
Abstract
This review presents an analytical and comparative survey of upper limb prosthesis acceptance and abandonment as documented over the past 25 years, detailing areas of consumer dissatisfaction and ongoing technological advancements. English-language articles were identified in a search of Ovid, PubMed, and ISI Web of Science (1980 until February 2006) for key words upper limb and prosthesis. Articles focused on upper limb prostheses and addressing: (i) Factors associated with abandonment; (ii) Rejection rates; (iii) Functional analyses and patterns of wear; and (iv) Consumer satisfaction, were extracted with the exclusion of those detailing tools for outcome measurement, case studies, and medical procedures. Approximately 200 articles were included in the review process with 40 providing rates of prosthesis rejection. Quantitative measures of population characteristics, study methodology, and prostheses in use were extracted from each article. Mean rejection rates of 45% and 35% were observed in the literature for body-powered and electric prostheses respectively in pediatric populations. Significantly lower rates of rejection for both body-powered (26%) and electric (23%) devices were observed in adult populations while the average incidence of non-wear was similar for pediatric (16%) and adult (20%) populations. Documented rates of rejection exhibit a wide range of variance, possibly due to the heterogeneous samples involved and methodological differences between studies. Future research should comprise of controlled, multifactor studies adopting standardized outcome measures in order to promote comprehensive understanding of the factors affecting prosthesis use and abandonment. An enhanced understanding of these factors is needed to optimize prescription practices, guide design efforts, and satiate demand for evidence-based measures of intervention.
Introduction
The design of any successful product hinges upon an interactive and ongoing partnership between the designer and the end user. This is especially true in the realm of prosthetics where the product is an intimate extension of the body and as such, must adhere to a high standard of quality while balancing the many, and often conflicting, design requirements of the user. More and more, consumers are unwilling to make the traditional trade-off between form and function and are demanding both in their product selections. The market for upper limb prostheses is no exception, resulting in an extensive list of design criteria in the areas of function, durability, appearance, comfort and usability. Perhaps the greatest pitfall awaiting engineers and clinicians involved in the development of prostheses is an eagerness to tackle the looming design challenges with a battalion of technology before the needs and desires of the end user are clearly defined and translated into specific engineering requirements. Current prosthetic options range in both functionality and cosmesis to address a variety of user needs and lifestyles. The extent to which they have succeeded in this purpose has been the subject of many clinical and consumer studies. Nevertheless, general trends and inferences regarding prosthesis usage and acceptance have remained particularly elusive, a probable consequence of the heterogeneous population base and methodological differences that restrict comparisons between studies. The purpose of this paper is to provide a critical review of prosthesis use and abandonment as documented in the last 25 years, and to provide guidelines and directions for future research. This review is relevant to physicians, prosthetists, occupational therapists, and allied health professionals involved in clinical activities such as prescription, fitting, and training with prosthetic devices, as well as those embarking on research and development activities in the area of upper limb prosthetics.
Method
Literature search
The relevant literature was collected via a search of Ovid (MEDLINE, CINAHL, EBM Reviews, EMBASE, and Ovid Healthstar), ISI Web of Science, and PubMed using the following Keywords: upper limb and prosthesis or prostheses. The search was limited to English communications dating onwards of 1980. The literature search returned 1435 references, distributed in a number of areas as depicted in Figure 1.
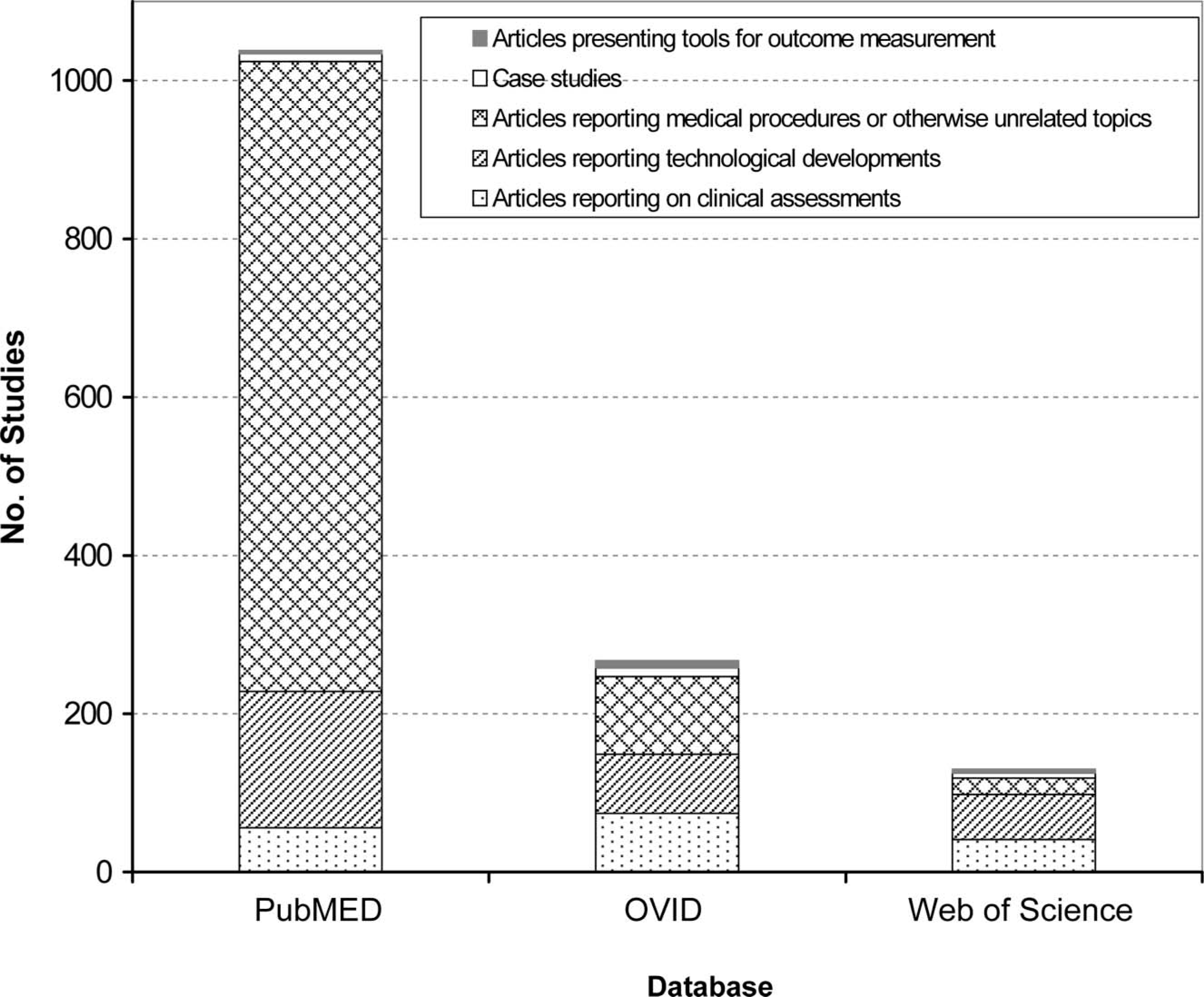
Results of literature search and distribution of studies by topic.
Selection criteria
Articles reporting on (i) tools for outcome measurement, (ii) specific case studies, and (iii) medical subject matter (i.e., surgical procedures, descriptions of medical conditions and treatments) were excluded from this study. From the remaining articles, those focused on: (1) Rejection rates for myoelectric, body-powered or passive prostheses; (2) Functional analysis and patterns of wear associated with prosthesis use; (3) Consumer satisfaction with prosthetic options; or (4) Technological advancements and experimental devices, were extracted.
Data synthesis
Approximately 200 articles were included in the review process once overlap between databases was removed. References cited in these studies were also examined. A collection of 40 articles documenting rejection rates for various prostheses was identified. These studies were reviewed in terms of patient selection and study design, and form the basis for quantitative comparisons in the following discussion. Quantitative measures describing the sample population (e.g., age, level of amputation), the study methodology (e.g., date, follow-up period), and the prostheses of study (e.g., rejection rates, time worn), were extracted for comparative purposes. The following taxonomy was developed to distinguish between the different methodological approaches applied in each study in order to frame the context, (i.e., the availability of prostheses and uniformity of experimental conditions), in which the results were collected:
Exclusive (E): Subjects are uniformly provided with a single type of prosthesis. Access to alternate prostheses and prosthetic history may or may not be detailed. Non-exclusive studies, where participants had access to a variety of devices, were subdivided as follows: Uncontrolled (U): Subjects use a variety of different prostheses, but are not uniformly provided with any one device. Some subjects have access to more than one type of prosthesis, while others use a single device. Details regarding availability, usage history, and external factors (e.g., maintenance costs, training, etc.) that may affect rejection or acceptance rates are generally not detailed extensively. Controlled (C): Subjects are uniformly (or approximately so) provided with multiple prostheses to use and select from according to their preference. Studies of this genre that compare aspects of the different prostheses provided, specifically rates of rejection, are further classified as controlled comparatives (CC).
