
Abstract
Background:
Different recommendations exist regarding what age is best for first-time fitting of myoelectric hand prostheses in children.
Objectives:
To compare prosthetic skill, prosthetic use and risk for rejection over time between children fitted with myoelectric hand prostheses before or after 2½ years of age.
Study design:
Prospective case-control design.
Methods:
The cases were nine children fitted with myoelectric hand prostheses before the age of 2½ years, whereas the controls were 27 children who were fitted with myoelectric hand prostheses after the age of 2½ years. The Skills Index Ranking Scale was used to classify prosthetic skill, and prosthetic use was categorised based on wearing time and pattern. Independent samples tests were used to compare data between groups. To estimate and compare the risk of prosthesis rejection between groups and over time, survival analysis was used.
Results:
Cases showed prosthetic skill early, but controls had caught up by the age of 3½ years. Cases had a significant (p = 0.046) decrease in prosthetic use at the age of 9 years. In the long term, cases had a higher percentage of prosthesis rejection.
Conclusions:
Considering young children’s development of prosthetic skill and prosthetic use over time, this study shows no additional advantages from fitting a myoelectric hand prosthesis before 2½ years of age.
Clinical relevance
Children may be fitted with myoelectric hand prostheses to assist in daily tasks and to prevent future over-use problems. Most children fitted with myoelectric hand prostheses before 4 years of age become regular users. No advantages of fitting myoelectric hand prostheses before 2½ years of age were observed.
Background
Children with transversal upper limb reduction deficiency (TULRD) are recommended to be fitted with hand prosthesis at an early age because prosthesis use encourages motor learning and prosthetic integration into the body scheme. However, there is an ongoing debate concerning the optimal age for first-time fitting of myoelectric hand prostheses (MEP). 1 This article is an attempt to determine the impact of two different recommendations of first-time fitting of MEP on promoting successful rehabilitation with respect to prosthetic skill development and continual prosthetic use.
The prevalence of children with TULRD is estimated at 3.8/10,000 live births, 2 with a dominance of unilateral deficiency below the elbow.3,4 Using the unaffected side and the residual limb for daily task performance may result in over-use problems. 5 However, access to a functional prosthesis, for example, an MEP, is considered to reduce this over-use and affect adjustment to the deficiency by facilitating independence. 6 Compared to normative data, children with MEP have similar psychosocial adjustment. 7 Furthermore, they have the same opportunities in education and employment 8 as their peers. Provision of MEP to children has, thus, become standard practice in the Swedish health care system.
The fitting of a passive hand prosthesis by the age of 6 months is commonly recommended,9,10 and it is believed that early fitting of a passive hand prosthesis is a factor affecting continual prosthetic use. However, the recommended age for first-time fitting of an MEP is not fully established in the literature. In Scandinavia, the recommended age for MEP fitting is from 2½ to 4 years; 11 the rationale being that fitting an MEP at this age range would promote continual prosthetic use and adequate prosthetic skill to perform daily tasks. In North America, it is recommended that fitting of an MEP take place as early as 10–15 months of age.9,12 The rationale for this early fitting is that the children will be more able to use the prosthetic hand. Both recommendations have been used clinically in different parts of the world. However, no study has compared the impact of the two recommendations in terms of child development in prosthetic skill and continual prosthetic use.
Two factors may influence continual prosthetic use. One factor is the age of first-time fitting of the MEP. A Swedish cohort in 1992 10 showed that the lowest rejection rate was in individuals fitted with the MEP between the ages of 2 and 4 years, the same result as was shown later by Egermann et al. 13 Another factor that can influence prosthetic use is prosthetic skill. The relationship between prosthetic use and prosthetic skill has been previously explored.14,15 However, little is known about whether the age of first-time MEP fitting has any impact on prosthetic skill development in the short- and long-term. Furthermore, does age at first-time fitting have any impact on prosthetic use over time? The aim of this study is therefore to compare prosthetic skill, prosthetic use and risk of rejection over time between two groups of paediatric myoelectric prosthesis users fitted at different ages.
