
Abstract
Background:
Prosthetists and orthotists have a responsibility to direct treatment toward enabling their clients to perform desired activities and to facilitate participation of their clients in all areas of life. This may include provision of assistive technologies to help clients meet goals related to participation in sexual activities. To help prosthetic and orthotic students develop competencies in dealing with the sexual health of their future clients, it is necessary to generate knowledge of their own perceived competence and capacity.
Objectives:
To explore prosthetic and orthotic students’ attitudes and competence toward working with sexual health and to evaluate reliability and validity of the Students’ Attitudes Towards Addressing Sexual Health questionnaire.
Study design:
Cross-sectional study.
Methods:
Students enrolled in all three years of an undergraduate prosthetic and orthotic program were requested to complete the Students’ Attitudes Towards Addressing Sexual Health questionnaire (n = 65). Reliability and validity were evaluated using the content validity index and Cronbach’s alpha.
Results:
Students felt unprepared to talk about sexual health with future clients and thought that they would be embarrassed if they raised the issue. No differences were identified between students enrolled in each of the three years of the program and few differences were observed between male and female students. The content validity index values were low but improved as the students’ level of education increased. Internal consistency of the questionnaire was acceptable (α = 0.86).
Conclusion:
Prosthetic and orthotic students are unprepared to address sexual health issues with their future clients. There is a need to provide students with training related to sexual health issues.
Clinical relevance
This study indicates the need for additional education of prosthetic and orthotic students in issues related to sexual health and how to address sexual health issues with clients. Results can be used to develop training programs for students and will serve to improve the sexual health of individuals who receive prosthetic and orthotic services.
Background
Persons with physical disabilities have an interest and desire for sexual expression which often goes unrecognized. A consequence of this is that they often experience low sexual esteem and decreased sexual health (Box 1). 3 Many of the client groups regularly managed by prosthetists/orthotists have been identified as experiencing sexual health problems. These individuals include people who have had a stroke,4,5 individuals with cerebral palsy,6,7 persons with spinal cord injuries,8,9 and those who have undergone an amputation.10–12
Sexual health is defined by the World Health Organization as “a state of physical, emotional, mental and social well-being in relation to sexuality.” Achieving sexual health and wellbeing without fear, discrimination, threat, or violence is recognized as a fundamental human right.1,2
Clients often feel uncomfortable in initiating discussions about sexual issues with health professionals and indicate that they expect the clinician to initiate discussion related to the topic.13,14 Unfortunately, many medically trained professionals are not comfortable in discussing sexual health issues either and discussions related to sexual wellbeing are subsequently neglected. 15 In a survey of amputation team members, including prosthetists, 78% of participants indicated that they had not received any questions about sexuality in the 4 weeks prior to administration of the survey, while 67% reported that they did not address sexuality with their clients. 16 Prosthetists have rated their self-perceived knowledge and ability to recognize sexual problems as “insufficient.” 16
In accordance with the International Classification of Functioning Disability and Health (ICF) model, health professionals have a responsibility to direct treatment toward enabling their clients to perform desired activities and to facilitate participation of their clients in all areas of life.14,17 As providers of assistive technologies, prosthetists/orthotists can play an important role in helping their clients to meet goals related to participation in sexual activities, as a means of maintaining or establishing sexual relationships. Individuals who have undergone an amputation have indicated that the development of prostheses and assistive devices to facilitate sexual activity would improve their sexual life. 18 These could include orthoses to facilitate positioning, 19 limb prostheses specifically for sexuality-related reasons, 20 and cosmetic prostheses to enhance a person’s perceived body image and attractiveness. 12
There are numerous factors that influence the ability of health professionals to address issues related to sexual health. Personal attitudes and beliefs can affect a professional’s level of comfort in addressing sexual health issues, 21 while the level of communicative training received in dealing with sexual health issues has also been demonstrated to affect level of knowledge, conversational skills, recognition of sexual problems, and personal comfort. 14 Failure of health professionals to recognize sexual health issues means that they may remain unresolved.