The above taxonomy will be used to characterize each study and its reported results, as well as to present observations on the typical methods used in this field of study.
Results
The following will review the literature associated with the primary prosthetic options, namely passive (usually cosmetic) and active prostheses (body-powered systems or externally powered electric/myoelectric systems). Topics of interest include rates of rejection and consumer satisfaction, along with patterns of wear and use. The tables to follow specify documented prosthesis rejection rates for each of the prosthetic options, along with relevant characteristics of the sample populations and the methodological design (i.e. duration of follow-up, the number of rehabilitation centres involved, and response rates).
Passive prostheses
Although less often the subject of quantitative study than active prostheses, the few studies that have focused on passive prostheses have attributed these devices not only with cosmetic, but significant functional value (van Lunteren et al. 1983; Fraser 1998; Pillet and Didierjean-Pillet 2001). Passive prostheses are affiliated with widely variable rejection rates with reports ranging from 6% (Kejlaa 1993) to 100% (van Lunteren et al. 1983) as evident in Table I.
Documented rejection rates of passive prostheses
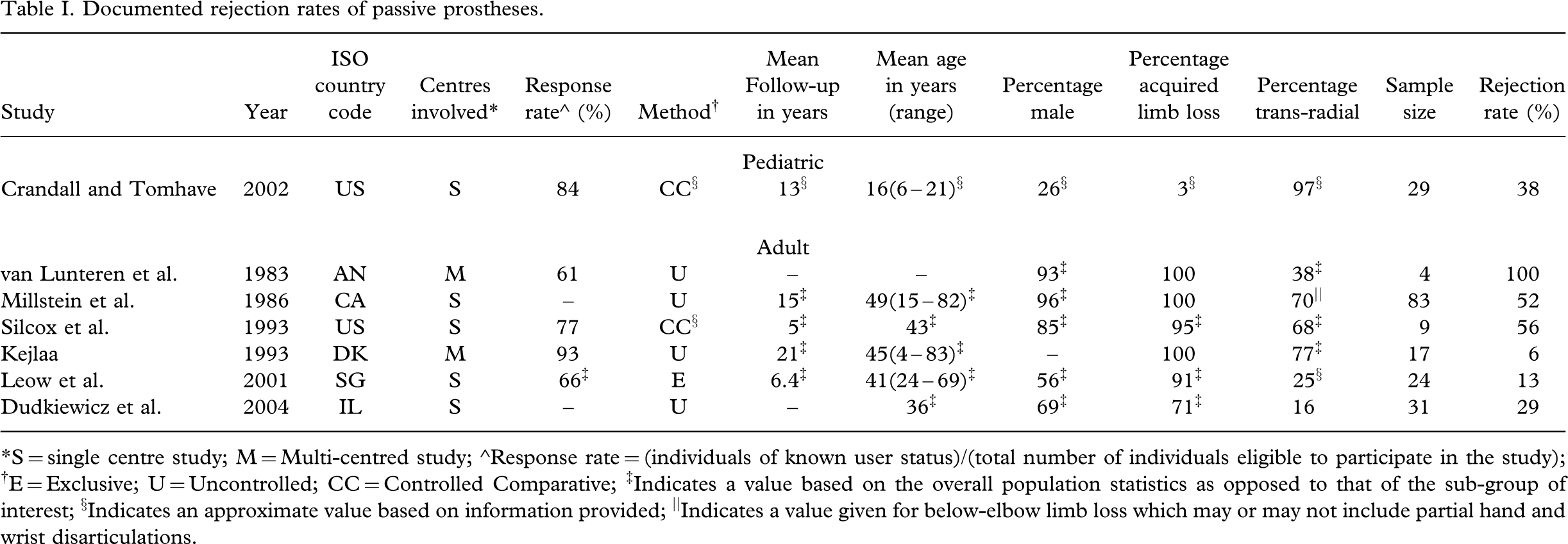
∗S = single centre study; M = Multi-centred study; ∘Response rate = (individuals of known user status)/(total number of individuals eligible to participate in the study); †E = Exclusive; U = Uncontrolled; CC = Controlled Comparative; ‡Indicates a value based on the overall population statistics as opposed to that of the sub-group of interest; §Indicates an approximate value based on information provided; ||Indicates a value given for below-elbow limb loss which may or may not include partial hand and wrist disarticulations.
From the seven studies reporting rejection rates over a period from 1983 – 2004, no indication was apparent that the acceptability of passive prostheses has declined in recent years despite the advent of myoelectric devices with functional as well as cosmetic appeal. Recent evidence suggests that cosmetic prostheses tend to have a higher rate of permanent use both in adult and pediatric populations (Dudkiewicz et al. 2004; Crandall and Tomhave 2002), with less temporary disuse stemming from decreased discomfort and maintenance requirements (Dudkiewicz et al. 2004). Developments in life-like silicone gloving with increased cosmesis (Huang et al. 2001) may also have enhanced consumer satisfaction with passive prostheses. Recent data pertaining to the widespread use of passive prostheses are not available in the literature, with the last international recount documenting a higher prevalence of passive devices in European countries such as the UK and Sweden, while myoelectric and body-powered prostheses were more common in West Germany and the United States, respectively (LeBlanc 1988). Despite the lack of active grasping function, passive prostheses tend to elicit the fewest user concerns, the most significant being wear temperature followed by glove problems, excessive weight, wear on clothes, and strap irritation (Kejlaa 1993).
Literature detailing use and satisfaction with passive devices, especially in pediatric sectors, is limited. In particular, a lack of controlled methodologies has been applied to their evaluation. Further study should be conducted to determine the extent to which quality of life is affected by lack of functional prosthetic manipulation and whether this is indeed offset by increased comfort and reduced maintenance. Additionally, the implications of passive versus active prosthesis use or non-use should be explored with respect to the health of the contralateral limb. A spectrum of passive prostheses exists ranging from stationary devices, to those that can be moved and locked in different positions by the opposite hand (Fairley 2005), to those that are spring-loaded to respond to the presence of an object at the fingertip (Sol 1999a). The value of these different devices should be investigated further, as it is likely that their acceptability and functionality is not one and the same. Exploration of techniques such as osseointegration may in the future alleviate many areas of user dissatisfaction related to discomfort with sockets and sleeves, as well as provide a greater measure of sensory feedback (Hagberg et al. 2005; Branemark et al. 2001). Progress in the latter could potentially benefit all varieties of prostheses.
Body-powered prostheses
Despite the technological appeal of electric devices, body-powered prostheses have remained a popular choice in upper limb prosthetics, particularly in the US where, as of 2003, they remained the preferred option for initial active fitting in the majority of pediatric clinics (Shaperman et al. 2003). Overall rejection rates of body-driven prostheses ranged from 16% (Bhaskaranand et al. 2003) to 66% (Kruger and Fishman 1993) as evident in Table II. Rejection in the adult population was generally lower than that of the pediatric sector. No clear trends in rejection rates were manifested in the studies analysed in terms of year, type of study, or follow-up period.
Documented rejection rates of body-powered prostheses
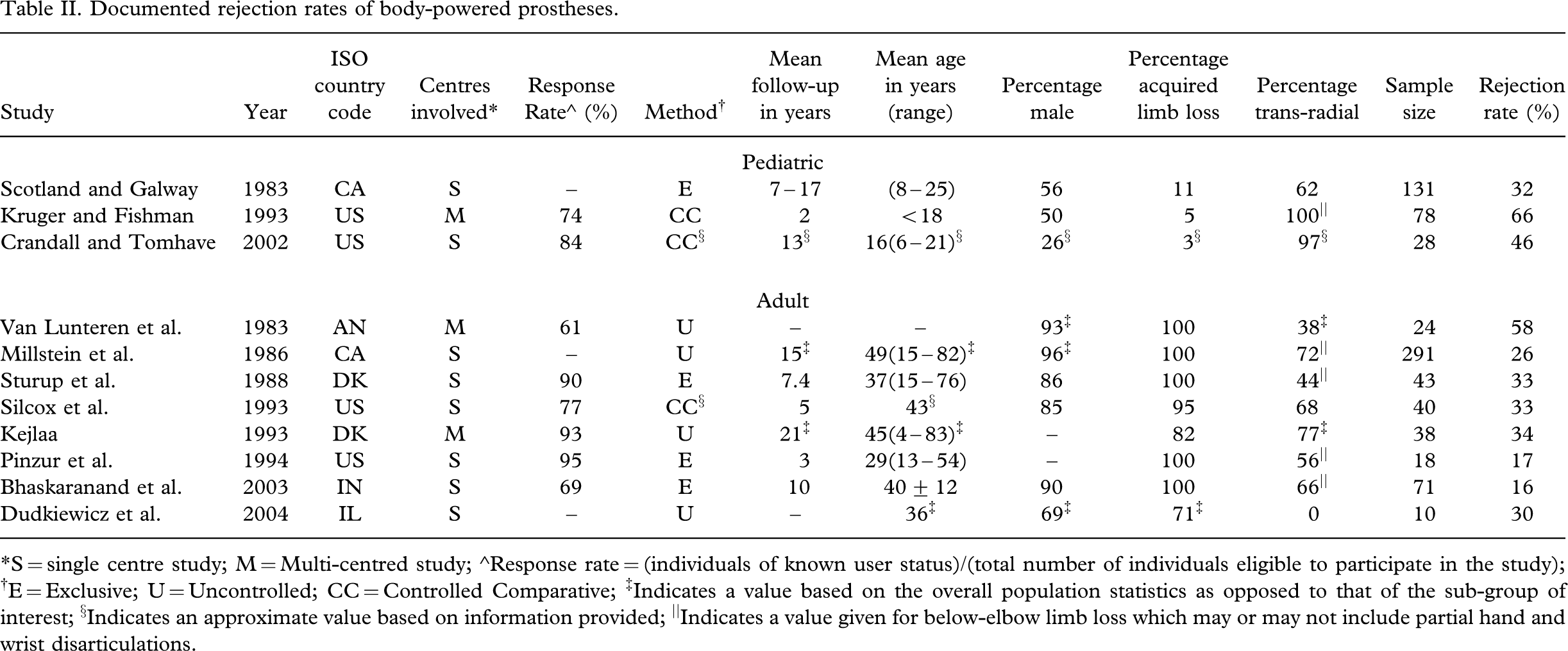
∗S = single centre study; M = Multi-centred study; ∘Response rate = (individuals of known user status)/(total number of individuals eligible to participate in the study); †E = Exclusive; U = Uncontrolled; CC = Controlled Comparative; ‡Indicates a value based on the overall population statistics as opposed to that of the sub-group of interest; §Indicates an approximate value based on information provided; ||Indicates a value given for below-elbow limb loss which may or may not include partial hand and wrist disarticulations.
