
Abstract
Background:
Substantial improvements have been perceived in surgical results following major lower limb amputation, but there remains observed variation in amputation quality for patients referred for prosthetic rehabilitation from different hospitals.
Objectives:
To assess various elements that influence residual limb quality and evaluate their impact on progress through initial prosthetic rehabilitation and mobility outcome after rehabilitation.
Study design:
Clinical survey.
Methods:
A revised 10-item residual limb scoring system was used to survey a succession of 95 primary amputees with transtibial and transfemoral amputations (100 residual limbs) presenting for rehabilitation.
Results:
The majority of residual limbs scored highly, supporting the perception of generally good amputation quality. There were significant differences in average residual limb scores between some hospitals. The overall scores showed weak or minimal correlation to progress through rehabilitation and mobility outcome but residual limbs scoring higher in seven of the items of the score showed significant advantages in key aspects of progress or mobility at discharge.
Conclusion:
There is need for continued collaboration between surgeons and rehabilitation centres to ensure consistent high standards. The revised residual limb score used in this survey needs further refinement for future use.
Clinical relevance
Residual limb quality is an important component influencing prosthetic rehabilitation. This survey of residual limbs at one Rehabilitation Centre suggests encouragingly good surgical results but highlights differences between hospitals. A particular issue is the need for effective collaboration between surgeons and prosthetic rehabilitation professionals to optimise residual limb preparation.
Keywords
Background
With better understanding of surgical technique and postoperative care, prosthetic rehabilitation has improved. 1 It is important, however, that the operative procedure is undertaken with the same care used in other reconstructive procedures. The importance of a sturdy soft tissue envelope and benefit of myodesis and myoplasty is well established. 2 Bony prominences should be resected and bone rasped for a smooth contour. 2 Optimal residual limb length, orientation and musculature reduces centre of mass excursion, aberrant gait and energy cost. 3 Heterotopic ossification can be a problematic in traumatic- and combat-related amputations. Many can be managed conservatively, and those with refractory symptoms benefit from surgical excision with low recurrence rate. 4 Most surgeons agree that nerves should be isolated, gently pulled and cleanly divided so that the cut end retracts well proximal to the level of bone section. 2 There is emerging evidence of the benefit of targeted muscle reinnervation (TMR) to prevent neuroma pain. 5
Although the developments above are noted, the authors have observed variation in the quality of amputation of patients referred to their centre from different hospitals. Amputees with favourable features such as optimal length, 6 bone end, muscle cover, proximal joint range and strength, vascularity and less pain progressed faster and achieved a higher Special Interest Group in Amputee Medicine 7 (SIGAM) grade.
It was felt that a tool to assess residual limb quality by rehabilitation centres would add evidence to support amputation surgery. Chakrabarty 8 proposed a scoring system for residual limb quality and identified that better quality limbs were fitted earlier and achieved their expected mobility grade sooner. He correlated quality of surgery with seniority of the surgeon. The authors revisited his system but felt that key determinants such as myodesis/myoplasty and vascularity were not included. There was also overlap between items such as shape and ‘dog-ears’ (surplus skin on either ends of amputation wound).
It was hypothesised that using the revised system, higher scores would correlate to faster progress through rehabilitation and improved mobility and that the score could guide improvement in residual limb quality.
Methods
Inclusion criteria
As this was a survey of standard of residual limb presentation, all primary transtibial and transfemoral amputees were assessed from the point of initiating the survey until a target of 100 residual limbs was reached. Both genders, any age and any cause of amputation were included. Only transtibial and transfemoral levels were included being the most prevalent and as both are transdiaphyseal – necessitating bone sectioning and muscle re-attachment – the same scoring approach could be used.
Based on guidance from the NHS Health Research Authority, this investigation fell under the category of a survey, so research ethical approval was not sought. Participants were not randomised to different groups, only standard care was delivered and the outcomes are non-generalisable.
Data collection
The survey was conducted from September 2011 until August 2012. The target was to assess amputees at their primary rehabilitation appointment. A multidisciplinary approach was taken with two clinicians scoring together: the rehabilitation consultant always led, and the same designated physiotherapist and/or prosthetist assisted (staff are the first three authors). Within usual practice for the centre, and with consent from the patient, residual limb photographs and X-rays were taken. Operation notes were accessed where possible. Scoring took approximately 15 min. After assessment, data were compiled in a database.
It is routine for the prosthetists to log casting, fitting and prosthesis delivery dates. The physiotherapists routinely record number of appointments each amputee attends for gait training, date of discharge from initial rehabilitation and three mobility outcome measures at discharge and at 6-week and 6-month follow-up appointments: SIGAM grade, Two-Minute Walk Test (TWT 9 ) and Timed Up and Go Test (TUG 10 ). SIGAM score was used in preference to Locomotor Capability Index (LCI 11 ) as it is more common in the United Kingdom. Six months after the last patient in the survey completed rehabilitation, these measures were collated, and as far as possible, SIGAM gaps were filled from clinical notes for patients who failed to keep the reviews.
