
Abstract
Background:
Low back pain is a common secondary disabling condition in the transfemoral amputee population. Transfemoral amputees are at risk of excessive lumbar lordosis; it has been suggested that increased lumbar lordosis may be associated with low back pain. However, the relationship between lumbar lordosis angle and low back pain has not yet been studied in this population.
Objective:
To determine whether the extent of lumbar lordosis is associated with low back pain in transfemoral amputees.
Study design:
Case–control observational study.
Methods:
Participants included eight transfemoral amputees without low back pain and nine transfemoral amputees with low back pain. Etiology of amputation was primarily trauma. All participants underwent lateral view radiographs of the lumbar spine, from which lumbar lordosis angle and sacral inclination angle were measured.
Results:
Lumbar lordosis angle mean ± standard deviation was 46.1° ± 12.4° in participants with low back pain and 51.0° ± 12.6° in those without. Sacral inclination angle mean ± standard deviation was 38.3° ± 8.7° in participants with low back pain and 39.1° ± 7.5° in those without. There was no significant difference in lumbar lordosis angle or sacral inclination angle between participants with and without low back pain.
Conclusion:
This study suggests that increased lumbar lordosis angle and sacral inclination angle are not significantly associated with low back pain in transfemoral amputees of a primarily traumatic etiology.
Clinical relevance
Low back pain (LBP) is a common, disabling condition in transfemoral amputees. In the clinical setting, increased lumbar lordosis is implicated in LBP. This study does not support an association between increased lumbar lordosis and LBP; further study is needed to understand the increased prevalence of LBP in this population.
Keywords
Background
Lower extremity amputation affects more than 600,000 people in the United States 1 and is associated with substantial functional limitations.2,3 Secondary disabling musculoskeletal conditions such as low back pain (LBP) are increasingly being recognized as an important source of additive disability. LBP is extremely common in those with lower extremity amputation with a 1-month prevalence that varies between 64% and 71%3,4 compared to a 1-month prevalence of 23% in the general population. 5 About half of lower extremity amputees with LBP report this pain as either moderate or severe in intensity,3,6 and it is often reported to be the most bothersome pain symptom. 4 Furthermore, LBP is associated with lower physical health-related quality of life and more severe disability in amputees. 2 Although some studies do not show a difference in LBP by amputation level,2,6 others suggest that transfemoral amputees have a higher prevalence of LBP than transtibial amputees,4,7 as well as more intense and bothersome pain. 4 Despite its greater prevalence and associated disability, the underlying etiology of LBP in transfemoral amputees has received insufficient study to date.
The etiology of LBP is often multifactorial, including mechanical, psychological, and social factors. Certain populations are thought to be at an increased risk due to mechanical factors such as increased lumbar lordosis. For example, adolescent female gymnasts with LBP have a significantly greater lumbar lordosis angle (LLA) than those without pain, 8 and an association between LBP and the magnitude of lumbar lordosis in pregnant women has also been identified. 9 Transfemoral amputees are another population in which it has been suggested that increased lumbar lordosis may be associated with LBP. 10 Transfemoral amputees are at risk of excessive static (i.e. postural) and dynamic (e.g. during walking) lumbar lordosis; if the prosthetic socket is not aligned in adequate flexion, a typical requirement for transfemoral prosthetic sockets, 11 or if the hip flexion angle of the socket does not adequately accommodate a patient’s hip flexion contracture, this can result in increased anterior pelvic tilt and excessive lumbar lordosis. 12
The association between the extent of lumbar lordosis and LBP has been extensively studied in the general population with conflicting results. A number of studies have demonstrated an association between LBP and increased lumbar lordosis,13,14 while others have found either no association15,16 or even a reverse association (i.e. subjects with LBP have decreased lordosis compared to those without pain).17,18
In the transfemoral amputee population, there have been extremely limited study measuring outcomes related to lumbar lordosis. Gaunaurd et al. 19 studied pelvic innominate inclination, although this study did not include comparison with a control group and did not assess association with LBP. Friel et al. 20 reported an association between “iliopsoas length” (as measured by the Thomas test) and LBP. However, the relationship between LBP and direct measurements of lumbar lordosis in individuals with lower extremity amputation has not been previously studied. We hypothesize that LBP in transfemoral amputees is associated with increased postural LLA.