Evidence indicates that acceptance of body-powered prostheses depends largely on the type of terminal device, be it hand or hook. Body-powered hands are typically associated with rejection rates as high as 80% (Millstein et al. 1986) and 87% (Kejlaa 1993), with common complaints targeting slowness in movement, awkward use, difficulty in cleaning and maintenance, excessive weight, insufficient grip strength and high-energy expenditure needed to operate (Millstein et al. 1986; Kejlaa 1993). Body-powered hooks on the other hand are generally selected for functional value, durability, lower weight and good visibility of objects being handled and, overall, are more acceptable to users (Millstein et al. 1986). Owing to the modularity of body-powered devices, individuals can often be fitted with both a hand and a variety of hooks. It should be noted that several of the studies listed in Table II did not distinguish rejection rates of body-powered prostheses in terms of terminal device (van Lunteren et al. 1983; Silcox et al. 1993; Scotland and Galway 1983; Sturup et al. 1988; Bhaskaranand et al. 2003).
Reported consumer complaints with respect to body-driven prostheses generally include excessive wear temperatures, abrasion of clothes, wire failure, unattractive appearance, with the most commonly recounted hindrance being harness discomfort and/or breakage (van Lunteren et al. 1983; Kejlaa 1993; Bhaskaranand et al. 2003; Dudkiewicz et al. 2004). Short-term goals for future development of body-powered prostheses were identified by Atkins et al. in 1996 and included provision of more durable cables, more comfortable harnesses, and improved gloving material, while long-term objectives were aimed at increased wrist movement, and improved control mechanisms requiring less visual attention and enabling coordination of multiple joints.
Recent advancements in line with these goals have included the development of more colourful and aesthetically pleasing hooks for children (Plettenberg 2005), a harness-free, elbow controlled body-powered prosthesis (Sol 1999b), developments in silicone gloving, and systems for humeral rotation (Ivko 1999). The AdVAntage Arm is an example of one system developed in response to typical user concerns, boasting lighter weight, independent control of the elbow and terminal device, cable recovery for effective use at any elbow position, internal routing of polymer cables, adjustable forearm length and lift assist (Cupo and Sheredos 1998). Despite initially positive reviews, the AdVAntage Arm did not enter the commercial market. The extent to which initiatives such as these have addressed the goals as identified by Atkins et al. (1996), and recent consumer opinion with regards to the design of body-powered devices, is not available in the literature surveyed.
Electric prostheses
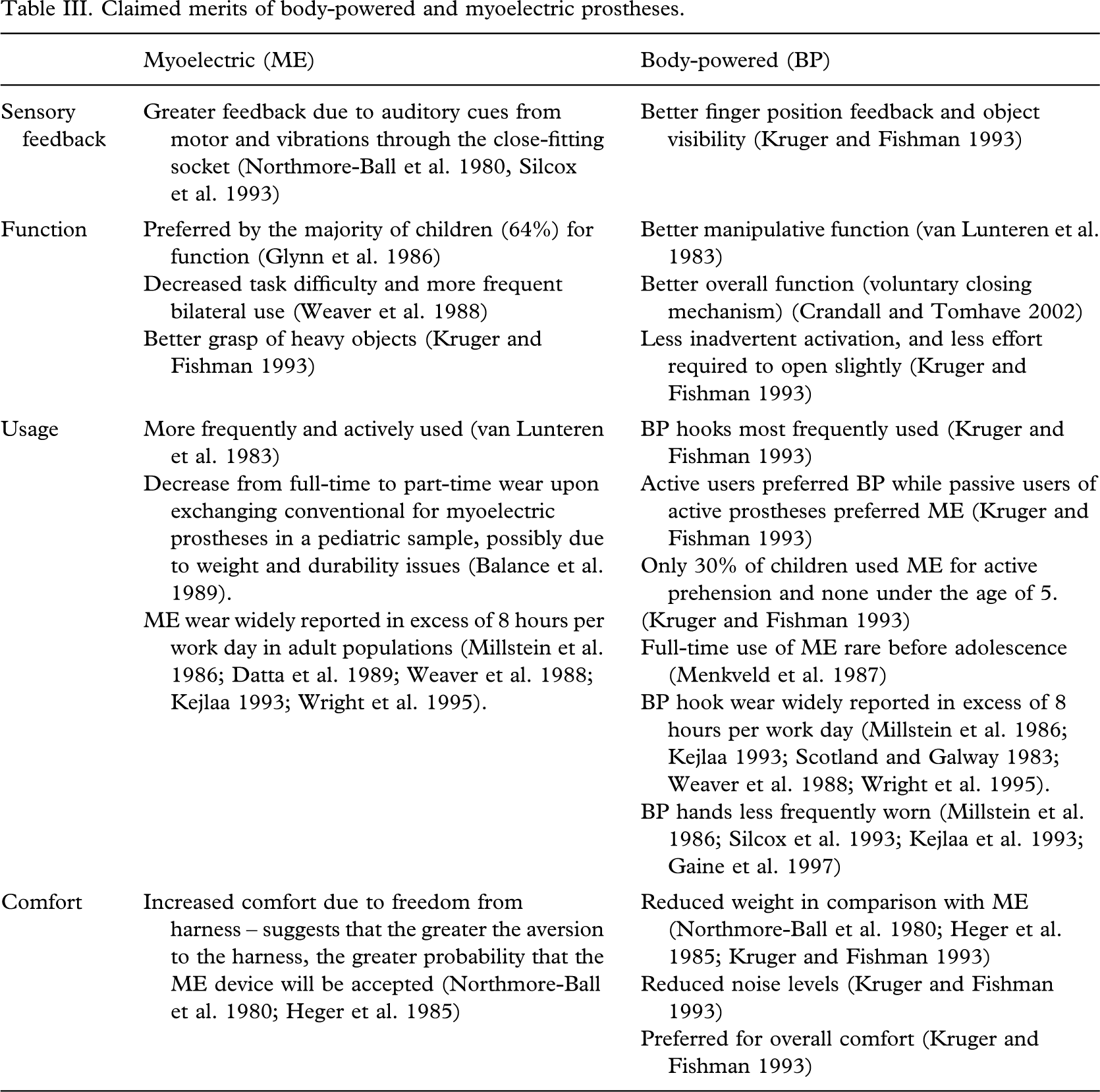
With the lure of bionic sophistication, electric prostheses are indeed an enticing substitute for body-powered devices. Electric prostheses are generally accepted to offer advantages in appearance, increased pinch strength, ease of operation, and lack of harness (Scotland and Galway 1983; Trost 1983; Datta et al. 1989; Ballance et al. 1989; Glynn et al. 1986; Weaver et al. 1988). In contrast, users can typically expect increased maintenance such as glove and battery replacement, in addition to higher cost and weight (Scotland and Galway 1983; Datta et al. 1989; Ballance et al. 1989). More disputed are features such as sensory feedback, overall function, and comfort, of which the merits of electric over body-powered prostheses are more indeterminate as presented in Table III. These areas of controversy are presented only to suggest areas where further exploration is warranted and to emphasize the extent of variance between studies conducted in this area, a likely derivative of the highly heterogeneous sample populations and experimental methodologies.