Methods
Design, participants and procedure
A prospective case-control design was chosen for the study. Cases were children fitted with an MEP before 2½ years of age (early MEP fitting), and controls were children fitted with an MEP after 2½ years of age. The following criteria were used to recruit children for early MEP fitting: (1) congenital TULRD below the elbow, (2) use of a passive hand prosthesis from 6 months of age and (3) living within 250 km of the fitting centre to decrease travel time. Nine children met the criteria for the case group. A control group of children fitted according to the regular procedure, that is, fitted after the age of 2½ years, were recruited according to the first two criteria. To increase the power of the study, the number of controls was multiplied by three, which gave a total of 27 children in the control group. Both groups of children were fitted with an Otto Bock 2000 prosthetic hand with a two-site myoelectric control system. Other than a passive hand prosthesis from 6 months of age, no other type of prostheses was provided to this sample. Participant demographics are presented in Table 1.
Participant demographics.
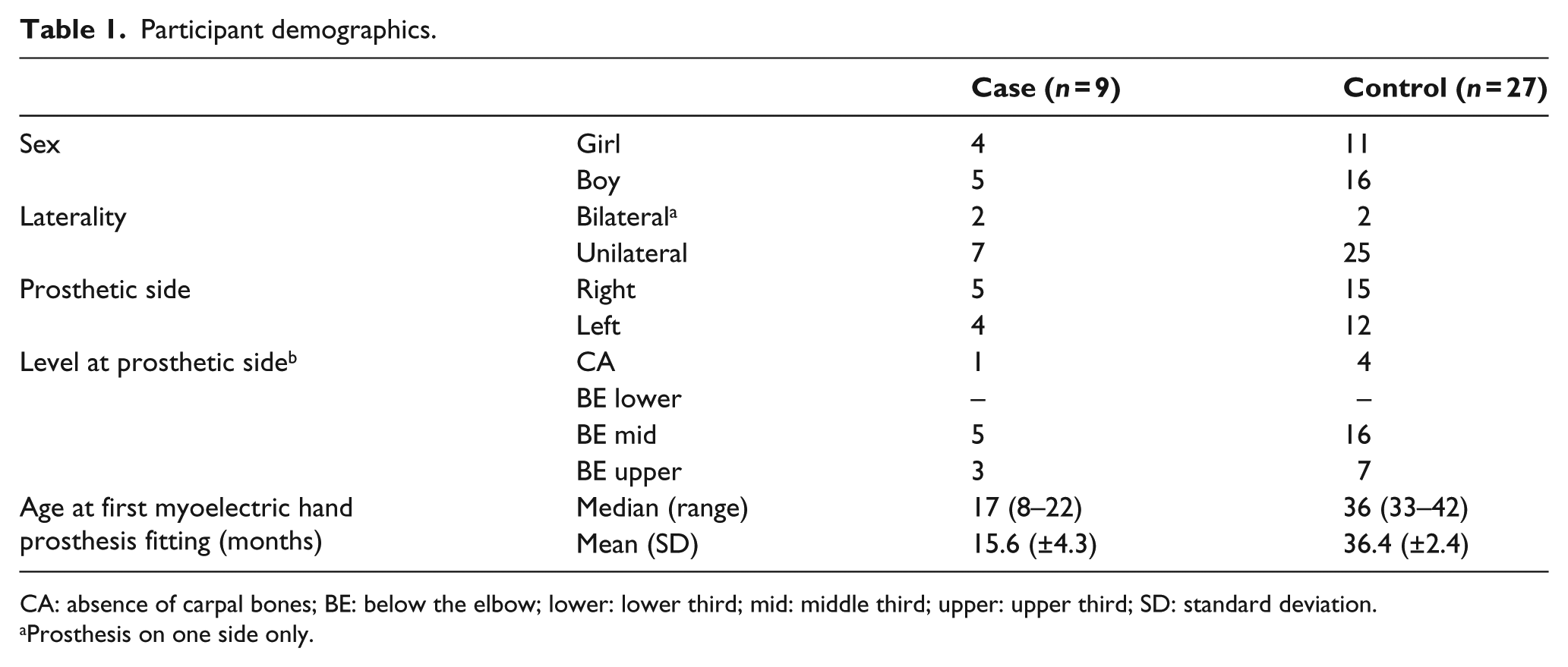
CA: absence of carpal bones; BE: below the elbow; lower: lower third; mid: middle third; upper: upper third; SD: standard deviation.
