
Abstract
Background:
Shock-attenuating pylons are commonly fitted to prostheses in order to compensate for the anatomical and biomechanical shock-absorbing features of the lower limb removed upon amputation. However, studies concerning their shock-attenuating capacity are highly variable and, to date, have not yet been reviewed, making them difficult to interpret and apply in clinical practice.
Objectives:
To synthesise and appraise the available literature examining the effectiveness of shock-attenuating pylons in attenuating shock upon limb loading compared to rigid pylons among lower limb amputees.
Study design:
Systematic review.
Methods:
A comprehensive search of seven databases was conducted using search terms concerning amputation level, shock-attenuating and rigid pylons as well as measures of shock attenuation. All studies yielded were screened against established inclusion and exclusion criteria before eligible articles were appraised using the Quality Assessment Standard for Crossover Studies adapted from the Cochrane handbook.
Results:
Nine articles were eligible for inclusion. While there was a trend among studies to indicate only a limited positive effect of shock-attenuating pylons in attenuating transient impact forces, limitations to the study designs, namely, in sampling, poor reporting of methodological details and heterogeneity of outcomes made conclusive interpretation of results difficult.
Conclusion:
While the current body of literature does not reconcile with claims made by manufacturers of shock-attenuating pylons, it is insufficient to conclusively determine how effective shock-attenuating pylons are, in comparison with conventional rigid pylons, in attenuating transient impact forces among lower limb amputees. Higher quality research is required to better guide decisions regarding prescription of shock-attenuating componentry in clinical practice.
Clinical relevance
When delivered well, research can provide clinicians with objective and reliable data that can be applied in their practice to guide prescription of componentry. However, methodological limitations to research may compromise the reliability of findings, thereby producing potentially misleading outcomes. These limitations must be recognised and appreciated such that findings may be interpreted accurately and applied appropriately.
Keywords
Background
Upon initial weight acceptance early in the stance phase of gait, the lower limb is exposed to a high transient impact force caused by rapid deceleration of the stance limb with respect to the ground surface.1–4 This impact force, or shock, is transmitted through the musculoskeletal system from the heel to the spinal column and through to the head.4,5
In able-bodied individuals, a number of anatomical structures and biomechanical strategies have been identified as being crucial for reducing this shock. These primarily include the soft tissues beneath the calcaneus,6–9 passive motion of the ankle joint10–12 and knee joint, 4 muscular regulation of lower limb stiffness,13–15 as well as the viscoelastic properties of subchondral bone and the menisci at the knee joint.16–19 Without the presence or full function of these mechanisms to sufficiently attenuate repeated shock forces, the risk of developing a number of injurious overload conditions is heightened, including subchondral bone microfractures, degeneration of articular cartilage and the aggravation of low back pain.4,18,20–22
However, while lower limb amputees lack some of the above-mentioned strategies for shock attenuation, they frequently place less loading on their amputated limb in comparison with their sound limb when walking. 23 As such the knee of the amputated limb is less likely to be as susceptible to conditions such as pain and osteoarthritis as that of the sound limb or able-bodied individuals.24–27 Nevertheless, given that the residual limb is unfamiliar to repetitive loading and is vulnerable to skin breakdown,25–27 inadequately attenuated loading may result in undue pain, discomfort and even ulceration of the residual limb within the prosthetic socket. It is possible that this residual limb discomfort, which has been demonstrated to be a common issue among transtibial amputees,28,29 may in some cases be a contributing factor towards asymmetrical loading between the amputated and sound limb as well as asymmetries in gait pattern. 30 It is understandable then that residual limb problems have been shown to demonstrate a positive relationship with the presence and intensity of lower back pain 28 and impaired functional mobility. 31
In an effort to restore the safety, comfort and mobility of lower limb amputees to a level similar to that prior to amputation, a number of prosthetic components have been designed to compensate for the shock-attenuating function of the musculoskeletal structures removed through amputation. In addition to the presence of products like the cushioned heel of the SACH (solid ankle cushioned heel) foot 32 and compliant elastomeric liners,33–35 modular shock-attenuating pylons (SAPs) are commonly prescribed and fitted to prostheses in place of a completely rigid pylon for this very purpose. Components such as the Össur Total Shock (Össur, Reykjavik, Iceland), Ottobock Triton Vertical Shock (Ottobock, Duderstadt, Germany) and the Endolite Tele-torsion Pro (Chas A Blatchford & Sons Ltd, Basingstoke, UK) have been designed and are marketed to compensate for the loss of important anatomical structures involved in shock absorption as well as improve amputee safety, mobility and comfort.36–38
Numerous pieces of research concerning SAPs have been undertaken, all with variable quality and methodologies. However, to date, there has been no review performed to exclusively examine their ability to attenuate shock forces during initial loading of the prosthesis. Regardless, SAPs are often prescribed to accommodate high-impact activities, alleviate residual limb discomfort within the prosthesis socket or if function of joints proximal to the residual limb is compromised. In the era of evidence-based practice, it is important to clearly discern the known and unknown effects of SAPs in comparison with using a completely rigid pylon through collectively reviewing and appraising the available literature.
As such the aim of this systematic review was to synthesise and appraise the currently available literature examining the efficacy of SAPs in attenuating shock upon loading of the prosthetic limb compared to rigid pylons among lower limb amputees. The review aims to build upon the work of Highsmith et al. 39 who broadly reviewed evidence concerning SAPs in addition to other prosthetic interventions. This additional, in-depth evaluation of the literature is necessary in order to more rigorously evaluate the available literature, potentially identify the impact of SAPs among lower limb amputees to better guide clinical decision-making, as well as identify aspects of research into SAPs that require further attention.