Claimed merits of body-powered and myoelectric prostheses
Of all prostheses, myoelectric devices have been the most extensively studied in terms of rejection rates, likely owing to the need to quantitatively justify their higher cost. Table IV summarizes reported rejection rates of 22 studies over the past quarter century with a highly variable range from 0% (Dalsey et al. 1989) to 75% (Crandall and Tomhave 2002) rejection. It was hypothesized that advances in engineering, social funding, prosthesis availability, training services and the burgeoning culture of technology, might be reflected by decreased myoelectric rejection rates with time. Interestingly, no trends suggesting a decrease in rejection rates in recent years were apparent in the data. This may however also be a function of population characteristics. The importance of documenting follow-up periods is emphasized, with several studies suggesting an increased rate of rejection of myoelectric prostheses with lengthened follow-up (Silcox et al. 1993; Kruger and Fishman 1993; Heger et al. 1985). Complete documentation of attributes related to the individual (i.e., level of limb loss, lifestyle etc.) and the prosthesis (i.e., control strategy, components, etc.) facilitates comparison between studies and is vitally important when dealing with the diversity of the upper limb deficient population.
Documented rejection rates of myoelectric prostheses
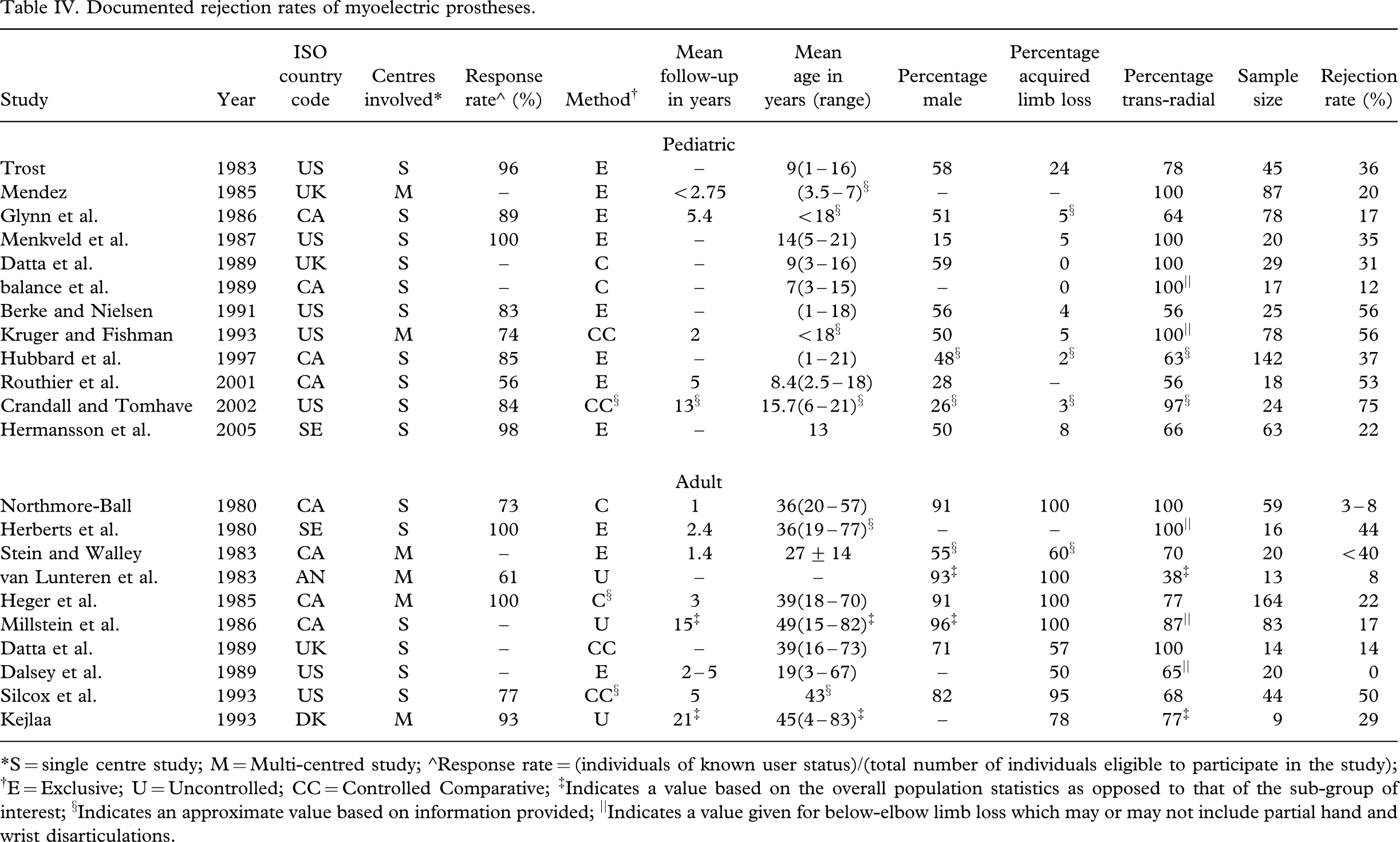
∗S = single centre study; M = Multi-centred study; ∘Response rate = (individuals of known user status)/(total number of individuals eligible to participate in the study); †E = Exclusive; U = Uncontrolled; CC = Controlled Comparative; ‡Indicates a value based on the overall population statistics as opposed to that of the sub-group of interest; §Indicates an approximate value based on information provided; ||Indicates a value given for below-elbow limb loss which may or may not include partial hand and wrist disarticulations.
Atkins et al. (1996) concluded that future development of myoelectric prostheses should aspire in the near term towards improved gloving material, batteries/charging units, reliability of the hand and electrodes, and towards the provision of greater finger movement, less visual attention, and greater wrist movement in the long term. Weight-related complaints, which range in prevalence with anywhere from 13% (Datta et al. 1989) to 81% (Hubbard et al. 1997) of pediatric populations indicating this to be a major issue in prosthesis rejection and disuse, should also be addressed, along with excessive wear temperature (Kejlaa 1993; Ballance et al. 1989; Routhier et al. 2001). Durability was also a significant concern with electric prostheses, especially for young children (Datta et al. 1989; Northmore-Ball et al. 1980; Heger et al. 1985; Herberts et al. 1980; Hubbard et al. 1997).
A large number of advancements are underway to address the variety of user concerns in areas of comfort, durability, function, control, and appearance with respect to myoelectric prostheses. Table V summarizes a few of these innovative endeavours, portraying the future visions for powered prostheses. Recent commercial advancements in lightweight lithium batteries (Williams 2005), life-like silicone gloving materials (Huang et al. 2001), prosthesis designs with increased speed and slip control (McGahey and Mandacina 2005), modular designs with increased finger articulation (Gow et al. 2001), programmable microprocessors and tools for optimizing control strategies (Lake and Miguelez 2003), together with techniques for fabricating and customizing silicone sockets (Ullendahl 2005; Herbert et al. 2005), are promising developments in need of quantitative clinical assessment. Initiatives to improve control strategies, (Chan and Englehart 2003; Nishikawa et al. 2000; Ajiboye and Weir 2005, Huang et al. 2005; Khadivi et al. 2005; Sibelius et al. 2005a, 2005b), to exploit mechanomyography as a means of circumventing problems of perspiration and electrode placement (Silva et al. 2005), to create multi-articulated mechanisms with adaptive grasp (Carrozza et al. 2004; Kyberd et al. 2001; Yang et al. 2004; Light et al. 2000; Dechev et al. 2001), and to endow prostheses with greater sensory feedback (Carpaneto et al. 2003; Cranny et al. 2005; Riso 1999; Zecca et al. 2004, Dhillon and Horch 2005), are avenues by which vast improvements are expected in the future. Additionally, ongoing exploration of novel materials and actuators such as shape memory alloys (De Laurentis and Mavroidis 2002; dos Santos et al. 2003), pneumatic actuators (Pylatiuk et al. 2005; Caldwell and Tsagarakis 2002), micromotors (Kyberd et al. 2001; Del Cura et al. 2003), ultrasonic motors (Pons et al. 2002) and electroactive polymers (Del Cura et al. 2003), along with implantable myoelectric sensors (Weir et al. 2005), reinnervation strategies for increased control sites and simultaneous coordination of joints (Kuiken et al. 2004), and osseointegration (Hagberg et al. 2005; Branemark et al. 2001), may pave the way for a new generation of more functional, comfortable, and aesthetically pleasing powered prostheses.
