
Abstract
Background:
The ability to walk with a prosthesis is the main objective of rehabilitation following amputation, and distance and speed of walking achieved are considered determining factors in amputees’ perception of quality-of-life.
Objectives:
To assess walking abilities and improvement in gait distance and speed parameters in patients undergoing transfemoral amputation with a femoral implant that allows distal support of the residuum.
Study design:
Experimental before-and-after study.
Methods:
Ten transfemoral amputation patients received a titanium implant that allowed distal weight bearing of the residuum within the socket. The post-intervention follow-up period was 14 months. We evaluated the functionality using a 2-min walk test and the physiological cost index.
Results:
The etiology of amputation was traumatic in six patients (60%). The mean 2-min walk test score was 98.4 ± 19.5 m prior to the femoral implant and 122.5 ± 26.1 m at 14 months (p < 0.008), representing an improvement of 24.5%. The mean gait speed prior to the femoral implant was 0.82 ± 0.16 and 1.02 ± 0.21 m/s at 14 months (p < 0.008). The physiological cost index showed no differences (p < 0.55).
Conclusion:
The results of this study show an improvement in the distance walked and gait speed in amputees 14 months after having received a femoral implant.
Clinical relevance
This article provides additional insight into the use of a femoral implant that allows distal support of the residuum to improve walking abilities and gait distance and speed parameters in patients undergoing transfemoral amputation, mainly those of vascular origin.
Keywords
Background
Amputation of a lower limb is a definitive surgical procedure and has important functional, psychological, and social sequelae that affect the quality of life of the person involved. 1 Two levels of amputation have been described in femoral amputations: transfemoral amputation (TFA) and knee disarticulation (KDA). Preservation of the femoral condyles in a patient with KDA facilitates distal support within the socket in contrast to what occurs in TFA. This allows direct transfer of the weight bearing loads toward the residual limb and consequently an increase in independence for walking and lower energy consumption compared with TFA.2–4 The ambulation of patients with more proximal amputations is less efficient and requires higher energy consumption than that of patients with more distal amputations of traumatic and vascular origin. 5
The ability to walk with a prosthesis with or without technical aids is the main objective of rehabilitation following the amputation of a lower limb; distance and speed of walking achieved are considered determining factors in amputees’ perception of quality of life. 6 The inability to walk quickly is considered by 59% of patients to be a sign of poor quality of life, and thus, any action aimed at improving gait and speed also has a direct impact on the quality-of-life improvement of these patients. 7
The advantages of KDA compared with TFA have led to the design of an endomedullar implant with a distal spacer that allows a direct load on the residuum over the distal surface of the socket and performs the same function as the femoral condyles, thereby achieving greater walking ability.8,9 Several studies have evaluated the functional capacity of TFA following the placement of a titanium implant in the femoral medullary canal, which allows direct anchoring of the prosthetic knee to the implant but does not facilitate distal weight bearing of the residuum, similar to what occurs with KDA.10–13
The aim of this study was to evaluate the walking abilities and improvement in the parameters of gait distance and speed in patients undergoing TFA who were at least 1 year past amputation with a femoral implant that allows distal support of the residuum. In addition, we assessed the same parameters of gait distance and speed, classifying the patients into groups according to their age, gender, and cause of amputation.
Methods
Participants
We performed an experimental before-and-after intervention study in a group of 10 TFA patients who received a titanium implant allowing distal weight bearing of the residuum within the socket acting each patient as its own control. Participants were recruited from 1 March 2011 through 1 March 2013 in the outpatient department of Rehabilitation Hospital de Mataró, in Spain. The demographic sample data are shown in Table 1.
Demographics of study sample at inclusion (n = 10).