Methods
Search strategy
A systematic search of the literature was conducted in August 2017 by the primary author (M.F.) using CINAHL (EBSCO, 1981–2017), Cochrane Library (1993–2017), EMBASE (OVID 1974–2017), MEDLINE (OVID, 1946–2017), ProQuest Nursing and Allied Health (1969–2017), SCOPUS (Elsevier, 1823–2017) and Web of Science (ISI, 1955–2017) databases.
The search strategy was formulated by including search terms related to the population, interventions and outcomes of interest, as well as their synonyms and acronyms, in combination with wildcard and Boolean operators. These search terms were utilised as part of a title, abstract and keyword search and were limited to articles in the English language within each database. 40
Although the purpose of this systematic review was to exclusively examine the impact of SAPs upon weight acceptance, many SAPs are described to also have a torsion attenuating capacity. For this reason, search terms pertaining to the interventions included those related to both modular SAPs and torsion-attenuating pylons. Furthermore, as the number of ways in which the shock-attenuating capacity of SAPs can be measured varies greatly, narrow definitions of specific outcome measures would have inappropriately limiting. A wide variety of search terms pertaining to both kinematic and kinetic variables were thus included. This search strategy was developed and refined such that at least a collection of known articles, relevant to this systematic review, were yielded.
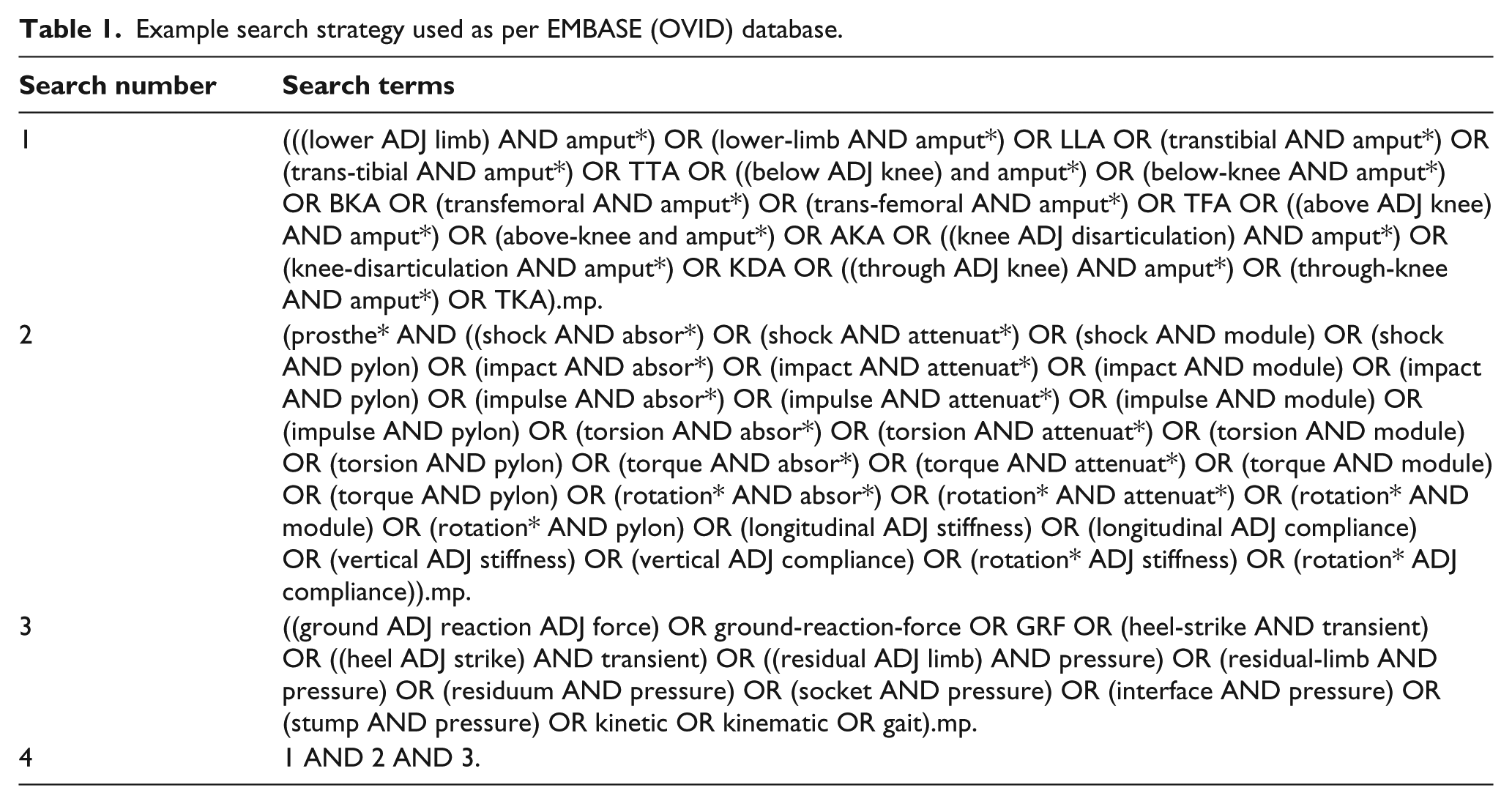
In keeping with the Preferred Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 41 a full description of the search strategy including the search terms utilised has been provided as per one database (Table 1).