Ongoing research and development of myoelectric prostheses
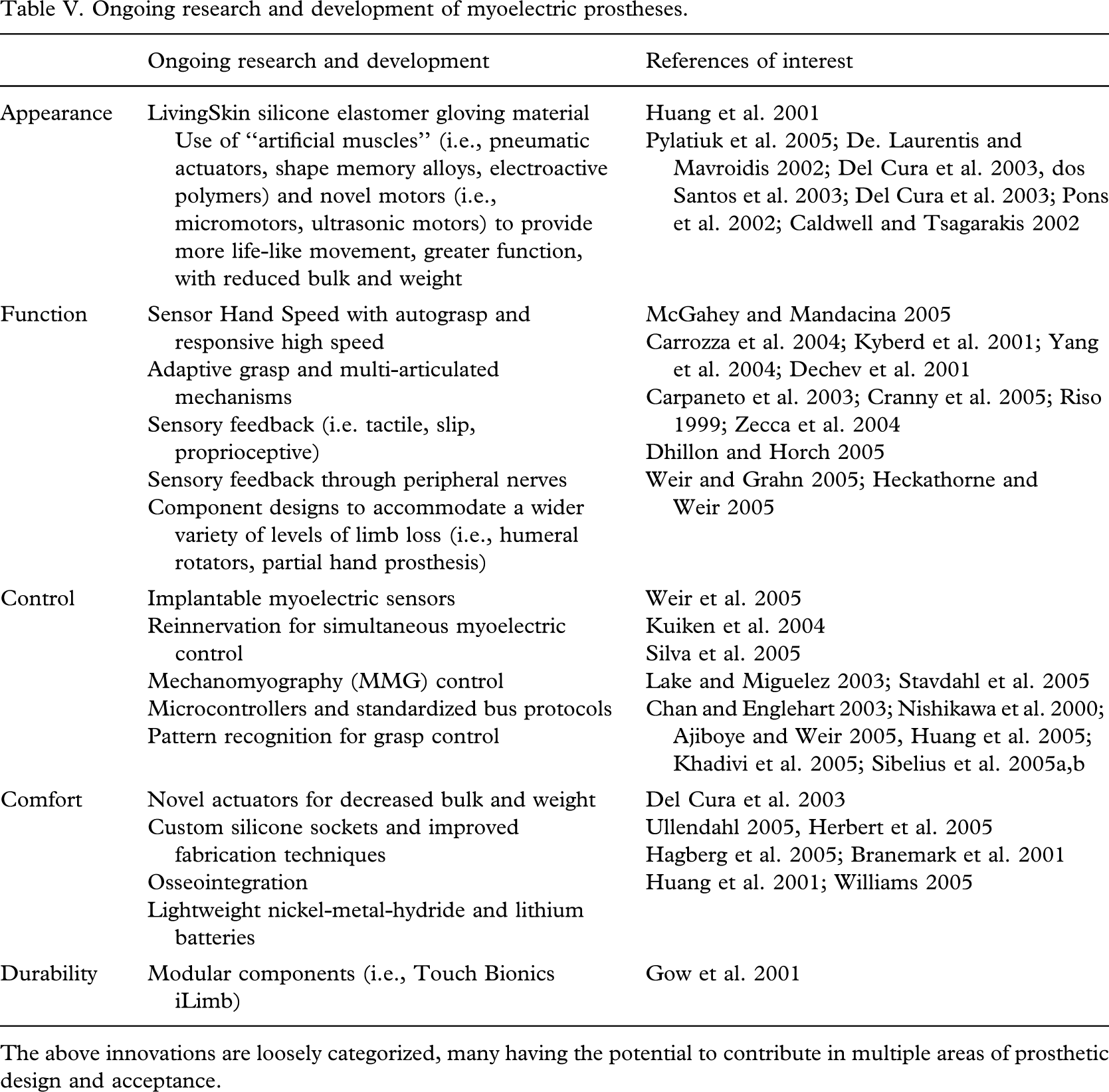
The above innovations are loosely categorized, many having the potential to contribute in multiple areas of prosthetic design and acceptance.
Prosthesis design: Overall impact on wear, use and abandonment
Patterns of wear
Interest in patterns of wear stems from the need for quantitative measures of prosthesis acceptance. Correlations between full time prosthesis wear and factors of interest such as spontaneous active use of the device (Ballance et al. 1989) and prosthesis satisfaction (Davidson 2002) have been made, justifying the collection of information to this point. Both body-powered prostheses and electric devices, if worn, tend to be well-used, often upwards of 8 h per workday, with extensive use for social activities and at work/school (Fraser 1998; Crandall and Tomhave 2002; Silcox et al. 1993; Fraser 1993; Northmore-Ball et al. 1980; Hubbard et al. 1997; Kyberd et al. 1998; Durance and O'Shea 1988; Pruitt et al. 1997, Millstein et al. 1986; Datta et al. 1989; Weaver et al. 1988; Kejlaa 1993; Wright et al. 1995; Scotland and Galway 1983). Prosthesis wear is typically reduced on weekends (Millstein et al. 1986; Hubbard et al. 1997; Routhier et al. 2001) and in the home (Silcox et al. 1993; Ballance et al. 1989; Hubbard et al. 1997; Pruitt et al. 1997). A few exceptions notwithstanding (Fraser 1998; Burger and Marincek 1994), passive and body-powered hands are generally the least consistently used and often primarily for social activities (Millstein et al. 1986; Silcox et al. 1993; Kejlaa 1993; Gaine et al. 1997). It is difficult however to make comparisons between the wear patterns of passive and active devices, as the latter is typically prescribed to established and consistent wearers (Hacking et al. 1997). In general, use of multiple prostheses is widely recommended (Crandall and Tomhave 2002; Leow et al. 2001; Trost 1983; Datta et al. 1989; Mendez 1985).
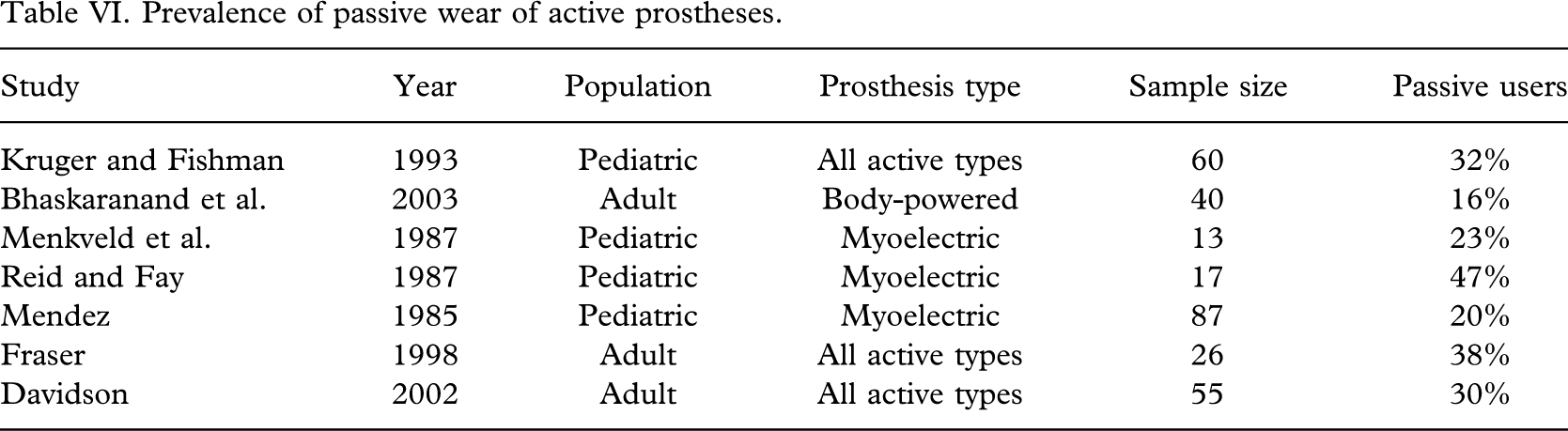
Nature of use
Prosthesis use is notoriously challenging for activities of daily living involving hygiene, eating, grooming and dressing (Kejlaa 1993; Weaver et al. 1988; Routhier et al. 2001; Thornby and Krebs 1992; Datta et al. 2004; Davidson, 2002) while the functional value of active mechanisms is often not exploited in social situations where the prosthesis may be used strictly as a cosmetic passive device (Northmore-Ball et al. 1980). This introduces another interesting sub-group: Passive wearers of body-powered or electric prostheses who do not use the active capabilities of their device. As extracted from the reviewed literature, the prevalence of this group is seen to range between 16% (Bhaskaranand et al. 2003) and 47% (Reid and Fay 1987) with a weighted average of 27% (Table VI).
Prevalence of passive wear of active prostheses
Overall rejection rates
Based on the available literature of the past 25 years, rejection of all prostheses and subsequent non-use appears was observed in approximately 1 of every 5 individuals with upper limb deficiency (Table VII). It is probable that this number may in fact be even higher as the majority of studies are conducted through rehabilitation centres that may not necessarily have access to non-wearers not using these services. Individuals with positive prosthetic experiences may also be more predisposed to participate in studies regarding their use (Fraser 1998; Fraser 1993; Kyberd et al. 1998; Melendez and Leblanc 1988).
