
Abstract
Background:
Disability is inextricably linked to poverty. A total of 80% of the disabled population lives in low-income countries. The demand for prosthetic and orthotic services in these countries is increasing, and a variety of methods to provide services are currently used.
Objectives:
To assess current models of provision to facilitate sustainable, evidence-based prosthetic and orthotic services.
Study Design:
Literature review.
Methods:
A literature search was performed through Medline (Ovid), PubMed, ISI Web of Knowledge, EMBASE and RECAL Legacy using combinations of subject heading and text word searching strategies. Full-text publications were critically appraised and ranked according to the Scottish Intercollegiate Guidelines Network guidelines.
Results:
Three areas were deemed pertinent to the research question. Studies were grouped into one or more of these categories based on the issues addressed: instigators, types of service provision, demographics and region-specific issues. It was found that many complex factors influence prosthetic and orthotic services in low-income countries. Demographic and regional idiosyncrasies require prosthetic and orthotic services to be tailored to address the specific needs of individual countries.
Conclusions:
The lack of and quality of available research made efficacy of methods used to provide services in low-income countries difficult to determine.
Clinical relevance
This review aims to highlight areas of best practice in prosthetic and orthotic services in low-income countries and to show where further research is required in order to develop evidence-based prosthetic and orthotic services.
Keywords
Introduction
The World Health Organization (WHO) estimates that 650 million people worldwide are disabled. This equates to approximately 10% of the world’s population. Of those people, 80% currently live in low-income countries (LICs). 1 The World Health Survey carried out in 2004 found, across 59 countries, the prevalence rate of disability in the adult population to be 15.6%, from 11.8% in high-income countries (HICs) to 18% in LICs. 2