Example search strategy used as per EMBASE (OVID) database.
Eligibility criteria
Articles were included if they reported on the efficacy or effectiveness of SAPs in attenuating measures of shock upon loading of the prosthesis in comparison with that of rigid pylons among lower limb amputees. As several variables observed during initial prosthetic limb loading may be influenced by the presence of SAPs and their potential to attenuate shock, eligibility was not limited to any one reported outcome, but rather any which were relevant to shock attenuation upon residual limb loading.
It is important to recognise that while many SAPs are fitted to prostheses as individual modular components, some are fitted as a part of the prosthetic foot module (e.g. Össur Reflex Rotate; Össur, Reykjavik, Iceland). Any articles comparing such prosthetic feet to equivalent feet without a SAP or to when the SAP is immobilised were also included. Technical notes and opinion pieces were excluded. Articles not in English were also excluded by virtue of the search strategy.
Study selection
After removing duplicate articles from the search results, M.F. independently screened all titles and abstracts identified from the search for inclusion. The full texts of potentially relevant papers were retrieved and further assessed for inclusion. In the case where there was uncertainty over eligibility for inclusion, a second opinion from the second author (E.T.) was sought. Any disagreement was resolved via discussion until a consensus on the eligibility for inclusion was reached. Given that the eligibility criteria for inclusion were not complex, the use of two authors to determine eligibility was deemed unnecessary. 42 The referencing software Endnote X7 (Clarivate Analytics, Philadelphia, PA, USA) was utilised to manage the screening process. Reference lists of articles included were also hand searched to determine whether further articles could be included.
Data extraction and quality assessment
Relevant demographic, methodological, outcome and quality appraisal information was extracted from each article and recorded in a Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) spreadsheet based on the Cochrane Consumers and Communication Review Group’s data extraction template. 43
The methodological quality of each article was assessed using the quality assessment standard for a cross-over study 44 adapted from the Cochrane handbook 45 and Cochrane Collaboration tool for assessing risk of bias. 46 This tool was deemed appropriate for the quality and risk of bias assessment given that a preliminary review of the included studies revealed all to be of a repeat-measures cross-over design. Not only is this tool specific to cross-over studies but also grades the risk of bias for each of nine items as low, high or unclear, allowing the methodological quality of different articles to be clearly presented and compared. These nine items are not part of a hierarchical scale.
The data extraction and quality assessment were also undertaken by M.F., yet E.T. was consulted in the case of any uncertainty. Both authors discussed the matter until a consensus was achieved. In cases where there was a lack of clarity within articles pertaining to information relevant to this systematic review, the appropriate corresponding author was contacted to seek the relevant information.
Results
Summary of results
The search of databases yielded 294 articles (Figure 1). After the removal of duplicates, 101 articles were screened for eligibility, of which 947–55 met the criteria for final inclusion. Hand searching the reference lists of the included articles did not yield any additional papers.
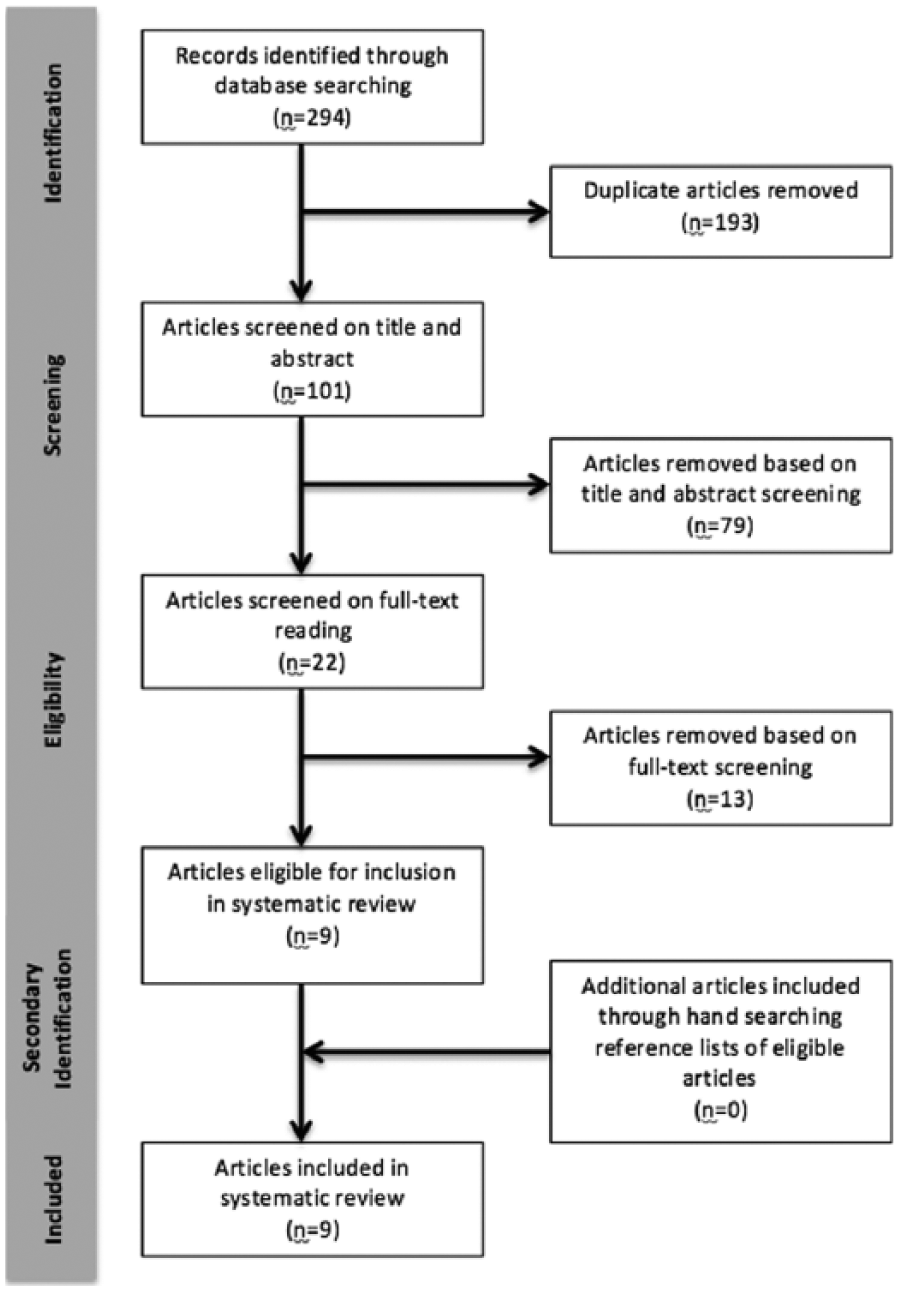
PRISMA flowchart of included studies.
