
Abstract
Background:
Crossover feet incorporate features of energy-storing feet and running-specific feet. As such, crossover feet may be suitable for both daily ambulation and participation in physically demanding activities.
Objectives:
To compare crossover feet and energy-storing feet on performance-based tests including a range of low-level (e.g. sit-to-stand) and high-level (e.g. jogging) activities.
Study design:
Cross-sectional, repeated measures.
Methods:
Participants with transtibial amputation completed a battery of performance-based outcome measures, including the Five Times Sit-to-Stand, Timed-Up-and-Go, Four Square Step Test, and the Comprehensive High-level Activity Mobility Predictor. Participants wore duplicate prostheses fit with crossover feet and energy-storing feet to perform the tests; the order of foot conditions was randomized. Paired t tests were used to evaluate differences between feet and order of testing.
Results:
Data from seven participants showed improvements in all measures while using crossover feet. Improvements in the second foot condition were also observed, indicating a practice effect for all measures. However, differences between feet and order of conditions were not statistically significant (p > 0.05).
Conclusion:
Results of this study suggest that crossover feet may improve low- and high-level mobility outcomes. However, intervention effects are small and practice effects were observed in all outcomes. Future research is needed to evaluate the influence of practice effects on performance-based mobility measures.
Clinical relevance
Crossover feet may improve transtibial prosthesis users’ performance compared to energy-storing feet across a range of activities, but additional research is needed. Practice effects may be an influential factor in the measurement of performance-based mobility outcomes and should be considered when performing a clinical assessment.
Keywords
Background
A primary rehabilitation goal for people with transtibial amputation (TTA) is to restore participation in desired activities using a prosthesis. Selection of appropriate prosthetic components is therefore central to achieving a successful clinical outcome. Prosthetic feet, for example, are designed to replace absent structures of the ankle–foot complex and promote users’ mobility. Despite advances in prosthetic foot technology, mobility outcomes in people with TTA remain limited relative to individuals without amputation. Specifically, it has been well established that people with TTA walk more slowly,1,2 asymmetrically,3,4 and less efficiently5,6 than people without amputation. Furthermore, comparative effectiveness studies have routinely shown that discrepancies between people with and without amputation persist, regardless of the type of prosthetic foot selected.7,8 Gailey et al., 9 for example, found no significant differences in mobility performance among four categories of prosthetic feet using measures such as the 6-min walk test and the Amputee Mobility Predictor.
One reason differences in prosthetic feet have been difficult to measure is that prior studies have typically assessed relatively low-level tasks, such as walking on level surfaces. Contemporary prosthetic feet, which are often designed to promote a user’s ability to participate in a range of low- and high-level activities, have demonstrated functional benefits during more demanding tasks, such as running. For example, TTA prosthesis users have achieved oxygen consumption rates similar to people without amputation when using running-specific feet (RSF). 10 A recent study even found significant differences in energetic outcomes between models of RSF. 11 Select types of energy-storing feet (ESF) have also been shown to significantly reduce oxygen costs during running, relative to other prosthetic feet. 12 Therefore, assessment of mobility during high-level activities may be important when evaluating and/or comparing prosthetic feet.
Crossover feet (XF) are an example of a recent prosthetic technology designed to accommodate a range of activities beyond simple locomotion. 13 Similar to RSF, XF incorporate an extended keel that permits users to engage in high-level activities. XF also include elements of ESF (i.e. heel and foot shell) that are not present in RSF. This unique combination of features allows XF to be used both as daily and sports-specific prostheses.13,14 Results from a prior study showed that XF and ESF were functionally equivalent on most outcomes when participants with TTA walked in a laboratory. 14 Conversely, participants reported significantly improved mobility and fewer activity restrictions when using XF at home and in the community, compared to when they used ESF. All participants also preferred XF to ESF during activities like fast walking, jogging, and sports. However, participants’ performance during these types of high-level mobility activities was not directly measured in the prior study.