Methods
The Institutional Review Board at VA Puget Sound Health Care System approved this study. Study participants were prospectively recruited from a local amputee database and through private sector and Veterans Administration amputee/prosthetic clinics. Inclusion criteria were being over 18 years of age and less than 65 years of age; having been fit with a prosthesis and having used a prosthesis for at least 2 years; wearing the prosthesis for at least 8 h per day; being able to walk at least 150 ft without the use of upper extremity aids; having a comfortable prosthesis; and having a history of no significant falls within the previous 6 months. Exclusion criteria were etiology of amputation being tumor with active disease or ongoing treatment; cognitive status or language function that was inadequate to participate; significant lower extremity pain condition or other neurological condition that would interfere with gait; onset of back pain prior to amputation; or significant depression (CES-D score ⩾16). 21
Participants that met the general inclusion and exclusion criteria were divided into two groups based on self-report of LBP. Participants who answered “yes” to the question, “Since your amputation have you experienced persistent, bothersome back pain?,” were placed in the LBP group, while participants who answered “no” were placed into the group without LBP.22,23 The pain levels of all participants were further characterized using the Chronic Pain Grade questionnaire to rate their current pain intensity and their average pain intensity over the previous 3 months on a scale from 0 (“no pain”) to 10 (“pain as bad as could be”). The Chronic Pain Grade questionnaire has previously been shown to be a reliable and valid tool for measuring chronic pain 24 and has been used in previous studies of pain in the amputee population. 25
A series of questionnaires was utilized to provide a demographic description of the two groups and to identify potentially confounding variables. This included age, gender, current height and weight. Body mass index (BMI) was calculated as body weight in kilograms divided by the square of height in meters. 26 Smoking history was measured by pack-years, which was defined as the maximum number of cigarettes smoked per day multiplied by the number of years smoked. 27 Psychological well-being was assessed using the Mental Health Scale of the SF-36. 28 The 24-item Roland-Morris Disability Questionnaire was used to assess physical disability related to LBP. 29 The Charlson Co-Morbidity Index was utilized to measure general medical status. 30
Each subject underwent a lateral view radiograph of the lumbar spine during static standing while wearing their prosthesis. Conventional radiologic techniques were used. On the radiographic film, lines were drawn tangential to the superior endplate of L1 and the inferior endplate of L5. Lines were then drawn perpendicular to these endplate lines and the acute angle formed by their intersection was the LLA (primary outcome measure, Figure 1), using methodology described previously. 31 The sacral inclination angle (SIA, secondary outcome measure), which is a measure of pelvic tilt and is often studied in association with the LLA,16–18 was also measured; a line was extended from the superior endplate of S1 to the edge of the film, which, on our upright films, was perpendicular to the ground. The acute angle formed from the intersection of the line with the edge of the film defined the SIA (Figure 1). These angles were measured using a hand-held goniometer to the nearest degree by an orthopedic spine surgeon, who was blinded to pain status. Intra-rater reliability for radiographic assessment of lumbar lordosis measurement has been shown to be excellent (intraclass correlation ranged from .90 to .95 for different observers) and for pelvic tilt measurement has been shown to be moderate (intraclass correlation ranged from .70 to .74 for different observers). 32
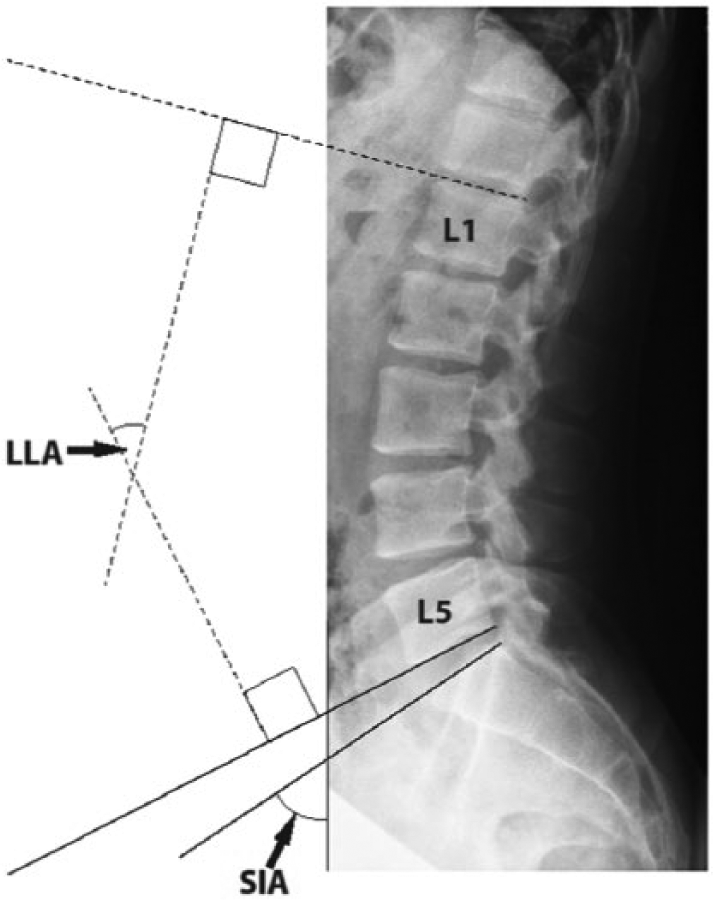
Standing lateral view radiograph of the spine and pelvis showing the methodology for measurements of lumbar lordosis angle (LLA) and sacral inclination angle (SIA).