Scoring system development
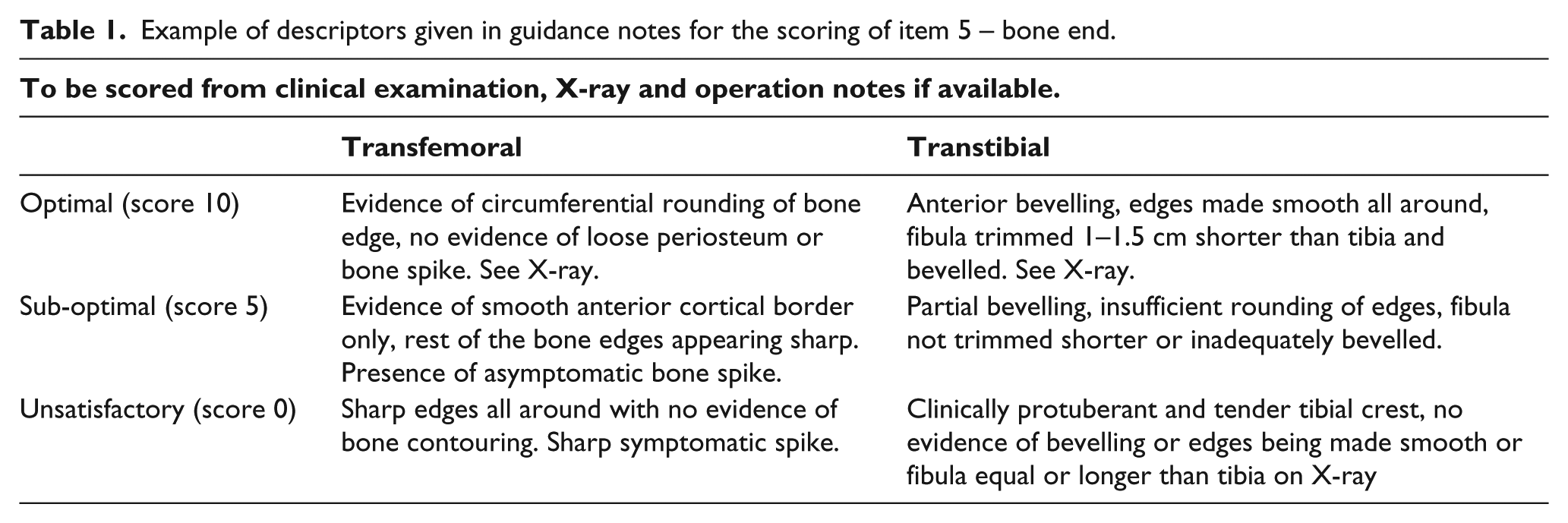
Starting from the limited literature available,8,12,13 the scoring system was refined based on the experience of a multidisciplinary amputee rehabilitation team, a key textbook 14 and in consultation with referring surgeons. In total, 10 items were identified pertinent to residual limb quality: wound/scar state, length, shape, pain/tenderness, contouring/rounding of bone end, muscle/fascia cover, proximal joint, vascularity, skin condition and sensation. Each item was scored on a 3-point scale as optimal (10), sub-optimal (5) or unsatisfactory (0). This scoring reflected the perceived level of impact of each item on the amputee’s symptoms and on progress and outcome in rehabilitation. Guidance was developed to aid consistency, giving criteria for each score drawing on knowledge of best practice for amputation surgery. 14 (Table 1 gives an example of scoring guidance. Full guidance is in the electronic appendix.) In total, 10 amputees were assessed to test the scoring and develop familiarity for the clinical team. Minor amendments were then made to the scoring and guidance.
Example of descriptors given in guidance notes for the scoring of item 5 – bone end.
Data analysis
Data manipulation utilised Microsoft Excel 2003. Amputation causes were grouped into six categories: congenital, dysvascularity, infection, neoplasia, neurological disorder and trauma. Information gathered from department databases enabled calculation of days between key stages of rehabilitation. SIGAM grades were converted to an 11-point ordinal scale for analysis (Table 2). Normal distribution patterns could not be assumed, so non-parametric analysis methods were used, accepting this may have reduced the power of analysis (performed with Minitab v13).
Progress measures through rehabilitation and outcome measures at discharge from rehabilitation (DC) and at 6-week and 6-month follow-up appointments.