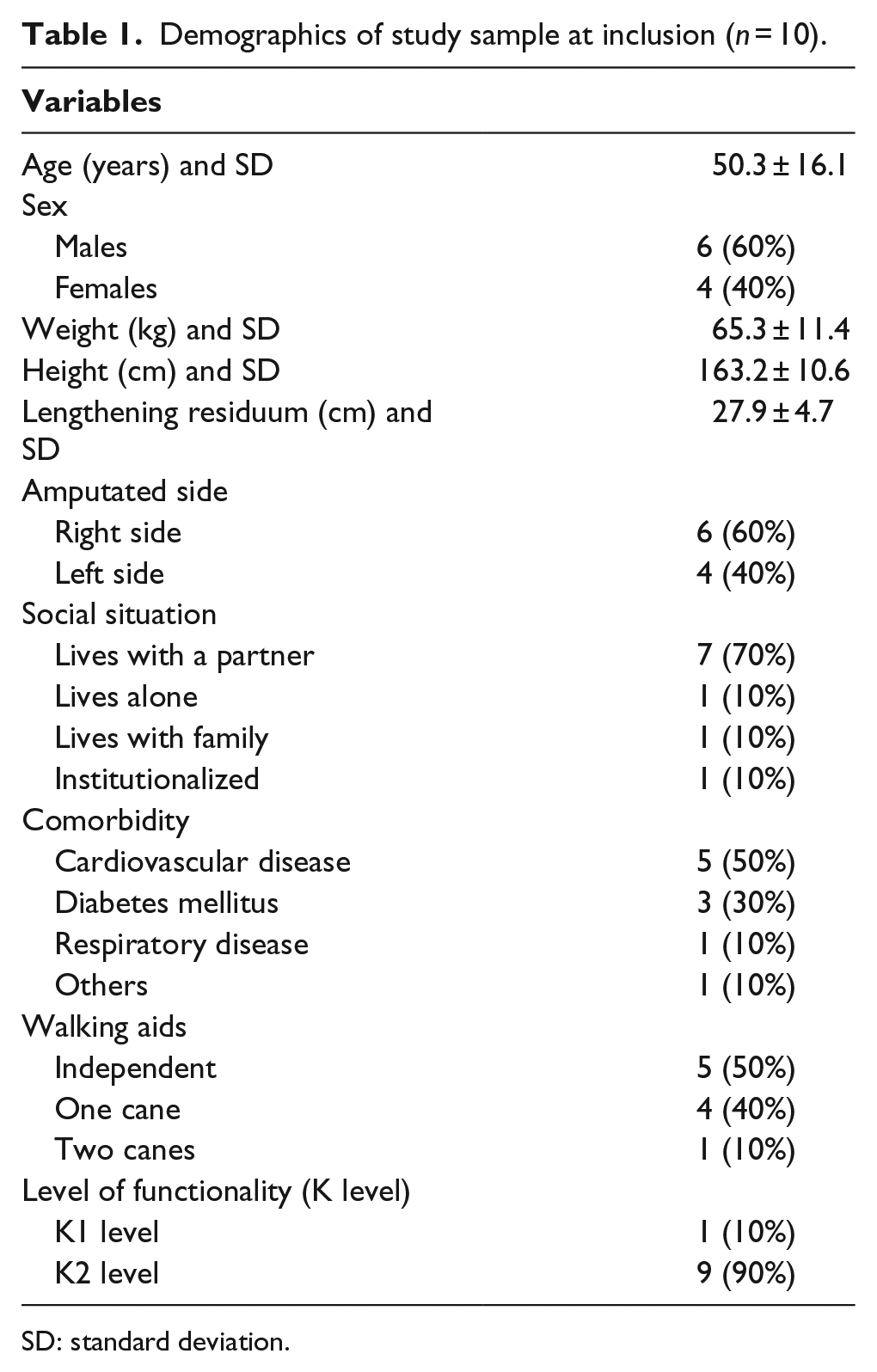
SD: standard deviation.
Inclusion criteria were as follows: length of the femur of the amputated limb of at least 15 cm measured from the greater trochanter, use of the prosthesis for at least 12 months prior to enrollment and more than 6 h/day, ability to walk indoors with or without supervision, and with or without ambulation aids and unilateral femoral amputation. The criteria for exclusion were the presence of cognitive impairment hindering the ability to follow instructions and/or perform the tests, body weight over 100 kg, active oncologic pathologies, psychological disorders, previous residuum infection, active infection, residual femur length less than 15 cm measured from the greater trochanter, pregnancy, and hip flexion deformity greater than 30°.