Wilcoxon rank sum tests were used to determine whether demographic and potentially confounding variables differed between those with and without LBP. Differences in LLA and SIA between these groups were assessed using two sample t-tests with significance set at p = .05. Statistical analyses were carried out using R version 3.3.2.
Results
A total of 203 individuals with transfemoral amputation were available for recruitment. Eighty three were excluded because they did not reside within the local geographic area. Letters were sent to those remaining to determine whether they would agree to be contacted by telephone by a research coordinator. Forty could not be contacted, 31 replied that they did not wish to be contacted, 18 did not wish to participate after being contacted, 7 were ineligible to participate, 4 had died, and 20 individuals were enrolled after initial screening. Three of these individuals were subsequently excluded due to exclusionary criteria on further screening. Seventeen participants completed the data collection protocol. Of these, nine were placed in the LBP group and eight were placed in the group without LBP based on the criteria described above. All participants were male. Of the amputations in the group with LBP, six were due to trauma, one to tumor, one to vascular disease and one to congenital causes. In the group without LBP, all amputations were due to trauma. In the LBP group, the mean pain intensity at time of study ± standard deviation (SD) was 4.3 ± 2.0 and the mean pain intensity over the previous 3 months ± SD was 4.8 ± 1.8. The group without LBP reported pain intensity of 0 at the time of the study and over the previous 3 months.
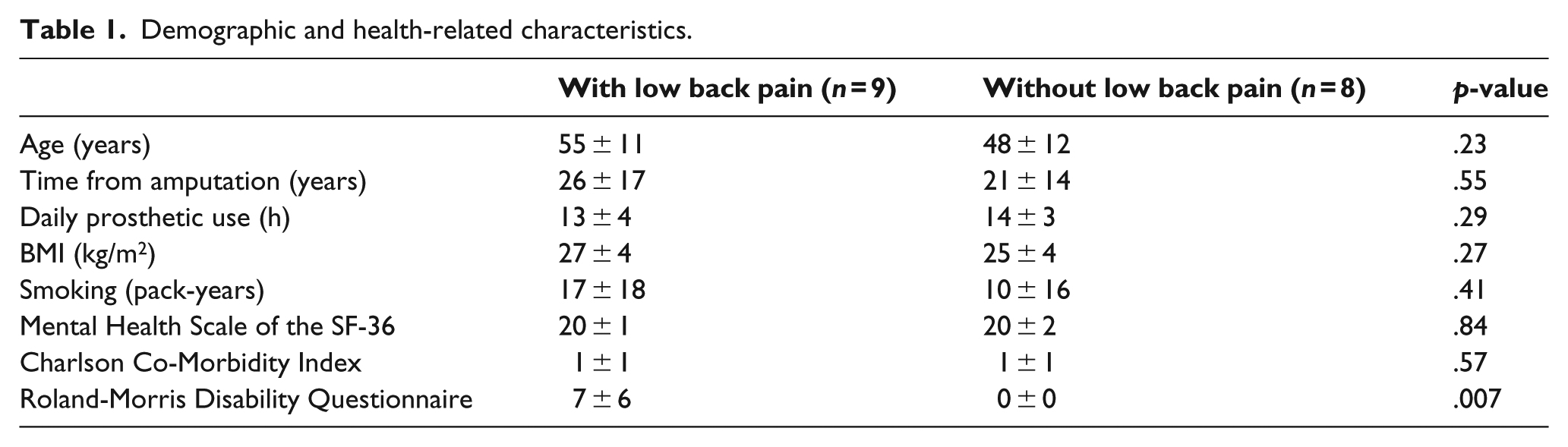
Table 1 includes the demographic and potentially confounding variables for both groups, including the age, time since amputation, daily prosthetic use, BMI, smoking history, Mental Health Scale of the SF-36, Roland-Morris Disability Questionnaire, and Charlson Co-Morbidity Index. There were no significant differences between groups in any of these measures except for the Roland-Morris Disability Questionnaire, where the LBP group had a mean score of 7 and the group without LBP had a mean score of 0.