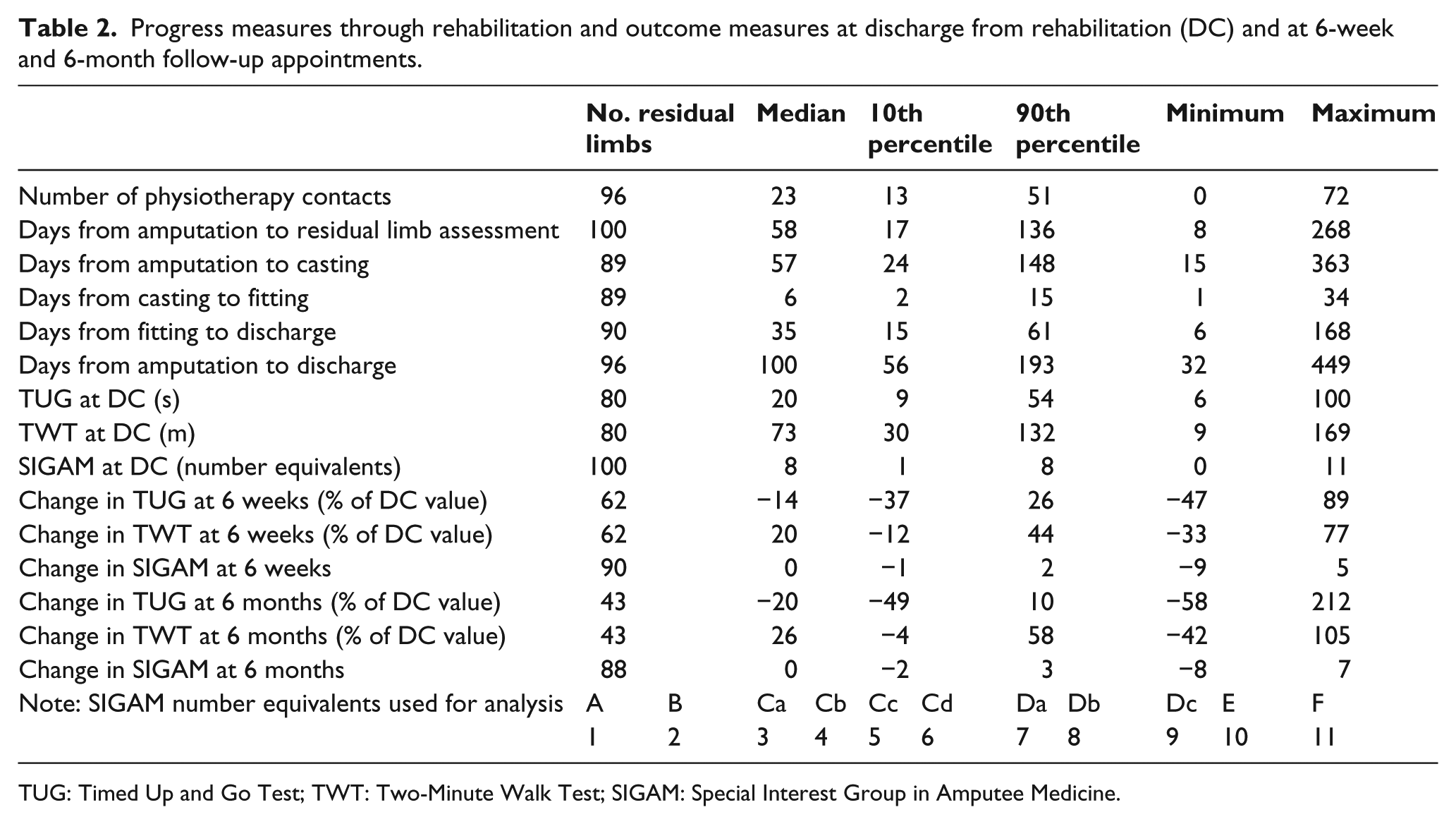
TUG: Timed Up and Go Test; TWT: Two-Minute Walk Test; SIGAM: Special Interest Group in Amputee Medicine.
The Kruskal–Wallis test compared total scores for the three main causes of amputation – dysvascularity, infection and trauma (other causes had too few data points to be included) – and compared scores for each referring hospital (those with one or two amputations were grouped together as ‘other’). Where significant difference in median score was indicated between groups (p < 0.05), the Mann–Whitney test was employed for comparison of each pair combination, with Bonferroni correction. The Mann–Whitney test was also used to compare total scores for the two levels of amputation, and the two surgical methods for transtibial amputation (transfemoral amputations were performed with one dominant surgical method).
Spearman rank correlation coefficients were generated to explore correlation between total residual limb score and each of age, progress measures through rehabilitation, outcome measures at discharge and change in outcome measures at 6 weeks and 6 months. In the absence of clear criteria, the following descriptive terms were used for the strength of positive correlation: 0–0.25 ‘minimal’, 0.25–0.5 ‘weak’, 0.5–0.75 ‘moderate’, 0.75–1 ‘strong’ (and equivalent intervals for negative correlation).
For each of the items within the score, the amputations were split into two groups: those scoring 10 and those scoring 5 or 0. The Mann–Whitney test was applied to explore whether there were significant differences between the groups in terms of age, progress through rehabilitation, mobility outcome at discharge or change in mobility at 6 weeks or 6 months.
Results
Distribution of total scores across the 100 limbs was positively skewed (Figure 1) with most scoring relatively highly; the lowest score being 45. Figure 2 gives scores for each of the 10 survey items. A total of five residual limbs could not be scored for item 5 (bone end) because X-rays were not available, and two of these could not be scored for item 6 (muscle cover). Apart from item 5, all items had more than 50 residual limbs given a score of 10. In all items, a score of zero was seldom applied (less than 10 residual limbs in each), and items 2 (length) and 7 (proximal joint) did not have any residual limbs scoring zero.