Prosthesis on one side only.
Recruitment continued over a period of 8 years (1994–2002). During the first regular control for follow-up of use of the passive prosthesis, parents of children who fit all three inclusion criteria were given oral and written information about the study and were asked whether they wished their child to have an early fitting of an MEP. All the parents who were offered an early fitting accepted. Parents of children who fit the first two inclusion criteria were given oral and written information about the study during a regular follow-up visit and decided on a regular MEP fitting. They were asked whether data from their child’s regular fitting could be part of the study. After agreeing to participate, their children were fitted with MEP according to plan, and follow-up data were collected and registered in the patients’ files. The casting procedure was the same for both groups: during a regular visit to check up on prosthetic fit and use, a new socket was made. After 3 weeks, the fitting of the MEP occurred at the clinic. The case group was fitted between 8 and 22 months of age, and the control group was fitted between 33 and 42 months of age (Table 1). The information given to the parents about MEP maintenance and use was the same in both groups.
Both groups of children received structured training from 3 years of age. Follow-up visits to assess the development of prosthetic skill and prosthetic use were made every 3 months until the cases turned 3 years. Between the age of 3 and 6 years, the case and the control groups were followed-up every 6 months, and after the age of 6 years, follow-ups were scheduled based on the concomitant need for service or training. Data on prosthetic skill and prosthetic use were collected by four specialised occupational therapists and recorded from the child’s first fitting to the following 17 years.
Due to the study design, there were some missing data at the follow-up visits. With respect to prosthetic skill, four patients were lost to follow-up: in the case group, one from the age of 9 years and two from the age of 12 years; and in the control group, one from the age of 12 years. All of these losses were caused by prosthetic rejection. By the last follow-up visit, another four subjects in the control group had been lost: three due to prosthetic rejection and one who moved to another clinic.
The study was approved by the Örebro County Council Ethical Review board (D-nr 500: 16 349/01) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. Before inclusion, informed consent was obtained from the parents and/or the children themselves.
Outcome measures
The Skills Index Ranking Scale (SIRS), an observation-based method used to categorise a person’s ability to operate an MEP, was used to assess prosthetic skill.3,16 The SIRS consists of 14 levels (Figure 1) ranging from ‘wears the prosthesis’ (level 1) to ‘throws objects from above the shoulder’ (level 14) scored as either pass or fail. Based on observations of the child during play or other daily tasks, the occupational therapist assesses which level the child has reached. The validity of the SIRS has been evaluated, and the ordering of the levels, that is, the difficulty of each level, has been confirmed (unpublished data, 1997).