To develop an educational intervention which will allow prosthetic and orthotic (P&O) students to feel competent and able to assist in improving sexual health for their future clients, it is vital to create knowledge of their own perceived competence and capacity as well as their educational needs in this field. In a recent study of Swedish occupational therapy, physiotherapy, and nursing students, respondents expressed a need for increased sexual health education and improved communication skills regarding sexual health. 22 Interestingly, this study identified differences in attitudes of working with sexual health between students studying in different programs, with occupational therapy and nursing students demonstrating a more positive attitude toward working with sexual health issues than physiotherapy students. Given that P&O students were not included in these or any other studies related to professional attitudes and competencies in sexual health issues, there is a need to explore the topic further. To enable comparisons with students from other professions, it is beneficial if studies involving P&O students utilize the same instrument, Students’ Attitudes Towards Addressing Sexual Health (SA-SH) questionnaire. 22
The aim of this study was to explore P&O students’ attitudes and perceived competence toward working with sexual health in their future profession. Given that psychometrics of questionnaires may differ in various populations, the study also aimed to evaluate the aspects of reliability and validity of the SA-SH questionnaire for P&O students.
Methods
Participants
Of a total of 81 students enrolled in all three years of an undergraduate P&O program, 65 responded to the survey (80%). The sample size was determined by the number of students enrolled in the program, which is the only program educating prosthetists/orthotists in Sweden. All students present at the time of data collection agreed to participate and there were no missing data. The mean age of the participants was 24 years (standard deviation (SD) = 5; range 19–41 years) and most respondents were women (n = 43).
Procedures
The paper-based SA-SH questionnaire, with written information about the study, was distributed during face-to-face lectures to all P&O students enrolled at a Swedish University. The questionnaire was distributed approximately halfway through the academic year, in January 2017. The procedure was chosen to enhance the response rate and avoid low response bias. 23 Prior to receiving the questionnaire, the students were given verbal information concerning the study and were assured that participation was voluntary and confidential. Students had the option to openly decline to answer the questionnaire, to answer the questionnaire, or to hand in the questionnaire unanswered/partly answered.
The SA-SH questionnaire
The SA-SH questionnaire addresses student attitudes toward addressing sexual health issues in their future profession. The SA-SH is composed of 22 items distributed across four domains: present feelings of comfort in addressing sexual health, future working environment, fear of negative influence on future client relations, and educational needs. 22 Items within the questionnaire are to be answered on a Likert-type scale with five options: disagree, partly disagree, partly agree, agree, and strongly agree. Items 9–14 and 16–18 were reversed for analysis as these items were phrased in a negative way compared to all other items. 22 Descriptive questions related to gender, age, and educational level within the program are also included.
Analysis
Descriptive statistics were used to analyze each item within the SA-SH questionnaire. Boxplots were used to show all 22 items for the entire group of respondents in medians, quartiles (25% and 75%), and the lowest and highest values that were not outliers (1.5 × interquartile range (IQR)). The Kruskal–Wallis test was used to determine if differences existed between students enrolled in each of the three years of the program, while a Mann–Whitney test was used to determine differences between male and female respondents.
All analyses were performed in SPSS version 21 (IBM Corp., Armonk, NY, USA). The significance level was set at p < 0.05. When the Kruskal–Wallis test was applied, a Bonferroni adjustment was made to account for multiple comparisons (p < 0.017).
Psychometric testing of the SA-SH questionnaire
The SA-SH questionnaire has been demonstrated as valid and reliable for students representing numerous health care professions22,24 but has not previously been used with P&O students. As a result, some psychometric testing was considered necessary in this pilot study. The psychometric testing of the SA-SH questionnaire for P&O students was conducted by computing the content validity index (CVI) and by investigating internal consistency of items in the questionnaire. The CVI was used to assess the relevance of each item on a four-point scale (1 = extremely relevant, 2 = quite relevant, 3 = slightly relevant, 4 = not relevant). The scale was dichotomized by combining extremely relevant/quite relevant (1 and 2) in one group and slightly relevant/not relevant (3 and 4) in the other group. Relevance recommendations are item-level CVI (I-CVI) >0.78 per item and the sum of the CVI (S-CVI) for each item >0.90.25,26 Reliability, measured as internal consistency, was analyzed using Cronbach’s alpha, with a Cronbach’s alpha of 0.70–0.95 considered as an acceptable range. 27
Ethics
Ethical issues have been considered and informed consent to participate in the study was obtained by answering the questionnaire, after being given verbal and written information regarding the study. The data collected were anonymous to the researcher analyzing the results and no identification, such as name or student identification, was used on the questionnaires. This study does not fall under Swedish law for ethical approval but was approved by the head of the department.