The purpose of this study was therefore to extend from prior research and compare the effect of XF relative to ESF on performance-based outcome measures that include a range of low-level activities (e.g. sit-to-stand, walking short distances, turning around a cone) and high-level activities (e.g. quick-stepping, jogging, side-stepping). It was hypothesized that users’ performance on low-level activities would be equivalent between foot conditions. In contrast, users would exhibit significantly improved performance during high-level activities while using XF compared to ESF. Results of this study could be used to inform prescription practices, select outcome measures, and provide preliminary data to power larger studies.
Methods
A repeated-measures, crossover study was designed to compare mobility performance in people with TTA using ESF and XF. This study was conducted subsequent to a prior study that evaluated laboratory- and community-based outcomes associated with use of these feet. 14 All study procedures were reviewed and approved by a University of Washington institutional review board.
Participants
Individuals from the prior study 14 were recruited to participate in this secondary study. Sample size was determined pragmatically based on the availability of candidate participants and resources (i.e. time, space, and funding) available for data collection. Participants were previously recruited from local clinics that employed prosthetists experienced in fitting and aligning both feet. Eligibility criteria included the following: (1) 18 years of age or older, (2) unilateral TTA for more than 1 year, (3) amputation due to non-dysvascular reasons, (4) experience with prosthesis for more than 6 months, and (5) classified as Medicare Functional Classification Level (MFCL) 3 or higher. Individuals were excluded if they had comorbid health conditions that would limit participation in study activities (e.g. walking for 6 min, answering self-report surveys). Participants were recruited for this secondary study if they had the ability to safely engage in high-level tasks (e.g. jogging) based on evaluation by a study prosthetist and consensus of the study team.
Interventions
Participants used two standardized prostheses that were fabricated for the prior study. 14 Socket design, interface, suspension, and footwear were identical between prostheses. One prosthesis included an Össur (Reykjavik, Iceland) Vari-flex foot (ESF) and the other an Össur Cheetah Xplore foot (XF). Duplicate prostheses were fabricated to accommodate the different attachment methods required for each foot (i.e. distal attachment for ESF, direct posterior lamination for XF). All participants had at least 1 month of accommodation time in each prosthesis during the prior study. Two study prosthetists verified fit and alignment of both prostheses using visual inspection, gait analysis, and participant feedback prior to testing.
Procedures
Participants each attended a single data collection session. The order of prosthetic foot condition was determined using simple randomization and assigned (i.e. ESF-XF or XF-ESF) according to a computer-generated list. A battery of performance-based outcome measures was administered by the same researcher in the sequence described below. Measures were selected to assess participants’ ability to perform low- and high-level tasks such as sit-to-stand, walking, turning, jogging, quick turning, weaving, and side-stepping. For each test, participants were read standardized instructions based on developers’ guidelines, provided a demonstration, and asked to practice one time (Appendix 1). Participants then completed each outcome measure twice and the best recorded score or fastest completion time was used for analysis. Participants were encouraged to rest between trials to mitigate fatigue effects. Participants then exchanged prostheses and rested for at least 5 min before repeating all tests.
Outcome measures
Five Times Sit-to-Stand (5×STS)
The 5×STS test measures lower extremity strength, transitional movements, and balance. 15 The 5×STS has shown evidence of high inter-rater (intraclass correlation coefficient (ICC) = 0.93–0.98) and test–retest reliability (ICC = 0.89–0.98) in healthy and in clinical populations, such as in individuals with chronic stroke, 16 Parkinson’s disease, 17 or cerebral palsy. 18 The 5×STS has also demonstrated convergent construct validity when compared to the Dynamic Gait Index (ρ = −0.68), 15 balance measures (r = −0.71), 17 and gait speed measures (r = −0.60). 17 Lower 5×STS times indicate better performance.
Timed-Up-and-Go (TUG)
The TUG test measures low-level functional mobility. The TUG was developed to evaluate functional limitations and fall risk in older adults 19 but has shown evidence of high inter-rater (ICC = 0.93–0.96) and test–retest (ICC = 0.88–0.96) reliability in people with lower limb amputation.20,21 The TUG has also demonstrated convergent construct validity when compared to the Four Square Step Test (FSST) (r = 0.88) and gait speed measures (r = −0.61). 19 Participants were also asked to complete the TUG at two different speeds. For the first two trials, participants were instructed to walk at a comfortable speed (TUG-comf); then, participants were instructed to repeat the TUG walking as quickly as possible without running (TUG-fast). Lower TUG times indicate better performance.