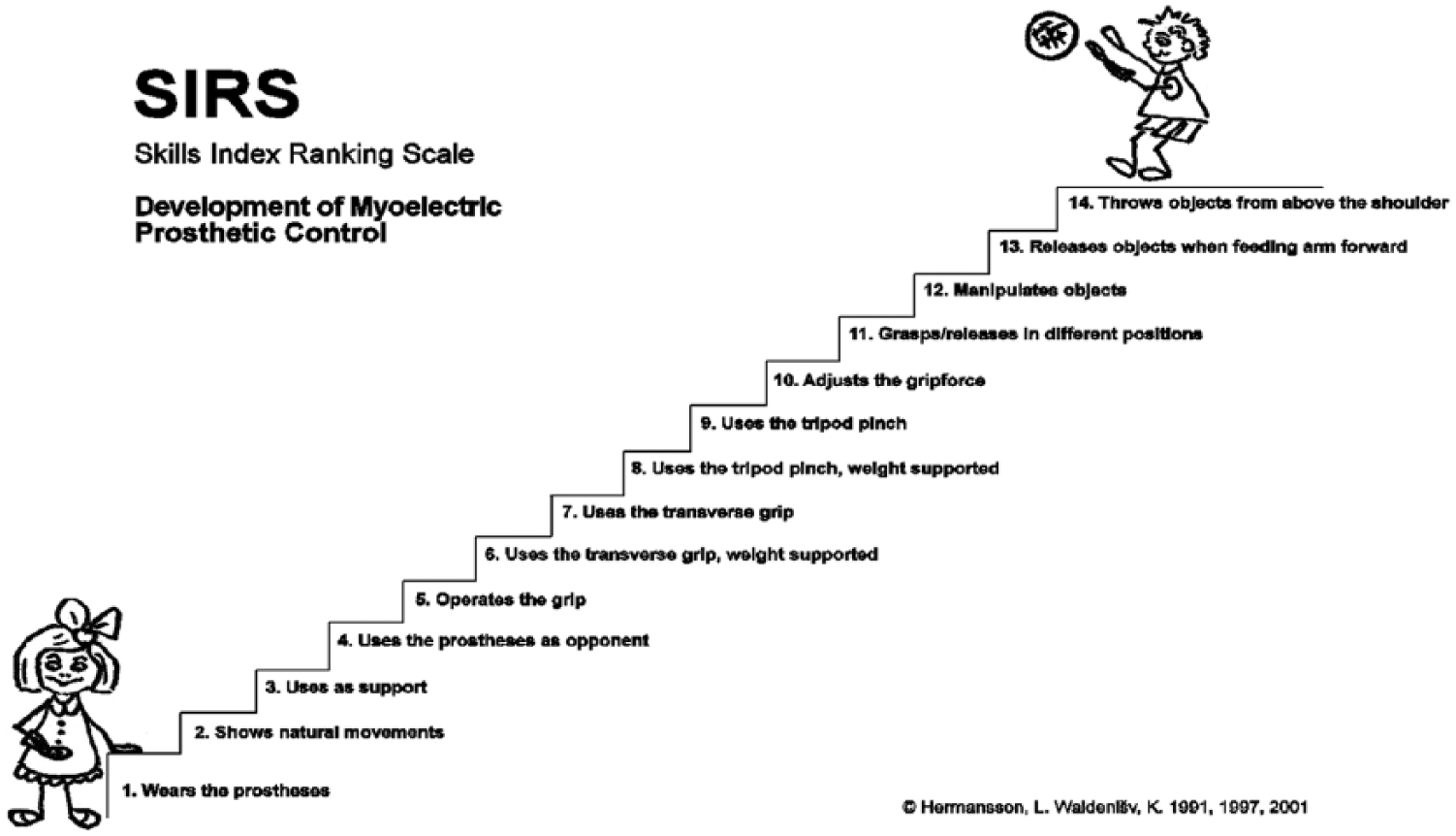
Skills Index Ranking Scale.
The children’s prosthetic use was categorised over time. Prosthetic use was based on both wearing time (how long) and when the prosthesis was used, and scoring ranged from 1 to 5: 1 = full time, more than 8 h per day, 7 days a week; 2 = part time, 4–8 h/day, 5–7 days a week; 3 = occasional, less than 4 h/day, 1–7 days a week, but regularly for one or more specific situations or tasks; 4 = sporadic, some time every month, randomly; or 5 = non-user, not used during the last month. On the basis of the parents’ or the child’s reports, the occupational therapist categorised the child’s prosthetic use.
Statistical analysis
Since the two groups were not completely matched, we used independent samples tests to compare between groups. Hence, the Mann–Whitney U test was used to compare the groups based on age, prosthetic skill and prosthetic use (significance level p < 0.05). Statistical analyses were performed using the SPSS for Windows, version 23.0 (IBM, Inc., Armonk, NY, USA).
