
Abstract
Background:
The dysfunction of individuals with upper limb deficiencies affects their daily lives and social participation.
Objectives:
To clarify the adaptive behaviours and motor skills of children with upper limb deficiencies.
Study design:
Cross-sectional survey.
Methods:
The subjects were 10 children ranging from 1 to 6 years of age with unilateral upper limb deficiencies at the level distal to the elbow who were using only cosmetic or passive prostheses or none at all. To measure their adaptive behaviour and motor skills, the Vineland Adaptive Behavior Scales, Second Edition was used. They were evaluated on the domains of communication, daily living skills, socialization and motor skills. We also examined the relationship of the scores with age.
Results:
There were no statistically significant scores for domains or subdomains. The domain standard score of motor skills was significantly lower than the median scores of the domains and was negatively correlated with age.
Conclusion:
Children with upper limb deficiencies have individual weaknesses in motor skill behaviours, and these weaknesses increase with age. It may be helpful in considering approaches to rehabilitation and the prescription of prostheses to consider the characteristics and course of children’s motor skill behaviours.
Clinical relevance
Even if children with unilateral upper limb deficiencies seem to compensate well for their affected limb function, they have or will experience individual weaknesses in motor skills. We should take this into consideration to develop better strategies for rehabilitation and prostheses prescriptions.
Keywords
Background
Limb deficiencies in children are mainly congenital, with congenital upper limb deficiencies occurring at a prevalence of 4.1–5.0/10,000 total births.1,2 In Japan, the prevalence is unknown, and prostheses for children with congenital upper limb deficiencies have not been sufficiently prescribed especially when the deficiencies are unilateral. Even when they have prostheses, many are just cosmetic and not sufficiently functional. In Japan, almost all prostheses are created using the public health system or the social welfare system.
We think there are two reasons for few prescriptions of upper limb prostheses in Japan. When the deficiency is unilateral and distal, it is thought that the child has some functional impairment but the impairment has little influence on activity limitations or participation restrictions. When the deficiency is proximal, technological difficulty and costly prosthetics become problematic.
In children with congenital upper limb deficiencies, the advantages of prostheses in daily living are controversial. For example, for unilateral congenital below-the-elbow deficiencies, while James et al. 3 reported that prostheses do not improve function or quality of life, Crandall and Tomhave 4 reported that offering a variety of prosthetic options can often improve the children’s functional lifestyle.
In order to determine the effectiveness and adaptability of a child’s prosthesis, it is important to evaluate aspects such as performing activities of daily living and overall physical function, including upper limb function. There are evaluation methods which use outcome measures, such as prosthetic management and use, the degree of satisfaction with the prosthesis, stump pain, and prosthesis training effectiveness. 5 Evaluation methods for children who have upper limb deficiencies or who use prostheses include the Assessment of Capacity for Myoelectric Control,6,7 the Child Amputee Prosthetics Project–Functional Status Inventory,8–10 the Child Amputee Prosthetics Project–Prosthesis Satisfactory Inventory, 11 the Prosthetic Upper Extremity Functional Index,12,13 the Unilateral Below-the-Elbow Test 14 and the University of New Brunswick Test of Prosthetic Function; 15 however, these assessment methods are disease specific and limited to characteristics of upper limbs. Indeed, the characteristics of affected children according to general, standardized evaluation methods are unknown.
To obtain consent to supply sufficient the upper limb prostheses using the system of public health benefits, the prostheses need to result in improvements not only in specific movements or actions but also in universal capacity and daily living. Prior to achieving this, it is necessary to elucidate whether children with upper limb deficiencies show disadvantages on general standardized evaluation methods. The Functional Independence Measure for children16,17 is a widely used instrument that measures independence in activities of self-care, sphincter control, transfers, locomotion, communication and social cognition. However, because the score is rated regardless of age, it is difficult to describe the characteristics of a group comprising children of different ages. The Pediatric Evaluation of Disability Inventory (PEDI) 18 is a norm-referenced assessment to examine functional skills and caregiver assistance in three domains: mobility, self-care and social functioning. Although the PEDI was translated into Japanese, unfortunately it had been not standardized in Japan.