The included nine articles examined variables reflective of shock forces experienced upon lower limb amputees loading their prosthesis both with a SAP and rigid pylon or the SAP immobilised. In total, the studies included 78 participants (mean = 8.67). Although the details of these studies were unclear in a number of cases, many were performed within a laboratory or rehabilitation facility,48–51 with the assistance of a certified prosthetist to undertake the fitting and alignment of prostheses.48–50,52–55 Despite observations of minor trends, the vast majority of studies were suggestive that SAPs show no strong effect for a difference in the ability to attenuate shock as compared to rigid pylons among transtibial amputees while undertaking different modes of activity, including walking, running and stepping down from an elevated platform.47–50,53–55 Some studies did report isolated but significant differences in group variables, including a reduction in knee flexion upon initial contact when fitted with a SAP and while walking at a controlled speed, 48 as well as differences in select variables among individual participants.51,55 These findings, however, were not consistent with the overall trend of the included studies.
Among the few transfemoral amputees which were studied, measures of shock revealed inconsistent findings between different interventions when participants stepped down from an elevated platform. While some outcomes were indicative of no differences between interventions, isolated variables were indicative of an improved ability to attenuate shock when fitted with a SAP. 52
Characterisation of included studies
Participant characteristics
Participant characteristics have been presented in Table 2. In brief, study participants were predominantly male (≥85.9%), aged 16–81 years and with a unilateral transtibial amputation due to trauma (n ≥ 54; 69.2%). Only one study included transfemoral amputees (n = 5; 6.41%), of which all were male with a mean age of 42.1 years. 52 The activity level of participants varied greatly between studies, with most only requiring that participants be able to complete the performance-based outcome measures utilised in the study. Studies also tended to include participants experienced in wearing prostheses for a period of at least 6 months and excluded potential participants presenting with comorbidities such as neurological impairments. The type of prostheses participants used in their everyday lives varied greatly, but the vast majority were not routinely using a SAP. Participant body weight was consistently limited to the weight restrictions indicated by the manufacturer of SAPs, with the exception of one study. 51