Results
Table 1 presents the number of students and responses per year level. Descriptive results for each item included in the questionnaire are presented for each domain (Figures 1 to 4). In relation to comfortableness (Figure 1), the sex and cultural background of clients appeared to influence how comfortable students felt in discussing sexual health issues. In general, students felt unprepared to talk about sexual health with future clients. The students believed that future clients might feel embarrassed and uneasy if they bought up sexual issues and that such conversations might create a distance between them and their client (Figure 2). They also indicated that they would not take time to deal with client’s sexual issues in their future profession (Figure 2).
Participants, responses received, item-level CVI (I-CVI) variance, sum of the CVI (S-CVI) results, and median values regarding how students scored the relevance of each question.
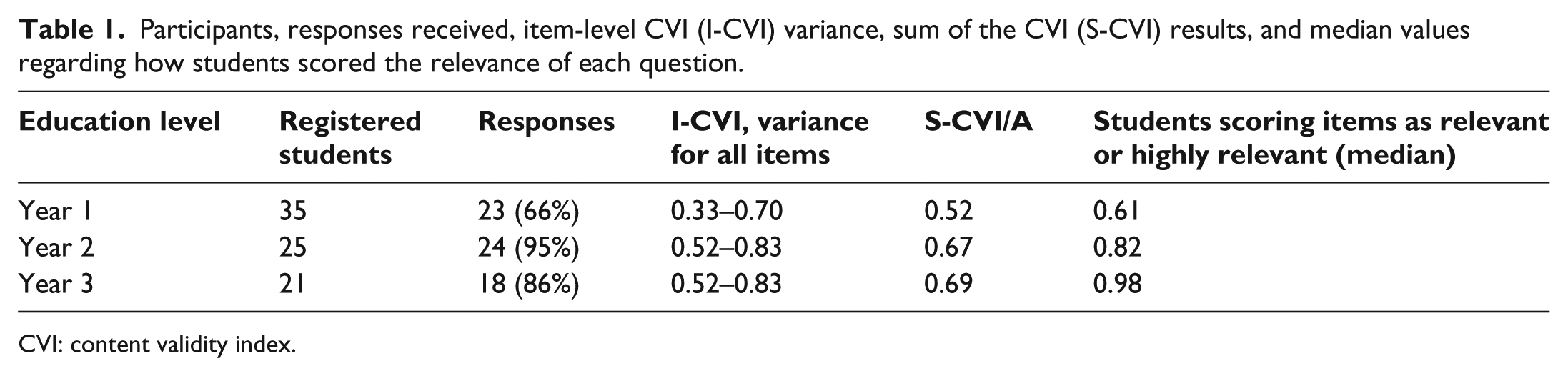
CVI: content validity index.