Each patient underwent pre- and post-operative controls to evaluate the study variables. The post-intervention follow-up period was 14 months. All patients underwent surgery by the same surgical team, maintaining the same prosthetic knees and feet used previously. This study was approved by the Ethical Committee of Hospital de Mataró Hospital. All participants gave their informed consent.
Implant
The femoral implant designed for this study is a class IIb femoral implant and is composed of two pieces (Figures 1 and 2). The femoral stem is made of a titanium alloy (Ti-6Al-4V) according to the ASTM F-136 standard to facilitate anchorage within the residual femoral canal. The length of the femoral stem ranges from 120 to 180 mm, with a diameter of 11–17 mm. The second piece is a spacer made of high-density polyethylene (ultra-high-molecular-weight polyethylene (UHMWPE)) with a diameter of 54–62 mm, which is distally connected to the stem by a titanium screw and a polyethylene plug. The spacer or cushion allows distal support of the residuum within the socket (Figures 1 and 2).
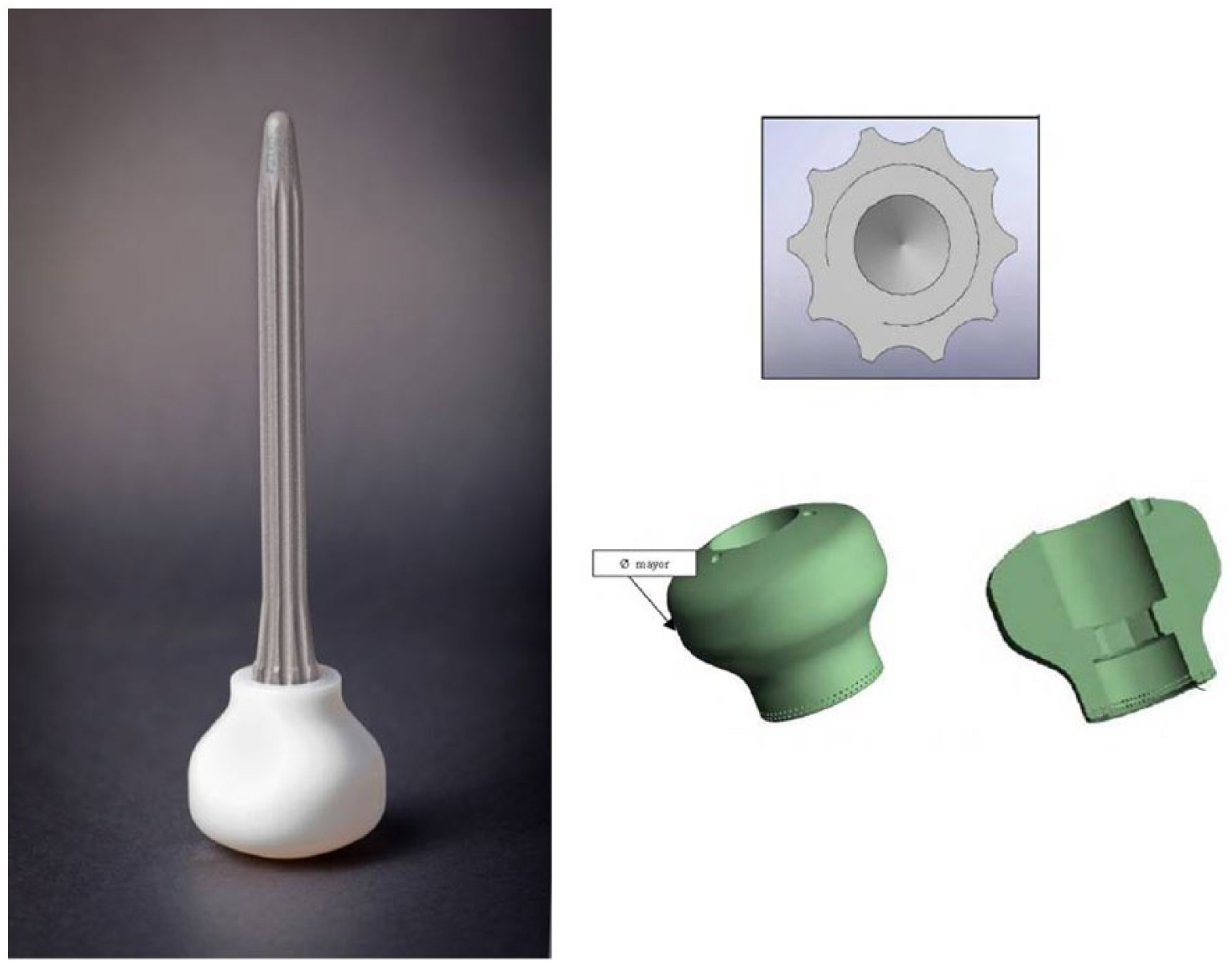
Osseointegrated femoral implant.