In this study, we interviewed the guardians about their children’s behaviour using the Vineland-II survey interview form. The Vineland Adaptive Behavior Scales, Second Edition (Vineland-II)19,20 is an adaptive behaviour scale composed of the domains of communication, daily living skills, socialization, motor skills and the optional domain of maladaptive behaviour. The Vineland-II uses standard scores to describe an individual’s overall functioning, as well as his or her level of functioning in each of the adaptive behaviour domains. Domains and adaptive behaviour composite standard scores have means of 100 and standard deviations of 15. The v-scale scores, which describe individual’s relative levels of functioning compared with others of the same age on the subdomains, have means of 15 and standard deviations of 3. Its applicable age range is from 0 to 90 years (the Japanese version is from 0 to 92), and while it is employed mainly for children with intellectual and developmental disabilities, autism spectrum disorders (ASD), and attention-deficit hyperactivity disorders (ADHD), it has been also used in cases of post cardiac arrest, 21 deafness 22 and congenital diaphragmatic hernia. 23 The purpose of this study was to elucidate the characteristics of children with upper limb deficiencies from the perspective of their adaptive behaviours especially motor skills.
Methods
Subjects
The subjects were recruited from outpatients of the Department of Rehabilitation Medicine of our university hospital between January 2015 and November 2016. A total of 10 children ranging from 1 to 6 years of age with unilateral congenital upper limb deficiencies at the level distal to the elbow who were using only cosmetic or passive prostheses or none at all and had no coexisting disease affecting adaptive behaviour (i.e. ASD or ADHD) were included. There were seven boys and three girls. All had transverse deficiencies; forearm in three, complete carpal in one, partial carpal in five and monodactyly in one. Three children had used cosmetic or passive prostheses in the past 3–4 months, while the rest had never used any prostheses.
Procedure
This study was approved by the Ethics Committee of the Faculty of Medicine of the University of Tokyo (ethical approval number: 2372-[2]). The results of the children’s deficiency level, complicating disorders and Vineland-II interview were retrospectively examined via their medical charts. At the University of Tokyo Hospital, all patients are given an explanation about personal information protection, including the use of clinical data for research. In this study, there were no subjects who refused the provisions for use of clinical data.
We implemented the Japanese version of the Vineland-II interview form as a part of outpatient examination and treatment. An explanation was given to the guardians of all of the children regarding the performance of Vineland-II as part of their evaluation, to which they provided oral consent. The interviewees were the children’s guardians. We conducted semistructured interviews. This study did not examine the optional maladaptive behaviour domain.
Statistical analysis
We analysed each standard score and, from these, examined the children’s adaptive behaviour characteristics. We also analysed individual strengths and weaknesses on domains. The Wilcoxon signed-rank test was used. We also analysed individual strengths and weaknesses on domains. Additionally, the correlations between age and individual strengths and weaknesses on domains and motor skills were analysed using the Spearman rank method. Statistical analyses were performed using JMP® Pro 11.0.0 (SAS Institute Japan). p < 0.05 was considered significant.
Results
Adaptive behaviour composite score, domain standard scores and subdomain v-scale scores are shown in Table 1. The adaptive behaviour composite score was 104.0, while the domain standard scores for communication, daily living skills, socialization and motor skills were 106.0, 99.7, 103.0 and 97.5, respectively. There were no statistically significant scores of either domains or subdomains.