LICs account for 84% of the world’s population and 90% of the total disease burden. 3 However, fewer than 3% of persons with disabilities in LICs have access to required rehabilitation services. 4 Without access to the rehabilitation they require, those with disability may become entrenched in a cycle of poverty (Figure 1). 5
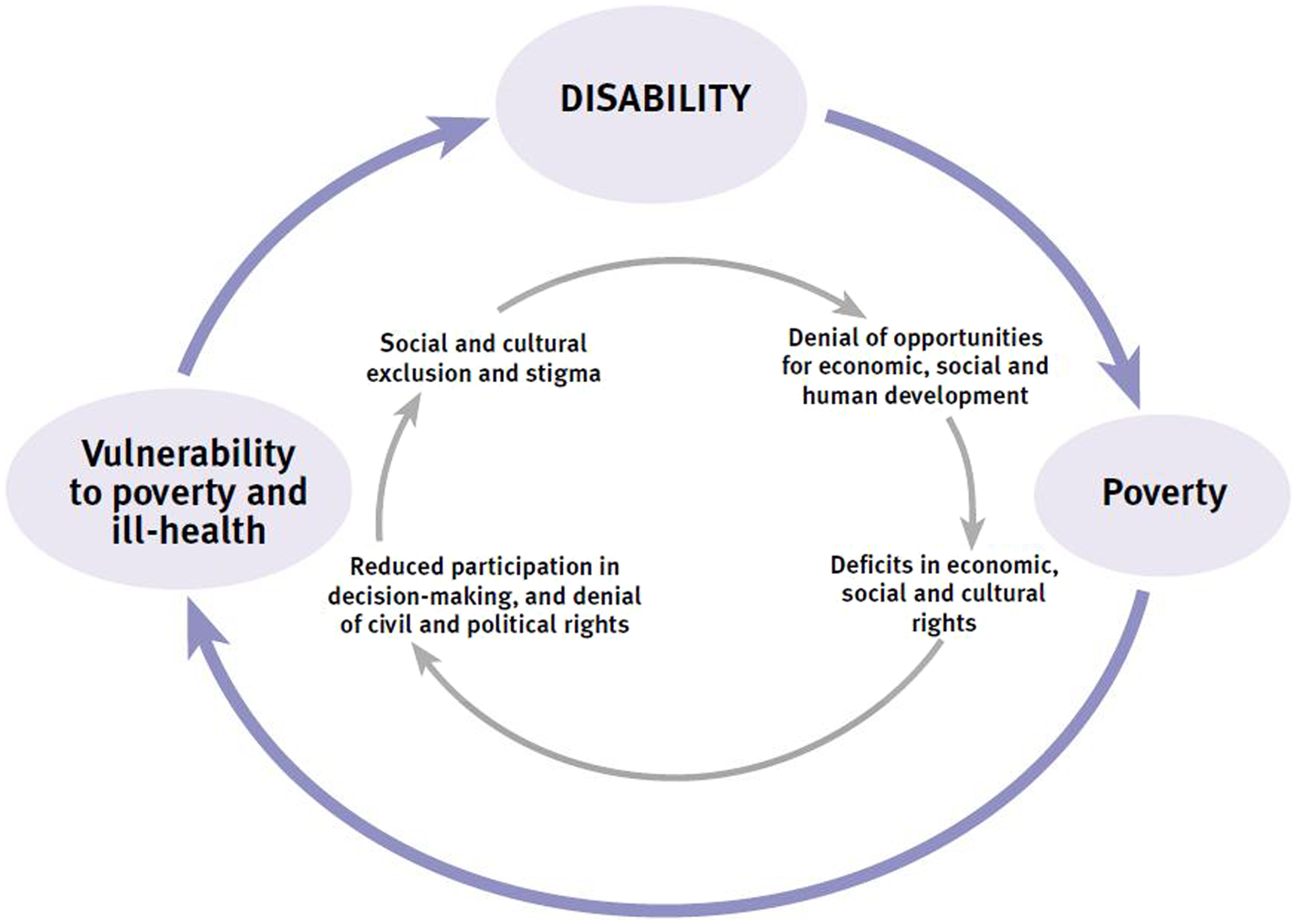
Poverty and disability.
The WHO estimates that among the disabled people living in LICs, the need for prostheses will have risen to 30 million by 2011. 1 The need for orthotic intervention is thought to be even higher 6 but remains underreported as requirements are not as visible as are those of prosthetics. 7
To address rehabilitation issues, a plethora of legislation has been produced.2,7,8 Despite this, varied levels of service provision exist in LICs. Entitlement to access rehabilitation services is emphasised in legislation. However, in countries where the gross national income is low, rehabilitation services are rarely prioritised6,9,10 as primary health care understandably takes precedence. 6 Conversely, as primary health-care initiatives achieve success, greater demand is created for rehabilitation services as more disabled people survive infancy. 11
More research is required to assess current models of service provision in LICs. This review will assess current literature to examine evidence into different methods of prosthetic and orthotic service provision. Instigating factors will be addressed and discussed in the context of demographic and regional issues. Finally, variations in service provision will be discussed.
Methodology
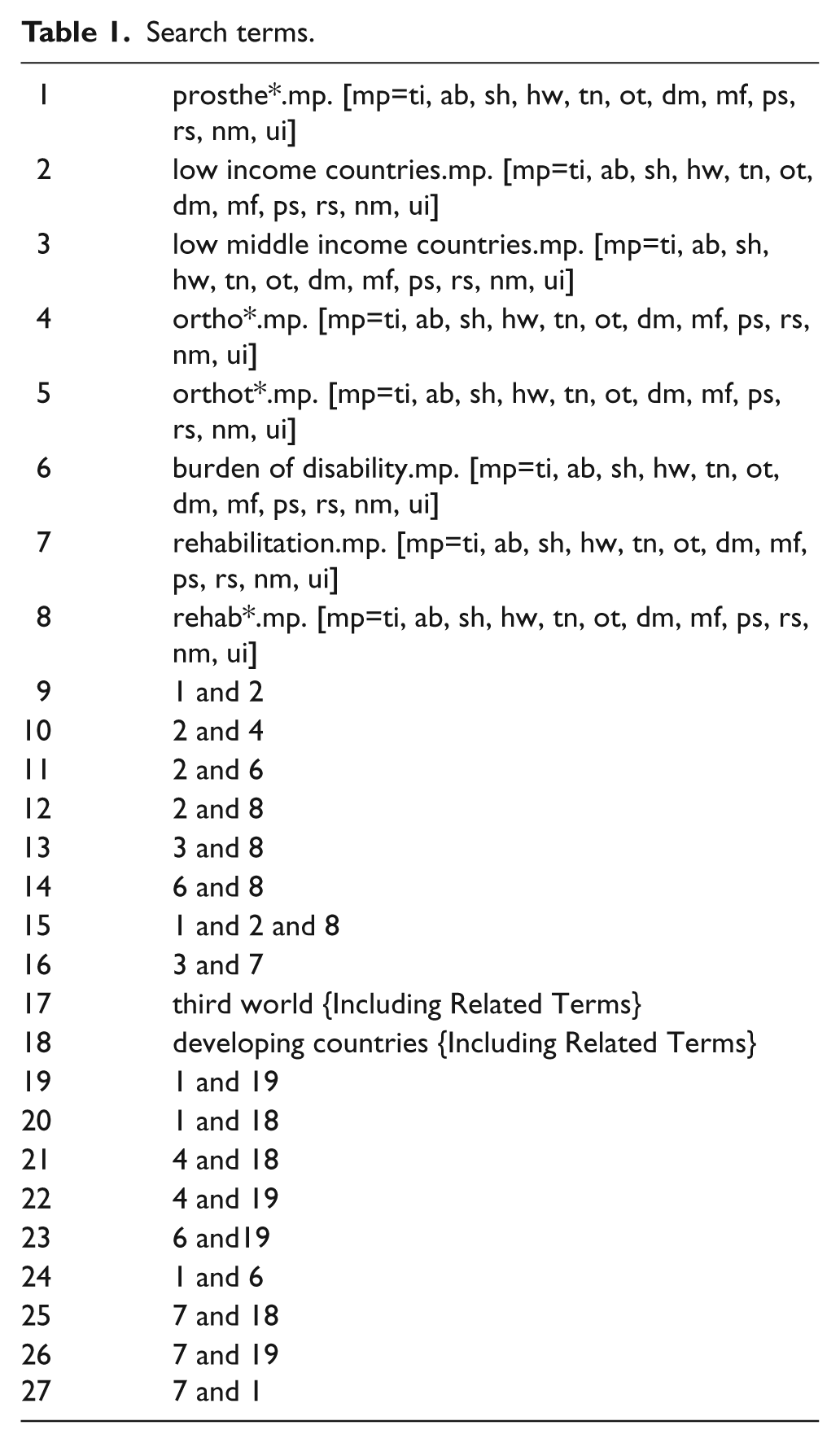
A literature search was performed through Medline (Ovid), PubMed, ISI Web of Knowledge, EMBASE and RECAL Legacy using combinations of subject heading and text word searching strategies. The search strategy used a combination of the following keywords: Prosthe*, low income countries, low middle income countries, ortho*, burden of disability, rehabilitation, rehab, third world, developing countries (see Table 1).