To estimate the risk of prosthesis rejection in the cases compared to the controls, we used survival analysis (using STATA 13.0). Prosthetic rejection was defined as those patients who were categorised as non-users. First, a Kaplan–Meier graph plot was produced to visualise the percentage of prosthesis rejection in each group. Second, the risk of rejection was expressed using a hazard ratio (HR), which measured the risk of rejection in the case group compared to the risk of rejection in the control group over time.
Results
Prosthetic skill increased over time and varied between the groups (Figure 2), although with no statistically significant differences between the groups. At 3½ years of age, when all the controls had been fitted, the median SIRS level was 7 in the cases (interquartile range (IQR): 5–10) and 8 in the controls (IQR: 7–9; p = 0.604). The case group reached SIRS level 5 operates the grip at 12 to 39 months of age (median 24, IQR: 21–33 months), whereas the control group reached SIRS level 5 at 33–45 months of age (median 36, IQR: 36–39 months). At 12 years of age all but one subject in the case group and all but two subjects in the control group had reached the highest skill, SIRS level 14.
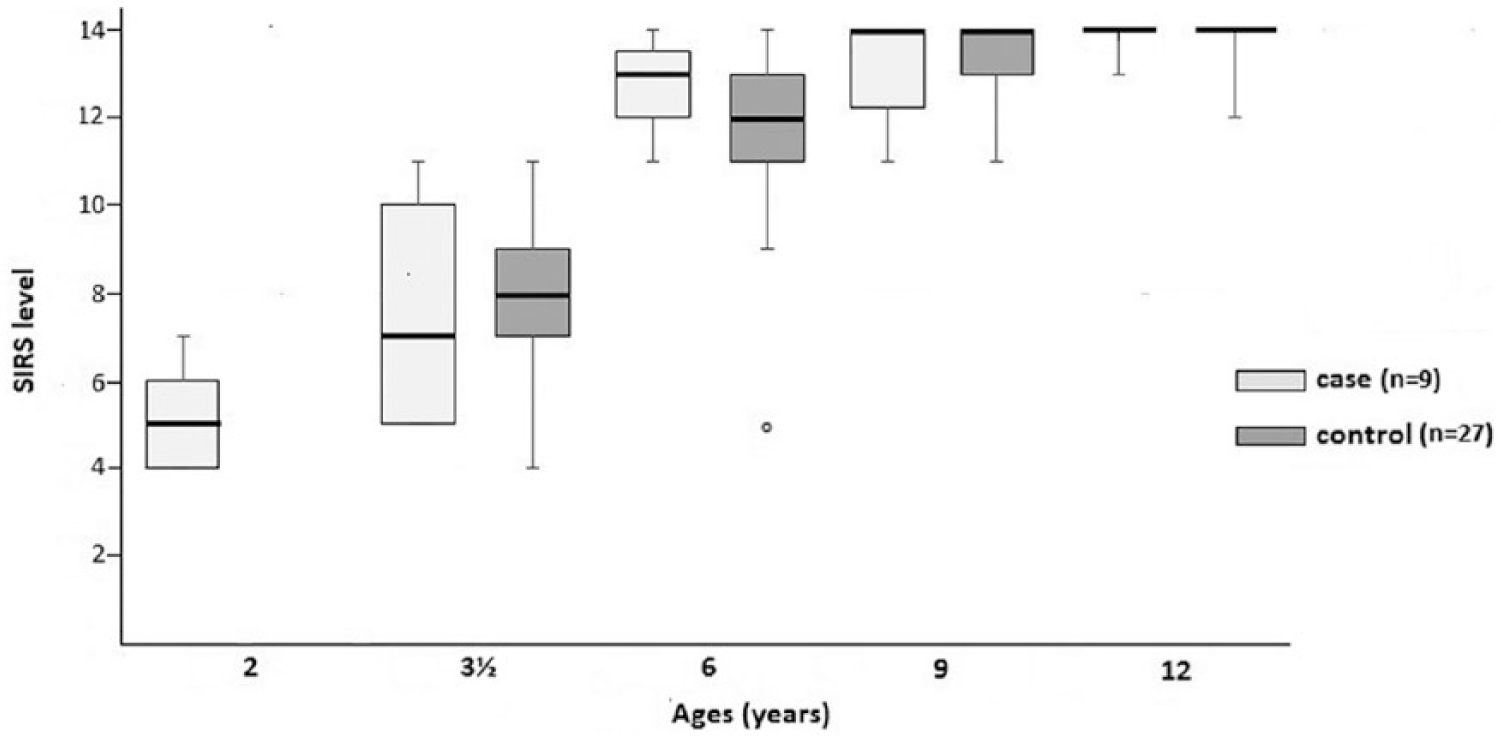
Development of myoelectric prosthetic skill as measured by Skills Index Ranking Scale (SIRS, range 1–14) at five different ages (years); comparisons between two groups – cases, children fitted at 8–22 months of age (n = 9) and controls, children fitted at 33–42 months of age (n = 27). The median value is shown as the line in the box, with the 25th and 75th percentile as the lower and upper hinges, respectively. The ‘whiskers’ indicate the range of the values, whereas the circle shows one extreme value. (At the age of 2 years, only cases were fitted, hence there is no result from the controls.)
