
Abstract
Background:
People with lower limb amputation report the need to concentrate on walking. Dual-task paradigms are often used to study such interactions between cognition and the control of balance and gait in people with lower limb amputation.
Objectives:
To summarize evidence related to dual-task standing and walking in people with lower limb amputation and discuss implications for future research.
Study design:
Structured review.
Methods:
A structured search was completed in PubMed, CINAHL, and Web of Science from database inception to May 2017. Eligible articles were in English, included participants with lower limb amputation, and assessed dual-task standing or walking. Study information was extracted by one reviewer and assessed for accuracy by a second.
Results:
A total of 12 articles met eligibility criteria. Seven examined differences in dual-task standing or walking, and five assessed dual-task walking across microprocessor-controlled and non-microprocessor-controlled prosthetic knee conditions.
Conclusion:
Results suggest that (1) dual-task interference in standing is greater for people with lower limb amputation than non-amputees and (2) the use of microprocessor-controlled knees improves dual-task performance for people with limited mobility compared to non-microprocessor-controlled knees. The small number of studies, diversity of dual-task methods, and methodological limitations challenge the synthesis of study results. Future research should assess specific clinical characteristics that can affect dual-task performance in people with lower limb amputation.
Clinical relevance
Understanding how people with lower limb amputation use increased attention in balance and gait to compensate for limb loss can inform prosthetic interventions and training. Dual-task research suggests that people with amputation use increased cognitive control for standing compared to controls and microprocessor-controlled knees improve dual-task walking in people with limited mobility.
Keywords
Background
For people with lower limb amputation (LLA), loss of physical limb structures and peripheral motor and sensory systems contributes to profound mobility challenges. Mobility limitations commonly experienced by people with LLA include impaired postural stability,1–3 increased energy expenditure while walking,4–6 decreased gait speed,5–7 and pronounced gait asymmetries.7,8 Such limitations may result in difficulties negotiating uneven terrain, 9 hills, 10 and stairs.11,12 It is also conceivable that these impairments contribute to restrictions in walking activity13,14 and the high incidence of falls15,16 reported by people with LLA.
In addition to these mobility limitations, many people with LLA report the need to “concentrate on every step.”15,16 This perception may reflect increased reliance on cognitive resources to compensate for loss of peripheral afferent feedback and efferent control. Increased use of cognitive resources when standing and walking may limit resources available for concurrent cognitive tasks, such as social interaction or observing the environment. Furthermore, the need to concentrate on walking has been correlated with falls and fear of falling in people with LLA. 17 Reducing the need to concentrate during these tasks may serve to both improve quality of life and promote safety in this clinical population. Microprocessor-controlled knees with stumble recovery have been noted to increase perceived confidence and reduce fear that the prosthetic knee will buckle, 18 giving this technology the potential to reduce the need to concentrate on standing and walking with a prosthesis.
Dual-task methods assess simultaneous performance of a postural task and a cognitive or motor task to study how cognitive processes, such as concentration or executive function, interact with postural tasks, such as standing and walking. 19 Declines in performance on one or both tasks (i.e. dual-task interference) can be used to infer relative contributions of cognitive resources to postural control. 20 Dual-task interference is often assessed in research using performance changes from single-task to dual-task conditions. Changes (and possible dual-task interference) can occur in the postural control task, the concurrent cognitive or motor task, or in both tasks.
An underpinning assumption of these experiments is that dual-task interference is caused by limited cognitive resources (i.e. capacity theory 21 ) or processing (i.e. bottleneck theory 22 ). The capacity theory hypothesizes that, in circumstances when simultaneous performance of one or more tasks requires cognitive processing that exceeds the available capacity, performance quality of one or more tasks declines. 21 The bottleneck theory postulates that simultaneous performance of multiple tasks can lead to processing interference where the neural system prioritizes one of the tasks and temporarily postpones action on the other, leading to performance decline on the non-prioritized task. 22 Both theories assert that when increased cognitive resources or processes are required for performance of a task, remaining resources or processing channels available for the performance of a concurrent task may be insufficient and result in decline in performance on one or both tasks.
Thus, people who are required to allocate additional cognitive resources to postural tasks will experience greater dual-task interference than those for whom postural tasks are relatively automatic. However, methodological choices, such as selection of postural and cognitive tasks, use of directions for task prioritization, and inclusion of baseline (or single-task) conditions, can profoundly affect investigators’ ability to appropriately and meaningfully interpret results from dual-task studies.20,23,24
Because dual-task paradigms are a non-invasive means to infer the extent to which cognition is employed during standing and walking, investigators1,2,9,25–33 have used these performance-based methods to objectively assess the perceived need to concentrate on walking in people with LLA. However, results from performance-based dual-task studies of standing and walking often do not support the hypothesis that people with LLA have increased dual-task interference compared to people without LLA. Such studies are inconsistent with survey-based studies15–17 that note a large percentage of people with LLA report using heightened concentration for walking. A structured literature review was therefore conducted to assess research examining dual-task standing and walking in people with LLA and to offer potential explanations for discrepancies between performance-based and self-reported study results. The objectives of this review were (1) to identify, appraise, and synthesize original research that used dual-task methods to study standing and walking tasks in people with LLA and (2) to propose recommendations for future research.