Four Square Step Test (FSST)
The FSST measures dynamic stability and ability to step over small objects forward, laterally, and backward. 22 The FSST has shown evidence of high inter-rater (ICC = 0.96–0.99) and test–retest (ICC = 0.78–0.98) reliability in healthy 22 and in clinical populations, such as in individuals with balance disorders (ICC = 0.93) 23 or Parkinson’s disease (ICC = 0.78–0.90). 24 The FSST has also demonstrated convergent construct validity with the TUG (ρ = 0.69–0.88)22,23 and the Dynamic Gait Index (ρ = −0.51). 23 Lower FSST times indicate better performance.
Comprehensive High-level Activity Mobility Predictor (CHAMP)
The CHAMP measures core strength, functional mobility, and agility. 25 In people with lower limb amputation, the CHAMP has shown evidence for high inter-rater (ICC = 1.0) and test–retest (ICC = 0.97) reliability, 25 as well as convergent construct validity with the 6-min walk test (r = 0.80) and Amputee Mobility Predictor (r = 0.87). 26 The CHAMP is comprised of four sub-tests, including the Single Limb Stance, Edgren Side Step Test, T-test, and Illinois Agility Test. In accordance with developer instructions, a third trial of each sub-test was offered when participants demonstrated disqualifying events (e.g. crossing legs during side-stepping). 25 Higher CHAMP scores indicate better performance.
Analysis
Paired t tests were conducted to evaluate differences between foot conditions. The threshold for statistical significance (α) was set at 0.05. Experiment-wise type I error rate was controlled for multiple comparisons using Dunn–Sidak correction procedures. Outcome measures scored in seconds based on participants’ timed performance (i.e. 5×STS, TUG-comf, TUG-fast, FSST) were treated as a family for correction procedures. Statistical analyses were performed using SPSS, Version 19 (IBM SPSS Statistics for Windows, Version 19.0; IBM Corp., Armonk, NY, USA).
Results
Participants