There was a statistically significant difference in prosthetic use between the groups; at 9 years of age, the cases had a lower use compared to the controls (p = 0.040). Overall, there was an increasing and wider range of prosthetic use within the case group (Table 2). After 17 years from first-time fitting, the median value for prosthetic use was 2.00 (IQR: 1.00–4.00) in the case group and 1.00 (IQR: 1.00–4.00) for the control group; a statistically insignificant difference p = 0.370.
Prosthetic use at various ages – comparisons between children fitted with myoelectric hand prosthesis before versus after 2½ years of age.
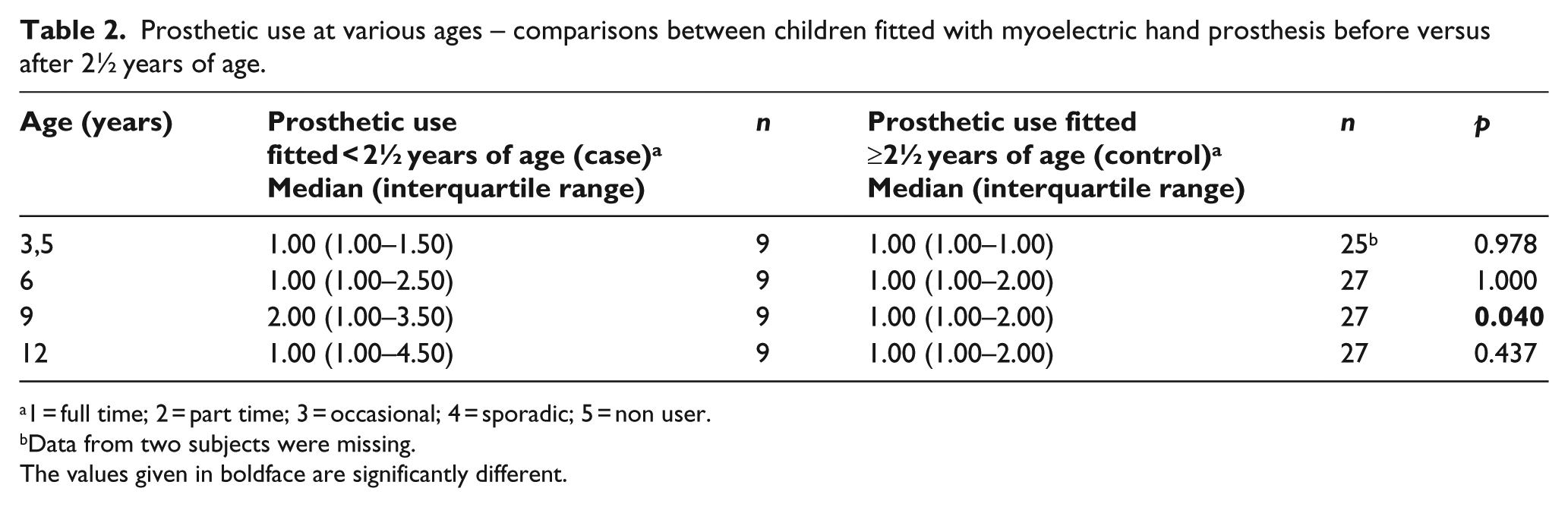
1 = full time; 2 = part time; 3 = occasional; 4 = sporadic; 5 = non user.