Femoral implant in a patient following surgery.
Surgery
The surgical approach to the femur takes advantage of the patient’s existing scar. Afterward, the distal part of the residual femur is smoothed out and the medullary canal of the femur is reamed to the appropriate diameter to create the final space for the implant’s stem. Trial implants are used to determine the appropriate size of the implant, both in length and diameter of the stem, as well as the size of the spacer. The spacer size is the largest size that permits closure without soft tissue tension. Finally, the definitive implant is assembled and press-fit into the femur. Soft tissue closure is performed with a correct myoplasty that completely covers the spacer.
Rehabilitation
At 15 days post-intervention, the patients started with a program of distal charges to the residuum, initially 5 kg and augmented to a 20 kg maximum at 4 weeks. Between 4 and 6 weeks, a provisional socket with distal support was manufactured and the definitive socket was made at 12 weeks. During this period, the patients performed gait and balance training 3 times per week at the Rehabilitation Department.
Measure
2-Min walk test
The 2-min walk test (2MWT) is frequently used to measure post-procedure results following the procedure in transfemoral amputees. The 2MWT measures the number of meters walked by the patient in 2 min with or without aids. We used this test in TFA because it is correlated with measures of physical functioning and has been reported to be a useful tool to assess changes after a rehabilitation program and prosthetic use in this population.14,15
Physiological cost index
The physiological cost index (PCI) measures the energetic efficiency of walking and is determined together with gait speed and heart rate before and after exercise. In the PCI test, the patient stood for 2 min quietly at the departure line, after which the heart rate was measured by the tester and the physiotherapist. The PCI was calculated as follows: PCI (beats/m)=[heart rate at end (beats/min) - heart rate at rest (beats/min)]/speed (m/min). Oxygen saturation and heart rate were recorded throughout the test using a pulse oximeter (Digit® Finger Oximeter; Smiths Medical PM, St Paul, Minnesota, USA). Because the distance for this test is not standardized, we chose the distance walked in 2 min, similar to other TFA studies.6,16
Data analysis
Descriptive statistical analysis of the baseline data was performed. The mean values and standard deviation were used for the quantitative variables while percentages were used for qualitative variables. The non-parametric Mann–Whitney U test was used to analyze the differences between dependent quantitative variables, while the Wilcoxon test was used to evaluate the differences between independent quantitative variables. The results with p <0.05 were considered statistically significant. Data analysis was performed with SPSS 12.0.
Results
A total of 10 participants (60% men and 40% women) with a mean age of 50.3 ± 16.3 years were included in the study. The etiology of amputation was traumatic in four patients (40%), peripheral vascular disease in four (40%), and due to oncologic disease in two (20%). The amputation involved the right side in six patients (60%) and the left side in four (40%).
The average time since amputation was 8.07 ± 5 years, and eight patients (80%) reported pain prior to surgery. The number of hours of daily prosthesis use was 10.1 ± 2.2 h and the level of amputation was the middle third in all the patients.
The patients obtained a mean score of 98.4 ± 19.5 m in the 2MWT prior to the femoral implant procedure and 122.5 ± 26.1 m at 14 months after surgery, showing a statistically significant difference (p < 0.008), and representing an increase of 24.5%. Gait speed also significantly increased from a mean score of 0.82 ± 0.16 m/s prior to the femoral implant to 1.02 ± 0.21 m/s at 14 months (p < 0.008).
The patients obtained a mean PCI score of 0.57 ± 0.28 prior to the placement of the femoral implant and 0.51 ± 0.23 at 14 months after surgery, showing a not statistically significant difference (p < 0.55).