Methods
Data sources and eligibility criteria
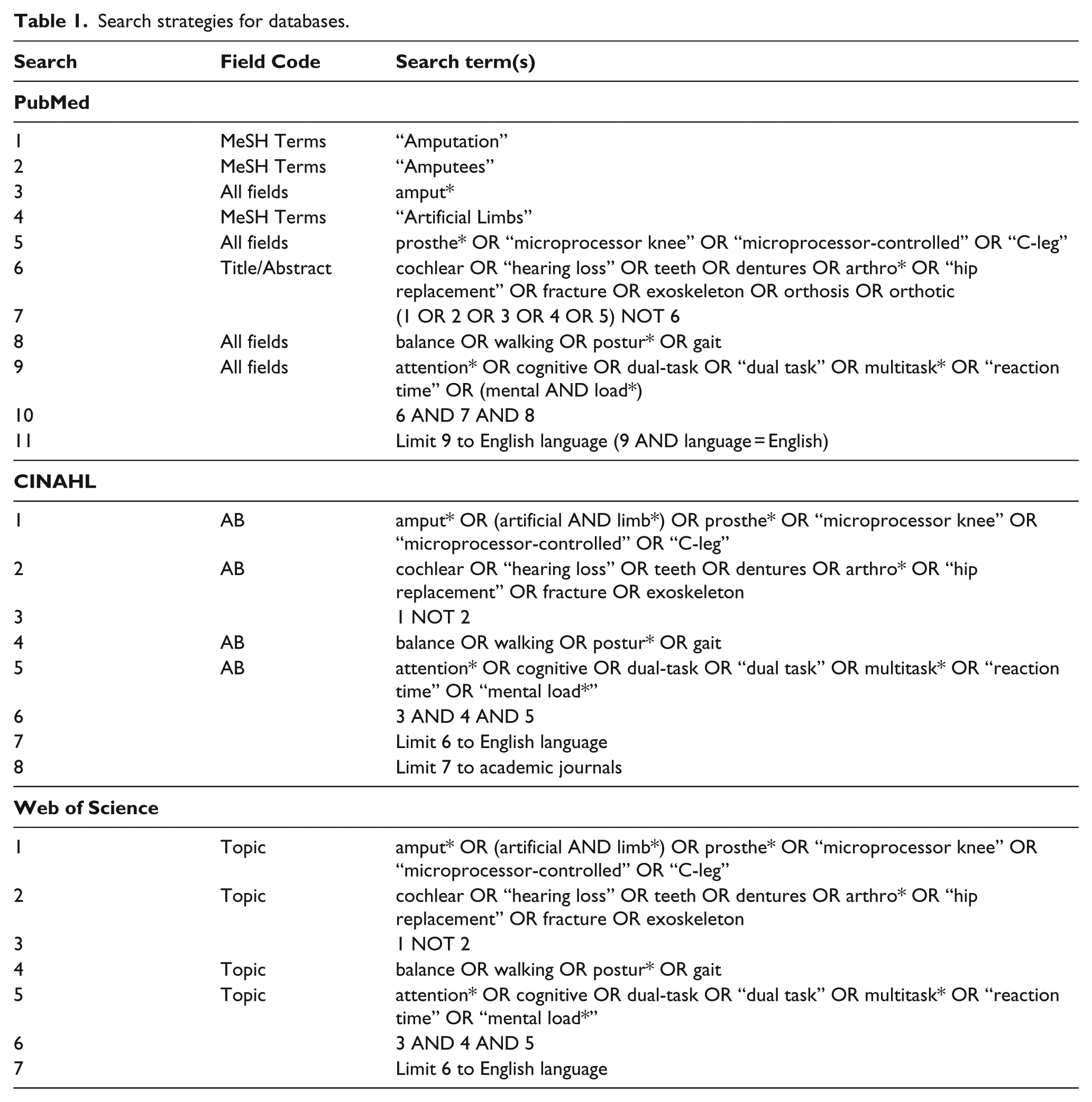
A comprehensive search of the literature was performed from database inception (earliest date: 1965) through May 2017 using three electronic databases: PubMed (1966–05/2017), CINAHL (1982–05/2017), and Web of Science (1965–05/2017). Search strategies for the three databases are provided (Table 1). References of selected articles were also searched to identify additional articles.
Search strategies for databases.
Criteria for inclusion in this review were (1) published in English; (2) adult participants with LLA of any etiology; (3) participants currently use a prosthesis; and (4) the primary or secondary outcome measures assessed dual-task performance during standing or walking tasks with a concurrent cognitive or motor task. Articles were excluded if they were an abstract, thesis, dissertation, or review.
Article selection and data collection process
Two reviewers evaluated titles and abstracts to determine the eligibility of articles identified by the literature search. Potentially eligible articles were obtained and assessed using the criteria stated above. Pertinent information, including study and sample characteristics, postural and cognitive task characteristics, and dual-task related findings, was extracted into evidence tables by a single reviewer and corroborated by a second (Tables 2–4). Study quality was classified using the Physiotherapy Evidence Database (PEDro) Scale, which consists of 11 assessment criteria to determine the validity of study methods (Table 5). Meta-analysis of results was not possible because of the variety of study designs, methodologies, and outcomes measured.
Study and sample characteristics for studies of dual-task performance in people with LLA.
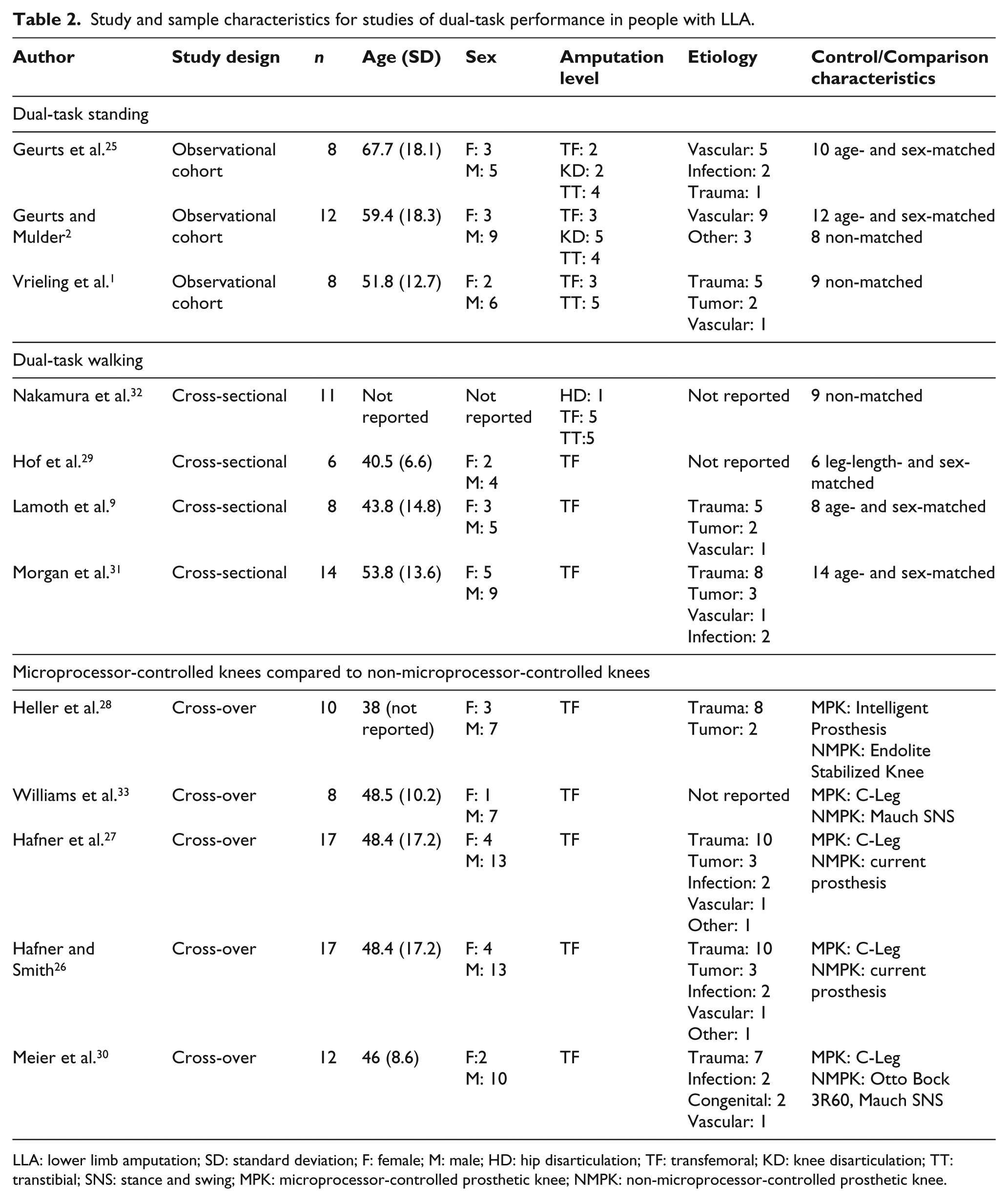
LLA: lower limb amputation; SD: standard deviation; F: female; M: male; HD: hip disarticulation; TF: transfemoral; KD: knee disarticulation; TT: transtibial; SNS: stance and swing; MPK: microprocessor-controlled prosthetic knee; NMPK: non-microprocessor-controlled prosthetic knee.