Documented overall rejection rates of any prosthesis
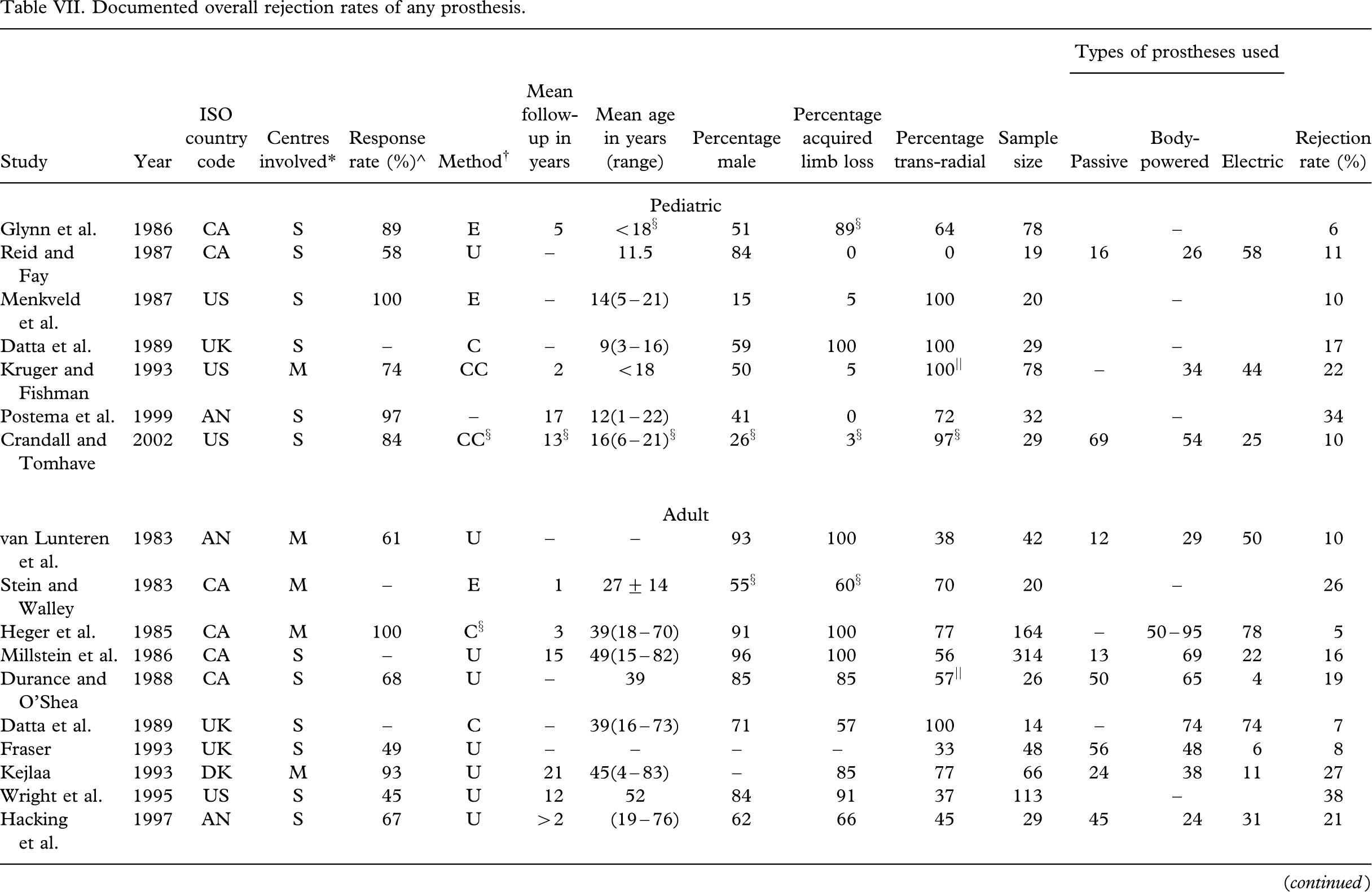
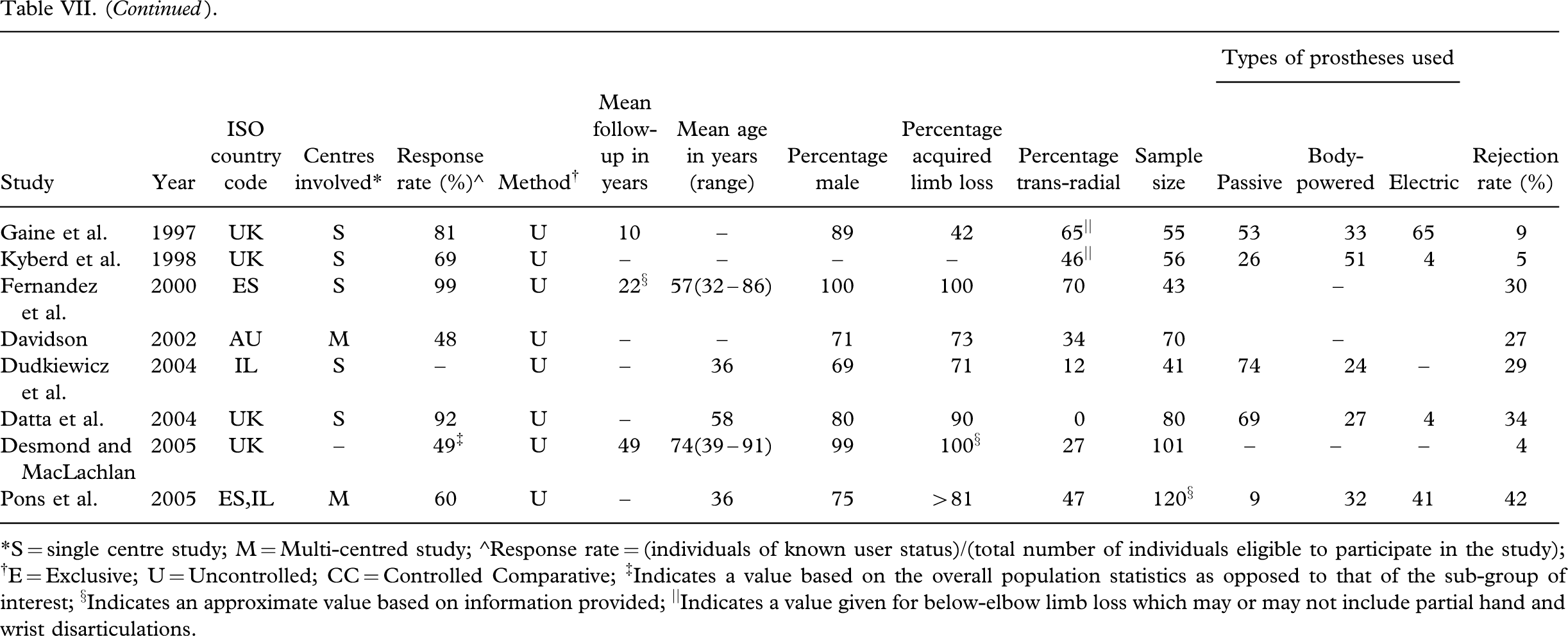
∗S = single centre study; M = Multi-centred study; ∘Response rate = (individuals of known user status)/(total number of individuals eligible to participate in the study); †E = Exclusive; U = Uncontrolled; CC = Controlled Comparative; ‡Indicates a value based on the overall population statistics as opposed to that of the sub-group of interest; §Indicates an approximate value based on information provided; ||Indicates a value given for below-elbow limb loss which may or may not include partial hand and wrist disarticulations.
The extent to which prosthesis design affects rejection is not clearly defined. Kejlaa (1993) determined that the majority of prosthesis rejections were due to external factors such as delayed prosthetic delivery, medical complications, or lack of need, with only 22% of cessations attributable to prosthetic problems or discomfort. Glynn et al. (1986) on the other hand noted a much higher contribution with 91% of myoelectric rejections resulting from prosthetic-related problems involving comfort, lack of function, and durability. An Indian study noted that 50% of its sample reported repeated mechanical failure of body-powered prostheses as a reason for prosthesis rejection while 38% noted financial constraints (Bhaskaranand et al. 2003). Postema et al. (1999) observed that the primary factors associated with pediatric rejection included lack of functional gain, unattractive appearance, and excessive weight. Melendez and LeBlanc (1988) consulted with amputees currently not wearing a prosthesis and determined that 72% would reconsider using a prosthesis if certain design improvements were made particularly in the area of comfort, while 89% felt that they were simply more functional without the prosthesis, a recurring justification for prosthesis cessation (Scotland and Galway 1983; Trost 1983; Wright et al. 1995; Hubbard et al. 1997; Melendez and Leblanc 1988; Durance and O'Shea 1988). Perhaps the latter rationalization should not be overly surprising considering that an estimated 90% of activities of daily living can be performed one-handed (Glynn et al. 1986).
