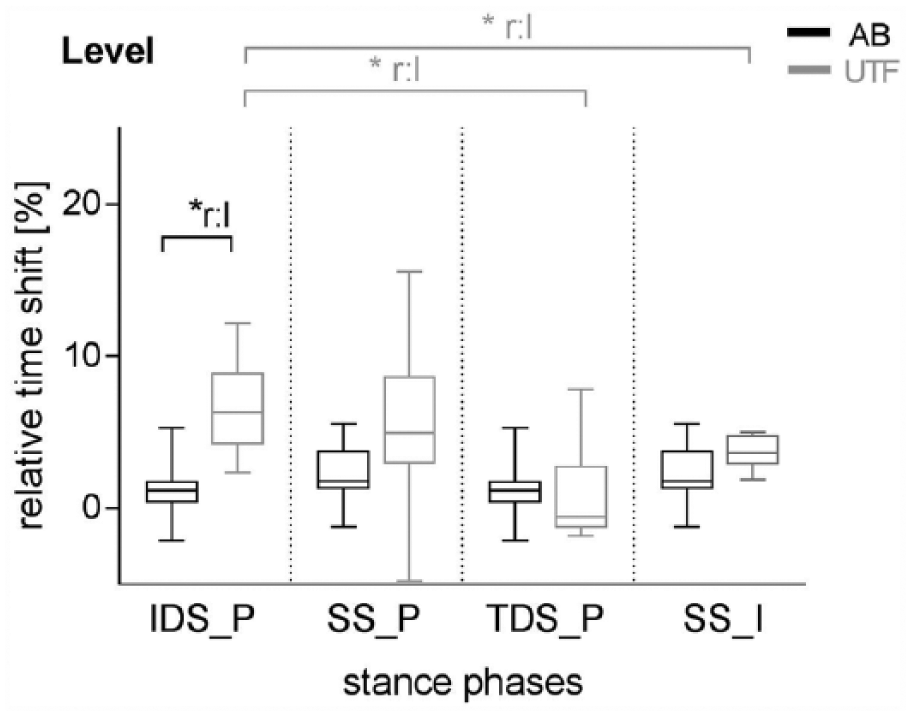
Boxplots of relative time shift between extreme values of CoM height and CoM forward velocity in the initial and terminal double-limb support (IDS_P and TDS_P) and single-limb support (SS_P and SS_I) phase of level gait.
Median (IQR) of relative time shift of unilateral transfemoral (UTF) and able-bodied (AB) participants during initial and terminal double and single-limb support phases in level gait.
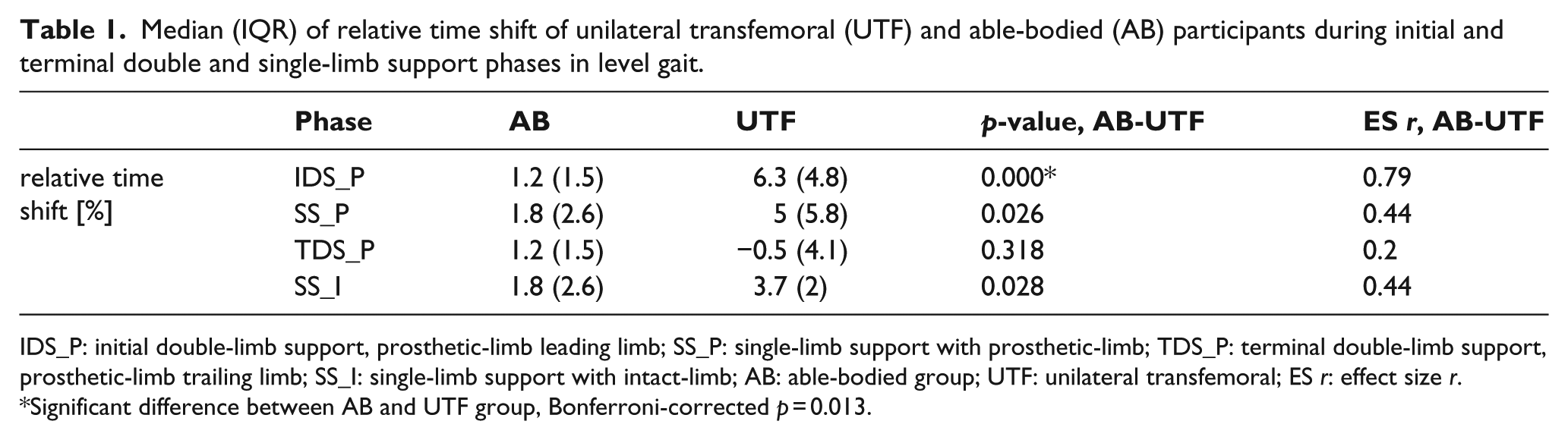
IDS_P: initial double-limb support, prosthetic-limb leading limb; SS_P: single-limb support with prosthetic-limb; TDS_P: terminal double-limb support, prosthetic-limb trailing limb; SS_I: single-limb support with intact-limb; AB: able-bodied group; UTF: unilateral transfemoral; ES r: effect size r.