Postural and cognitive task characteristics for articles describing dual-task studies in people with LLA.
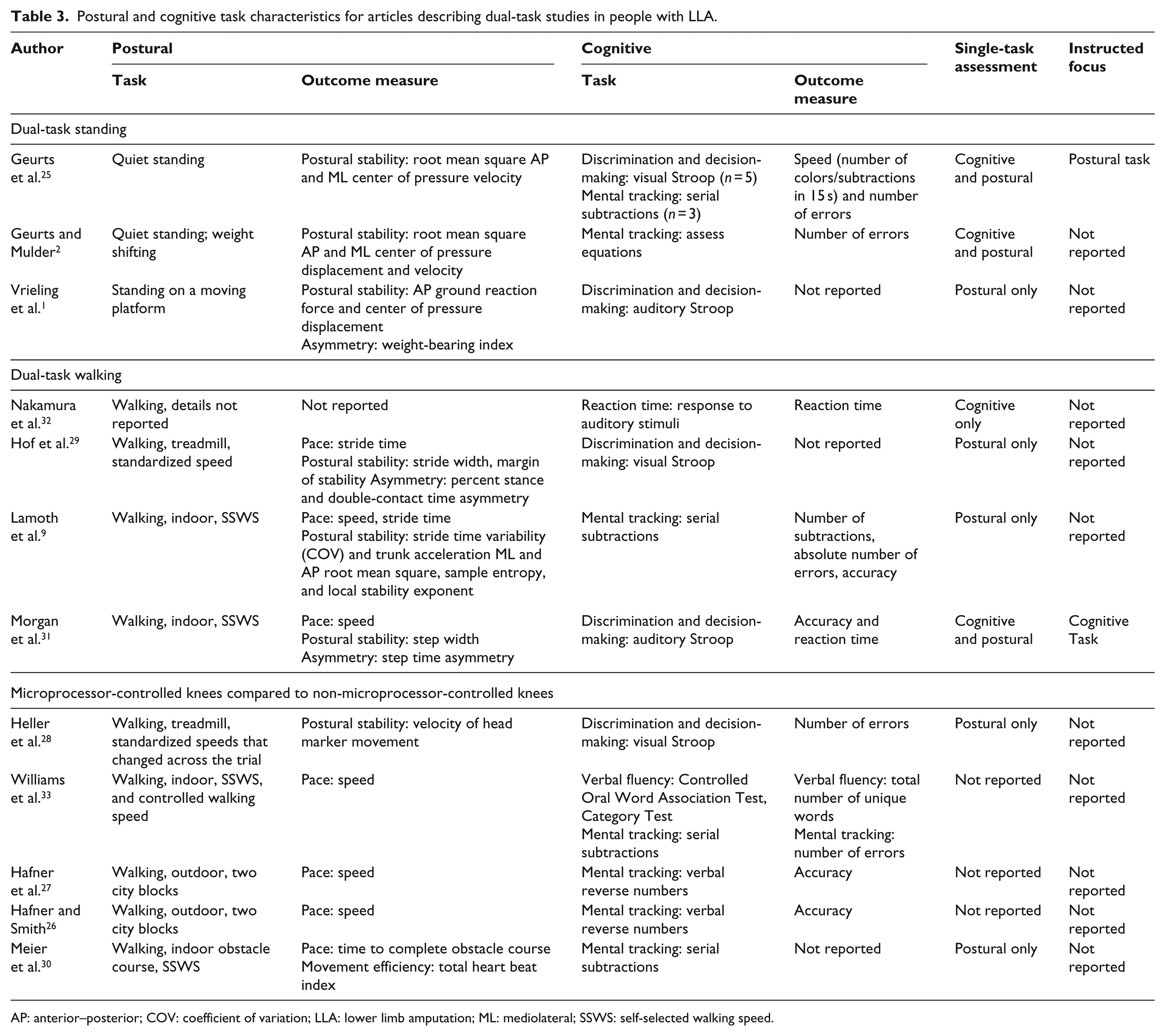
AP: anterior–posterior; COV: coefficient of variation; LLA: lower limb amputation; ML: mediolateral; SSWS: self-selected walking speed.
Dual-task related findings for articles describing dual-task studies in people with LLA.