Search terms.
Only articles available in English were considered. The searches spanned the period from the earliest date of each database until March 2011. Secondary searches were subsequently carried out. Pertinent citations from reviewed articles were examined. In addition, as many professionals in LICs do not have an opportunity to publish their opinions and activities in peer-reviewed journals, secondary sources were considered, including conference proceedings, editorials, media publications and information garnered from reputable websites.
Full-text publications were critically appraised and ranked according to the Scottish Intercollegiate Guidelines Network (SIGN) guidelines, 12 designed to evaluate the evidence base for clinical guidelines for the National Health Service (NHS) in Scotland.
Based on the abstracts, broad inclusion criteria were applied to ensure that all relevant evidence was included. Articles were required to relate to disability rehabilitation, contain information on rehabilitation in LIC and include information regarding prosthetics and orthotics. Studies were excluded if only the abstract was available.
Results
Following application of inclusion criteria and removal of duplicates, 82 articles remained. Three areas were deemed pertinent to the research question. Studies were grouped into one or more of these categories based on the issues addressed:
Instigators;
Demographics and region-specific issues;
Types of service provision.
Instigators
The Convention on the Rights of Persons with Disabilities (CRPD) became legally binding on 3 May 2008. 13 Four action triggers are thought, by Staats, 7 to be required prior to instigation of prosthetic and orthotic services programmes: social equality and awareness of disability, political equality of the disabled, sufficient demand for services and a moral imperative towards rehabilitation.