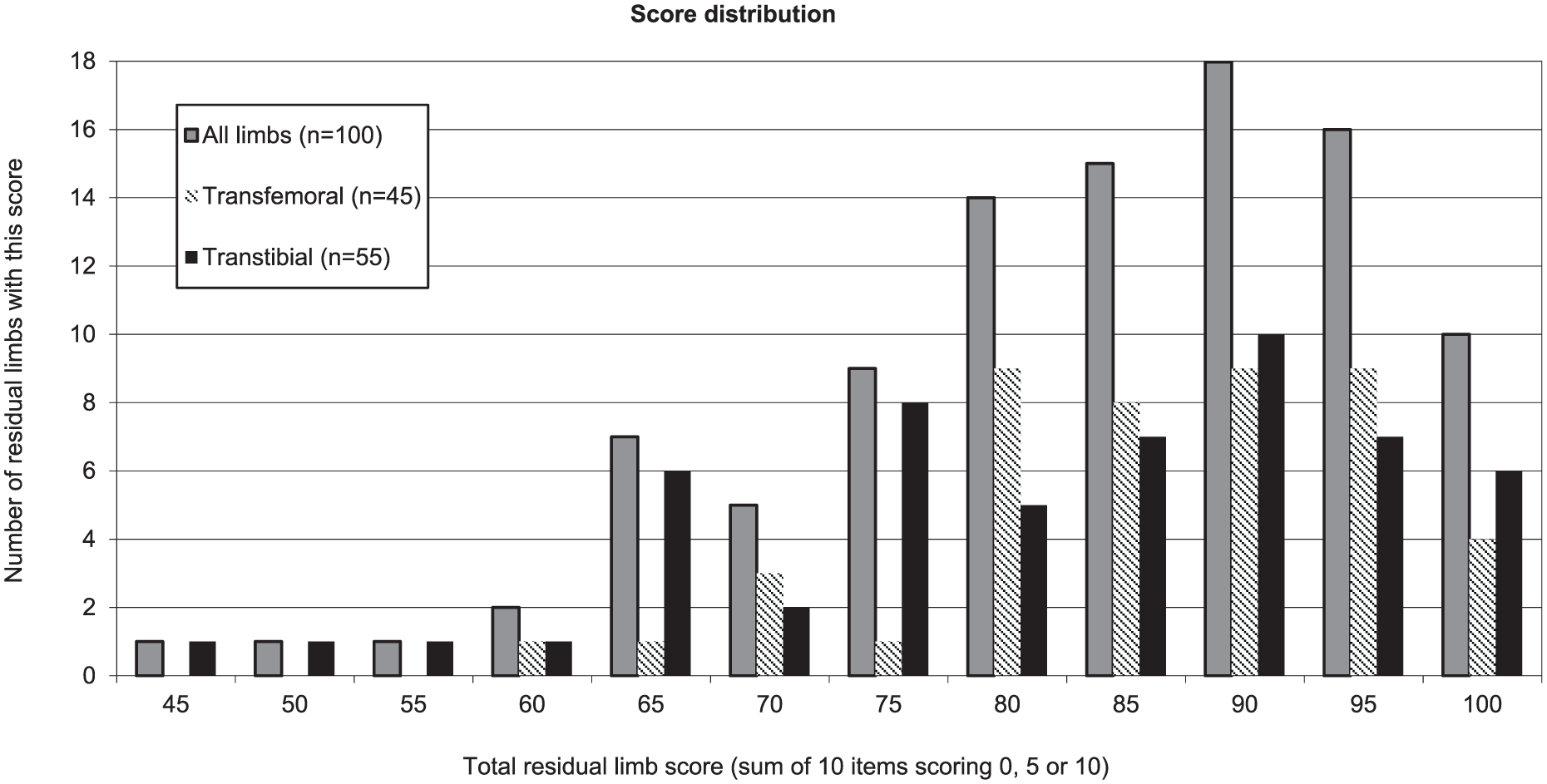
Histogram showing distribution of total limb scores for the 100 residual limbs. Data are shown for all limbs and are also broken down into transfemoral and transtibial limbs.
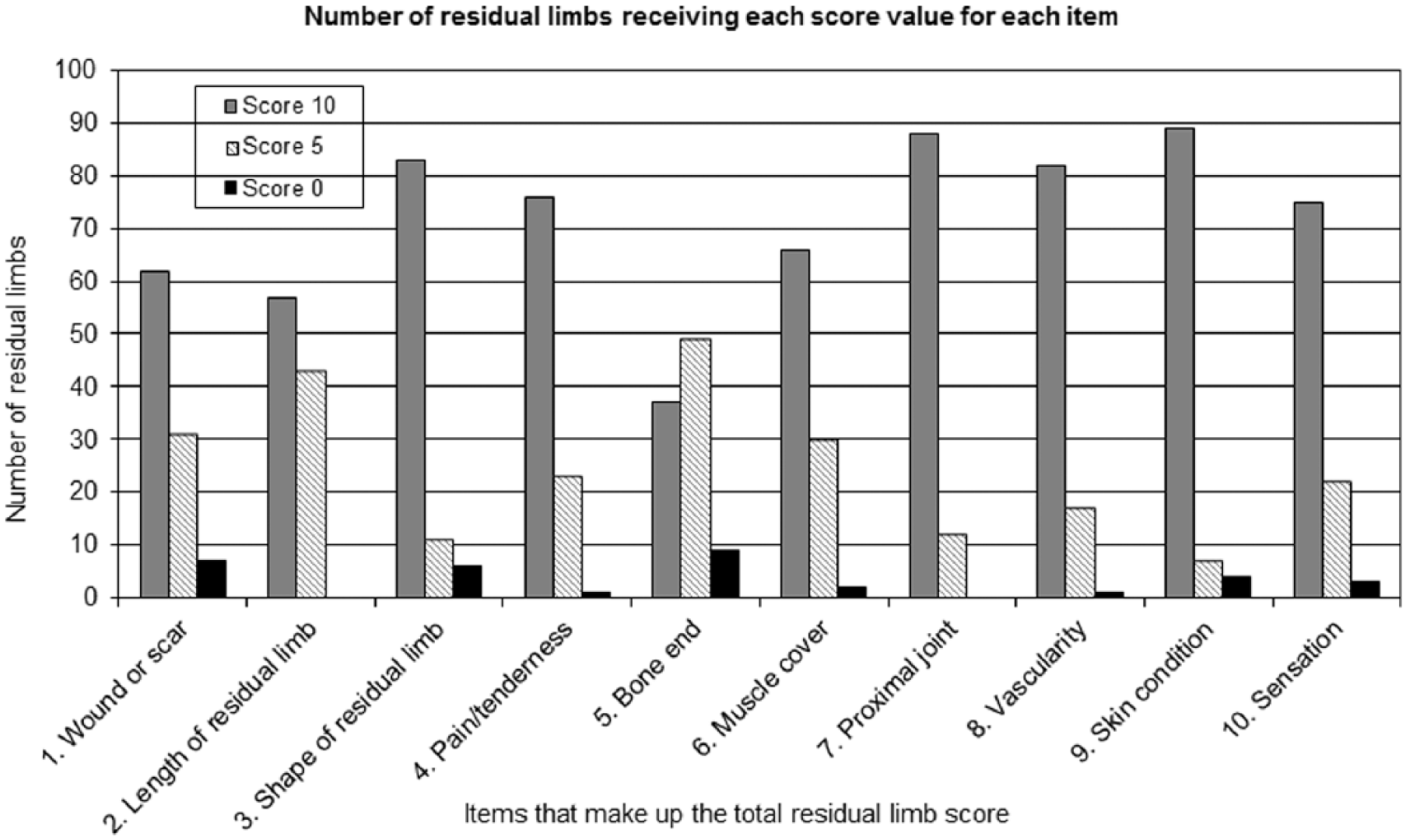
Number of residual limbs receiving each score value (0, 5 or 10) for each of the 10 items across the 100 residual limbs.