Significant difference between AB and UTF group, Bonferroni-corrected p = 0.013.
Discussion
The aim of this study was to assess the efficacy of the application of an inverted pendulum model to the overground gait of individuals with UTF. The prosthetic limb of individuals with UTF more closely replicates the characteristics of a rigid segment than does an intact leg, due primarily to the non-articulation or reduced articulation of the prosthetic knee during stance and also the mechanical nature of prosthetic componentry making up a large proportion of the affected limb. However constrained movement in the prosthetic ankle joint may act against the inverted pendulum model. Therefore, it is not intuitively clear, whether the inverted pendulum model would represent UTF gait well. The results of this study partially support the hypothesis that the inverted pendulum model would be applied similarly to both AB gait and UTF gait during intact-limb stance but less so during prosthetic-limb stance. As hypothesised, the magnitude of relative time shifts between CoM height and velocity maxima and minima in the AB group were consistently close to zero across all phases of the gait cycle, indicating that an inverted pendulum model is a reasonable estimation of AB gait. In the UTF group, the relative time shifts were not consistent across all phases of the gait cycle and showed an increased relative time shift for IDS_P, during which the prosthetic-limb was being loaded, compared to the gait phases in which the prosthetic-limb was in SS, terminal DS or in swing. During IDS_P, the maximum CoM forwards velocity occurred after the minimum CoM height, as has been reported previously in individuals with UTT. 12 The IDS_P was the only phase showing a statistically significant increase in relative time shift between the CoM height and forward velocity maxima and minima for the UTF group, compared to the AB group. This suggested that while an inverted pendulum model of gait could be applied appropriately to AB gait, this was not generally the case in the UTF group, especially during the IDS_P phase. However, the lowest observed relative time shift in the UTF group also occurred during prosthetic-limb stance, during TDS_P. During TDS_P, UTF gait appeared to function in accordance with the inverted pendulum model in a way most like that of the AB group, with maximum CoM velocity occurring almost synchronously with minimum CoM height (median difference − 0.5 % gait cycle); therefore, the hypothesis that the model would perform less well during prosthetic stance was only partially supported.
The results from this study are similar to that of previous research, where the application of an inverted pendulum model to the gait of individuals with UTT was found to be inappropriate. 12 This study demonstrates that for individuals with UTF, during the IDS_P phase when the prosthetic-limb is being loaded, significant temporal separations between CoM maximum velocity and minimum height occur. This can possibly be explained by an altered loading response knee flexion pattern induced by the prosthetic knee type resulting in minimum CoM height occurring earlier than in the AB group. If this was due to the possible use of the controlled stance phase flexion provided by 7 out of the 10 knee types or due to a locked knee during stance phase cannot be answered by this study. Thus, peak CoM velocity is observed while the CoM is being elevated in individuals with UTF. Conversely, the two events are coincident in AB individuals, as loading response knee flexion appears to extend the CoM lowering phase in order to allow minimum CoM height to coincide with CoM peak forwards velocity (Figure 1). Similarly, the same direction of temporal offset between minimum CoM height and peak CoM velocity observed in UTT participants, where the CoM is accelerating forwards while it is being elevated, 12 may be due to reduced loading response flexion, which typically occurs in such individuals because of impingement of the knee by the socket and the desire to reduce in-socket/residuum torques. Given that both UTF and UTT participants have similar relative time shifts between maximal and minimal CoM displacements and velocities during IDS_P, it would appear reasonable that restricted loading response knee flexion could, at least partially, be an explanation for this temporal offset.