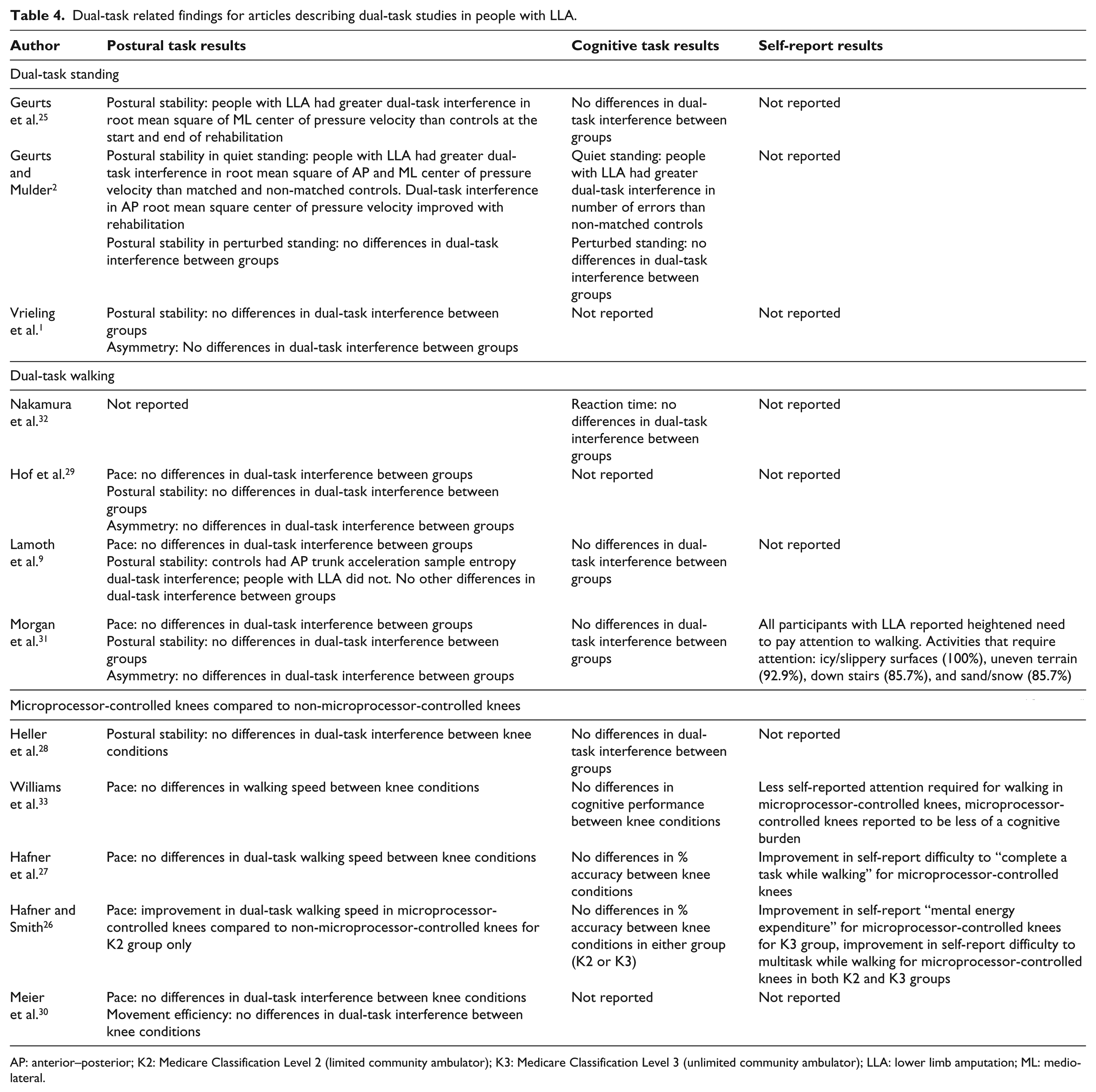
AP: anterior–posterior; K2: Medicare Classification Level 2 (limited community ambulator); K3: Medicare Classification Level 3 (unlimited community ambulator); LLA: lower limb amputation; ML: mediolateral.
Quality assessment of reviewed articles.
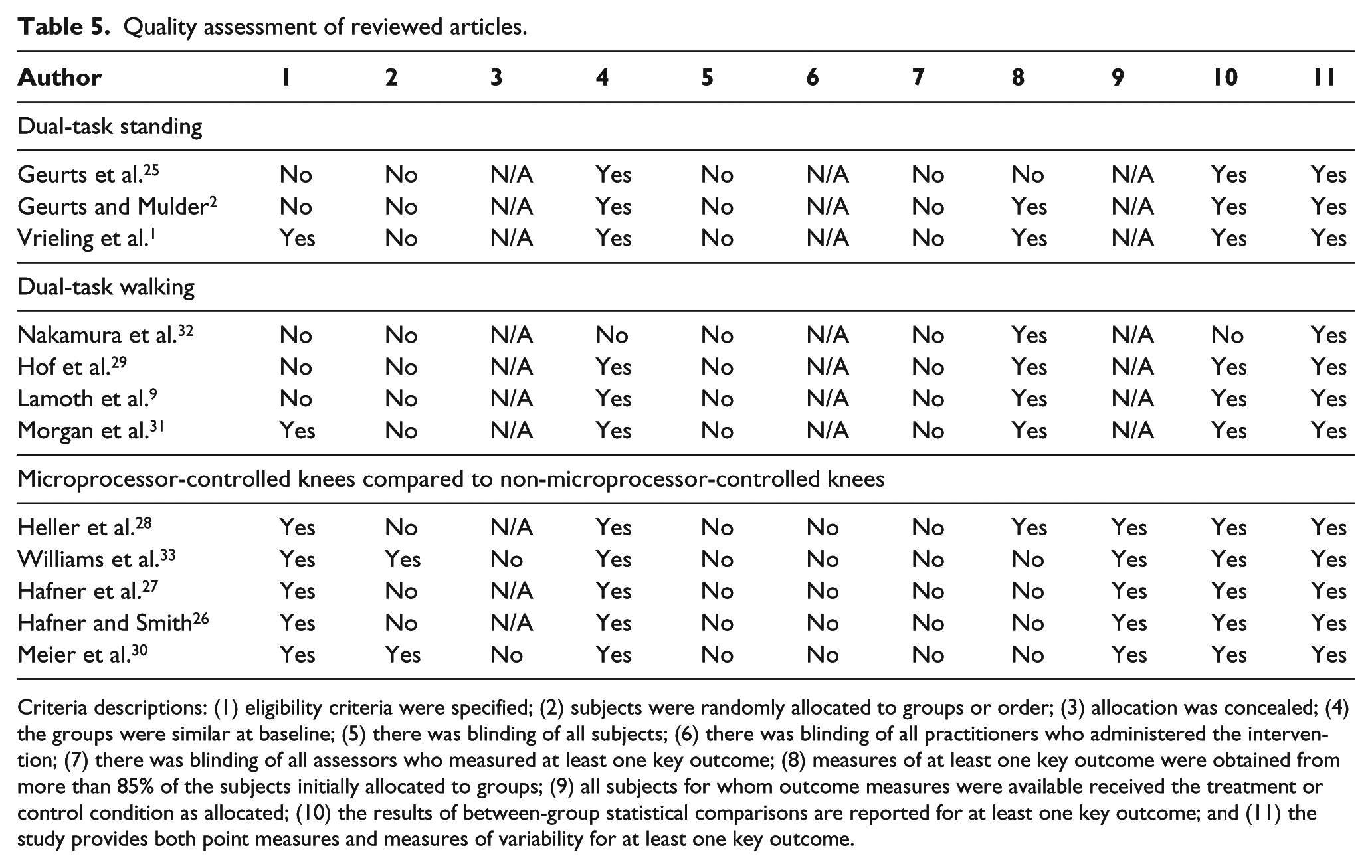
Criteria descriptions: (1) eligibility criteria were specified; (2) subjects were randomly allocated to groups or order; (3) allocation was concealed; (4) the groups were similar at baseline; (5) there was blinding of all subjects; (6) there was blinding of all practitioners who administered the intervention; (7) there was blinding of all assessors who measured at least one key outcome; (8) measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; (9) all subjects for whom outcome measures were available received the treatment or control condition as allocated; (10) the results of between-group statistical comparisons are reported for at least one key outcome; and (11) the study provides both point measures and measures of variability for at least one key outcome.