Figure 3 gives cohort characteristics divided into age range, cause of and surgical method for amputation. The residual limbs represented 95 individuals, with 5 people having bilateral amputation at differing levels and time stages. In total, 55 amputations were transtibial.
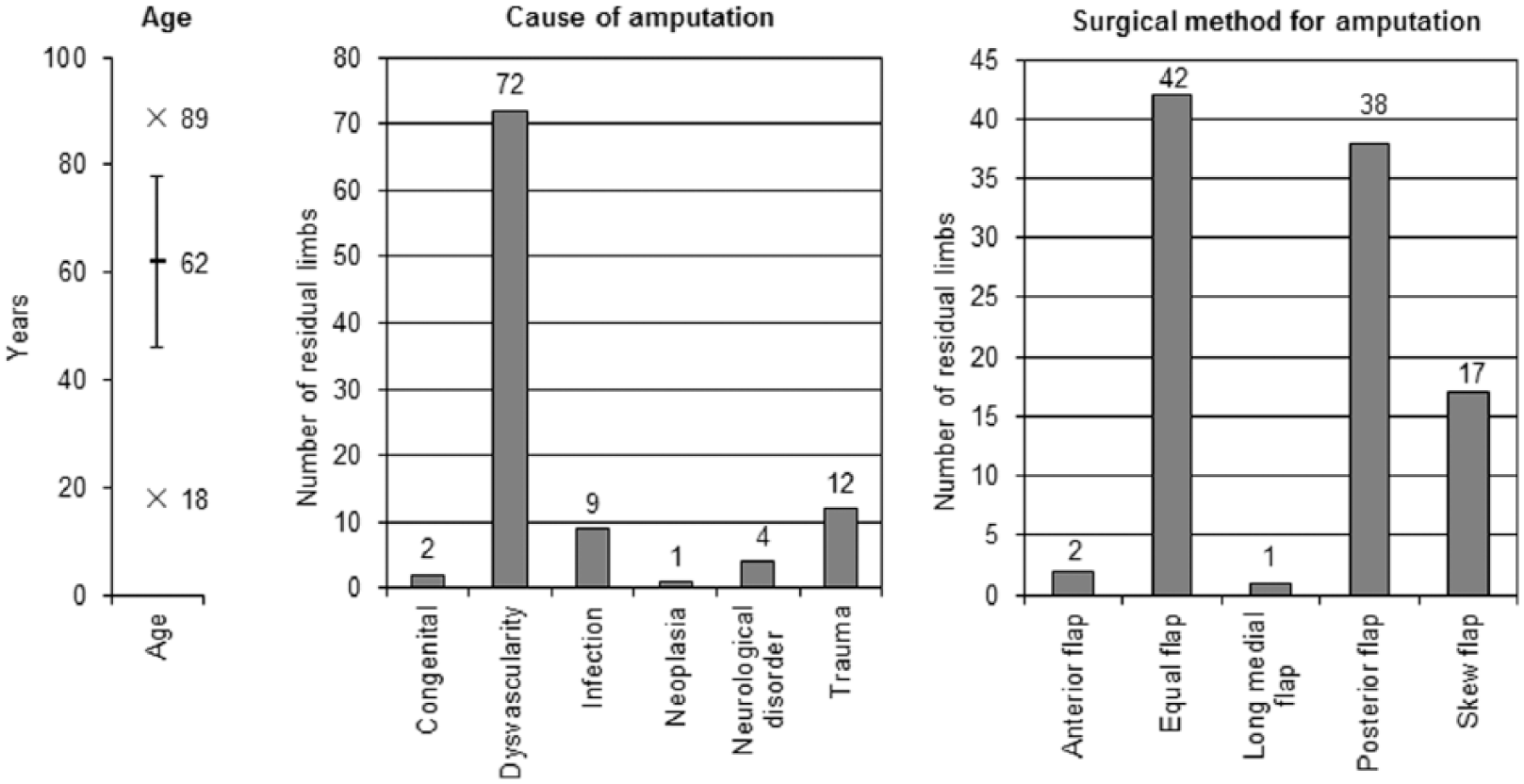
Summary of cohort characteristics (95 individuals, 100 residual limbs). Age given as mean (line) ± 1 standard deviation (error bars), maximum and minimum (x).