Seven male participants with unilateral TTA were recruited and completed all study activities between October 2016 and September 2017 (Table 1). On average, participants were young (37.0 ± 9.8 years), experienced prosthesis users (12.9 ± 11.6 years since amputation). Most participants had an amputation due to trauma (n = 6). Participants were classified by study prosthetists as either unlimited community ambulators (K3: n = 3) or active adults (K4: n = 4).
Participant demographic information and initial clinical assessment.
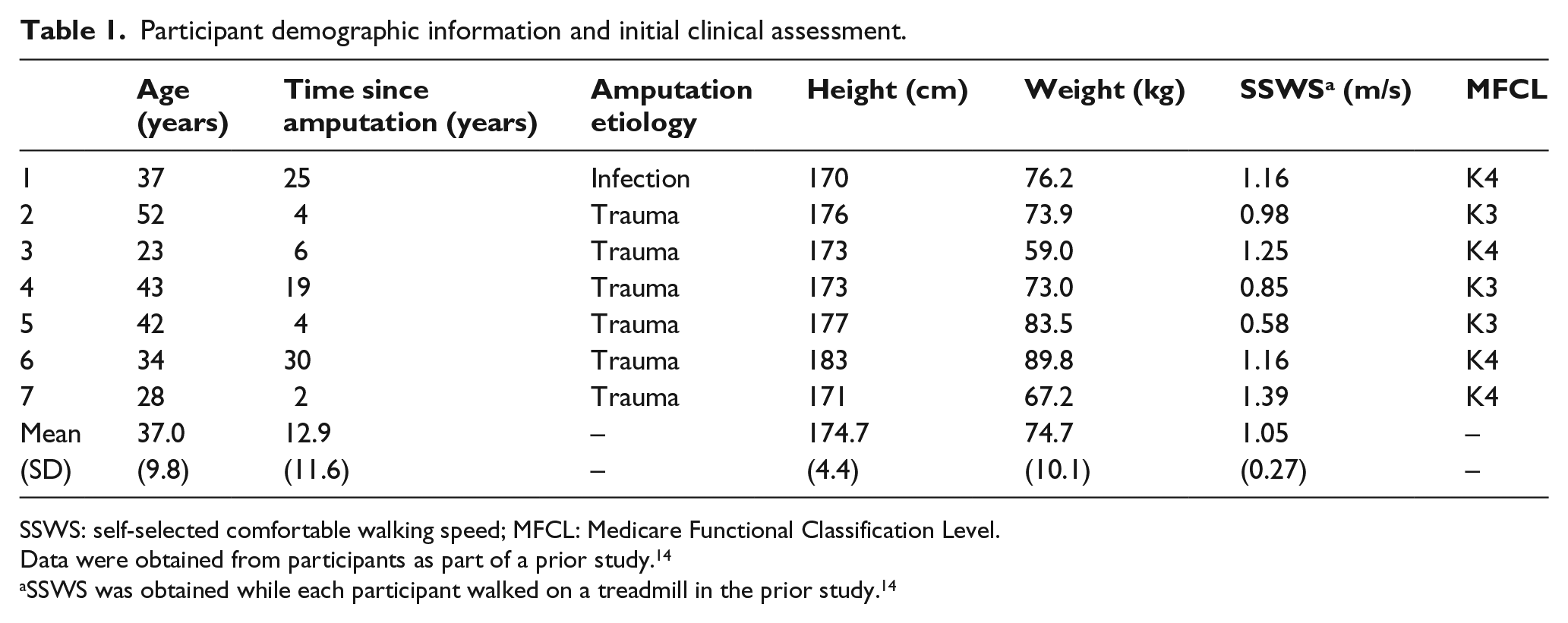
SSWS: self-selected comfortable walking speed; MFCL: Medicare Functional Classification Level.
Data were obtained from participants as part of a prior study. 14
SSWS was obtained while each participant walked on a treadmill in the prior study. 14
Individual results
More than half of the participants (n = 4) exhibited equivalent or better performance in all outcome measures when using XF compared to when using ESF (Table 2). Five out of seven participants performed better in the high-level measures (i.e. TUG-fast, FSST, CHAMP) while using XF. Mean improvements, relative to each individual’s timed performance while using ESF, were 10% during the 5×STS, 3% during the TUG-comf, 6% during the TUG-fast, and 7% during the FSST. However, none of the individual participants demonstrated differences that exceeded published estimates of minimum detectable change (MDC) for lower-limb prosthesis users in TUG times (3.6 s) or CHAMP scores (3.74 points).20,25 Population-specific MDC estimates for other measures (i.e. 5×STS, FSST) were not available for comparison.
Participant and group performance for all outcomes.
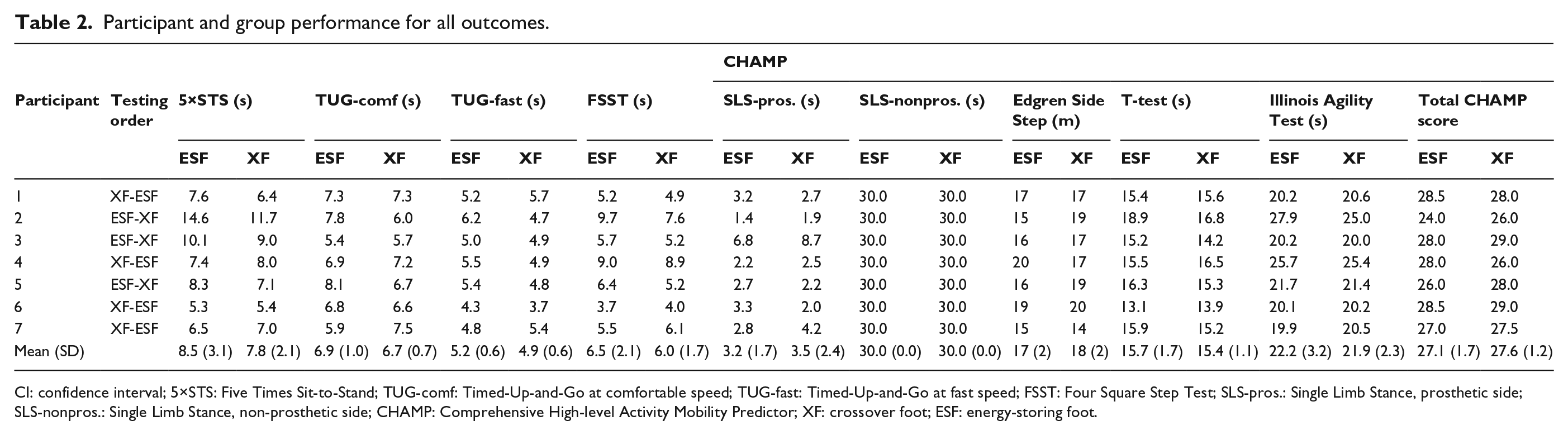
CI: confidence interval; 5×STS: Five Times Sit-to-Stand; TUG-comf: Timed-Up-and-Go at comfortable speed; TUG-fast: Timed-Up-and-Go at fast speed; FSST: Four Square Step Test; SLS-pros.: Single Limb Stance, prosthetic side; SLS-nonpros.: Single Limb Stance, non-prosthetic side; CHAMP: Comprehensive High-level Activity Mobility Predictor; XF: crossover foot; ESF: energy-storing foot.