Adaptive behaviour composite score, domain standard scores and subdomain v-scale scores of Vineland-II. a
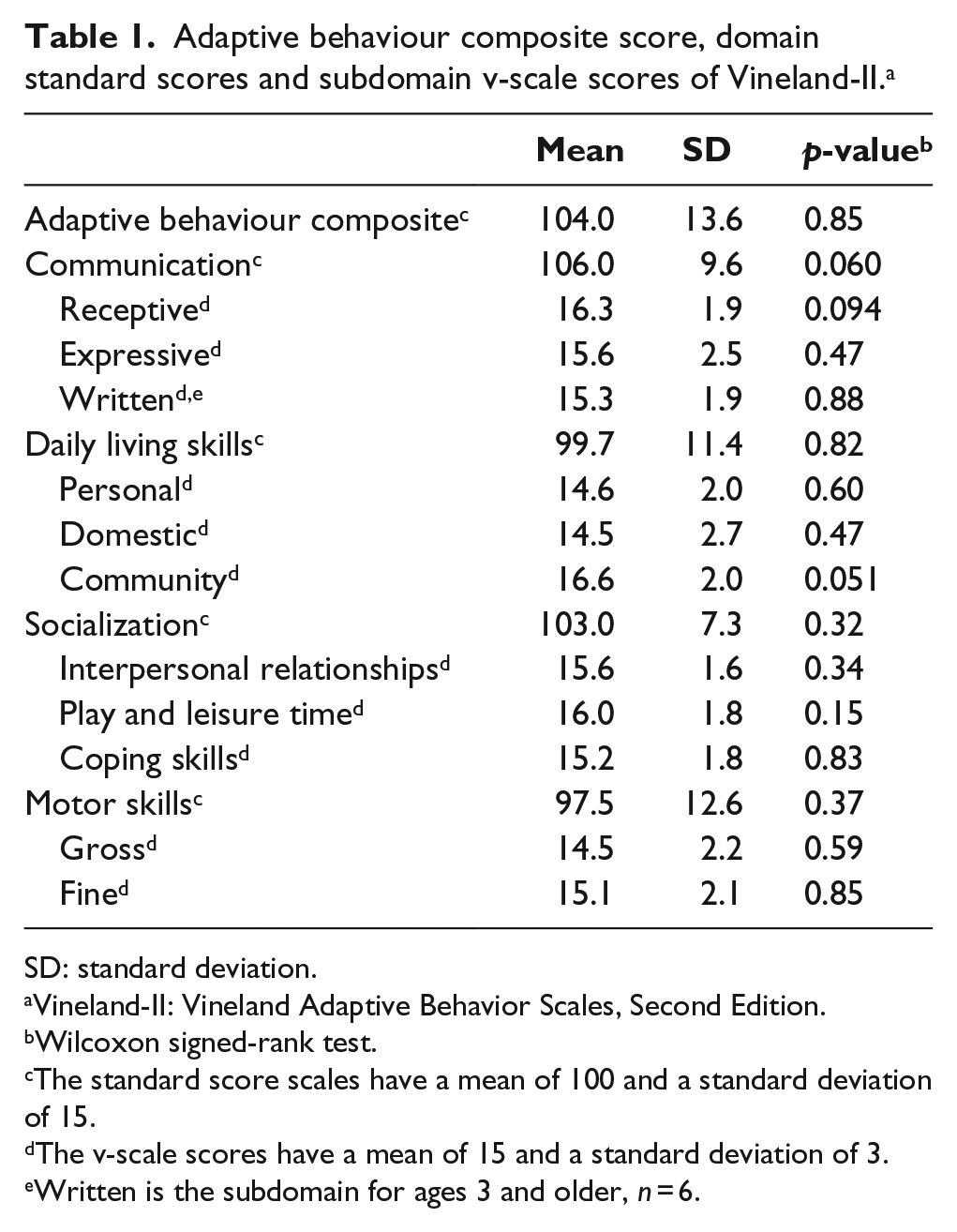
SD: standard deviation.
Vineland-II: Vineland Adaptive Behavior Scales, Second Edition.
Wilcoxon signed-rank test.
The standard score scales have a mean of 100 and a standard deviation of 15.
The v-scale scores have a mean of 15 and a standard deviation of 3.
Written is the subdomain for ages 3 and older, n = 6.
Individual strengths and weaknesses on domains are shown in Table 2. Communication was significantly higher, and motor skills was significantly lower than the median scores of the domains.