CRPD article 8 dictates that states take immediate, effective and appropriate measures to raise awareness and foster respect for the rights and dignity of persons with disabilities and promote awareness of their capabilities and contributions to society. 14 A total of 147 member states 15 have agreed to promote, protect and ensure the full and equal enjoyment of the human rights and fundamental freedoms of people with disabilities and to prompt respect for their inherent dignity. 16 This will be particularly challenging in LICs. To address this, the CRPD requires aid-giving countries to assist implementation. 14
The convention created a legal imperative for LICs and all other member states to promote media and public awareness, 7 which is imperative to instigating prosthetic and orthotic service development. There is often a great deal of media attention surrounding technological advances in the field, which are media friendly. 17 Very little coverage occurs, however, of the planning and research that creates sustainable services to meet the needs of the majority of patients. 18 This can lead to services becoming focused on new technology rather than on creating an effective service. 19
CRPD article 29 states that parties will guarantee political rights to persons with disabilities and the opportunity to enjoy them on an equal basis. 14 This may encourage the creation of a political imperative, 7 which has been suggested to pressurise governments into action. The UK Department of International Development stated in its 2000 report that there is a substantial and fundamental difference between disability and other types of disadvantage, such as poverty. 5 People with disabilities have physical barriers to participating in society, claiming and utilising their rights. The report suggests that persons with disabilities can only claim their rights once their practical needs, such as prosthetic and orthotic devices, have been met. 5 Paradoxically, in order to claim their rights and exert pressure on their governments to create prosthetic and orthotic services; disabled persons must have access to prosthetic and orthotic devices.
The third trigger thought to be required to instigate prosthetic and orthotic service provision is sufficient demand, where a critical mass of need is reached. 20 Legislation cannot affect the number of people requiring prosthetic and orthotic services, however, Article 32 of the CRPD ensures International Cooperation so that once critical mass is reached LICs have support to instigate services. 14 This article deals specifically with the need for prosthetic and orthotic services through suggested measures such as provision of appropriate, technical and economic assistance, including access to assistive technologies, and transfer of technologies.
The remaining trigger, ‘the moral imperative’ 7 is beyond the scope of even the most ambitious international legislation. To gain government support, stressing economic benefits of services may be more effective. Cummings 20 suggests that LICs find that treating disabled persons is fiscally responsible.
International legislation does not guarantee action but can act as a catalyst. It also provides a foundation in law to support attempts to implement prosthetic and orthotic services. 16 Concerted effort to enforce and monitor the effect of legislation on the lives of disabled persons is necessary. 6 Failure to do so may result in legislation having little impact on the patients in LICs.
The economic viability of prosthetic and orthotic services is an important factor. A study carried out to investigate low attendance at a rural prosthetic and orthotic service in India with large numbers of disabled persons found a variety of reasons for non-attendance. These included socio-economic issues and lack of proper transportation facilities. The authors believe that in order to increase service utilisation, people must be made aware that disabled persons can be rehabilitated and become independent members of society. 21 This reduces the demand on government funding and contributes to the economy.
Although LICs are categorised together due to their economic circumstance, it is important to consider countries on an individual basis as successful programmes are not necessarily transferable. 12
Cummings highlighted a list of factors to be considered when creating prosthetic and orthotic services, which can be adapted for use in most countries. These included social, economic, cultural, religious, psychological and climatic factors; available technology, materials and resources and time and distance constraints. 20
Other allied health professions have undertaken research into overcoming barriers in rehabilitation service provision.8,22 Research has focused on the Community-Based Rehabilitation (CBR) model first promoted by WHO as a way to reach the rural poor, up to 90% of the population in some LICs.19,23 Although this model has been in place for over 40 years, research has only recently begun investigating its effectiveness.23,24,52 Although WHO published updated CBR guidelines in 2010, 25 it remains unclear from the research where prosthetics and orthotics fit into this model.