Group results (by intervention)
On average, participants completed the timed performance outcome measures (i.e. 5×STS, TUG-comf, TUG-fast, FSST) faster while using XF compared to ESF (mean difference range: 0.2–0.8 s; Figure 1). Mean CHAMP scores were also improved in XF compared to in ESF. However, none of these differences were statistically significant (all p > 0.1).
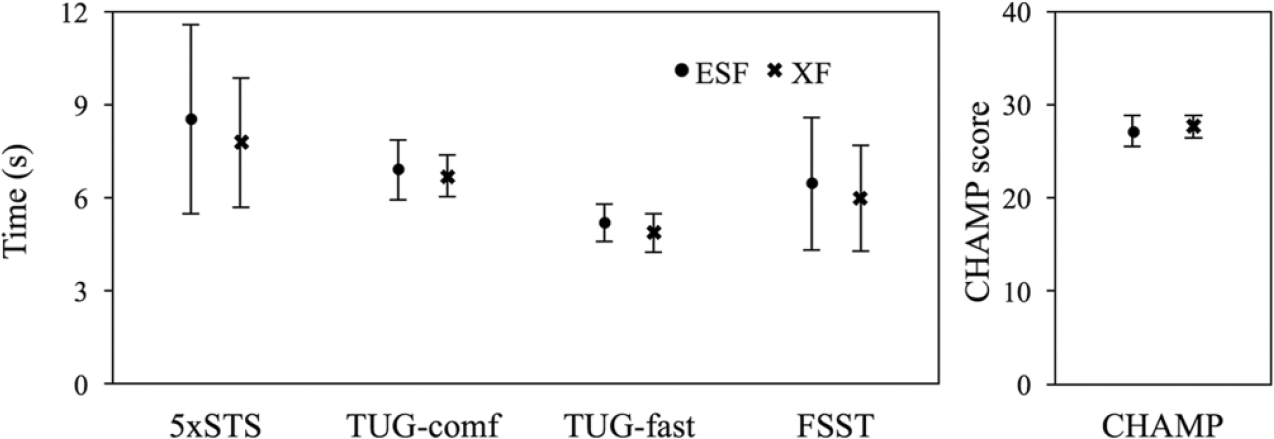
Mean group performance (n = 7 participants) on all outcomes. Faster completion on the timed tests reflects better performance, while higher scores on the CHAMP instrument reflect better performance. 5×STS: Five Times Sit-to-Stand; TUG-comf: Timed-Up-and-Go at comfortable speed; TUG-fast: Timed-Up-and-Go at fast speed; FSST: Four Square Step Test; CHAMP: Comprehensive High-level Activity Mobility Predictor.
Group results (by order of testing)
On average, participants completed the timed outcome measures (i.e. 5×STS, TUG-comf, TUG-fast, FSST) faster when using the second prosthesis compared to the first, regardless of foot (mean difference range: 0.3–0.7 s; Tables 2 and 3). Mean CHAMP scores in the second prosthesis were also improved compared to in the first. Although none of these differences were statistically significant (p ≥ 0.05), results suggest an effect due to order.