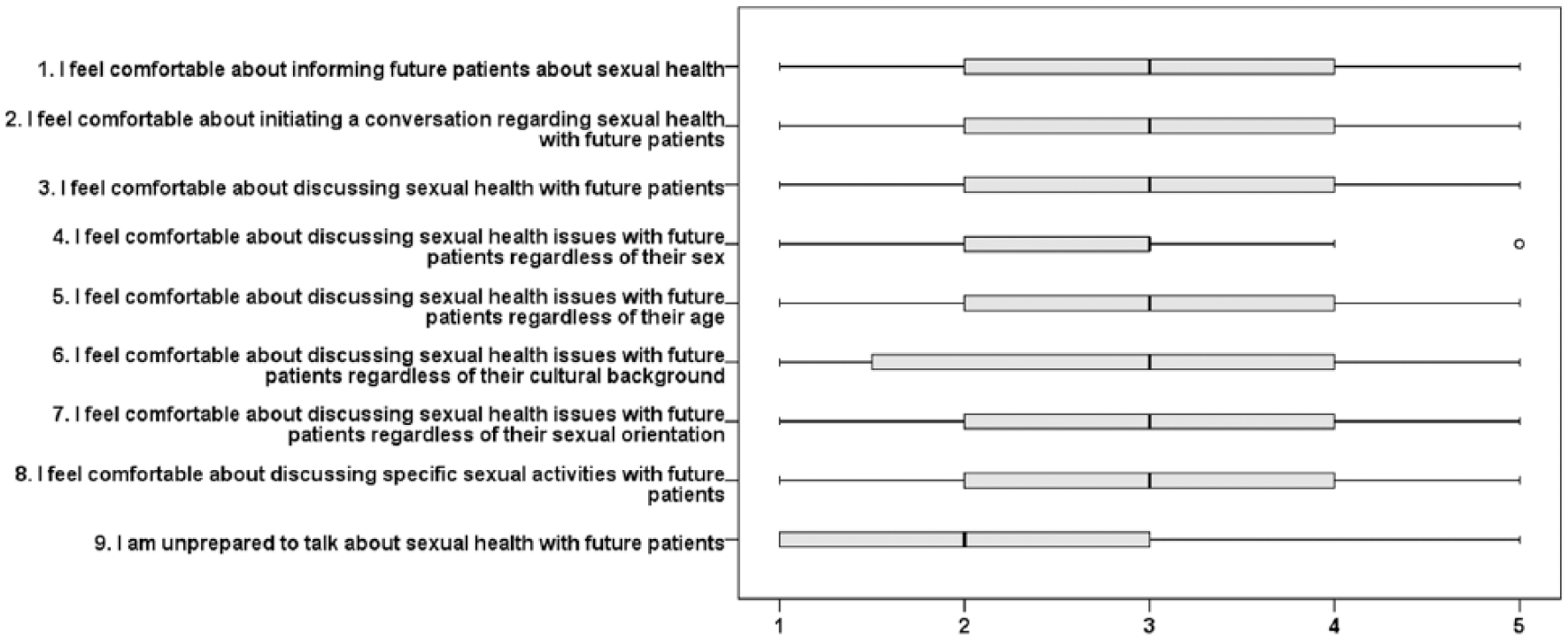
Present feelings of comfort in addressing sexual health (nine variables); boxes depict medians and quartiles, while whiskers represent the lowest and highest values that are not outliers (°). 1 = disagree, 2 = partly disagree, 3 = partly agree, 4 = agree, 5 = strongly agree.
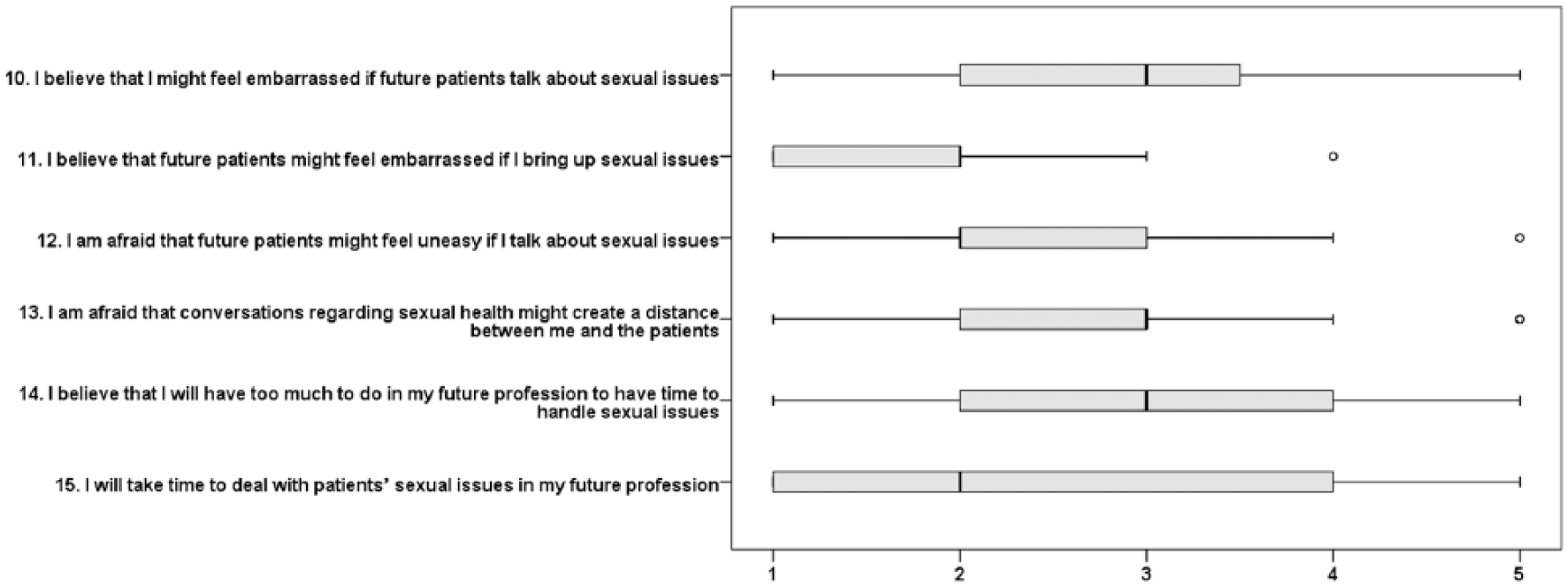
Future working environment (six variables); boxes depict medians and quartiles, while