A thorough assessment of the prosthetic and orthotic needs within a LIC is vital, not only to discover the specific needs of the country but also to serve as an instigator for meeting those needs.26,27 Needs assessment data are unclear. 26
Demographics and region-specific issues
Demographics of LICs create a patient population vastly different from that in HICs. Unlike HICs, most LICs have largely rural populations with some African nations having a 90% rural population. 28 LICs also have a considerably lower life expectancy than HICs resulting in a higher proportion of paediatric patients. 28 Paediatric patients create an even greater demand on limited resources as devices must be continually replaced due to growth and the higher activity level of children compared to adults.
Conversely, HICs have increasingly ageing patient populations, resulting in peripheral vascular disease, diabetes and other lifestyle-related diseases vastly outnumbering trauma. 29 However, diseases that have long been eradicated in HICs, such as polio and malaria, are common in LICs alongside diabetes, which is a growing problem. 30 Traumatic injuries due to poor health and safety and increased traffic with poor road safety are also common.
A study of prosthetic and orthotic services in India 21 highlights these differences. There were four times as many males as females, all patients were under 30, most males were between 11 and 30 years old and most females were below 10 years old. 22 This is indicative of many LIC societies where women often remain at home and men carry out manual labour with poor health and safety standards.
The commonalities of poverty, lack of resources, demographics and the prevalence of diseases, which have been eradicated in the rest of the world,28,30 can lead to sweeping generalisations regarding the needs of LICs. Unique aspects of each country’s history, politics, culture and social structure must be taken into account when planning any prosthetic and orthotic service. Failure to assess individual needs lead to failure of services 31 It is clear from the literature that disabilities have a major impact on quality of life in LICs. 5 It has been established that disability is inextricably linked to poverty. 5 In a vicious cycle, poor people are vulnerable to disability through poor health, living and working conditions. Subsequent disability is then a further detriment to their ability to prosper economically forcing them deeper into poverty. 5 High rates of disability are also related to high levels of illiteracy, reduced immunisation rates, poor nutritional standards, low birth weights, high levels of unemployment and reduced occupational mobility. 1
In the aftermath of war or disaster in LICs, all of the aforementioned issues become magnified by major physical destruction. Following a prolonged armed conflict where there has been a breakdown of health services, a lack of treatment and control of diseases alongside the inevitable increase in traumatic injuries, there is a massive increase in the demand for prosthetic and orthotic services. This creates a further burden on the already depleted resources. 31
The legacy of landmines remains and continues to contribute to an increased patient population long after conflict is over 50 . They also cause great problems for transportation and reaching patients. 30
Each LIC has individual problems and idiosyncrasies mitigating against a unified strategy for the prosthetic and orthotic needs of all LICs. Peizer 18 suggests a three-step process to tailor projects to the needs of the host country and create a sustainable service. He states that, first, meetings should be held between officials from the host country and the sponsors of the project. Input from the International Society for Prosthetics and Orthotics (ISPO) for training, evaluation and planning should also be sought. Second, site visits should be carried out with ISPO involvement, in order to evaluate the baseline situation and requirements of the host country. Third, the project should be designed and planned based on information gained in the previous two stages.17,18
Cultural norms such as sitting cross-legged, squatting, barefoot walking, genuflecting to elders or in religious ceremonies, navigating uneven terrain and many similar issues must be considered when providing prosthetic and orthotic services. 32 Specific challenges are encountered in each LIC. In Cambodia, the Khmer Rouge eradicated professionals and created a fear of education and the educated. 8 In Ghana, disabled persons are thought to be cursed and have historically been ostracised by society and even killed. 33 In Latin America, very large families entirely economically dependent on the father are commonplace. 34 In Vietnam, all services must be routed through the centralised Communist government. 28
Types of service provision
Peizer puts forward three models of service provision in LICs, 18 the aiding of research programmes, introducing new technologies into established centres and the establishment of new centres. 20 These are not the only models of service delivery utilised in LICs. In many countries, patients are still sent to Europe or America for treatment. 19 Foreign organisations take casts and impressions and send them home for fabrication. 32 Computer Aided Design–Computer Aided Manufacture (CAD-CAM) is being introduced to increase production levels. 35 CBR is being utilised in order to reach the rural poor. 23 Indigenous education and training programmes are being implemented to create an indigenous workforce. 30
There are issues surrounding each of these service models, particularly with sending patients overseas for treatment. 20 This can result in children being absent from their homes for extended periods. 19 Maintenance and replacement of devices also becomes an issue if there are no local services.