All six categories of amputation causes were represented, but dysvascularity was predominant. Kruskal–Wallis test between the three main causes (dysvascularity n = 72, trauma n = 12 and infection n = 9) did not indicate significant differences in total residual limb scores.
Amputations were performed by 25 surgeons at 16 hospitals; the majority came from six hospitals, with the other 10 referring only one or two individuals (grouped together as ‘other’ for seven-way analysis). Kruskal–Wallis test indicated a significant difference in total score between at least one pair of hospitals (p = 0.011). Mann–Whitney tests of each pair showed that one hospital had a higher median score than all others (p < 0.05 for all six comparisons), but this was significant for only two pairs with Bonferroni correction applied (p < 0.002). This particular hospital saw mainly orthopaedic cases with a high ratio of trauma aetiology (5 of 13) and only 1 dysvascularity case.
There was no significant difference in total scores between transfemoral and transtibial levels. At transtibial level, two surgical techniques were employed: posterior flap (n = 38) and skew flap (n = 17). The skew flap limbs had significantly higher median score (90 compared to 80, Mann–Whitney p = 0.0008). However, there was a significant difference in median age (53 years – skew – compared to 68 years – posterior, Mann–Whitney p = 0.0042) and different distribution of cause of amputation, posterior flap predominantly for dysvascularity (78%), while skew flap more evenly distributed between trauma (29%), dysvascularity (29%) and neurological disorder (24%).
Table 2 gives descriptive statistics of progress and outcome measures for the cohort. The intention was to score when patients first presented to the centre. In reality, 47 residual limbs were cast (i.e. rehabilitation began) before being scored, with gaps between 1 and 50 days.
Regarding progress measures, 96 residual limbs had record of discharge date from rehabilitation, and the other 4 were non-ambulant and did not go through prosthetic rehabilitation. Casting and fitting dates were only found for 89 and 92 residual limbs, respectively – it was unclear in other cases whether dates were not recorded or casting/fitting were not carried out. All patients were assigned a SIGAM grade at the point of discharge except for one who died before discharge. TUG and TWT outcome measures were collected for 80 residual limbs, with the others being non-ambulant (SIGAM A or B). As the Centre has found to be typical, there was subsequent drop-off in the numbers seen for all three outcome measures at 6 weeks (n = 64) and 6 months (n = 45). This corresponds to a drop-off of 14.9%/44.7% and 27.3%/42.4% at 6 weeks/6 months compared to discharge for the transtibial and transfemoral groups, respectively. Reasons include patients not attending, attending but needing prosthesis revision or being lost to the system. Where possible, SIGAM grades were assigned based on interpretation from patient notes (9 patients at 6 weeks and 15 at 6 months). A total of two individuals died before six-month follow-up.
Spearman rank correlations showed weak or minimal correlation between total residual limb scores and each of age, measures of progress through rehabilitation, outcome measures at discharge and change in outcome measures over time.
Considering the individual items, when split between those scoring 10 and those scoring 5 or 0, significant differences were indicated (Table 3). For length, those scoring 10 showed significantly lower age, higher TWT values and higher SIGAM grades at discharge. For pain/tenderness, those scoring 10 showed significantly higher SIGAM grades at discharge. For bone end those scoring 10 took significantly fewer days to progress from amputation to casting, from casting to fitting and consequently from amputation to discharge and showed significantly higher SIGAM at discharge. For muscle cover, those scoring 10 took significantly fewer days to progress from amputation to casting and consequently from amputation to discharge and showed significantly higher SIGAM at discharge. For proximal joint, those scoring 10 took significantly fewer days to progress from amputation to casting and from casting to fitting, but difference in progress from amputation to discharge was not deemed significant. This group showed significantly lower TUG and higher TWT values at discharge. For vascularity, those scoring 10 showed significantly higher TWT values and SIGAM grades at discharge. For skin condition, those scoring 10 required significantly fewer physiotherapy contacts during rehabilitation. There were no significant differences at 6 weeks and 6 months, which probably correspond to the drop-off in patients for the two levels of amputation; these were very similar at 6 months.
Significant differences between survey items and measured outcome results for those items scoring 10 and those scoring 5.