whiskers represent the lowest and highest values that are not outliers (°). 1 = disagree, 2 = partly disagree, 3 = partly agree, 4 = agree, 5 = strongly agree.
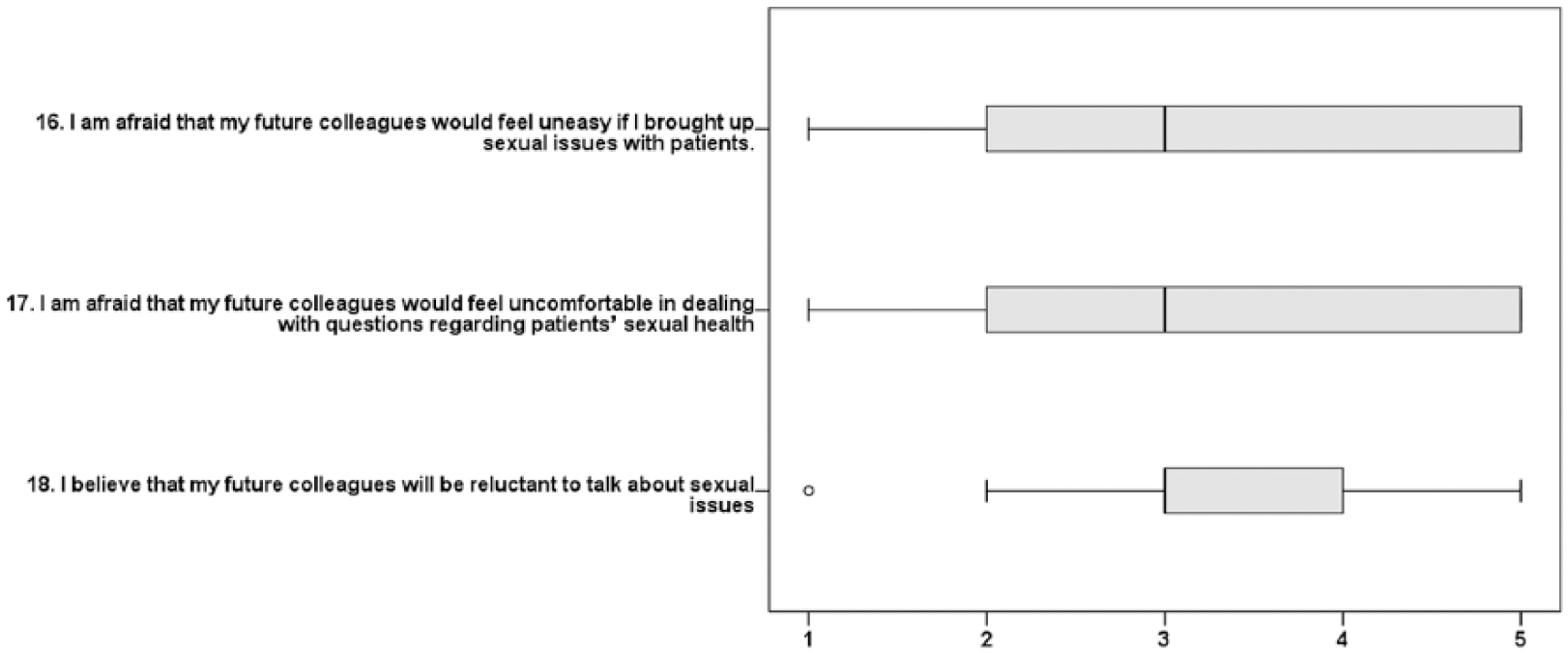
Future colleagues (three variables); boxes depict medians and quartiles, while whiskers represent the lowest and highest values that are not outliers (°). 1 = disagree, 2 = partly disagree, 3 = partly agree, 4 = agree, 5 = strongly agree.