Data from two subjects were missing.
The values given in boldface are significantly different.
Of the 36 children, 7 (19.4%) rejected their prosthesis during the study period. The first rejection occurred in the case group after 7 years and 9 months of wearing the prosthesis, and it occurred when the child was 9 years old. When comparing the two lines (Figure 3), the cases had a higher percentage rejecting their prostheses than the controls. The risk of rejection was expressed as an HR of 2.83; that is, the case group had a 2.83 times higher risk of rejection compared with the controls. However, the 95% confidence interval (CI: 0.63–12.8) showed that the difference in risk was not significant.
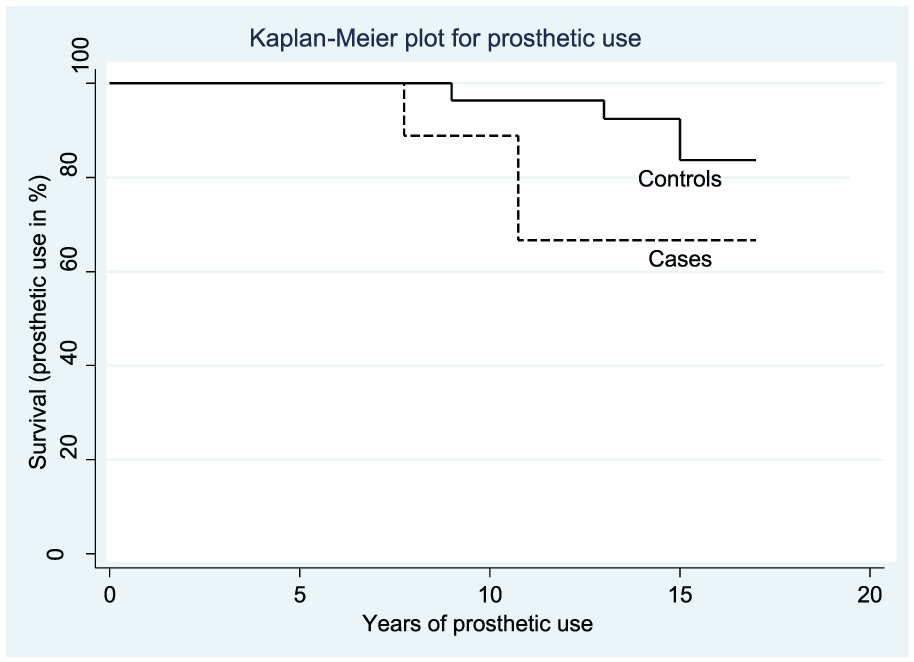
Kaplan–Meier plot showing the percentage of prosthetic use over time (years) measured in terms of cumulative survival figures in two groups – cases, children fitted before 2½ years of age (n = 9) and controls, children fitted after 2½ years of age (n = 27). A drop indicates the end of myoelectric prosthetic use (rejection) by a child. First rejection occurs in the case group after wearing the myoelectric prosthesis for 7 years and 9 months; 17 years from fitting time, more than 60% of cases and 80% of controls are using their myoelectric prosthesis.
Discussion
To the best of our knowledge, this report describes the first prospective study comparing prosthetic skill, prosthetic use and risk of rejection over time between children fitted with MEP before and after 2½ years of age. Despite the small sample size, we found no difference in prosthetic skill development, but we did find a significant difference in prosthetic use at 9 years of age. In the long term, after 17 years, more than 80% of all children were still using their MEP.