Demographic and health-related characteristics.
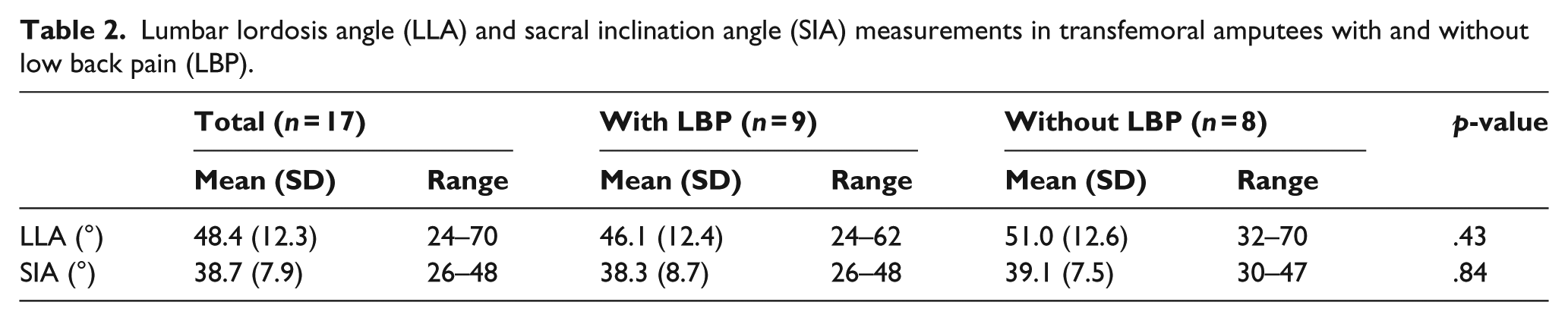
LLA mean ± SD was 46.1° ± 12.4° in participants with LBP and 51.0° ± 12.6° in those without LBP (Table 2). There was no significant difference in LLA between participants with and without LBP (mean difference 4.9°, 95% confidence interval −17.8 to 8.0; p = .43). SIA mean ± SD was 38.3° ± 8.7° in participants with LBP and 39.1° ± 7.5° in those without (Table 2). There was no significant difference in SIA between participants with and without LBP (mean difference .8°, 95% confidence interval −9.3 to 7.7; p = .84). Figure 2 shows a plot of the LLA and SIA for all participants.
Lumbar lordosis angle (LLA) and sacral inclination angle (SIA) measurements in transfemoral amputees with and without low back pain (LBP).
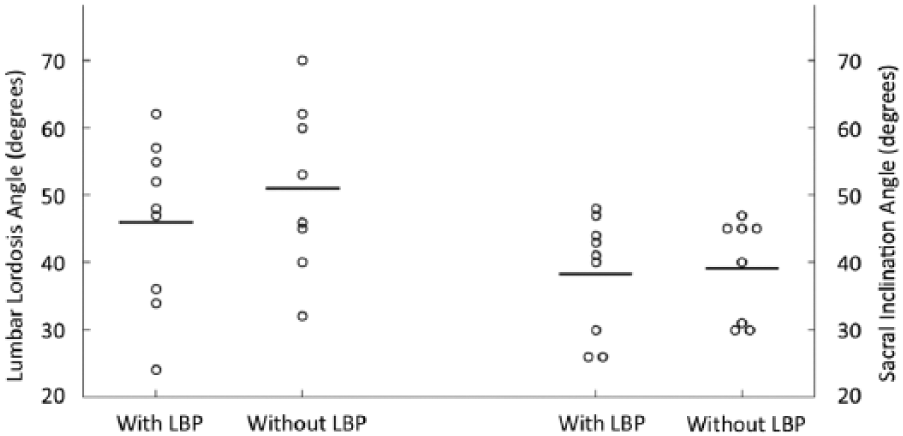
Distribution of lumbar lordosis angle and sacral inclination angle in study participants with and without low back pain (LBP).
Discussion
In spite of the substantially greater prevalence of LBP in the transfemoral amputee population compared with the general population, the underlying cause is incompletely understood. Greater lumbar lordosis has been shown to be associated with LBP in certain populations.8,9 Although greater lumbar lordosis has been suggested as a potential cause of LBP in transfemoral amputees, 10 evidence of this relationship is lacking. In this study, we did not observe a difference in LLA or SIA between transfemoral amputees with and without LBP.
Since other non-mechanical factors such as number of co-morbid medical conditions, 33 depression, 34 smoking history, and BMI 27 have been associated with LBP, we also compared relevant demographic and potentially confounding variables between transfemoral amputees with and without LBP and found no difference between groups in any of these measures except the Roland-Morris Disability Questionnaire on which the LBP group scored significantly higher, as expected.