Individual strengths and weaknesses on domains of Vineland-II. a
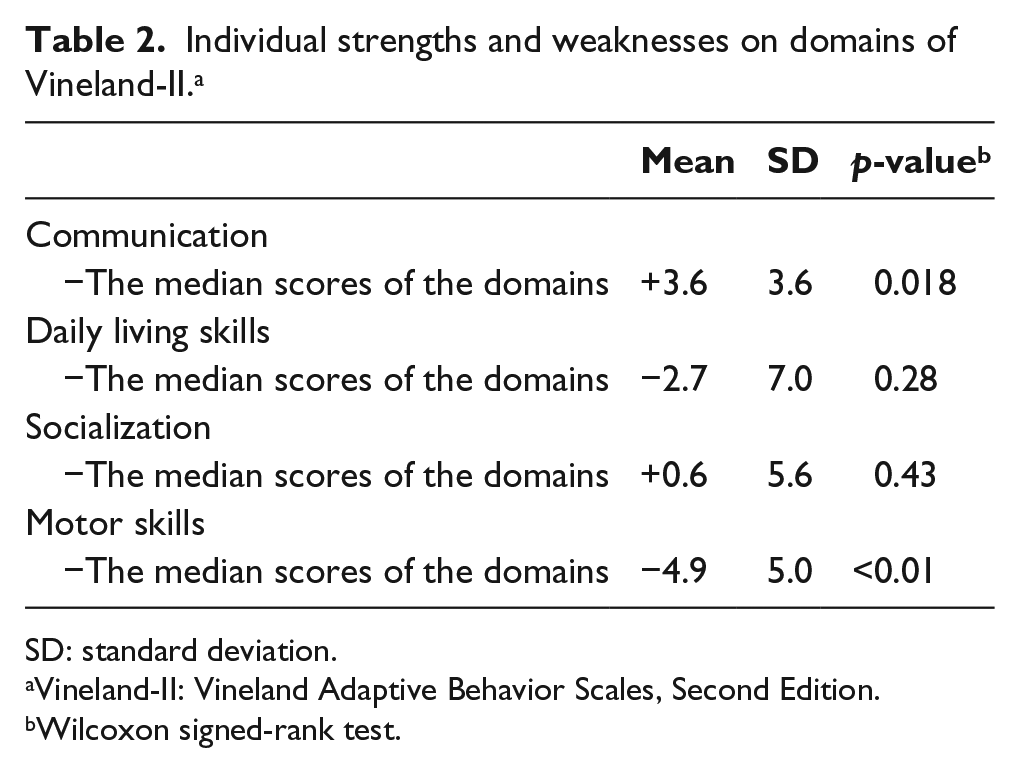
SD: standard deviation.
Vineland-II: Vineland Adaptive Behavior Scales, Second Edition.
Wilcoxon signed-rank test.
Correlations of individual strengths and weaknesses on domains and motor skills scores with age are shown in Table 3. Significant negative correlations were found between age and the difference of motor skills scores from the median scores of the domains, motor skills scores and gross motor skills scores. Figure 1 shows the relationship between age and the difference of motor skills scores from the median scores of the domains. There was no clear relationship between age and fine motor skills.
Correlations of the scores of Vineland-II a with age.