Table 2 shows the individuals’ differences in performance with and without implants. Tables 3–5 show the results obtained when classifying the patients by groups of gender, age (<50 and >50 years), and cause of amputation.
Individual differences in performance without and with implant.
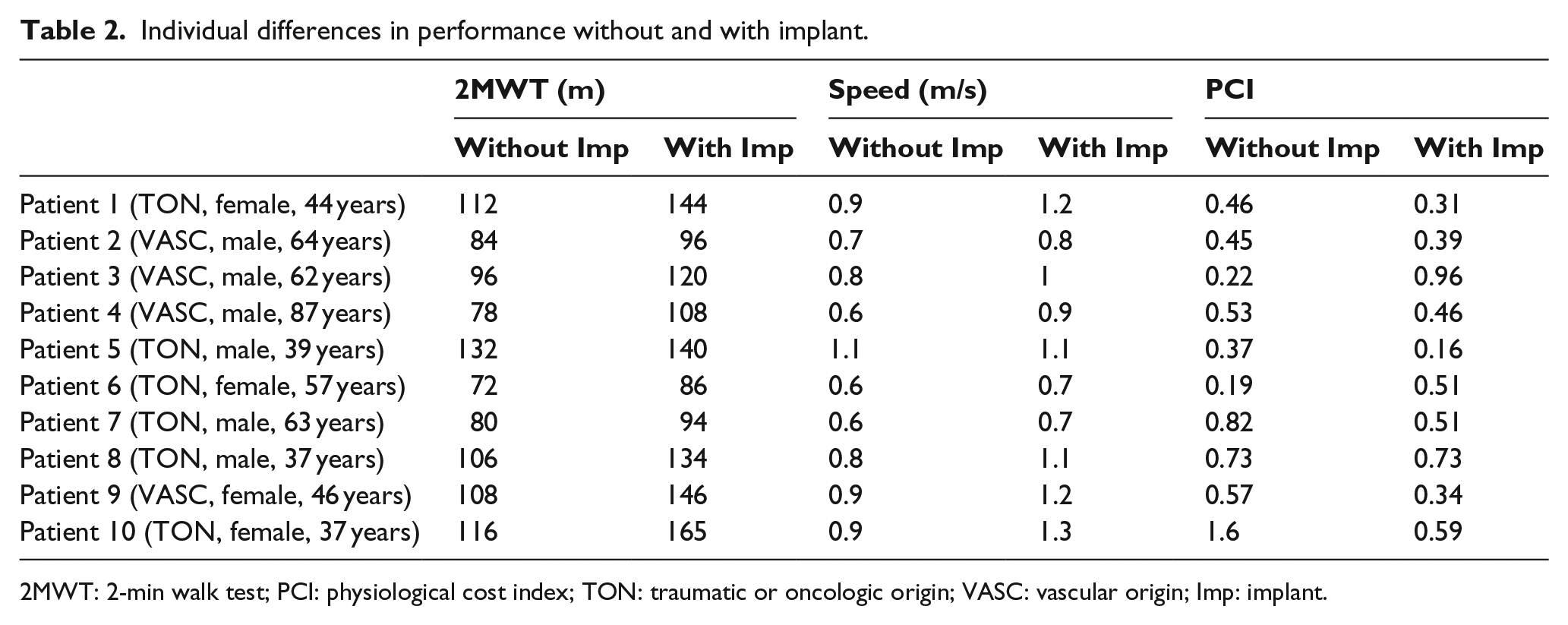
2MWT: 2-min walk test; PCI: physiological cost index; TON: traumatic or oncologic origin; VASC: vascular origin; Imp: implant.
Means and standard deviation classified by age groups.