Demographic characteristics of study participants.
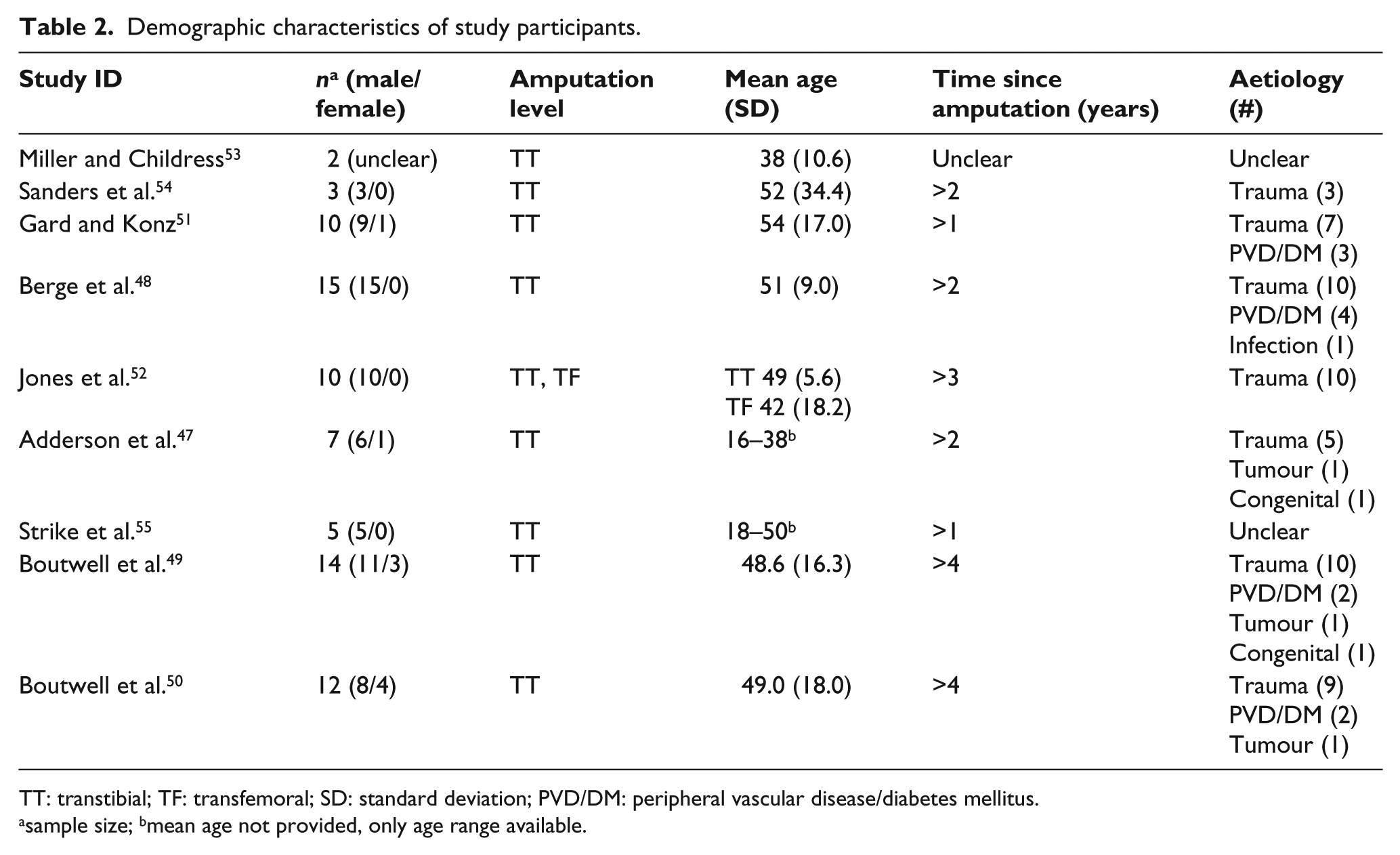
TT: transtibial; TF: transfemoral; SD: standard deviation; PVD/DM: peripheral vascular disease/diabetes mellitus.
sample size; bmean age not provided, only age range available.
Study design
All nine of the included studies were of a repeat-measures cross-over design with at least one group exposed to at least two levels of intervention. Means of participant recruitment were also often left unreported, with the exception of one study which utilised a convenience sampling process. 49
Types of intervention
Four different models of SAP were examined throughout the nine studies: the Endolite Tele-torsion Pylon,49–52,55 Seattle Airstance,47,54 Mercury Telescopic Torsion Pylon 48 as well as the Reflex VSP foot module with integrated SAP. 53 Of these interventions, only the Endolite Tele-torsion pylon is still commercially available. Outcomes measured using these SAPs were compared to those measured using either a rigid pylon with all other componentry and alignment being maintained or the SAP being immobilised. When functional, the stiffness of the SAP was tailored according to the manufacturer’s recommendations in all but one study. 54 Participants maintained their own socket interface and means of suspension throughout the study period and in a number of articles also maintained other componentry (apart from the pylon) such as the prosthetic foot as well as footwear. Although not always specified, there was a great variability in suspension systems, including suprapatella cuffs, neoprene sleeves and shuttle locks,51,52,54 as well as prosthetic feet, ranging from SACH feet to energy storage and return (ESAR) feet.48–55 There were six studies48–50,53–55 which controlled for the prosthetic foot between participants and two which controlled for the footwear.49,50
Outcome measures
Measuring the shock-attenuating capacity
All investigations employed quantitative methods to evaluate the shock-attenuating capacity of SAPs in comparison with more rigid componentry; however, these methods widely varied in the measurement tools utilised (Table 3). The most commonly employed means of evaluating shock was measurement of the first peak vertical ground reaction force (GRF)47–51,53,55 magnitude and loading rate.47–51,55
Interventions and outcome measurements.