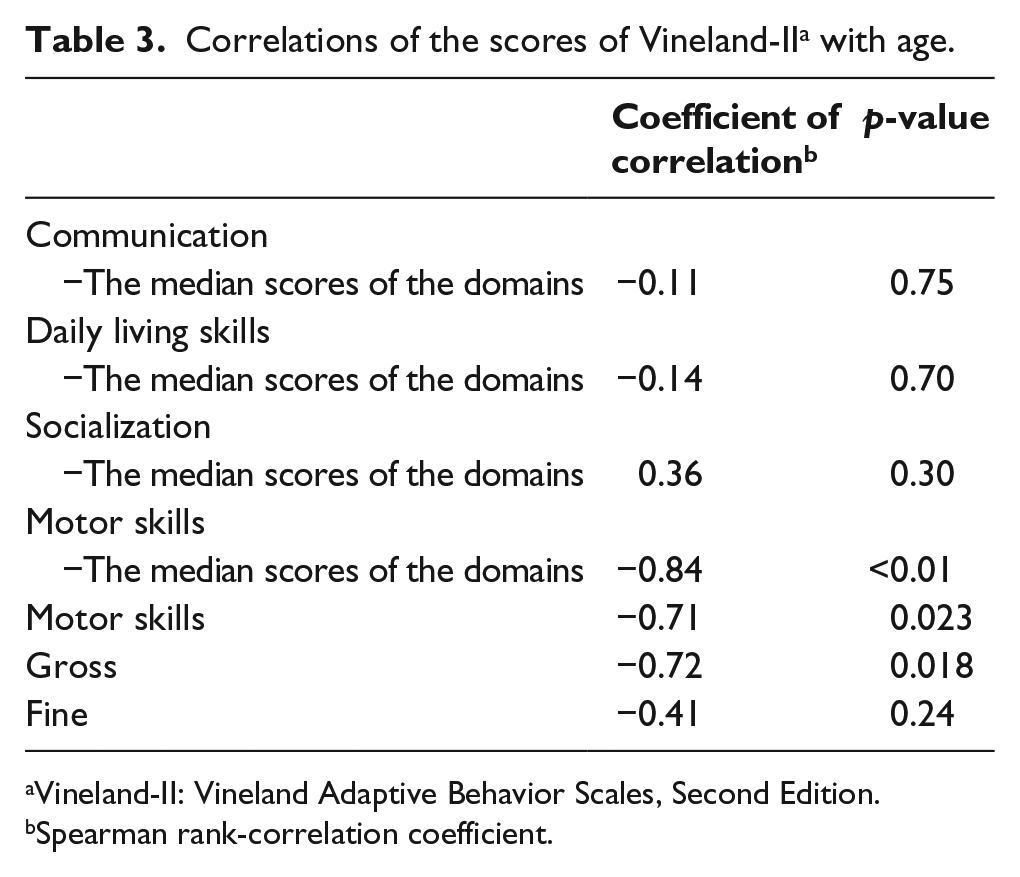
Vineland-II: Vineland Adaptive Behavior Scales, Second Edition.
Spearman rank-correlation coefficient.
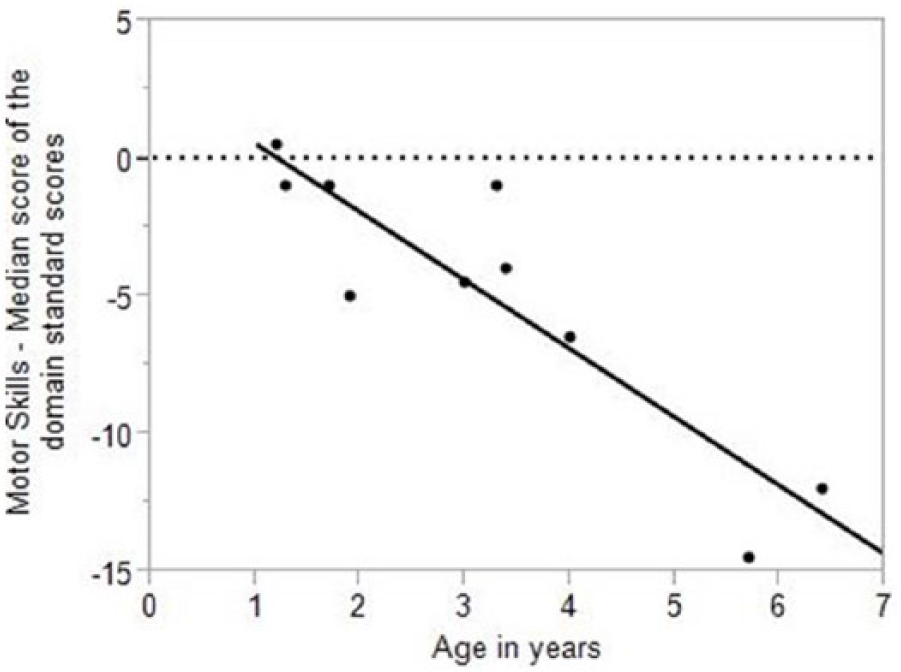
A significant negative correlation was found between age and relative motor skills in children with unilateral upper limb deficiencies at the level distal to the elbow.