Group mean differences (n = 7 participants), 95% confidence intervals, and effect size for all outcome measures by foot comparison and by order of testing.
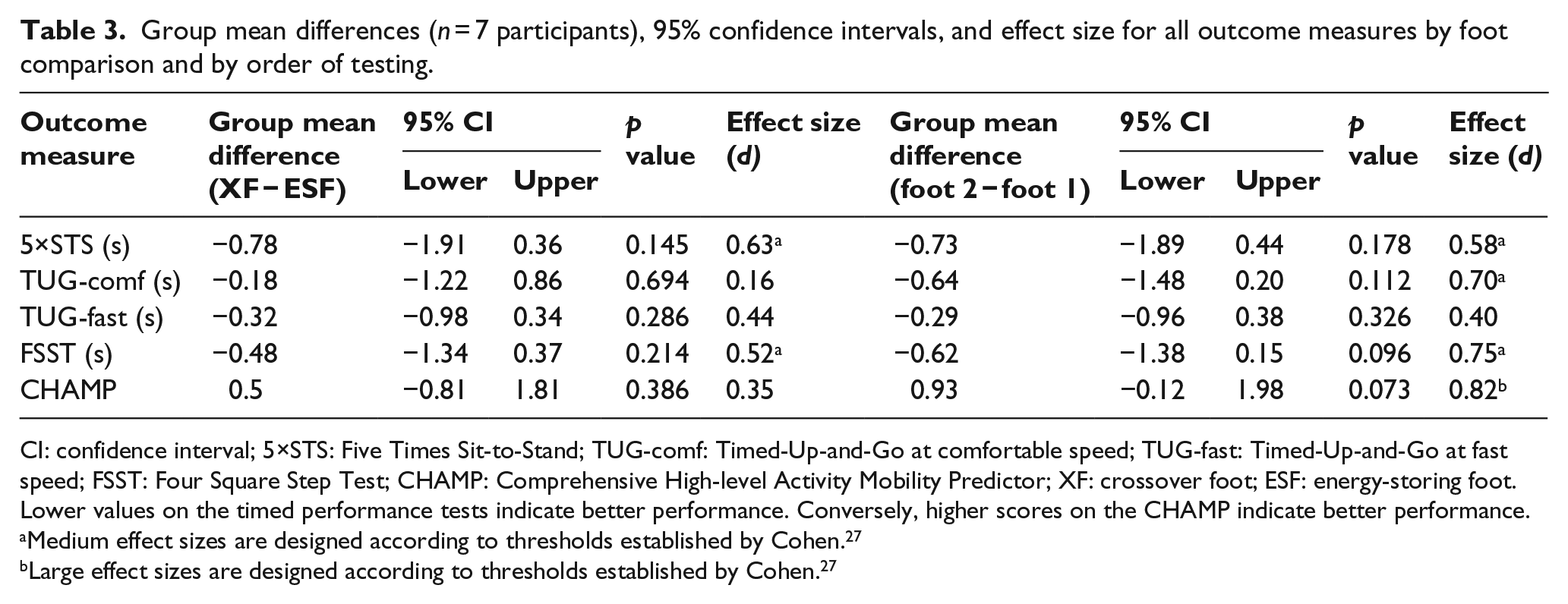
CI: confidence interval; 5×STS: Five Times Sit-to-Stand; TUG-comf: Timed-Up-and-Go at comfortable speed; TUG-fast: Timed-Up-and-Go at fast speed; FSST: Four Square Step Test; CHAMP: Comprehensive High-level Activity Mobility Predictor; XF: crossover foot; ESF: energy-storing foot.
Lower values on the timed performance tests indicate better performance. Conversely, higher scores on the CHAMP indicate better performance.
Medium effect sizes are designed according to thresholds established by Cohen. 27
Large effect sizes are designed according to thresholds established by Cohen. 27
Discussion
The purpose of this study was to compare the performance of individuals with unilateral TTA using XF and ESF across a range of low- and high-level mobility tests. Results of this study suggest that use of XF may be associated with slight improvements in low-level (e.g. sit-to-stand, walking short distances, turning around a cone) and high-level (e.g. quick-stepping, jogging, side-stepping) activities. However, while many individuals in this study performed the standardized outcome measures better when using XF, overall differences between XF and ESF did not reach significance in this sample of seven individuals.