Often services take a ‘relief’ approach. Although it is tempting to follow a route of instant gratification, without the planning and implementation of sustainable programmes, the initial achievements are nullified. 32
The overwhelming majority of patients who require prosthetic and orthotic services in LICs live in rural areas in extreme poverty. 1 In the 1970s, to coincide with goal of ‘Health for all by the year 2000’, 36 WHO began promotion of CBR to reach this large section of the patient population. In theory, CBR services contain three levels that work together to deliver appropriate rehabilitation services:
Community level;
Intermediate level;
Specialised or tertiary level. 20
Prosthetic and orthotic services, with their specialised nature and complex technology, are not easily placed into the CBR model. Whether or not CBR is the chosen model for service delivery, there must be provision made for the rural poor.
Most programmes that are set up by foreign non-governmental organisations (NGOs) have the ultimate goal of handing over to the local authorities. 26 One way of attempting to ensure programmes can be handed over to capable hands is to establish effective education and training programmes. Training and education must result in an accreditation that places graduates in an appropriate position within the hierarchy of the country’s health system.30,49 Without this there is a risk that graduates may leave the profession or emigrate to work overseas.34,49 The creation of an indigenous workforce, with knowledge of local culture, customs and lifestyle, within a respected profession could ensure sustainable services.
When compared to the lack of evidence for service provision, there are a plethora of articles regarding prosthetic and orthotic technology in LICs.17,51 There is a consensus in the literature that appropriate technology is required in LICs. A consensus does not emerge, however, regarding what constitutes appropriate technology.
Importing prosthetic and orthotic technology from industrialised countries often fails to meet the needs of disabled persons in LICs. 35 Technology from industrialised countries requires regular maintenance and is not designed for the environmental or lifestyle needs of disabled persons in LICs.17,51 Indigenous devices, however, are often regarded as primitive. 32
There has been much research regarding specific aspects of technology, again dominated by prosthetics. 17 The prosthetic foot in particular has been the subject of many studies, as it has been determined to be the component that fails most often in prostheses in LICs. 22 Research has and is being carried out to design prosthetic and orthotic technology that can withstand the rigorous demands of the environment and lifestyles in LICs.
Professional and clinical issues of creating ‘appropriate technology’, treating patients with complex problems and the sheer number of patients make service provision difficult. These problems at least fall within the skill set of the prosthetic and orthotic professional. The less researched problems of service delivery, administrative and organisational issues are often more difficult for professionals to address. The long-term sustainability and success of any project is placed in jeopardy if they are not addressed efficiently. 19
The right of access to prosthetic and orthotic services for all is now enshrined in international law. 15 Although this has been the case since 2008, very little impact has been reported in the lives of disabled persons in LICs. 9 Prosthetic and orthotic services have been characterised as ‘Good intentions, charity and small scale model programs’. 1 It is not possible to meet the extensive needs of the large number of disabled persons through individual small-scale initiatives no matter how well intentioned.
In order for the needs of disabled persons in LICs to be met, they must first be understood. 16 The vast majority of patients who require prosthetic and orthotic services in LICs are the rural poor;4,21 however, they are not represented in the decision-making process, with disability remaining a taboo. 33 In many LICs disability is seen as a curse or punishment. In order for legislation to be truly effective in protecting the rights of disabled persons, there must be consideration of cultural and social attitudes and measures introduced to address these barriers. Maintaining and replacing devices is imperative, particularly in paediatrics; however, poor literacy rates and language barriers can impede communication regarding accessing services.
The media and public awareness imperative 7 is important in influencing attitudes. The media must highlight not only the needs of disabled persons but also the success stories of disabled persons who participate in mainstream society following effective prosthetic and orthotic care.
Resources should be directed to areas where they are needed most. In order to do so, there must be a comprehensive assessment of the prosthetic and orthotic needs. 1
Three prosthetic-only needs assessment surveys were carried out in Cambodia by the American Red Cross. 26 Only 17% of the population, however, was surveyed due to issues with accessibility of communities and communication. The results were extrapolated out to represent the whole population. The 17% was from provinces that had not experienced high conflict. 26 This would suggest that the actual number of amputees in the total population may be much greater than the extrapolated 21,200 stated in the report. The orthotic needs of Cambodia were not considered despite the fact that orthotic needs are known to outweigh prosthetic requirements in most countries. 7 Baseline data are required to evaluate services and create evidence-based practice.