Results
In total, 12 articles1,2,9,25–33 met the stated eligibility criteria (Figure 1). Results from these 12 articles (11 studies) were grouped into three categories: dual-task standing, dual-task walking, and effects of microprocessor-controlled prostheses on dual-task walking (Tables 2–4). Seven studies compared dual-task standing and walking performance in people with and without LLA to test the hypothesis that people with LLA have greater dual-task interference (i.e. diminished performance on the postural and/or cognitive task in dual-task compared to single-task conditions) than people without LLA. Four studies (five articles) compared dual-task performance in people with LLA using microprocessor-controlled and non-microprocessor-controlled knees to test the hypothesis that microprocessor-controlled knees mitigate dual-task interference to a greater extent than non-microprocessor-controlled knees.
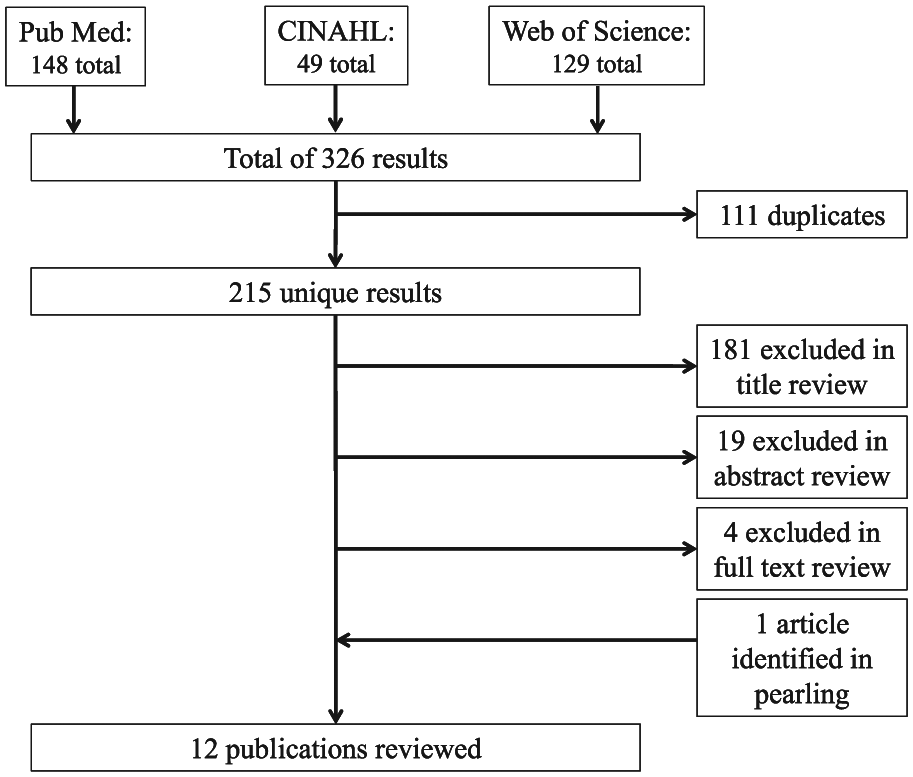
Schematic of search strategy and results. Search was performed on 5/30/2017.
Dual-task standing in people with LLA compared to controls
Study and sample characteristics
Three observational studies1,2,25 examined the effects of a concurrent cognitive task on postural control during quiet and perturbed standing tasks in a total of 28 people with LLA. Two2,25 examined longitudinal changes in dual-task standing throughout a period of post-amputation rehabilitation and one 1 assessed cross-sectional differences in standing under single- and dual-task conditions between people with and without LLA. Sample characteristics varied greatly both within and across the studies. All three included small samples of 8–12 people with LLA. Samples in each study varied in age, amputation level, time since amputation, prosthetic componentry, and etiology of amputation. One study 25 included an age- and sex-matched control group, one included a non-matched control group, 1 and one included both matched and non-matched controls. 2 While participants’ cognitive status was not reported in any of the studies, individuals with significant memory and attention deficits were excluded from two studies.2,25 Notably, investigators did not describe how memory and attention were assessed nor did they describe the number of individuals who were excluded based on these criteria.
Methods
Dual-task standing studies varied in terms of the postural control and cognitive tasks used in each. Standing postural control tasks included quiet standing on a stable surface,2,25 weight shifts in response to visual targets, 2 and standing on a surface that moved in a rhythmic, predictable manner. 1 Standing task performance was quantified using measures of postural sway (e.g. root mean square of the center of pressure displacement and velocity)1,2,25 and weight-bearing symmetry. 1 Cognitive tasks were either mental tracking tasks (e.g. mathematical functions2,25) or discrimination and decision-making tasks (e.g. choice reaction time tests using visual 25 and acoustic 1 stimuli). One study 25 used two cognitive tasks—the majority of participants were administered the visual Stroop, a discrimination and decision-making task, but participants who were unable to discern colors were tested with serial subtraction, a mental tracking task. All three studies assessed standing postural control under both single- and dual-task conditions. Two2,25 assessed cognitive performance under both single- and dual-task conditions and one 1 did not report cognitive task performance results. None of these studies clearly stated whether instructions to focus on the cognitive task or on the postural task were provided.
Results
Two studies2,25 investigated the effects of a concurrent cognitive task on postural sway in quiet standing in people with LLA and controls. Both studies described significantly greater dual-task relative to single-task sway in people with LLA at the start of rehabilitation compared to controls and found that people with LLA showed significant improvements in postural sway in either the sagittal2,25 or coronal 25 direction in the dual-task condition over a period of rehabilitation. However, significant changes in dual-task interference (defined as dual-task minus single-task) in coronal postural sway were only reported in one study. 25
Two studies1,2 investigated the effects of a concurrent cognitive task on postural control in complex standing conditions: visually guided weight shifting 2 and standing on a rhythmically moving surface. 1 Neither reported statistically significant differences in single-task relative to dual-task standing between people with LLA and controls. One 2 described fewer weight shifts and more cognitive task errors in people with LLA compared to non-matched controls. The other 1 did not report significant group differences in dual-task relative to single-task postural control performance when standing on a moving platform.