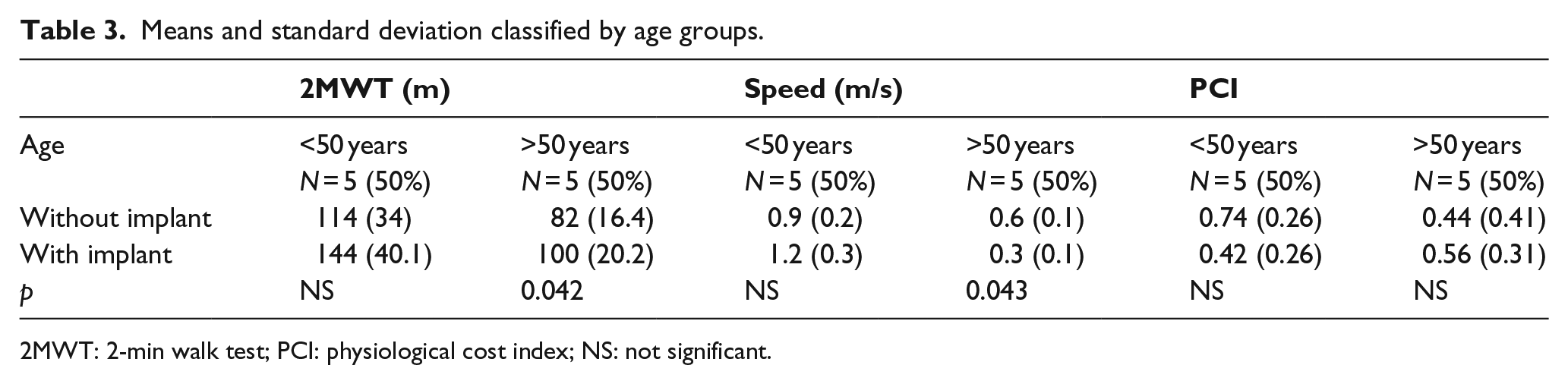
2MWT: 2-min walk test; PCI: physiological cost index; NS: not significant.
Mean values and standard deviation by gender.
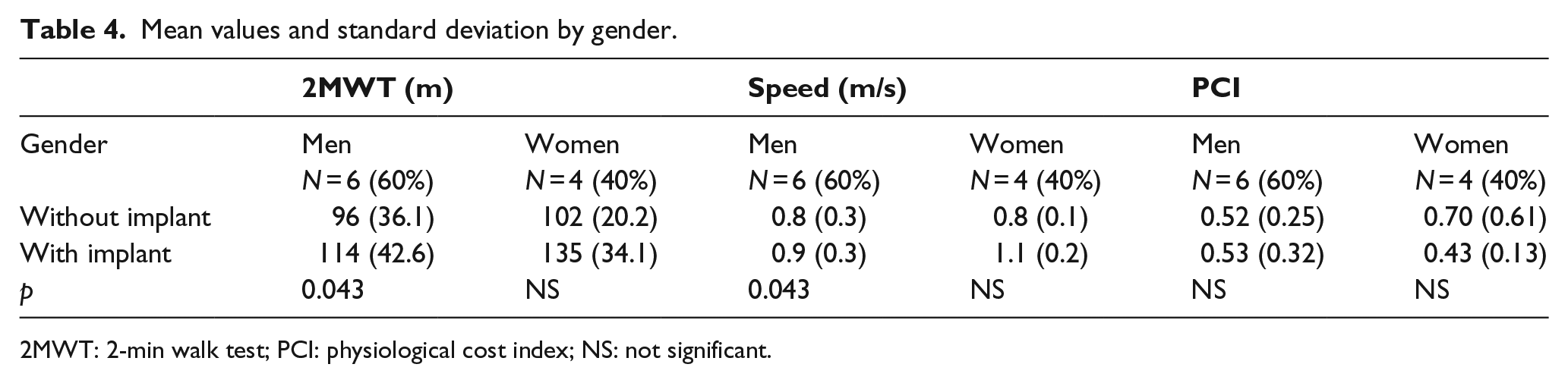
2MWT: 2-min walk test; PCI: physiological cost index; NS: not significant.
Mean values and standard deviation classified by causes of amputation.