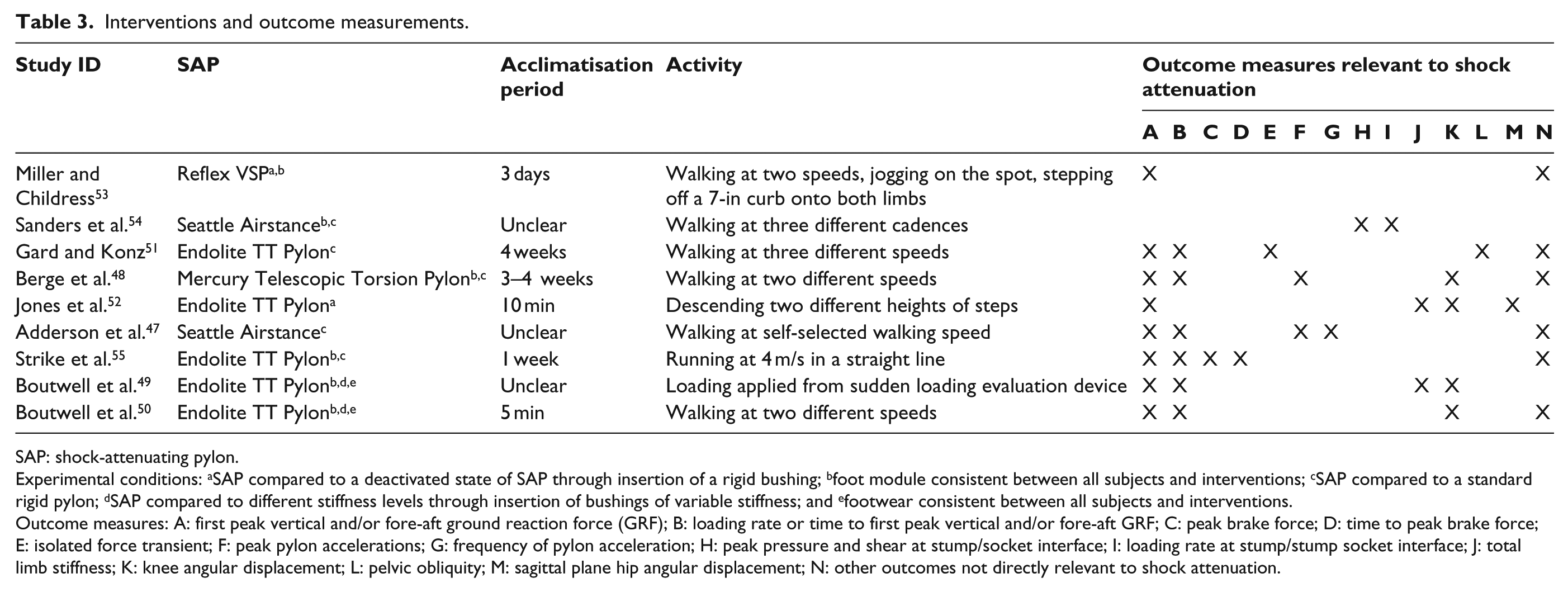
SAP: shock-attenuating pylon.
Experimental conditions: aSAP compared to a deactivated state of SAP through insertion of a rigid bushing; bfoot module consistent between all subjects and interventions; cSAP compared to a standard rigid pylon; dSAP compared to different stiffness levels through insertion of bushings of variable stiffness; and efootwear consistent between all subjects and interventions.
Outcome measures: A: first peak vertical and/or fore-aft ground reaction force (GRF); B: loading rate or time to first peak vertical and/or fore-aft GRF; C: peak brake force; D: time to peak brake force; E: isolated force transient; F: peak pylon accelerations; G: frequency of pylon acceleration; H: peak pressure and shear at stump/socket interface; I: loading rate at stump/stump socket interface; J: total limb stiffness; K: knee angular displacement; L: pelvic obliquity; M: sagittal plane hip angular displacement; N: other outcomes not directly relevant to shock attenuation.
Outcome measurements were usually taken with participants simply walking in a straight line at self-selected and/or controlled walking speeds over a short distance.47,48,50,51,53,54 Most measurements were taken after a period of acclimatisation which ranged from as little as 5 min 50 to as long as 4 weeks. 51 One study reported only one participant to acclimatise to the intervention, while their second participant did not spend any time acclimatising at all due to fitting difficulties. 53
Quality appraisal/risk of bias assessment
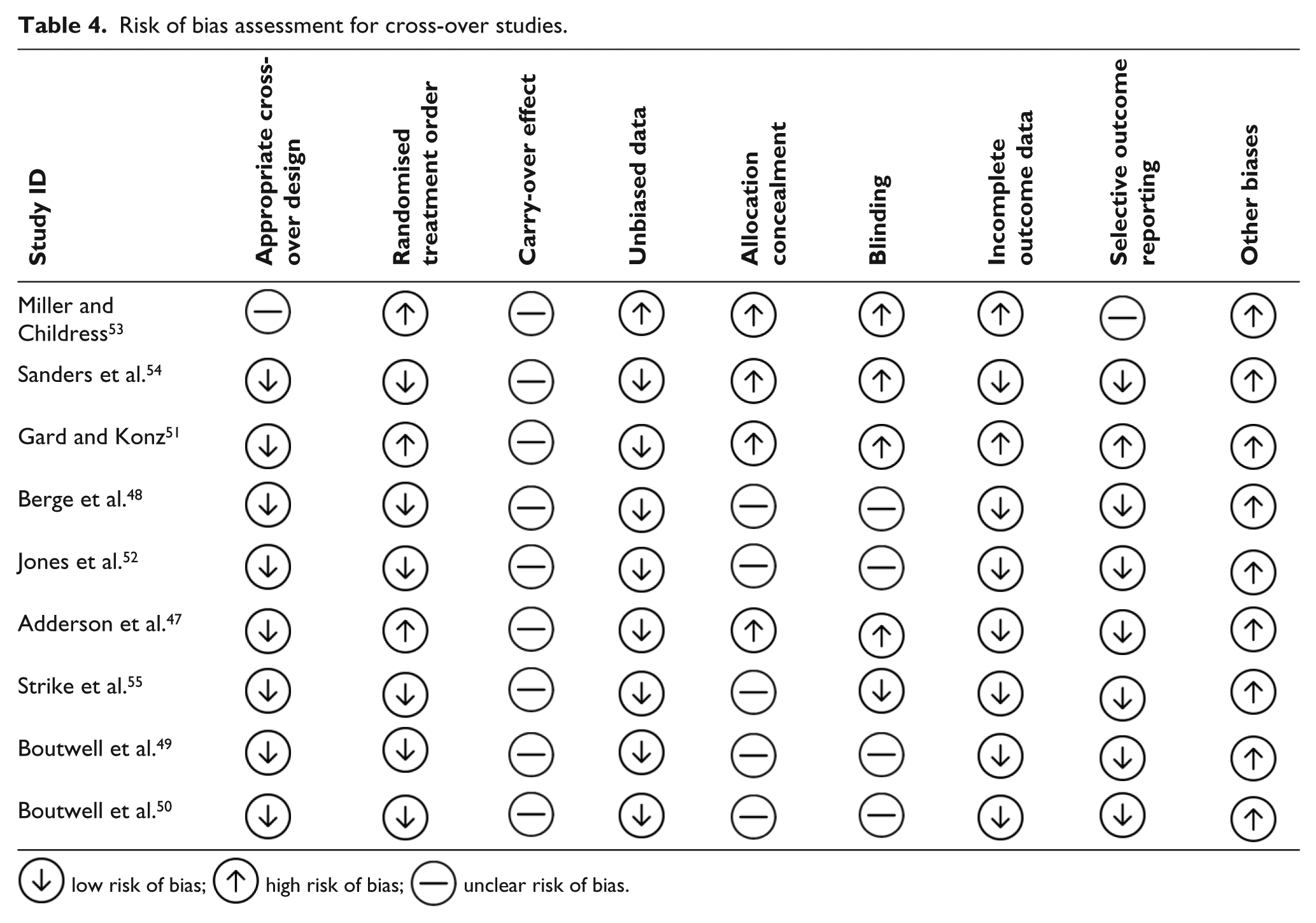
Based on the quality assessment standard for a cross-over study 44 adapted from the Cochrane handbook 45 and Cochrane Collaboration tool for assessing risk of bias, 46 there were a number of limitations affecting the internal and external validity of all of the nine included studies,47–55 as indicated in Table 4. It must be appreciated that while a carry-over effect was unlikely to have occurred between interventions, this item is required to be marked as unclear when assessment for a carry-over effect was not undertaken. Furthermore, among four studies,48–50,52 participants were blinded to the intervention, yet it is unclear as to whether researchers were also blinded and as such, these items were marked as unclear. Several other methodological limitations and risks to bias were presented among the included studies. These limitations included small sample sizes, sampling bias, limited representativeness of performance measures, inappropriate inferential analysis techniques as well as reporting biases.
Risk of bias assessment for cross-over studies.
 low risk of bias;
low risk of bias;  high risk of bias;
high risk of bias;  unclear risk of bias.
unclear risk of bias.
Discussion
The aim of this systematic review was to synthesise and appraise the available evidence comparing the efficacy of SAPs and rigid pylons in attenuating shock upon lower limb amputees loading their prosthesis. The majority of included studies47–55 concluded SAPs to demonstrate no clinically appreciable difference from rigid pylons among transtibial amputees. However, one study reported an improved shock attenuation capacity among transfemoral amputees when stepping down from an elevated platform.
Among the transtibial amputee population, these findings counter indications made by manufacturers of SAPs as well as measurements observed from bench testing studies.53,56 This could be suggested to be reflective of a redundancy of SAPs in a clinical setting, given the potential shock-attenuating capacity of other componentry and footwear.57–59 However, it must be acknowledged that the methodological limitations and heightened risks of bias presented in these studies are very likely to affect internal and external validity of their findings.