All three studies reported that standing postural control was significantly worse in people with LLA, regardless of single-task or dual-task condition. No significant between- or within-group differences 25 or group-by-task interactions 2 were observed for cognitive task performance.
Dual-task walking in people with LLA compared to controls
Study and sample characteristics
Four cross-sectional, observational studies9,29,31,32 examined dual-task walking in people with LLA compared to controls. Samples were small, with a total of 39 participants with LLA across all studies. Participant characteristics, such as amputation level, differed between studies. One study 32 included participants with LLA at the hip, transfemoral, and transtibial levels, along with non-matched controls. The other studies9,29,31 included participants with transfemoral amputation and controls matched by sex and either age9,31 or leg length. 29 Participants in all four studies varied with respect to time since amputation and age. The majority of participants had LLA secondary to trauma, however, etiology was not reported in two studies.29,32 Participants with LLA had statistically lower Montreal Cognitive Assessment (MoCA) scores than controls in one study. 31 Assessment of cognitive function was not described in the other studies.9,29,32
Methods
The four dual-task walking studies varied in their methodological approaches. One 32 described the effects of walking on cognitive task performance (i.e. reaction time) to characterize the relative cognitive demand of walking in people with and without LLA. Unlike other studies in this review, the investigators did not quantify postural or walking task performance. In addition, they did not conduct statistical analyses to compare dual-task outcomes between participants with LLA and controls. The other three walking studies9,29,31 investigated the effects of a concurrent cognitive task on walking performance (e.g. speed, gait variability). The choice of cognitive tasks varied across studies and included a mental tracking task (serial subtraction 9 ) and discrimination and decision-making tasks (visual 29 and auditory 31 versions of the Stroop test). Walking tasks were performed at self-selected speeds either on a level surface9,31 or on a treadmill. 29 Each study included three or more walking outcomes collected with various equipment such as a triaxial ambulant accelerometer, 9 an instrumented treadmill, 29 and a three-dimensional (3D) motion capture system. 31 Walking outcomes differed across studies and included measures of pace (i.e. walking speed9,31 and stride time9,31), asymmetry (i.e. percent time spent in stance phase and double-contact 29 and step time asymmetry 31 ), and postural stability (i.e. step or stride width,29,31 stride time coefficient of variation, 9 margin of stability, 29 mediolateral and anterior–posterior trunk acceleration, 9 local stability exponent, 9 and sample entropy 9 ). Three9,29,32 of the four studies did not describe directing participants to focus on either the walking task or the cognitive task in dual-task conditions, leaving open the possibility that participants prioritized different tasks.
Results
Walking study results were challenging to synthesize due to differences in study objectives and/or outcomes of interest. One study 32 that described the effect of walking on cognitive task performance reported that both people with LLA and controls showed a significant increase in reaction times when walking compared to standing. Statistical differences in the relative cognitive demand associated with walking between people with LLA and controls were not described in this study, despite inclusion of a non-matched control group. The investigators also reported reaction time in people with LLA by level of amputation. They found that reaction times were generally longer in people with higher levels of amputation in standing and all phases of stepping. However, the investigators did not statistically compare reaction times by group and they noted that there was high variability in performance among participants with LLA.
Overall, results from the three other studies showed that a concurrent task did not affect walking in people with LLA more than in controls. Investigators noted differences in walking performance between people with and without amputation across pace, asymmetry, and postural stability outcomes, though, importantly, walking performance was not differentially affected by the addition of a concurrent task. In other words, walking performance was consistently worse in people with LLA in both single-task and dual-task conditions. When a statistically significant decline in walking performance between single-task and dual-task conditions was measured for people with LLA, a similar decline was noted in controls. For studies9,31 that reported cognitive task outcomes, performance did not decline to a greater extent in people with LLA compared to controls, suggesting that dual-task interference was comparable between groups.
Self-report
One 31 of the four walking studies assessed participants’ self-report of attentional demands while walking. All 14 of the participants reported the need to “pay attention” while walking. The most common situations that required attention were walking on icy or slippery surfaces, over uneven terrain, downstairs, in sand, or in snow. This study did not compare self-report data from participants with and without LLA.
Effects of microprocessor-controlled prostheses on dual-task walking in people with LLA
Study and sample characteristics
Four longitudinal intervention studies (described in five articles26–28,30,33) compared the effects of microprocessor- and non-microprocessor-controlled knees on dual-task walking in people with transfemoral amputation. Each of these studies used within-participant designs, meaning that participants were exposed to all experimental conditions and served as their own controls. Three28,30,33 studies used a before-and-after design, and the fourth study26,27 (described in two articles) used a reversal design.
Sample sizes for these studies ranged from 8 to 17 participants, with a total of 47 participants across all studies (two articles26,27 described the same sample of 17 people). Three26,27,33 of the five articles reported attrition rates, which ranged from 19%26,27 to 56%. 33 All samples were homogeneous with respect to level of amputation, with all participants having amputations at the knee disarticulation or transfemoral levels. Participants across studies were heterogeneous with respect to age and etiology, with the majority of participants experiencing amputation secondary to trauma (25 of 39 participants, 8 not reported).
Methods
Each study compared dual-task performance when participants wore microprocessor-controlled knees or non-microprocessor-controlled knees to determine if microprocessor-controlled prostheses improved dual-task walking performance in participants with transfemoral amputation (TFA). Three26,27,30,33 of the four studies included the Otto Bock C-Leg (Ottobock, Duderstadt, Germany), a prosthetic knee with microprocessor control of both stance and swing phases of gait. The C-Leg uses sensors in the knee and pylon to inform rapid changes to the knee flexion and extension resistance. 18 The remaining study 28 included the Intelligent Prosthesis, a single-axis hydraulic knee with microprocessor control of swing phase only. As such, the Intelligent Prosthesis knee functions similarly to most non-microprocessor-controlled knees in stance when stability is most crucial. 34 The types of non-microprocessor-controlled knees used for comparisons were standardized in three28,30,33 of the four studies. Comparison knees included a single-axis knee with pneumatic swing control, 28 a polycentric knee with hydraulic swing control, 30 and a single-axis knee with hydraulic stance and swing control.30,33 The remaining study26,27 used participants’ current non-microprocessor-controlled knee as the comparison condition. All investigators standardized the prosthetic socket between conditions, randomized the order of knee allocation, and provided accommodation periods for each prosthetic knee condition from 4 to 32 weeks.