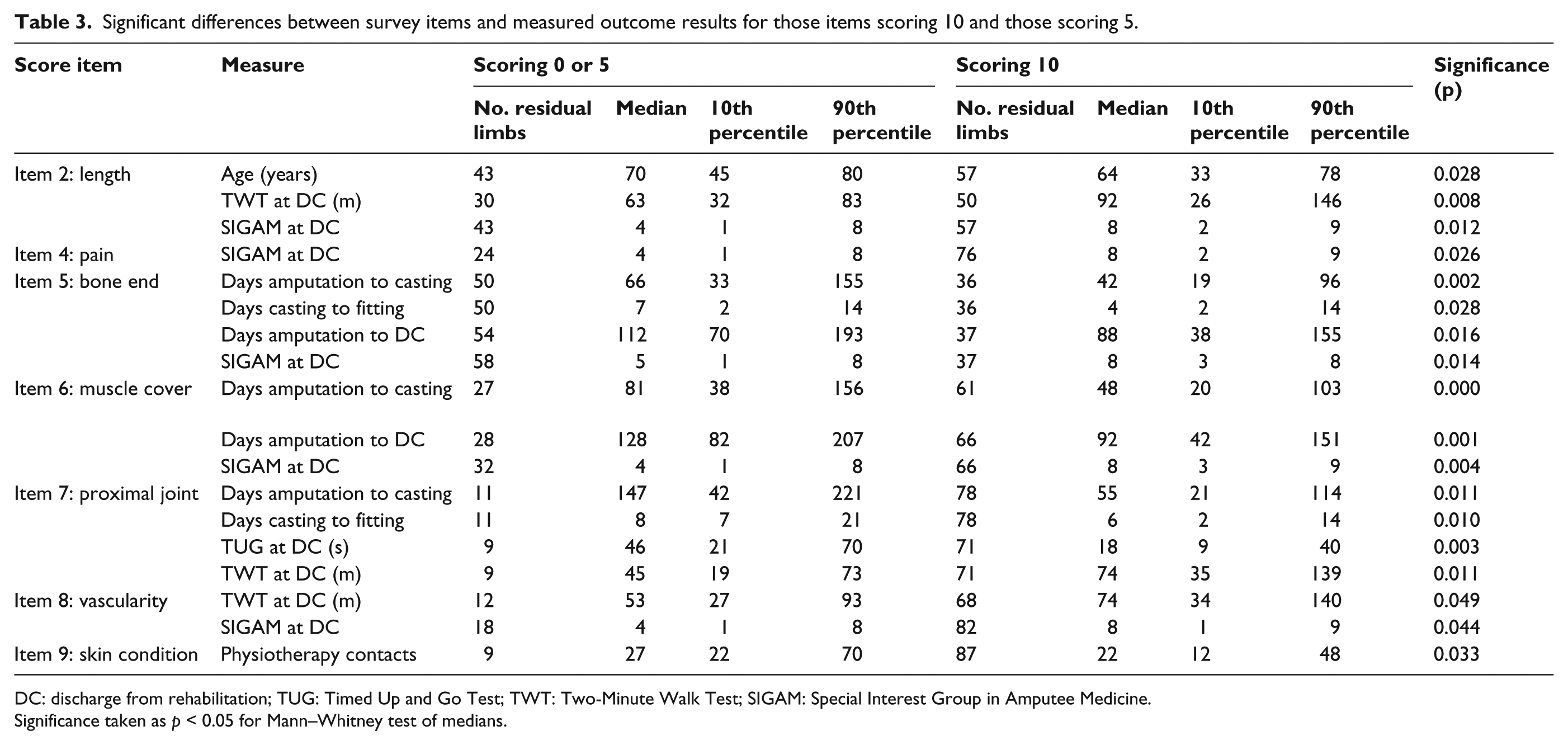
DC: discharge from rehabilitation; TUG: Timed Up and Go Test; TWT: Two-Minute Walk Test; SIGAM: Special Interest Group in Amputee Medicine.
Significance taken as p < 0.05 for Mann–Whitney test of medians.
Discussion
Recent trends of age and aetiology in UK lower limb amputees are matched in this cohort. 15 Moxey et al. 16 noted a variation of transtibial-to-transfemoral ratio across English health authorities of 0.73–1.21. The cohort in this study had a ratio at the favourable end (1.22), similar to previous years for the Centre.
The overall high scores reflect a generally good quality of surgery producing limbs satisfactory for rehabilitation. This is perceived as an improvement in the field over the last 2–3 decades, credited to the Royal College of Surgeons incorporating amputation surgery in surgical training 17 and improved communication between surgical and rehabilitation departments. In this study, a significant difference between hospitals was found. The highest median score was from one hospital where most amputations were carried out by a senior surgeon working closely with the rehabilitation centre. As expected, both transdiaphyseal amputation levels showed similar scores highlighting similarities in technique. At transtibial level, the significantly higher scoring of the skew flap technique is consistent with the experience of the authors in respect to early prosthetic fitting; however, this has not been investigated formally, for example, through multi-centre trials.
Chakrabarty 8 showed amputees with good quality residual limbs progressed quicker and achieved a better outcome. The weak or minimal correlation of overall score to measures of progress and outcome in this survey is possibly explained by the complex interaction of a variety of factors such as age, co-morbidities and psycho-social issues.
The hypotheses for the total limb score are not supported by the results. However, seven of the individual items showed significant differences in progress and outcomes at discharge between limbs scoring highly (10) and those scoring lower (5 or 0). Those scoring higher for length, bone end, muscle cover, pain, proximal joint, vascularity and pain progressed quicker through rehabilitation and had higher mobility grade (SIGAM) at discharge. Those scoring higher on skin condition required fewer physiotherapy contacts during rehabilitation. It is speculated that this may relate to fewer issues during the prosthetic fitting process. The lack of significance for the individual items at 6 weeks and 6 months is possibly due to the decreased sample size available for analysis.
Bone end was the lowest scoring item across the cohort, highlighting this key element for surgical training. This was also the hardest item to score as operative notes were often unavailable or did not describe the degree of bone contouring. Clinical examination and X-rays provided the required information for scoring of bone end and muscle cover (Figures 4 and 5). X-rays were not available in five cases. The authors believe that, standardising operation notes and where possible, obtaining X-rays is important. The notes should provide details of skin flap design, bone length and contouring, method of nerve section, myoplasty and myodesis. This would facilitate audit of postoperative symptoms to amputation technique by rehabilitation clinicians. The four items less directly influenced by the surgeon are sensation, proximal joint, vascularity and skin condition.