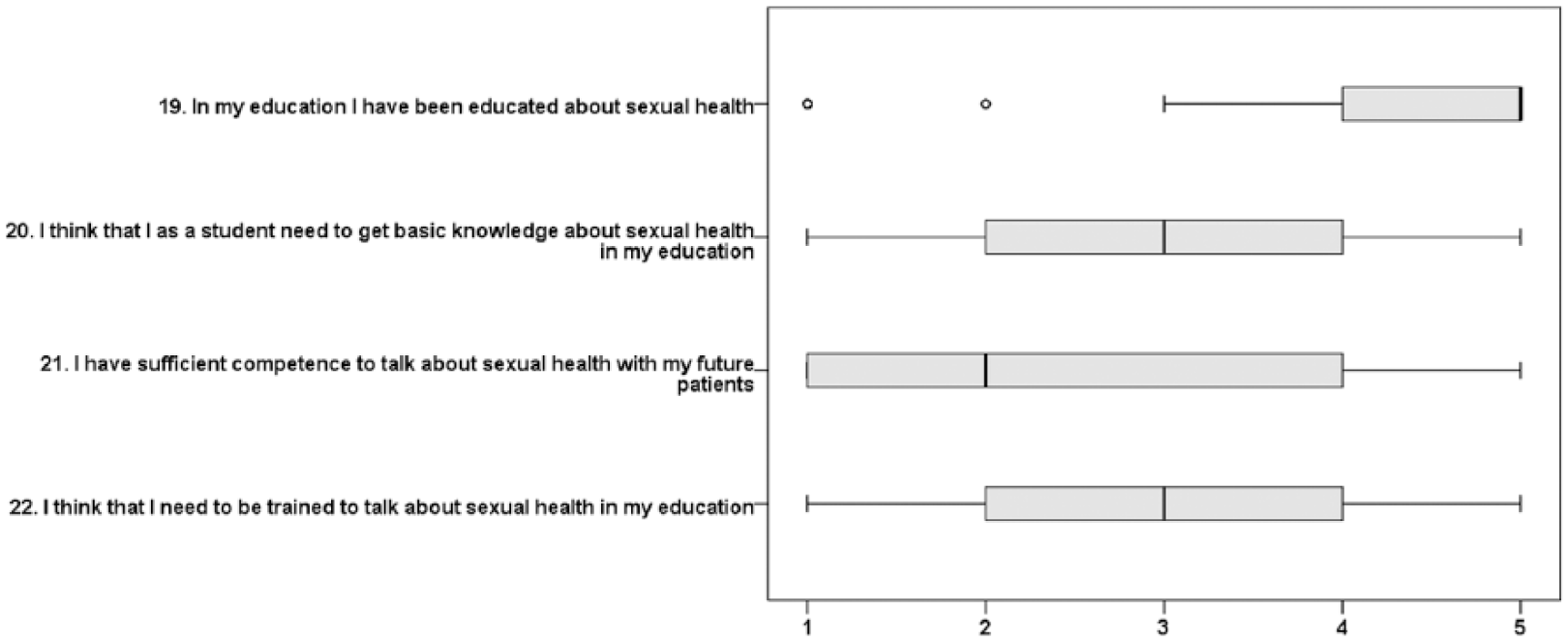
Education (four variables); boxes depict medians and quartiles, while whiskers represent the lowest and highest values that are not outliers (°). 1 = disagree, 2 = partly disagree, 3 = partly agree, 4 = agree, 5 = strongly agree.