Discussion
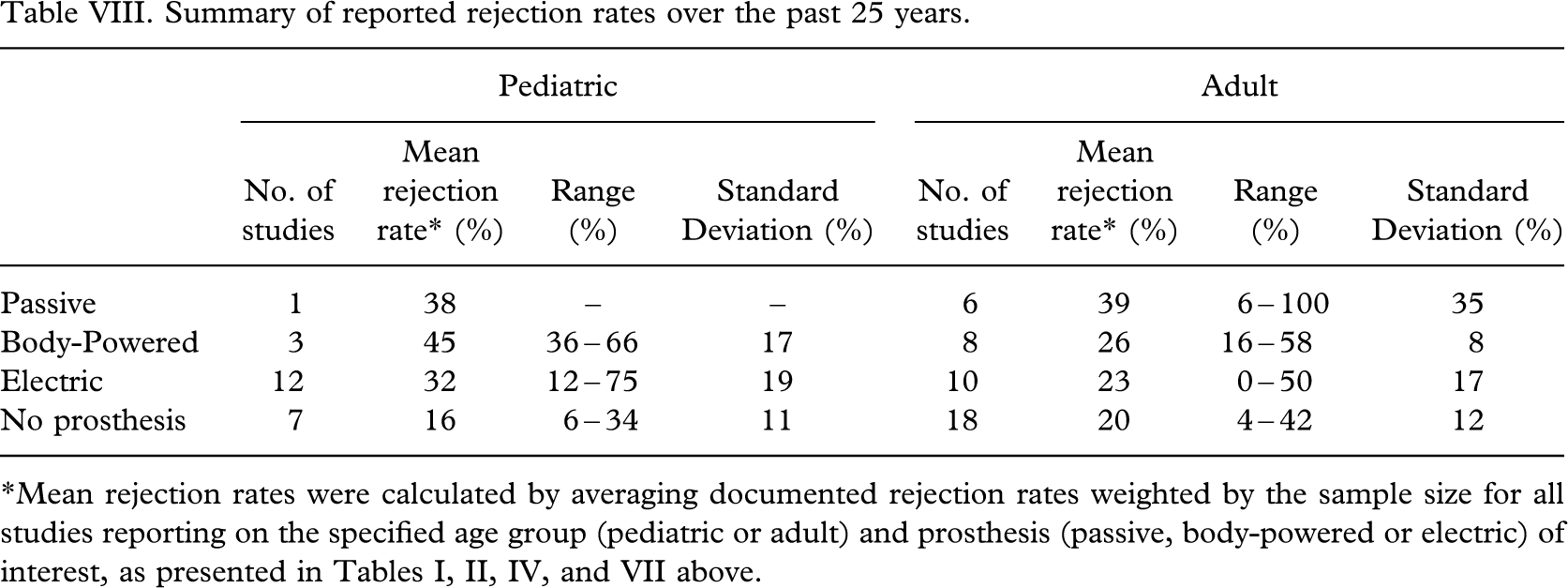
As detailed in the preceding sections, a number of studies reporting prosthesis rejection rates have been conducted in the past 25 years. Table VIII provides the average rejection rates (weighted by sample size) for the various prosthetic options as determined from an amalgamation of these studies. Differences in prosthesis rejection between sub-groups were evaluated using the Chi-squared test with Yates correction. A significantly higher proportion of rejections was observed within the pediatric as compared to the adult populations for both myoelectric (p = 0.01), and body-powered (p < 0.001) prostheses. The incidence of non-wear is statistically similar (p = 0.16) in children (16%) and adults (20%). With only a single study reporting on passive prosthesis use in the pediatric sector, comparisons with the adult population are limited for this genre of device. From the data collected, it is not evident that electric prostheses meet with higher acceptance than body-powered prostheses in adult populations (p = 0.1). Conversely, electric devices may be more widely accepted than body-powered devices by children (p = 0.002). No statistically significant differences in the proportion of rejections were observed between passive and myoelectric (p = 0.2) nor body-powered (p = 0.1) devices. Of note, is the expansive range and large variance in rejection rates as evident in Table VIII. It remains unclear as to what extent these variations can be attributed to differences in sample population, incongruities in methodological approach, and/or characteristics of the clinical programmes or the prostheses involved.
Summary of reported rejection rates over the past 25 years
Directions for future research
From this review, the authors propose the following critical recommendations for future research:
Increase generality of results. Approximately 80% of the identified studies have focused on an isolated population contacted through a single rehabilitation centre. In 80% of studies, less than 80 individuals were sampled with a mean sample size of 63 and a median of 45. This limits both the ability to generalize results, and the inclusion of non-wearers. Identifying significant sample populations is particularly challenging in this specialized field and is often coupled with more relaxed inclusion criteria and more variability among participants. Surprisingly however, the median sample size of uncontrolled studies (n = 52) is not substantially higher than that of controlled studies (n = 44). Incomplete and non-standardized documentation of participant characteristics, clinical interventions, and results has thus far precluded combination of the multitude of smaller studies in a formal meta-analysis. The generality of findings therefore remains in question as do the specific sources of variability between studies. Two avenues by which future studies may attempt to address this challenge are as follows: (a) Increase collaboration and multi-centred research to access a wider population. A review of the literature indicates that the median sample size for a single-centred study is 43 as compared to 78 for multi-centred research; (b) Use standardized tools for comprehensive data collection in order to facilitate comparisons between and meta-analysis of studies for greater generalization of findings.
Focus on controlled study designs. Figure 2 presents the distribution of studies by methodology type. Only three studies (Crandall and Tomhave 2002; Silcox et al. 1993; Kruger and Fishman 1993) in the past 25 years have compared rates of rejection of different prostheses having provided participants uniformly with the devices of interest. Only Crandall and Tomhave (2002) included passive devices along with electric and body-powered as one of the options. The proportion of studies applying an uncontrolled cross-sectional descriptive methodology has increased in recent years with a heightened emphasis on determining the incidence of non-wear independent of prosthesis type. Although such studies do possess their own merits (i.e., longer follow-up, convenience for multi-centre research), a clear need for controlled comparisons of prosthesis acceptance, is evident. It is reasonable to suppose that rates of rejection may differ in parallel with the options available to the individual should they choose not to use a particular prosthesis. The extent to which methodology affects reported rejection rates remains unclear. No distinct trends in rejection rates were noted with regards to methodology.
Deploy formal statistical analyses. Of the 40 clinical studies reporting rejection rates and factors affecting prosthesis acceptance, only 20% conducted a rigorous statistical analysis and reported the significance of confidence levels for observed correlations and effects (van Lunteren et al. 1983; Leow et al. 2001; Wright et al. 1995; Heger et al. 1985; Herberts et al. 1980; Postema et al. 1999; Thornby and Krebs 1992; Hermansson et al. 2005). Limitations in sample size and the large range of variance among participants is a widely asserted obstacle to statistical evaluation of results, especially in terms of sub-group analyses. The clinical importance of conclusions cannot however be ascertained without measures of statistical significance to ensure that observations are not merely a manifestation of random effects. Future studies should be carefully planned in terms of the intended subgroup analyses and expected results in order to enable effect sizes to be included in formal meta-analyses.
Conduct multi-factor analyses. Prosthesis acceptance and rejection is a complex issue dependent on a number of personal, contextual, and technological variables. Figure 3 provides a distribution of the factors studied in terms of prosthesis abandonment in the 40 clinical studies reviewed. Evidently, characteristics associated with the individual attract the most focus with almost 80% of studies considering at least one factor, while only 8% consider five or more of the possible seven characterizing factors identified herein (i.e., gender, age, origin of limb loss, level of limb loss, lifestyle/occupation, interfering medical conditions, hand dominance). Research of clinical, technological, and social factors is less prevalent with 53%, 34%, and 13% of studies addressing these respective issues. To date, no single study has quantitatively and exhaustively addressed all of these factors in order to provide a panoramic of the rehabilitation experiences of individuals with upper limb deficiency. The relative importance and possible interactions between each of these factors therefore remains largely unknown, supporting the need for multifactor studies. Analytical techniques such as multivariate analysis of variance (MANOVA) would facilitate the uncovering of main and interaction effects on rejection rates.
Develop and adopt standardized measurement tools. The lack of standardized outcome measurement tools with an absence of well-defined vocabulary and scales, adds to the challenge of studying largely variable populations, oftentimes precluding comparisons of results, especially internationally. As such, the possible influence of cultural factors remains obscure despite its growing pertinence to the clinical treatment of increasingly diverse client bases. Research efforts should continue to focus on standardized tools for outcomes measurement. The development of validated questionnaires for widespread use should be considered a high priority research area for assessment of individuals with upper limb deficiency.
Provide complete, descriptive documentation. In a number of previous studies, key variables known or suspected to affect prosthesis rejection rates have not been reported. For example, duration of follow-up is not reported in 43% of studies. Characteristics of the prosthesis such as the type of terminal device and the control strategies in place are often not reported or linked with rejection rates. History of prosthesis use, availability of prostheses, and alternative options should a particular prosthesis be rejected, are seldom discussed. Despite strong evidence that rejection rates between pediatric and adult populations may not be comparable, studies often combine these two groups without specifying the age distribution. Although characteristics of the population are in general given, those specific to the sub-groups of interest are often not reported. For example, a study yielding rejection rates for different types of prostheses (i.e., myoelectric versus body-powered) may often neglect to report relevant factors for each sub-group of users (i.e., differences in level of limb loss between the groups) making it difficult to determine the extent to which acceptance is a factor of prosthesis type as opposed to other characteristics of the sub-groups. Incomplete documentation hampers interpretation and comparison of results.
Capture contemporary consumer views. The most recent full-scale study focused on defining consumer satisfaction with prosthetic options was conducted nearly a decade ago (Atkins et al. 1996). Since that time, microprocessors have grown in prevalence owing to changes in reimbursement codes (Lake and Miguelez 2003), and advancements have been made in various areas, for instance silicone gloving material (Huang et al. 2001), and lightweight batteries (Williams 2005). Previous studies may not have captured changes in consumer views brought about by social and technological developments such as these. Initiatives to collect up-to-date feedback are essential to monitor evolving consumer preferences amid the digital revolution.