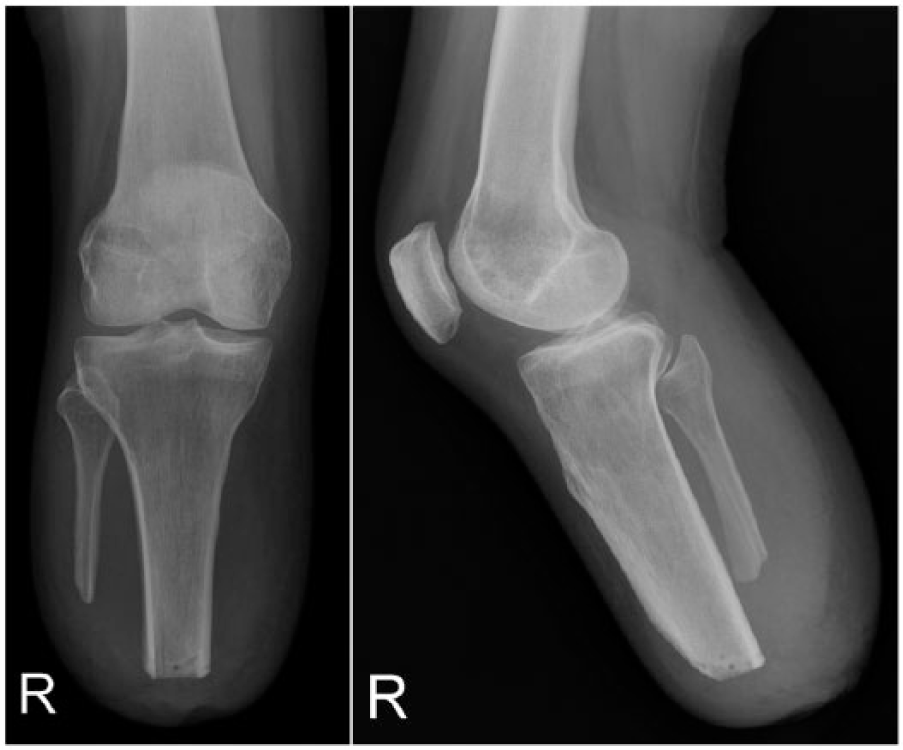
X-ray example of an optimal transtibial residual limb showing tibial circumferential chamfering, anterior cortical bevelling, drill hole for myodesis, fibula sectioned 1–1.5 cm proximal to tibia with oblique cut avoiding sharp lateral end and adequate soft tissue cover of the bone ends (myoplasty).

X-ray example of an optimal transfemoral residual limb showing no bone spur, circumferential rounding, drill hole for myodesis and adequate soft tissue cover (myoplasty).
A total of three items did not show significant differences in progress and outcomes: wound/scar, shape and sensation. This is surprising, particularly regarding progress through rehabilitation, as problems in these areas would be expected to cause delays. It may be that these aspects are less influential than expected, or their influence is masked or managed by other factors, for example, early postoperative oedema control or prosthetic socket accommodation of limb imperfections.
Given that the overall score showed minimal correlation but certain individual items were associated with better progress and outcomes, further work should consider weighting and possible removal of items. Even with weighting a strong correlation may be difficult to achieve due to the complexity of influencing factors/comorbidities. 18 This may be addressed through a larger multi-centre study and incorporating a quality-of-life measure such as Trinity Amputation and Prosthesis Experience Scales (TAPES 19 ). It is possible that the 3-point scoring system led to range attenuation effects and limited the correlations, 20 so use of an extended scoring approach could be considered.
The strengths of this study are the cohort representing national incidence, similar results between the two most common levels of lower limb amputation and identifying specific areas to feedback to surgeons (standardising operation notes and improving bone end contour 2 ). The difficulties with amputations in emergencies are acknowledged by rehabilitation clinicians. The need for an effective, ongoing, working relationship with prosthetic rehabilitation teams is also noted.
The main limitations of this survey are use of unvalidated, non-weighted scoring items and subjective scoring of items. When the survey was developed, the authors considered that it had face validity as the residual limb score items were based on best evidence and expert clinical opinion (see section ‘Methods’). In addition, although repeatability was not assessed formally, the scoring was based on the consensus of experienced clinicians, with a collective experience of over 70 years in a major UK amputee management unit.
There were some delays in initial scoring, drop-off in patients at 6-week and 6-month follow-up, lack of standardised operation notes, dependence on X-rays and the scoring not being done by all three assessors. A follow-up of outcome measures beyond the 6-month point would also be instructive.
Conclusion
This survey found a generally good quality of amputation surgery, but there was variation between referring hospitals. The total residual limb score showed weak or minimal correlation to progress and mobility outcome, and three items showed no significant differences for higher or lower scoring residual limbs. Residual limbs that scored higher in seven items showed significant advantages in important aspects of progress through rehabilitation or mobility outcome at discharge. Of these items, three are directly related to surgical decision and technique: length, bone end and muscle cover. Of these, bone end had the lowest score and feedback by rehabilitation clinicians to surgeons, for example, through teaching on surgical courses and in audit presentations at clinical meetings, to achieve optimal contour of bone end and myodesis/myoplasty is important.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.