The students agreed that their future colleagues would feel uneasy if the student, as a future professional, bought up issues related to sexual health and thought that their future colleagues would be uncomfortable and reluctant to talk about sexual health issues (Figure 3). Students indicated that they had received education about sexual health but did not have sufficient competence to discuss issues with future clients (Figure 4).
No significant difference was observed in item responses when comparing students from years 1, 2, and 3 of the prosthetics and orthotics undergraduate program (p > 0.05). Significant differences between male and female students were observed regarding question 15—I will take time to deal with clients’ sexual issues in my future profession (p = 0.002) and question 21—I have sufficient competence to talk about sexual health with my future clients (p = 0.036). In both cases, female students were more positive in their responses than male students.
Reliability and validity
Item-level CVI (I-CVI) and sum of the CVI (S-CVI) results are presented in Table 1. Results indicated that the items were not considered relevant enough, by the students, to reach the set goals for I-CVI and S-CVI, but there is improvement as students progress through their education. There was a great deal of variance between individuals in the rated relevance of items. Ratings in year 1 varied between 0 and 0.95, in year 2 between 0.14 and 1.0, and in year 3 between 0 and 1.0.
Psychometric testing of internal consistency was performed with Cronbach’s alpha showing 0.86 over the 22 items. Scores for individual domains ranged from a high of 0.91 for feelings of comfort in addressing sexual health, 0.75 for fear of negative influence on future client relations, 0.65 for future working environment, to a low of 0.28 for educational needs.
Discussion
Individuals who have a physical disability often struggle with low sexual esteem, low levels of sexual satisfaction, and limited sexual expression. 3 Assistive technologies, provided by prosthetists/orthotists to facilitate sexual activity, have been identified by clients as having the potential to change their sexual life for the better. 18 Despite this, prosthetists/orthotists do not appear to be addressing sexual health issues with their clients. 20 To change this pattern of behavior, it is necessary to introduce formal training on sexual health care into P&O educational programs. This will first require an understanding of students’ current knowledge and perceived needs.
Results of this study indicate that P&O students who responded to the questionnaire are not prepared to appropriately manage client-related sexual health issues in their future professional role. Despite indicating that they had been educated about sexual health, the group of students included in this study did not feel that they had sufficient competence to talk about sexual health with their future clients and did not indicate that they would take time to address sexual health issues in their future profession.
Many students responding to the questionnaire indicated that they did not feel comfortable discussing sexual health issues and this appeared to be more problematic when communicating with clients from different sexes and clients from different cultural backgrounds. Discomfort in discussing sexual health issues with clients from another gender has been a recurring theme in several studies involving health care providers,28,29 as is the preconceived notion that sex is less openly discussed by minority ethnic groups. 30 Results highlight the need for education which focuses on communication with clients on sexuality and sexual health.
Students felt that their future clients would feel more embarrassed in talking about sexual issues than they would themselves. They also believed that future clients would feel uneasy if they raised issues related to sexual health. Results reflect a common misconception among health professionals, who often believe that clients will initiate a discussion about sexual health issues if they have concerns. 30 Clients, however, indicate that they would prefer the health care provider to raise the topic 28 and feel more embarrassed if they are required to raise the subject themselves. 30
The SA-SH questionnaire has previously been used to explore perceptions of working with sexual health issues for students enrolled in nursing, physiotherapy, and occupational therapy programs. 31 Compared to students from other professional programs, P&O students responding to this survey were less comfortable in dealing with sexual health issues and felt that their future colleagues would feel more uneasy, uncomfortable, and reluctant in talking about sexual issues. This issue could be addressed by introducing sexual health education in an interprofessional learning environment. A notion which is supported by Penwell-Waines et al. 32 who suggest that interdisciplinary sexual health education would facilitate interprofessional referrals and teamwork when students enter their professional lives.