A wide range of values for lumbar lordosis has been reported in the general population. Using the same methodology as the current study, healthy adult LLA has been reported by Vialle et al. 35 to range from 13° to 69° with a mean of 43° ± 11.2°, while Lin et al. 31 reported LLA of 33.2° ± 12.1°. Similar data have been reported in Turkish coal miners with LBP (LLA of 31.6° ± 9.6°). 36 The LLA values in transfemoral amputees in the current study, both with and without LBP, fall within the broad range reported. However, the mean LLA values in the present study (48.4°) are somewhat higher than those reported for non-amputee participants in prior study, suggesting that transfemoral amputees may have increased LLA’s compared to non-amputees. As with LLA, SIA in the current study are broadly within the range reported in healthy individuals, but with somewhat higher mean values,16,18,31,35 suggesting that transfemoral amputees may have increased anterior pelvic tilt relative to non-amputees.
Biomechanical factors other than increased lumbar lordosis may contribute to the increased prevalence of LBP in this population. Kinematic and kinetic lumbopelvic asymmetries during walking have been hypothesized as an underlying mechanical etiology for the development and maintenance of LBP in those with lower limb amputation. 37 Transfemoral amputees with LBP have greater lumbar spine rotation in the transverse plane during walking than those without LBP, 22 and they also have less spinal intersegmental coordination in the frontal and transverse planes at faster walking speeds. 38 Leg length discrepancy has also been suggested to be a contributing factor to LBP in this population; 39 however, a recent study demonstrated no association between LBP and static or dynamic leg length discrepancy. 23 Other biomechanical factors that have also been suggested to be associated with LBP in the lower extremity amputee population include muscle imbalances and fatigue, 20 postural asymmetries, 19 and greater spinal muscle forces and spinal loads. 40 Alternatively, the increased prevalence of LBP in the transfemoral amputee population may be explained by factors unrelated to biomechanics, such as psychosocial factors, co-morbid painful conditions, and genetics, which are known to have important roles in LBP in the general population and potentially in the transfemoral amputee population.33,41–43
There are potential limitations to this study. Similar to the majority of human participant studies of transfemoral amputees in the literature, the sample size in the current study is relatively small. Although type II error cannot be ruled out, it is worth noting that in the case of LLA and SIA, there was a trend toward a larger angle in transfemoral amputees without LBP when compared to those with LBP, which is the opposite direction of effect than would be expected based on theorized biomechanical links to LBP. Although we did not include investigation of factors that may influence LLA (e.g. socket design, residual limb length), the goal of this study was to assess the relationship between LLA and LBP rather than to assess factors associated with LLA. Furthermore, it is worth noting that the vast majority of participants in this study had transfemoral amputation due to traumatic etiology; the results of this study are not necessarily applicable to those with a dysvascular etiology. Finally, due to the cross-sectional nature of this study, inferences cannot be made about causality. Future longitudinal study, including the addition of dynamic LLA measurement during walking and other functional activities, is deserved to better elucidate causative factors related to the high prevalence of LBP in the transfemoral amputee population.
Conclusion
LBP has been recognized as an extremely common impairment that contributes significantly to overall disability in transfemoral amputees. In individuals with long-standing transfemoral amputation of a primarily traumatic etiology with moderate persistent LBP, no difference in LLA or SIA was identified between those with and without LBP. These findings suggest that increased LLA is not associated with LBP in this population. Future prospectively designed study in a larger group of participants may be helpful to confirm these findings.
Footnotes
Acknowledgements
The contents of this article do not represent the views of the US Department of Veterans Affairs or the United States Government. The authors would also like to thank Jane Shofer, MS for performing the statistical analysis for this study.
Author contribution
Conception and Design: JMC, AS, MO
Analysis and Interpretation: MM, JMC, AS, PS, MO, DM
Data Collection: JMC, AS
Writing the article: MM, JMC, AS, DM
Critical revision of the article: MM, JMC, AS, PS, MO, DM
Final approval of the article: MM, JMC, AS, PS, MO, DM
Statistical analysis: JS.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs Matsumoto, Czerniecki, Suri, and Morgenroth’s participation in this study was funded by VA Puget Sound Health Care System, Seattle, WA. This material is the result of work supported with resources and the use of facilities at the VA Puget Sound Health Care System. Dr Suri is funded by Career Development Award #1IK2RX001515 from U.S. Department of Veterans Affairs Rehabilitation Research and Development Service.