An improved body of research should not only show the current state of prosthetic and orthotic provision in LICs but also demonstrate, through reliable data rather than extrapolated assumption, the scale of the demand for prosthetic and orthotic provision.
It is important for any public service to be cost-effective. Prosthetic and orthotic services must be seen to be economically beneficial in order to gain support from a host LIC government. In a study of Vietnamese amputees, 83% who had received functioning prostheses described themselves as employed. 31 Only 49%, however, were employed out of their homes, the remainder generally worked as home farmers. 30 These results show that, with effective prosthetic and orthotic treatment, disabled persons can be economically productive. 31
When NGOs and aid organisations provide prosthetic and orthotic devices without charge, however, they may affect indigenous efforts to provide prosthetic and orthotic devices as local workshops cannot compete with the free high-tech devices offered. 37 This may impact the local economy and can lead to local resentment of the foreign programmes. Supporting local initiatives with training and sourcing local materials may be a more effective use of resources to ensure sustainable services and economies without dependency on NGOs.
Often overlooked is the vastly different patient presentation facing prosthetic and orthotic professionals in LICs. 30 Poor surgical techniques and rehabilitation treatment add to complex patient presentations. 38 Consequently, patients present with untreated extreme joint contractures, poorly healed wounds, a greater number of transfemoral than transtibial amputations and untreated congenital conditions such as Talipes Equinovarus. 39 The complex nature of these patients requires a high level of education and training to provide effective prosthetic and orthotic services in LICs. 40 This is rarely the case. 30
Programmes in LICs are commonly staffed by a small number of expatriate Category I professionals alongside various categories of local staff. 27 The service in Harare, which previously utilised exclusively expatriate prosthetists, now operates with 11 Category II orthopaedic technologists, 7 of whom were trained at the Tanzania Training Centre for Orthopaedic Technologists (TATCOT) school in Tanzania.26,28
The Harare project illustrates consideration of sustainability. Education of local people to continue programmes not only creates sustainable prosthetic and orthotic service provision but also creates professionals who have an inherent local knowledge of local customs. 30 Education and training of the indigenous population is essential to ensure sustainable prosthetic and orthotic provision in LICs.
Expatriate professionals cannot remain indefinitely in LICs. Through passing on their skills to local people, the future of services can be ensured following their departure. Local professionals are invested in ensuring the survival of prosthetic and orthotic services. Beyond the moral imperative of serving in their own communities, there is a more calculable incentive in sustaining a service that maintains their professional status in a well-paid career. Promotion of professional status is important as in many LICs prosthetics and orthotics technicians lack training and equipment and are regarded as lesser members of the rehabilitation team and are paid accordingly.