It was hypothesized that users’ performance on low-level activities would be equivalent between foot conditions and significantly improved in high-level activities when using XF. Results of this study partially support this hypothesis since equivalent performance in both prosthetic feet was observed during low-level activities. However, individual and average percentage differences in performance between foot conditions on the high-level timed outcome measures (i.e. FSST, TUG-fast) were not greater than differences between feet in the low-level measures (i.e. 5×STS, TUG-comf). Results of the TUG tests may also be compared to assess the hypothesis that XF would improve users’ performance in high-level activities, since the tests are identical except for the speed at which each test is performed. The findings from the two TUG tests indicate that use of XF resulted in a larger effect, in terms of Cohen’s d, 27 during fast speed walking (d = 0.44, small effect size) than during comfortable speed walking (d = 0.16, no effect). Equivalent TUG-comf times and lower TUG-fast times may indicate that users are able to vary their walking speeds slightly more in XF than ESF. However, additional testing with a larger sample would be needed to confirm this hypothesis.
Interestingly, the test that exhibited the largest effect with the XF relative to the ESF was the 5×STS (d = 0.63, large effect). The 5×STS was initially characterized in this study as a low-level test but may be more indicative of high-level performance due to how participants were asked to perform the test (i.e. “as quickly as possible,” see Appendix 1). One possible reason for the observed difference between feet on the 5×STS could be that the XF design improves kinetic symmetry between the prosthetic and non-prosthetic limbs relative to the ESF. Significant asymmetries in sit-to-stand movements have been reported in people with TTA relative to people without amputation.28,29 Instrumented testing of participants in XF and ESF would be required to confirm this hypothesis and identify which components of sit-to-stand (e.g. seat off, deceleration 28 ) are most affected by foot design.
Participants in this study were generally younger, more active, and had more experience using TTA prostheses than prosthesis users often included in prior studies.20,21,25,30 Therefore, the data collected using performance-based outcome measures of mobility in this sample are consistently faster, or higher scoring, than previously published findings using similar outcome measures. For example, the mean FSST and TUG completion times in this sample were twice as fast as the mean times reported in Dite et al. 30 Similarly, the CHAMP scores recorded in this sample were higher than those reported for a sample of transtibial amputees in Gailey et al., 25 but lower than scores reported for active military personnel without amputation evaluated in the same study. Results of this study are important because they contribute data about the performance of active males with unilateral TTA which have not previously been represented in the literature. However, differences in the present sample and those included in previous studies challenge interpretation of these findings because MDC estimates were established in lower-mobility samples of individuals with dysvascular-related TTA and may not provide appropriate context.20,25
This study was intended to explore the effect of XF on high-level mobility activities not included in prior studies.13,14 Given the pilot nature (i.e. limited time and resources) of this study, a cross-sectional study design was used. Administering the selected performance-based measures within a single session resulted in an order effect. The effect was deemed by the investigators to be a practice effect that resulted from participants’ learning how to perform the outcome measures over repeated assessments. 31 Regrettably, practice effects associated with performance-based measures do not appear to be well studied, with a few notable exceptions. Gill and McBurney, 32 for example, found that both a 30-s standing test and 50-foot walk test required at least one practice trial before measuring people scheduled for lower limb orthopedic surgery. Kristensen et al. 33 found that at least two practice trials would be needed to administer the TUG to patients with hip fractures. Sawers and Hafner 34 recently reported that lower limb prosthesis users would need at least five trials on a narrowing beam walking test.
The practice effects found in this study varied across outcome measures, with the largest effect observed on the CHAMP composite score (d = 0.82, large effect) and the smallest effect observed on the TUG-fast (d = 0.40, small effect). However, it should be noted that the practice effect observed in the studied instruments does not necessarily imply they exhibit poor test–retest reliability. For example, Gailey et al. 25 found excellent test–retest reliability with the CHAMP (ICC = 0.97), but tests were administered on separate days, with 24–72 h between. Thus, administration of performance tests on different days may help to mitigate practice effects and should be considered whenever possible. The small effect observed on the TUG-fast may be because it was performed immediately following the TUG-comf. Practicing the same test again, albeit at a different speed, may have helped to stabilize participants’ performance on the TUG. As there was ultimately no measurable effect due to order on the TUG-comf, four trials may have been sufficient to mitigate the practice effect for this task.