Strengths and limitations of the included studies
Sample size
Sample sizes were consistently small, with the largest sample comprising only 15 participants. 48 Small sample sizes have been suggested to be acceptable when studying amputees given their relatively small population compared to that of other health conditions. 39 However, with such small sample sizes and inherently low statistical power for a given effect size, the capacity to confidently represent an effect of the intervention is limited. Small, low-powered studies are limited to detecting true effects only if they are very large. As such, samples as small as those in the included studies may not have been able to confidently detect smaller effects of SAPs among participants, which may actually be clinically relevant. 60
Alternatively, effects detected as being ‘significant’ (according to the convention of a positive predictive value utilised in the included studies) may be inflated in their magnitude from a true population effect or may even incorrectly detect an effect that is not actually present due to a high sampling error associated with small sample sizes. 60 Consequently, the sample sizes utilised in the included studies are greatly limiting to the reliability of their findings and should be approached with great caution.
Sampling bias
While SAPs are commonly indicated to be beneficial towards those who experience stump pain due to pressures within the prosthetic socket,36–38 studies tended to exclude potential participants who presented with stump pain or neurological conditions, such as neuromas. As such samples were not entirely representative of the population for whom SAPs may be suitable. Furthermore, only one 49 of the nine included studies stipulated their method of recruitment, which was one of convenience sampling, rendering the outcomes highly susceptible to selection bias.
Appropriateness of comparisons
A number of studies utilised much of the participants’ existing prosthetic componentry between conditions of intervention. All included articles47–55 demonstrated variability in and did not control for the impact of socket interface and suspension system between participants, while six articles maintained consistency in the foot module48–50,53–55 and two in footwear utilised for each participant.49,50 Although these components were maintained between interventions for each individual participant, it is possible that their varying capacity to attenuate shock would have a bearing on the shock attenuation capacity of the SAP and the outcomes measured in each study, thereby skewing group data. It is likely that participants fitted with stiffer prosthetic feet or wearing stiffer-soled shoes would experience a greater reduction in measures of shock than those with more compliant componentry.
Acclimatisation
Acclimatisation periods varied from 5 min 50 to 4 weeks. 51 While it has been suggested that as little as 200 steps are required for able-bodies individuals to acclimatise to new footwear, 61 the length of time required to acclimatise to prosthetic componentry remains undetermined. 62 As such those studies which implemented very short acclimatisation periods would have increased the risk of findings not being reflective of long-term use of the interventions, particularly without assessment for a carry-over effect.