In the immediate aftermath of natural disasters and conflicts, focus may be directed to relief rather than sustainability. Once the shift is made towards sustainability, however, the long-term legacy of many modern conflicts becomes an impediment to service provision. In 1997, there were approximately 120 million landmines spread across 71 countries. 41 A further 2–5 million landmines are suspected to have been deployed per year since then; causing profound medical, environmental and economic consequences. 41 There is not only a dramatic increase in the number of patients requiring prosthetic and orthotic services in areas where mines are highly concentrated but also the task of reaching these patients is made difficult and dangerous. In addition to isolating communities, landmines also disturb infrastructure by isolating power lines, bridges, water supplies, food transport, road and rail networks. 41
The plight caused by landmines has a major impact on the numbers of new patients created in these countries. 32 Much of the literature advocates an approach of preventative prosthetics, 32 which involves educating locals of the risks posed. This has been successful in reducing the number of farming accidents, road traffic accidents and other traumas. This, alongside improving health and safety standards, road safety awareness and introducing safer working practices, could dramatically reduce the number of patients requiring prosthetic and orthotic services as a result of trauma. 42
CBR has been the focus of rehabilitation efforts in LICs since the 1970s. 41 To link with other rehabilitation professions and to reach the rural poor, who constitute the majority of patients, it would appear beneficial to incorporate prosthetic and orthotic services within the CBR structure.24,25 The question remains as to where in the CBR structure these services would operate. It would be exceptionally difficult to provide prosthetic and orthotic services solely at community level. The specialised casting techniques are not easily transferable to volunteers or family members. 42
CBR has been hailed by many agencies, including the United Nations, as the way forward in providing rehabilitation services to rural communities in a cost-effective manner. 22 However, there are dissenters to this position. Haig et al. 43 in their 2009 article describe CBR as a politically expedient way to allocate the least amount of money possible to the problem. They suggest that CBR is a process of delegating highly skilled rehabilitation treatment to cheap uneducated locals without proper training or sufficient input from medical professionals. 43 Much of the burden of care falls upon family members, almost always women and girls. 44 There is a fear that rather than empowering local people, CBR will add to the burden of care placed on women and girls in poor rural communities. 44 This added responsibility may prevent girls from attending school further disadvantaging them. 44
By providing prosthetic and orthotic services through the CBR structure, there is a risk that services may be provided by volunteers with little or no training. Further research is needed to define the place of prosthetic and orthotic services within the CBR structure.45,48
There are problems surrounding all methods of service provision. Removing patients to HICs to receive treatment is utilised in some LICs, particularly in the immediate aftermath of natural disasters. 32 Although the patient receives the gold standard of care, there are serious social ramifications to this process, which is only available to minority of patients. 19
The desire to provide the best possible service to the largest numbers who require it has a major effect on prescription. The natural instinct is to consider technology as the pinnacle prescription choice in LICs. 39 This, however, is rarely true. 32 Western technology is not only prohibitively priced but is not designed to be used in the environments or cultures of LICs. 26 Even when projects utilise donated western devices, their complexity predisposes then to require regular repair and replacement. 46 It is difficult to refuse free devices even when they are not fit for purpose. This creates a false economy, however, as there is rarely the expertise to repair such devices, and the supply is not reliable enough to offer a sustainable service. 36 There is a need for support of research into utilising locally available sustainable materials.
There is now a substantial body of research regarding a variety of devices that provide an evidence base for prescription in LICs. 26 The same cannot be said for service provision. Clearly, there is a need for research regarding appropriate technology for LICs; however, there is little use for even perfect technology if it does not reach the people who need it.
Although there are a variety of methods employed to provide prosthetic and orthotic services in LICs, one feature that all successful programmes have in common is systemic planning. Advocates of telehealth in LICs consider the administration and organisation of projects to be the unglamorous and, therefore, underreported face of telehealth. 45 The same is true of prosthetic and orthotic provision. Although not high profile or media friendly, without strategic planning, focused administration and effective management, projects are likely to fail. 18
Conclusions and recommendations
Data regarding the provision of prosthetic and orthotic services in LICs are unclear. 20 To improve current service provision, increased knowledge of current service model provision and what is lacking is required. A detailed needs assessment must be carried out within individual LICs.
The literature makes it clear that disability is intrinsically linked to poverty. The right to have access to rehabilitation services is now enshrined in legislation. 16 This, however, is only the beginning, and there must be a concerted effort to ensure that legislation is implemented.
It is important to recognise the economic benefits of prosthetic and orthotic provision and impress these benefits upon the governments and funding organisations of LICs. 47 Strategic planning of any project is a necessity to ensure sustainability, and this includes securing long-term funding or support.
LICs are not a homogenous entity to which blanket policies or methods of prosthetic and orthotic service can be applied unilaterally. The regional issues discussed must be considered, and programmes should be tailored accordingly.
There is a distinct slant in the literature towards appropriate technology rather than provision of service. A substantial body of research is needed to prove the efficacy of the methods of service provision; maximise the effective methods and to develop evidence-based, sustainable services.
To create sustainable individually tailored prosthetic and orthotic services, a workforce of well-trained local prosthetic and orthotic professionals must be employed.
Although there is obvious requirement for services, more specific data are necessary to create effective prosthetic and orthotic services. These services have the potential to reach impoverished disabled persons and may provide opportunity to break the cycle of poverty and disability. 5
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.