During the transition from one leg to the other in AB gait, progression is typically accomplished via positive work through ankle plantar flexion of the trailing leg. Individuals with lower-limb amputation cannot actively generate power at the prosthetic ankle, and hence use a more energetically costly strategy involving positive work at the residual hip during early intact-limb stance.2,24 All participants in this study used the same, non-articulating energy-storing and returning prosthetic foot device, so (lack of) power generation at the prosthetic ankle was likely similar for all. However, the UTF participants were most divergent from the inverted pendulum model during IDS_P, when the intact-limb was pushing off. This suggests that it is the leading, weight accepting limb that modulates the timing of CoM maximum velocity and minimum height during DS and ultimately, adherence to the inverted pendulum model of gait. While a large body of research focuses on the (lack of) propulsion provided during TDS_P, the results of this study point at the reduction in passive and eccentric work during IDS_P also being an important factor in the higher metabolic cost of gait experienced by individuals with lower-limb amputation. Increased energy expenditure has been proposed to be associated with disruptions in energy transformations within the inverted pendulum model, 16 which would support this supposition. There are no supporting data, but our suggestion would be that while a lack of active work at the prosthetic ‘ankle’ during late stance undoubtedly contributes to the previously reported increased metabolic cost of walking in individuals with lower-limb amputation,9,10 the lack of passive, or eccentric, energy absorption during early and mid-stance does so too. This suggestion is supported by a previous finding in individuals with UTT, who experienced a significant reduction in mechanical work, per metre travelled, done at the intact leg when they used a hydraulically articulating ankle foot device that absorbed more energy during early stance, and returned less energy during late stance, than their customary, non-articulating prosthetic feet. 25 This should certainly be the subject of future study.
Finally, as impairments in gait function seem to be reflected by compliance, or lack of, to the inverted pendulum model, the resulting relative time shift might be of clinical relevance. For example, the size of the relative time shifts between CoM height and velocity maxima and minima could potentially be used as a tool to quantify the efficacy of innovative prosthetic device design features aimed at reducing the metabolic cost of walking and improving gait efficiency in individuals with amputation.
It has to be kept in mind that while all participants used the same type of ankle device, a variation of knee components were used and possible individual specific gait patterns induced by specific knee components were not considered. In addition, it has to be kept in mind that the results reflect the gait using a rigid ankle device, which could also contribute to the increased time shift in the IDS_P phase.
Conclusion
In conclusion, results from this study demonstrate that during level walking, an inverted pendulum model represents AB gait well, but deviation to the model were seen in parts of the UTF gait. In addition, UTF gait functioned mechanically most like AB gait during prosthetic-limb single and terminal DS and intact-limb SS. Divergence from inverted pendulum behaviour during the initial prosthetic DS phase following prosthetic-limb IC indicates that it is the loading limb that primarily modulates timing of CoM maximum velocity and minimum height, rather than the unloading limb. These findings may also help explain the increased metabolic cost of walking, compared to the AB individuals with UTF. This relationship should be further investigated.
Footnotes
Acknowledgements
The authors would like to thank Endolite Deutschland GmbH (Kulmbach, Germany) for providing the foot-component for the two UTF participants measured in Salzburg. Endolite Deutschland GmbH had no role in the study conception and design; in the collection, analysis and interpretation of data; in the writing of the manuscript and in the decision to submit the manuscript for publication.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.