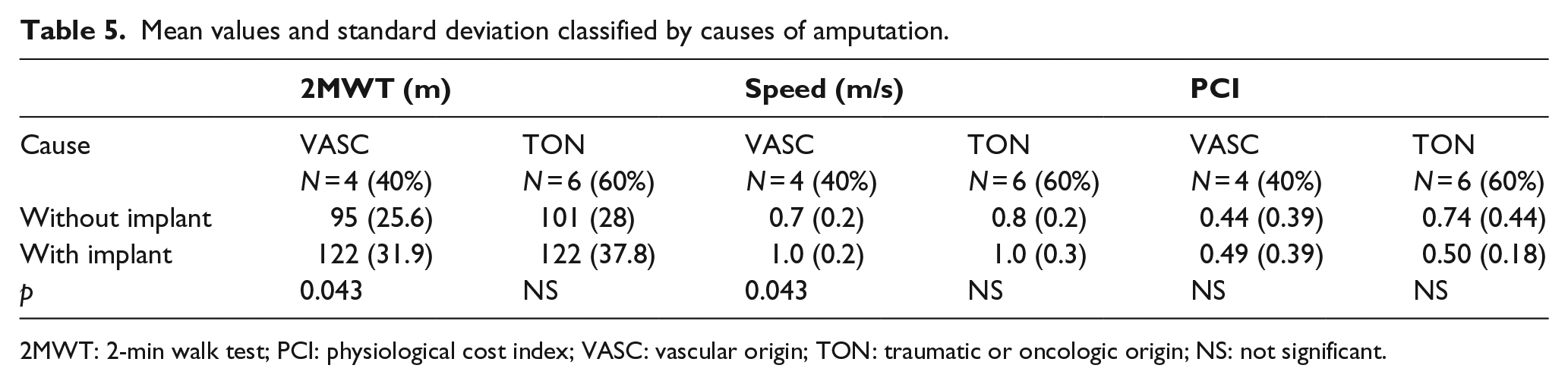
2MWT: 2-min walk test; PCI: physiological cost index; VASC: vascular origin; TON: traumatic or oncologic origin; NS: not significant.
Discussion
The results of this study showed improvements in functional capacity and gait speed of amputees 14 months after receiving a distal weight bearing titanium transfemoral implant for amputations of vascular, traumatic, or oncologic origin.
To our knowledge, this is the first study to evaluate the functional capacity of transfemoral amputees after the placement of an implant allowing distal weight bearing of the residuum. The studies described to date have only assessed the walking abilities of transfemoral amputees after the placement of a titanium implant in the femoral medullary canal allowing anchoring of the knee but not distal weight bearing of the residuum.10,11,17–19
The mean distance walked by the patients in this study prior to receiving the femoral implant was 98.4 m, differing from the results obtained by Brooks et al., 14 who reported 41.2 ± 34 m in the 2MWT. However, in contrast to our study, the mean age of their patients was 63.6 years, testing was performed 3 months after hospital discharge following amputation, and most of the amputations were of vascular origin. The differences between the results may be due to two factors: our study included amputations from several causes (vascular, traumatic, or oncologic) and the patients had already had a prosthesis prior to the placement of the implant. At 14 months after implantation, the patients walked a mean of 122.5 m in the 2MWT, which is a statistically significant increase of 24.1 m. Resnik and Borgia 20 considered a distance greater than or equal to 34.3 m in the 2MWT to be clinically relevant in transtibial and transfemoral amputees.
Several groups have reported improvements in the 2MWT following different interventions in amputees. In a short, intense physiotherapy program in 29 patients (21 transtibial and 8 transfemoral amputees) with a mean age of 36.93 years, Rau et al. 21 observed an improvement of 20.15 m in the intervention group compared to the control group. Darter et al. 15 also reported an increase of 29.18 m in the 2MWT after an 8-week home rehabilitation program in chronic transfemoral amputees. However, our results cannot be compared because no other study has used implants similar to those in our study.
When classifying the results based on age, gender, and cause of amputation, we found a significant increase in distance walked in the group of men over the age of 50 years and with amputations of vascular origin. These results may be due to the distal support provided by the femoral implant, which may increase the confidence in walking by older vascular patients with greater comorbidities and lesser basal functional capacity.
The increase in the distance walked is important because small increments in this value may increase independence in walking and activities of daily living (ADL). Lerner-Frankiel et al. 22 reported that patients with moderate family support needed to walk a minimum of 600 m a day to be able to live in an apartment and carry out ADL; this increased to 1100–1450 m/day to live independently without external support and carry out some activities outside the home. These values are similar to those reported by Geertzen et al., 23 who estimated a minimum distance of 500 m for amputees to be independent in their ADL. Improvement in the distance walked may be especially relevant in vascular patients over the age of 50 years with lesser initial functional capacity by allowing an increase in their walking capacity and ADL.