Walking conditions and outcomes varied across the prosthetic knee studies. The dual-task walking conditions included walking on a treadmill, 28 walking an indoor hallway, 33 walking an outdoor sidewalk,26,27 and traversing a standardized obstacle course with different terrain qualities. 30 Walking outcomes included measures of pace (i.e. self-selected walking speed26,27,33 or time to complete an obstacle course 30 ), postural stability (i.e. overall sway 28 ), and movement efficiency (i.e. total heart beat index 30 ). Four26–28,33 of the five articles did not report measurement of single-task performance on the walking tasks. The choice of cognitive task also varied and included a working memory task (reading numbers on a screen 28 ), a discrimination and decision-making task (visual Stroop test 28 ), a verbal fluency task, 33 and mental tracking tasks (i.e. serial subtraction30,33 and backward digit span26,27). None of the articles described measurement of single-task performance on the cognitive task or provided instructions for focus in the dual-task condition. One article 30 did not report dual-task cognitive performance.
Results
Of the four studies, only one 26 found that performance of a concurrent task differentially affected walking performance when using different knee components. The study showed that walking speed significantly increased while walking in dual-task conditions using the microprocessor-controlled knee compared to non-microprocessor-controlled knees, and that this increase was most evident in people who were categorized as limited community ambulators (i.e. those classified as Medicare Functional Classification Level K2). Another study 30 reported that the use of a microprocessor-controlled knee resulted in lower movement efficiency in dual-task relative to single-task walking. However, this difference is likely within the error of the measure and may not be clinically meaningful. There were no other significant differences reported based on measures of pace27,33,30 or postural stability. 28 No significant differences between non-microprocessor- and microprocessor-controlled knees were found in studies that reported cognitive task performance.26–28,33
Only one 30 study assessed walking over challenging terrain. The obstacle course used in this study may reflect walking conditions most affected by the features of a microprocessor-controlled knee with stance control. 35 Surprisingly, the investigators 30 reported trends toward dual-task improvements in walking across all knee conditions, which potentially reflected an arousal effect. Order effects may also explain these results, as single-task walking through the obstacle course always preceded dual-task walking.
Self-report
Three of the five articles26,27,33 used self-report surveys to assess the need to concentrate on walking and difficulty completing concurrent tasks while walking between knee conditions. Participants were asked about attention given to the walking and cognitive tasks during the research session 33 and administered questions assessing average cognitive burden in their daily lives.26,27,33 Results showed that participants reported significant reductions in attention during walking26,27,33 and average cognitive burden 33 in the microprocessor-controlled knee condition, relative to the non-microprocessor-controlled knee.
Discussion
The aim of this review was to examine evidence related to dual-task standing and walking in people with LLA. Based on the studies reviewed, there is some evidence that the dual-task interference in standing is disproportionately greater for people with LLA compared to non-amputees. However, current research does not support the hypothesis that dual-task interference during walking is greater in people with LLA compared to controls. Cognitive demand did not increase during walking in people with LLA compared to controls 32 and the addition of a cognitive task did not differentially impact walking.9,29,31
Evidence of heightened dual-task interference in standing, but not walking, in people with LLA is surprising given that greater interference was expected as postural tasks became more challenging. 19 One potential reason for this discrepancy is the difference in participant characteristics in these studies. In the two studies that found heightened dual-task interference for people with LLA in standing postural control, 63% 25 and 75% 2 of the participants reported vascular amputation etiology and the mean ages of 67.7 25 and 59.4 2 years. In comparison, fewer than 13% of participants with LLA reported vascular etiology in studies that did not find heightened dual-task interference in walking, and participants’ mean ages were between 40 and 54 years.1,9,31 It should be noted that the etiology of amputation29,32 and mean age 32 were not reported in several walking studies. Future studies could compare younger and older people with LLA or people with different etiologies (e.g. dysvascular and traumatic) to assess differences in dual-task interference that may be due to age and cause of amputation.
Among the four studies that examined the effects of microprocessor-controlled compared to non-microprocessor-controlled knees on dual-task walking, only one 26 provided evidence of improved dual-task walking performance in the C-Leg microprocessor-controlled knee compared to non-microprocessor-controlled knees. This study also provided evidence that the use of this technology may be most beneficial to people with LLA who are limited community ambulators (i.e. Medicare Functional Classification Level K2). The group of limited community ambulators who demonstrated improvements in dual-task walking were older (mean age 57.1 years) than those classified as unlimited community ambulators (i.e. Medicare Functional Classification Level K3, mean age 41.9 years). Mean age of the limited community ambulators in this study was also higher than that of participants (mean ages from 38 to 49 years) in other studies that assessed the dual-task walking performance in microprocessor- and non-microprocessor-controlled knees. Results from this study suggest that people with LLA who have heightened mobility limitations and/or older age have reduced dual-task interference when wearing microprocessor-controlled knees than when wearing non-microprocessor-controlled knees.
While there was little evidence that dual-task walking performance was worse in people with LLA or mitigated by the use of microprocessor-controlled knees, the studies26,27,31,33 that measured self-report outcomes in addition to performance outcomes contradicted performance evidence and suggests a need for greater concentration for walking in people with LLA. One study 31 that examined dual-task walking in people with and without LLA found that participants with transfemoral amputation reported heightened attention in walking and that this heightened attention was most commonly experienced in challenging walking conditions (e.g. icy or slippery surfaces, uneven terrain). Studies26,27,33 that examined dual-task performance of participants with transfemoral amputation found that participants reported significant reductions in the difficulty of dual-task walking26,27,33 and cognitive burden 33 when using a microprocessor-controlled knee outside the laboratory. These results demonstrate the value of collecting both self-report and performance-based data when assessing the role of attention in postural control and may suggest the need to assess dual-task walking in challenging or unpredictable walking conditions that better reflect home and community environments.
Recommendations for future dual-task standing and walking research in people with LLA
The small number of studies identified in this review suggests that dual-task research in people with LLA is in its infancy. Additional high-quality research is needed to understand the effects of a concurrent task on standing or walking in people with LLA, and it is critical that future research builds upon previous work to effectively inform our understanding of dual-task postural control in people with LLA.