Directions for future work
The findings of this study reveal that investigation into practice effects associated with the use of performance-based outcome measures in this population is needed. In addition, there is a dearth of information regarding consistent and standardized instructions for administration of performance-based measures, including the number of trials recommended for practice and which trial(s) to use to determine an individual’s level of performance. 35 These issues may challenge use of outcome measures for assessing and comparing prosthetic interventions in clinical practice. Use of performance-based measures in comparative effectiveness research in prosthetics may also be affected, as the impact of practice effects and scoring techniques on individual performance is not well-understood. Finally, establishing normative scores and estimates of meaningful change (e.g. MDCs and minimum important differences) for existing performance-based measures with a range of individuals with lower limb amputation is needed to improve clinicians’ and researchers’ ability to interpret important health outcomes. Addressing these challenges will inform both clinical application of outcome measures and their use in research.
Study limitations
One limitation of this work is the small sample size. However, it should be noted that this sample size is about average relative to other prosthetic foot studies, which have generally included between 3 and 16 participants. 7 As primary studies, many of these studies are likely to be under-powered or limited by methodological issues (e.g. practice effects like those observed in this study). This may explain why comparative effectiveness studies of this kind often report few significant differences between groups or between prosthetic interventions. However, pilot studies like this can also be used to revise data collection protocols and conduct a priori power analyses to support larger studies which can adequately assess the effect of an intervention in this population. The group differences observed in this study indicate that a minimum of 21 participants would need to be recruited for a future study to have 80% power to detect differences on all of the outcomes measures (i.e. 5xSTS, TUG-comf, TUG-fast, FSST, and CHAMP) at an α level of 0.05. The practice effects observed in this study also suggest that administering performance-based measures in a cross-sectional, repeated measures study design is not ideal. Future studies should attempt to mitigate learning effects by administering performance-based outcome measures during separate sessions (and randomize order of testing across the participants). In the event that cross-sectional data collection is necessary, participants may require additional practice trials on performance-based outcome measures. 31 However, as repeated practice trials may also introduce fatigue, research is needed to characterize the inter-related effects of practice and fatigue on performance testing in people with TTA.
Conclusion
The results of this study suggest that the use of XF may be associated with small improvements in performance-based mobility outcome measures across low- and high-level activities compared to use of the clinical standard ESF. These results support previous findings and indicate that use of XF may extend the range of activities in which individuals with unilateral TTA can participate using a single prosthesis. Future research, employing alternative study designs and/or including a larger sample of individuals, is warranted to substantiate the findings of this study. Practice effects were observed across all outcomes, with participants demonstrating improved performance during subsequent test attempts. Further research regarding practice effects and performance-based outcome measures in lower limb prosthesis users is indicated.
Footnotes
Appendix 1
Acknowledgements
The authors wish to acknowledge Angelina Boulicault, BS, Geoff Balkman, CPO, and Elen M. Feuerriegel, PhD for assistance with data collection; Greg Davidson, John Shaffer, and Ryan Blanck for donation of fabrication time and materials; and Össur ehf Iceland Research and Development for donation of prosthetic components.
Author contribution
Study concept and design: Brian Hafner, Elizabeth Halsne, Sara Morgan, Cody McDonald
Acquisition of data: Elizabeth Halsne, Cody McDonald, Sara Morgan, Brian Hafner
Analysis and interpretation of data: Elizabeth Halsne, Brian Hafner
Drafting of manuscript: Elizabeth Halsne, Brian Hafner
Critical revision of manuscript for important intellectual content: Sara Morgan, Cody McDonald, Sarah Cheever
Obtained funding: Brian Hafner
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the US Department of Defense through the Orthotics and Prosthetics Outcomes Research Program under award no. W81XWH-15-1-0458 (PI: Hafner). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Defense.
Institutional review board review
All study procedures were reviewed and approved by a University of Washington institutional review board (IRB #49150).