The increase in the distance walked in the 2MWT reflects an increase in gait speed, which is important because it may be translated into greater capacity of the individual to carry out community tasks such as crossing the street. In addition, interventions with rehabilitation programs that improve functional capacity are associated with improvements in gait speed.19,24,25 Walker et al. 26 estimated a normal gait speed to be of 1.38 and 0.75 m/s in tibial amputees of vascular origin, 0.6 m/s in vascular femoral amputees, and 0.86 m/s in traumatic amputees 6 months after receiving a prosthesis. In our sample, the gait speed at 14 months after the femoral implant was 1.02 m/s. The values reported in the literature vary greatly, from Rau et al. 21 reporting a speed of 1.32 m/s to Jones et al. who reported a speed of 0.78 m/s 25 after an intensive rehabilitation program in traumatic amputees. The differences between those two studies could be related to their samples: Rau et al. 21 included transtibial and transfemoral amputees, while Jones et al. 25 only included transfemoral amputees. The increase in our sample (0.2 m/s) is greater than that observed by Barnett et al. 24 (0.12 m/s) and may be related to the differences in the patients studied and the time after having received the prosthesis.
In this study, most of the patients (70%) showed an improvement of the PCI values 14 months after the placement of the implant, decreasing from 0.59 to 0.49. This improvement was not statistically significant in women (0.7 vs 0.43), in patients aged under 50 years (0.74 vs 0.42) or in amputees of traumatic origin (0.74 vs 0.5). On the other hand, the PCI values worsened, albeit not significantly, in males, patients over 50 years of age and in those of vascular origin. The reason for these differences may be that the group of women and amputees of traumatic origin were younger than the group of males and amputees of vascular origin.
Our results differ from those obtained by Hagberg et al. 6 who reported a PCI of 0.55 in a sample of 42 chronic transfemoral amputees of traumatic and oncologic origin compared with non-amputee patients ranging in age from 20 to 70 years. In our study, 40% of the amputations were of vascular origin, and thus the patients had greater comorbidity than the patients in the Hagberg study, with our PCI results being of great relevance. The results obtained in this study are similar to those of Hachiuska et al. 27 (0.52) who reported a change in the PCI in 12 older amputees when comparing two types of transfemoral sockets. Rau et al. 21 obtained a PCI of 0.189 after undertaking an intensive rehabilitation program. These results are much lower than those obtained in our study, but the sample in the study by Rau et al. included transtibial and transfemoral amputees in contrast to our study, which included only transfemoral amputees.
The PCI results obtained in this study indicate that the femoral implant only improves the energetic performance during walking in young patients and with non-vascular etiology, while the PCI achieved by patients older than 50 years of age with vascular surgery does not improve, possibly due to the associated comorbidities found in these patients, such as diabetes mellitus or cardiovascular disease.
This study has several important limitations that should be taken into account. The first is the total number of patients in the cohort; this preliminary study included a sample size of 10 patients. The second limitation is the heterogeneity of the sample, which was mainly determined by the causes of amputation. We included transfemoral amputees of vascular, traumatic, or oncologic origin with relevant different characteristics between the patients in these two groups. Finally, we believe that the inclusion criteria should be stricter with regard to the grade of patient mobility. Our patients presented an elevated mean of daily hours of prosthesis use with a consequent important grade of mobility. Compared to previous studies, our patients had an acceptable functional capacity before the implant placement, and thus, the results after intervention could have been more relevant if the patients included had been less active.
Conclusion
The results of this study show an improvement in distance walked and gait speed in amputees at 14 months after having received a femoral implant, especially in male patients, those older than 50 years of age and with amputations of vascular origin. Further studies are needed in larger cohorts of patients to confirm the improvements observed in this study using direct measurement of the residuum or experimental gait analysis.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Tequir S.L. (Valencia - Spain), and supported by a Grant from CDTI (National Technological Development and Innovation Center), through European funds in the FEDER program 2007–2013.