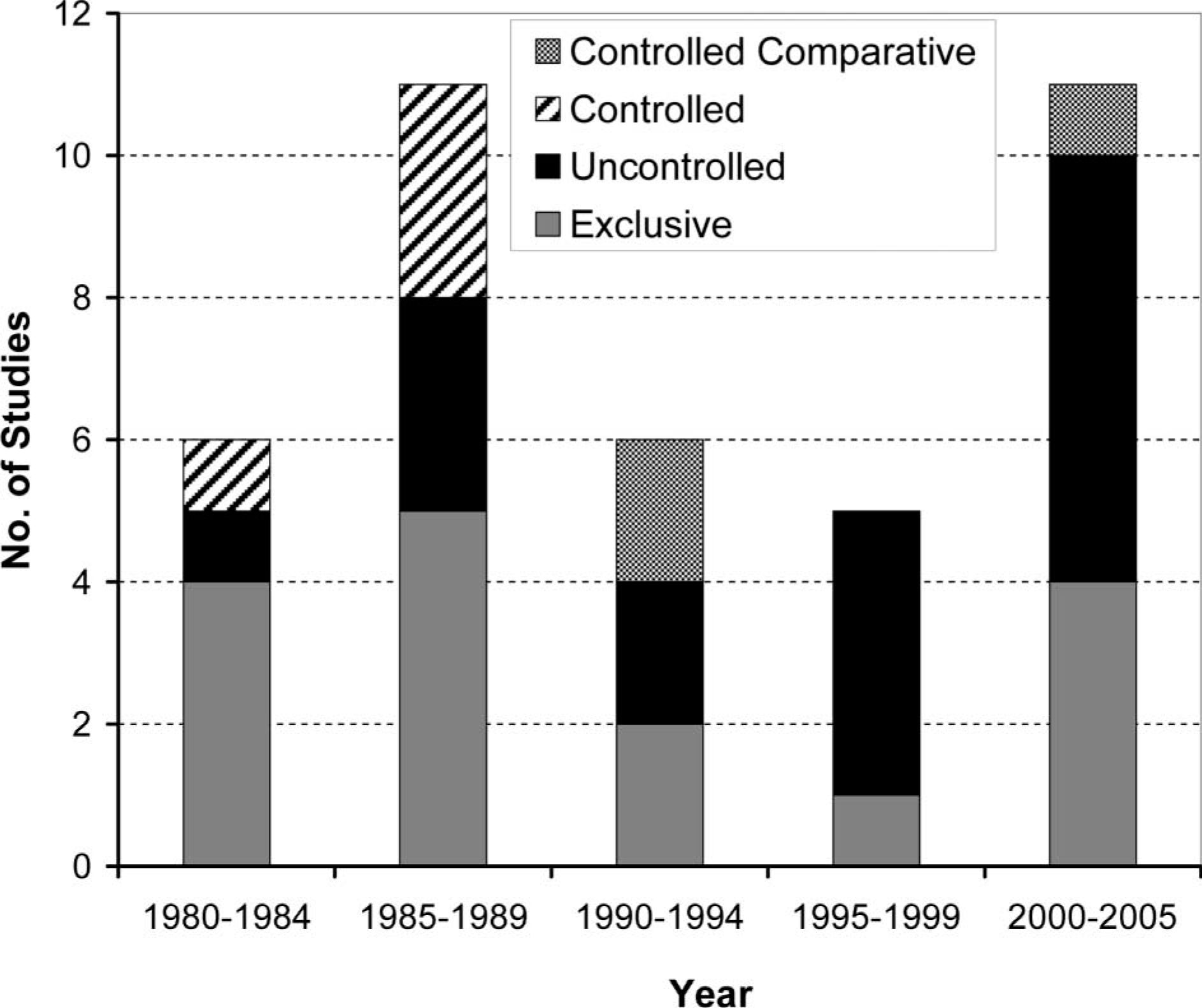
Distribution of studies by year and methodology type.
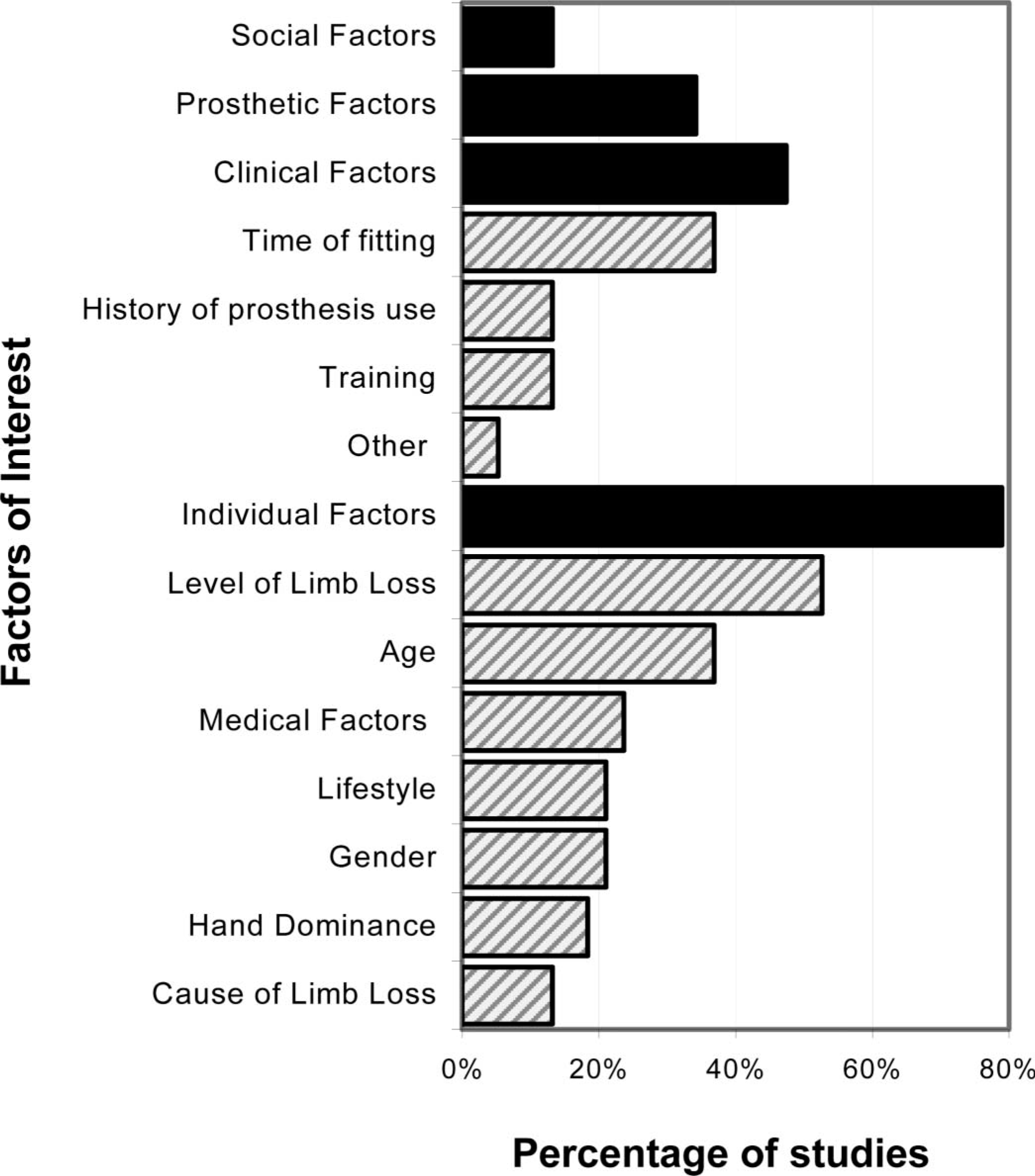
Distribution of social, prosthetic, clinical, and personal factors (solid bars) along with associated sub-factors (hatched bars) as studied in the past 25 years.
Conclusions
It remains difficult to sketch a truly reflective picture of the general state of upper limb prosthesis use and abandonment based on the available literature to date. The development and use of standardized tools for assessment of this population is vitally important to ensure that future studies do not remain as isolated pockets of knowledge, but contribute to a collective understanding of the factors affecting prosthesis acceptance and rejection. The ultimate goal of healthcare professionals and researchers in this field should be to provide the information, technology, expertise, and opportunities necessary for individuals with upper limb deficiency to maximize their quality of life, whether that be through use of active prostheses, passive prostheses, or no prosthesis at all. Increased emphasis on participatory research and consumer satisfaction is needed to ensure that future prosthetic designs can bridge the gap between research lab and clinic, clinic and home.
Footnotes
Acknowledgements
The authors would like to thank Colin Macarthur for his insight and guidance in the preparation of this manuscript. This work was supported in part by the Natural Sciences and Engineering Research Council of Canada, and the Canada Research Chairs Program.