Validity of outcome measures
The outcome measures employed were highly variable. Although there is no gold standard for measuring shock, it is often measured using accelerometers within several other fields, 63 as it was in only one study included in this review. 47 Indeed, measurements taken by accelerometers have been correlated with GRF data and knee flexion angles among able-bodied individuals when loading their lower limbs.64,65 However, the studies in this review included several other variables that are not exclusively reflective of or dependent on shock attenuation, including compression of the pylon, walking speed and step length symmetry. Interpretation of findings pertaining to these variables may be misleading when attempting to discern the clinically relevant shock-attenuating capacity of such interventions.
Inferential analysis
Statistical tests to assess the outcomes of group data were non-existent in two studies,53,55 making interpretation of results difficult. Other studies utilised techniques for evaluating multiple group comparisons; however, five of those employed statistical tests which assume a normal distribution of data47,48,51,52,54 without any assessment to determine whether the data were normally distributed and without adjusting/transforming their data to account for a non-normal distribution. Although the t-test and analysis of variance (ANOVA) are generally robust against distributions which deviate from normal, with very small samples such as those observed in the included studies, a normal distribution is unlikely. 66 Consequently, such studies are likely to have determined group data inaccurately or imprecisely. Evaluation of data distribution and use of non-parametric tests such as those used in two included studies49,50 or employing transformation techniques, if appropriate, would provide a more powerful, reliable statistical analysis and a favourable influence on statistical inferences.
Limitations of this review
This systematic review also acknowledges limitations of its own, namely, in that the only articles reviewed were those in the English language and that no assessment of inter-rater reliability was performed in determining the articles eligible for inclusion and also during the quality assessment. Furthermore, a meta-analysis was not conducted by virtue of the wide variability in methodologies and heterogeneity of outcomes measured within the included studies. This thereby limited the capacity to collate and collectively analyse the data from the included studies and potentially identify a common effect of SAPs for each level of amputation or mode of activity.
Clinical implications
Recognition and understanding of these methodological issues are essential when interpreting such literature and in application to evidence-based clinical practice. Clinical prescription and decision-making regarding the shock-attenuating capacity of SAPs in light of these particular studies should be approached with caution. It would be imprudent to ignore the limitations to their methodologies and interpretation of their findings indicated above as they greatly affect their generalisability to the greater lower limb amputee population and in turn their application to clinical decision-making regarding prosthetic prescriptions.
Future directions
More rigorously designed studies that minimise methodological biases are necessary to confidently evaluate the shock-attenuating capacity of SAPs in comparison with rigid pylons among lower limb amputees. Of particular significance is the need for an appropriate sample size determined through carefully considered power analysis and sensitivity analysis 67 as well as appropriate sampling techniques. Achieving an appropriate sample size through unbiased recruitment methods can be challenging within prosthetics research. Alternate study designs, such as the N-of-1 study design has been suggested for research that often experiences difficulty in achieving sufficient numbers of participants and, when designed well, also presents with the highest level of evidence in determining the effectiveness of an intervention, equivalent to that of a randomised controlled trial. 68 Although primarily intended to determine the most appropriate intervention for an individual participant in the era of patient-centred care, data from identical N-of-1 studies may be aggregated and collectively analysed, similar to a meta-analysis, such that data can be generalisable to and assist in making predictions for the greater amputee community.69,70
In doing so, the use of clinically appropriate outcome measures should be consistent across multiple studies. This would enable not only the research question to be answered more confidently but would also permit multiple study results to be pooled to formulate a greater body of evidence. Variables such as accelerometer and GRF data have already been shown to be effective in measuring biomechanical shock and thus may be valuable in demonstrating the potential magnitude of the physical shock-attenuating capacity within a prosthesis.63–65 However, at the same time, it is important that such data be supplemented and a possible relationship drawn with amputee experience-centred outcomes, including measures of socket comfort or activity level, in order to determine any potential impact of SAPs that may be clinically meaningful and relevant to both the clinician and amputee.
In addition, further research should also be able to control for the presence of many confounding variables such as the torsion-attenuating capacity of many designs of SAP.71–75 Similarly, the relative shock-attenuating capacity of other componentry including feet, knees, liners and footwear should also be accounted for so as to determine the necessity for SAPs within certain prosthetic prescriptions.
It would be advantageous to determine exactly which population group would benefit from such interventions, most importantly with regard to activity level, residual limb health and condition of proximal joints. Such studies should not only examine the immediate biomechanical implications of fitting an SAP, but should also investigate the long-term clinical implications of their use. This would encompass not only their shock-attenuating capacity but also potential postural deviations with compression, their added weight and supposed energy return upon unloading of the prosthesis,76–78 all of which may affect protection of proximal joints against overload conditions, residual limb skin breakdown, levels of activity and ultimately quality of life.
Conclusion
To date, there is insufficient evidence to suggest that SAPs are effective in attenuating the transient impact forces lower limb amputees experience upon loading their prosthetic limb. While the vast majority of study findings contradict claims made by manufacturers of SAPs, more rigorous studies are necessary to overcome the methodological limitations and heightened risks of bias present in the currently available body of literature. The N-of-1 study design has been suggested as a robust alternative to the repeat-measures cross-over design to more confidently formulate reasonable and necessary prosthetic prescriptions for lower limb amputees.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.