The overall findings indicate that children seem to learn to operate an MEP with a similar developmental pattern irrespective of age at first fitting. When fitted at an early age, children learned to operate the grip early, but there was a large variation within the group. In comparison, most children fitted after the age of 2½ years were immediately able to operate the grip, and the variation in prosthetic skill development was smaller within this group. The results suggest that fitting before the age of 2½ years can result in earlier prosthetic skills, but children fitted after 2½ years of age do progress faster and catch up with their peers within 1 year. However, the results need to be interpreted with caution.
This study is the first prospective study that compares two groups in which all the participants had received the same prosthetic options – first passive prostheses and thereafter MEP – with the only difference being the child’s age at first fitting of the MEP. This difference allowed us to focus on age as the main factor for the outcome. The results confirm earlier reports10,11,13 stating that the best age for MEP fitting is between 2½ and 4 years. In contrast to an earlier study, 17 the results from this study suggest that early fitting of an MEP (before the age of 2½ years) may have a negative impact on the future use of the MEP. In a meta-analysis, 18 it was found that a first fitting before 2 years of age generally leads to a lower rejection rate (pooled odds ratio (OR): 1/3.6), which is also supported by other studies.19,20,21 These conflicting results may be explained by the study sample populations – the previous studies were performed using heterogeneous samples containing children fitted with either passive-, body-powered or myoelectric prostheses, whereas this study sample was homogeneous. In this study, only children undergoing a first-time fitting of MEP were included. Despite limitation, we found a difference in prosthetic use between the groups at the age of 9 years. This result coincides with the so-called 9-year depressive crisis, 22 an existential crisis that occurs when children are able to understand their situation and compare themselves to other children. Some children are more affected than others, but we found no reason to believe that there was an over-representation of the 9-year crisis in the case group. The decrease in prosthetic use was also shown in the survival analysis. This result demonstrated a tendency towards a higher risk of rejection in the case group compared to the control group. Still, the overall rejection rate was lower compared to other studies.17,19,21
With respect to training, from the age of 3 years, all children were provided structured training. 16 At that age, most children are quickly aware of how to operate the grip, can perform bimanual activities and are ready to play and cooperate with others.11,16,23 The effect of structured training was indirectly shown by the small difference in prosthetic skill between the groups at the age of 6 years. Altogether, structured training and support for the child and parents to establish wearing habits and prosthetic skill may have contributed to the relatively low rejection rate among the study group as a whole.
There are some study limitations. First, the number of cases was low. To compensate for the risk of low statistical power, the number of controls was tripled. Despite this approach, we were not able to confirm the differences between the groups statistically. Another procedural limitation was that the four occupational therapists performing the assessments were not blinded. Due to the study design, blinding the therapists was not feasible; the therapists knew based on the child’s age that the child was in the case group. In the same way, the parents of the children in the case group were selected based on their living area, and they were asked for and did make a decision to participate in the study, suggesting that they were highly motivated to support their child in doing well. This selection bias may have influenced the result. However, despite the therapists not being blinded and the parents’ high motivation, the results showed no differences in favour of the case group.
There are both positive and negative aspects to consider in regard to fitting MEP before the age of 2½ years. One positive aspect is that the child gets used to the MEP early and has access to a grip whenever a grip is needed once the prosthetic skill is developed. A negative aspect is the extra burden the early fitting puts on parents with a large number of visits to the health-care provider at a usually demanding time of life. Furthermore, much parental attention is given to the development of prosthetic skill instead of to the child; the influence of these aspects on the child’s future development was beyond the scope of this study but needs to be studied. Further research is also needed to investigate the potential benefits of early fitting and the usefulness of the MEP in daily life for young children at different ages. There is also a need to understand the significance of structured prosthetic training, which is why studies on this topic are highly recommended.
Conclusion
Considering a young child’s development of prosthetic skill and prosthetic use over time, this study shows no additional advantages for fitting an MEP very early. In conclusion, the recommended age for fitting MEP in children is from 2½ to 4 years of age with consideration of the individual patient’s psychosocial and motor development.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by Swedish Association of Occupational Therapists and Stiftelsen Promobilia.