Discussion
There have been no prior studies on the adaptive behaviours of people with upper limb deficiencies, the characteristics of which we have elucidated in children using the Vineland-II interview form in this study. While their adaptive behaviours were generally average, their individual weakness in motor skills was revealed. On the other hand, they had individual strength in communication. Although all domains contain items requiring upper limb function, communication, which includes waving good-bye, pointing and gestures in the expressive subdomain and writing skills in the written subdomain, is less influenced by unilateral upper limb dysfunction than the daily living and socialization. We think this is a reasonable characterization of children with upper limb deficiencies.
The relationship between age and individual weakness in motor skills suggests that there is a delay in motor development that emerges after infancy. The delay is related to gross rather than fine motor skills. In this study, there is a tendency for the items in the gross subdomain such as catching a ball or riding a tricycle or a bicycle to be difficult to achieve. We think that if the residual limb can fill the role of non-dominant hand function, fine movements, which included the use of tools that required upper limb function such as scissors, despite taking time to learn, were acquired when prompted as necessary. Otherwise, catching a ball and riding a bicycle require more equal roles of both upper limbs. Although it is not impossible to ride a bicycle with one hand, it seems much more difficult to ride a bicycle with one hand from the first than after acquiring with two hands.
To achieve bimanual actions, we think there are needs to implement activity-appropriate prostheses and making appropriate adjustments on the side for utilizing tools. In the first year of life, children with unilateral upper limb deficiencies at the level distal to the elbow have no demand for complex movements, and their level of motor skills are comparable to the level of the overall adaptive behaviour. Nevertheless, it is thought to be good for children to start wearing a prosthesis under 2 years of age so that they will accept them without objection.24–26 Even though prostheses are not essential when children are under 1 year of age and they can compensate for their motor function via their residual limbs, prosthesis introduction is necessary considering the children’s eventual decline in relative motor skills and future utilization of body-powered or electric prostheses.
Limitations
The sample size of 10 children in this study is small and this might have influenced our results. Thus, further research needs to be conducted that examines a larger sample size. Additionally, the Vineland-II used in this study scores each interview item as merely done or not done, while things such as time taken or difficulty are not considered. Thus, even if a child from this study is said to be doing each interview item, it does not always mean that they are doing so easily. For example, even in patients who somehow use their lower limbs to perform a movement that would normally be done with upper limbs, it would merely be scored as done. During the calculation of subdomain raw scores, a basal is established when the individual performs all the activities described in four consecutive items and a ceiling is established when the individual never engages in the activities of four consecutive items. When computing subdomain raw scores, all items below the basal item are assumed to have a perfect score. Given these facts, the motor skills of older children risk the possibility of being overrated. These points need to be kept in mind when interpreting the present results.
The children with upper limb deficiencies who participated in this study were not using prostheses with voluntary hands (i.e. body-powered or electric prostheses), and therefore, the motor function and adaptive behaviours of those who do is unclear. An examination of the characteristics of children who are using functional prostheses or studies evaluating the effectiveness of prosthesis introduction or rehabilitation on motor function and adaptive behaviours are topics for further study.
Conclusion
The aforementioned limitations notwithstanding, we elucidated the characteristics of children with upper limb deficiencies from the perspective of their adaptive behaviours. They have individual weaknesses in motor skill behaviours, and the weakness increases with age. We think it is helpful in considering the appropriate approach to rehabilitation and the prescription of prostheses to consider the characteristics and course of children’s motor skill behaviours.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.