Sample sizes and characteristics
Studies included in this review had small samples that were heterogeneous with respect to important patient characteristics (e.g. age, etiology of amputation, and mobility limitations). Sample sizes ranged from 6 to 17 participants and investigators rarely described calculating sample size a priori. Studies with small samples have the potential to be underpowered, meaning that results may not be statistically significant even in cases where a true difference between groups or conditions exists.
A second consideration related to sample selection is the ability to generalize study findings to the larger LLA population. Among people with major LLA, the estimated prevalence of amputation due to dysvascular reasons is approximately 80%. 36 However, people with dysvascular amputation comprised only 53% of participants in the dual-task standing studies, 9% of participants in the dual-task walking studies, and 5% of the participants in prosthetic knee studies. In addition, epidemiological studies report that 67% of people with transtibial amputation and 85% of people with transfemoral amputation use assistive devices for walking outside of their home, 15 and 42% of people with LLA are over the age of 65. 36 In contrast, none of the reviewed studies included participants that required assistive devices during data collection, and only one study 25 reported mean participant ages over 65 years. Thus, participants in existing dual-task studies do not well represent the predominant etiology, functional ability, or age of the general population of people with LLA. Future dual-task research that intends to generalize results to the overall LLA population should therefore attempt to recruit samples that are representative in terms of amputation etiology, mobility limitations, and age. These is also a need for research that assesses whether dual-task walking differs in subgroups defined by these characteristics to better understand whether certain people with LLA are more affected by the addition of a concurrent task than others.
Methodological considerations specific to dual-task research
Overall quality of research methods in this area varied across studies. In addition, variations in methodological approaches across studies make interpretation of the overall evidence challenging. The lack of assessment of postural and/or cognitive task performance under both single-task and dual-task conditions makes it difficult to determine patterns of interference. Only three studies2,25,31 included in this review reported single-task and dual-task performance for both the postural and cognitive tasks. If the postural and cognitive single-task and dual-task data are not reported, potential trade-offs between the postural task and the concurrent cognitive or motor task cannot be assessed and results may be misinterpreted.
A second key methodological consideration is the instructions provided to participants under dual-task conditions. Only two studies25,31 noted instructions requesting that study participants prioritize either the postural or the cognitive task in dual-task conditions. When instructions for prioritization are not provided, some participants may prioritize the postural task, thus experiencing no change in the postural task and dual-task interference in the cognitive task. Others may prioritize the cognitive task and experience dual-task interference in the postural task and no change in the cognitive task. Collectively, this data set may appear to show no dual-task interference across tasks, when in actuality interference just presented differently based on participants’ task prioritization. While instructions for prioritization are not always considered to be ecologically valid, their provision mitigates the concern that study participants prioritize the postural and cognitive tasks differently. 23 Future dual-task research protocols should measure and report outcomes on both the postural and cognitive tasks in both single- and dual-task conditions. In addition, instructions for task prioritization should be provided and reported in order to adequately assess potential dual-task interference.
Postural task choice and outcome measures
Walking studies in this review examined relatively simple walking tasks performed overground or on a treadmill, but it is possible that flat, level walking is not sufficiently challenging to reveal differences in postural control between groups (e.g. people with LLA and controls, people using microprocessor- and non-microprocessor-controlled knees). People with LLA typically adapt well to simple, predictable walking tasks but they lack reliable prosthetic-side sensory inputs or motor outputs. These sensorimotor structures are crucial for adapting gait during more complex or unpredictable walking tasks, such as walking over uneven surfaces, negotiating slopes, and recovering from trips or slips. 19 Because the experimental conditions (e.g. level ground walking) used in the reviewed studies do not represent the situations that are most challenging for people with LLA, 31 it is possible that dual-task interference was minimal or not present. Future work should consider assessing dual-task walking over challenging or unpredictable surfaces that may more closely reflect a variety of daily walking tasks.
Another explanation for discrepancies between performance and self-report measures noted in this review is that outcome measures used to assess dual-task interference are not sensitive enough to detect differences in dual-task performance. There is evidence that suggests that measures such as residual standard deviation, 37 functional near-infrared spectroscopy (fNIRS), 38 or psychophysiological measures 39 may be more sensitive to changes associated with the addition of a concurrent task than the performance measures used most often in this body of research. Furthermore, processing speed may be more sensitive to the addition of a dual-task than postural outcomes and other cognitive task outcomes (e.g. error rate). Future research in this area could consider instructing participants to focus on the postural task while concurrently measuring processing speed on a simple reaction time task to measure difference in cognitive demand related to the postural task.
Another potential direction for measurement of dual-task interference in people with LLA is through development of improved self-report instruments. While self-report results have consistently found significant differences in microprocessor-controlled and non-microprocessor-controlled knees, instruments used to date have little evidence of psychometric testing in people with LLA.26,27,33 Additional testing of existing instruments or development of new psychometrically sound self-report instruments that assess cognitive control of standing and walking tasks may help investigators to understand the role of cognition in the control of balance and walking in people with LLA, both within laboratory and real-world environments.
Clinical implications
Since there is little definitive evidence of differential dual-task decline in previous research, one might speculate that people with LLA do not require heightened cognitive control for postural tasks, particularly walking. There is also little evidence to support the assertion that microprocessor-controlled knees can reduce the cognitive control required for walking tasks in people with LLA. However, self-reported data from survey research15,16 and three26,27,31,33 studies included in this review suggest that people with LLA perceive a need to concentrate on walking. Furthermore, methodological issues such as small samples, heterogeneous study populations, variations in choice of concurrent tasks, and critical limitations in the application of dual-task methods may limit the ability to conclude that people with LLA do not require heightened cognitive control for postural tasks.
Limitations of this review
This review was limited to peer-reviewed articles. Thus, emerging studies that have been disseminated as abstracts, dissertations, or theses and are not yet available as peer-reviewed articles are not included. Furthermore, the search strategy used would not identify studies that included a dual-task, but did not discuss this aspect of the study in their abstract or keywords. Finally, few studies were identified and results could not be synthesized in a meta-analysis due to heterogeneity in research aims, sample characteristics, and measured outcomes.
Conclusion
The relatively few studies assessing dual-task standing and walking in people with LLA suggest that little is known about interactions between cognition and postural tasks in this population. Definitive conclusions about the allocation of cognitive resources during standing and walking in people with LLA cannot be drawn due to small samples, sample heterogeneity, and variation in methods used in dual-task studies to date. To build upon current evidence, future research should estimate sample sizes using data from studies included in this review. Participants should be recruited to better represent the population of people with LLA, particularly with regard to important patient characteristics (e.g. amputation etiology) that are likely to affect dual-task performance. Investigators should also consider alternative techniques like standardized self-report measures and neural imaging to assess dual-task standing and walking in people with LLA.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.