Students in this study rated the need for knowledge and to be trained to talk about sexual issues lower than students from other health professions. 31 Surprisingly, P&O students in this study reported that they had received more education about sexual issues when compared to results from other health professions. 31 Given that no significant difference was observed across years 1 to 3 of the program, one can only assume that the education students received in relation to sexual health was prior to entering the P&O program. Results may reflect the fact that the P&O program in particular has a large proportion of students from other Scandinavian countries. Students from these countries may have had a different experience regarding sexual health education than their Swedish peers. It is also relevant to note that the majority of students in this study were female. This may have affected the results and should be explored further with a larger sample of students. Gender differences have been reported in previous studies which have applied the SA-SH questionnaire, with female students indicating a greater need for training and being less comfortable discussing sexual health issues with clients. 31
Results of this investigation support findings from previous work which has indicated that prosthetists involved as members of amputation teams have insufficient knowledge about sexual health issues that may affect their clients. 16 In contrast to this study however, prosthetists working in the Netherlands have indicated that discussing sexuality with their clients is part of their professional responsibility. 16 Results indicate that the relevance of sexual health issues for prosthetists/orthotists does not become clear until after clinicians have entered the profession.
Several issues have been identified that should be addressed in the education of prosthetists/orthotists. First, students need to be aware that it will be their responsibility, and not the responsibility of their future clients, to routinely raise issues related to sexual health. They should receive training in sexual health issues and obtain skills in communicating with clients regarding improving their level of comfort in raising and discussing the topic. Importantly, communication with clients from the opposite sex and minority groups should be emphasized. Students should also be made aware of the role that other health professionals play in addressing sexual health issues. We suggest that this issue should be addressed using a co-productive approach incorporating the students’ views of their educational needs together with the needs of the clients. 33
The extent to which results of this study can be generalized to other P&O programs is not clear. Scandinavia is well known for its tolerance for sexuality and a progressive approach to sex education, 34 and although the results did not reflect this progressive approach to sexual education, it is possible that individuals from more conservative countries would have different views.
Psychometric testing
The CVI is typically used to assess expert opinion regarding the relevance of a questionnaire to the topic under investigation. While P&O students are experts at being students, they cannot be considered experts on the topic of sexual health related to their future profession. This may be a reason for the relatively low CVI values in this study and may also provide an explanation for the increased CVI values recorded for the third year students. Prior to conducting this pilot project, lecturers from the P&O program were invited to comment on the relevance of the questionnaire. Their assessment was that the questionnaire was highly relevant.
It is possible that the level of relevance of items rated by students reflects their knowledge of the profession. Results clearly demonstrated that the relevance of items, as perceived by students, increased as they progressed through their education. As students proceed through their education, they participate in theoretical and practical training as well as clinical placements. During this time, they would be expected to become more and more aware of the role of prosthetists/orthotists and the relevance of addressing sexual health issues.
While the relevance of each item within the questionnaire was evaluated using the CVI, psychometric testing of internal consistency was performed with Cronbach’s alpha. Results for the total 22 items included in the SA-SH questionnaire demonstrated acceptable results; however, Cronbach’s alpha for the educational needs domain was low. This is likely due to the varied responses to items within this domain. For example, most students indicate that they have received education related to sexual health (item 1 in the domain) but rate low on having sufficient competence to talk about sexual health issues. The low alpha value has minor implications for this study as clustered items were not analyzed.
Conclusion
Sexual health assessment and intervention should be an integral part of the P&O practice. Students within the undergraduate program included in this study are clearly not sufficiently prepared to address issues related to sexual health with their future clients. They are not comfortable in discussing sexual health with their future clients and do not consider that they have sufficient competence to talk about sexual health issues. Improved training and education of P&O students is required regarding sexual health issues and to allow students to develop strategies for communicating with future clients from a range of backgrounds.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.