
Abstract
Background:
Evaluation of the effects of brace treatment on quality of life in adolescent idiopathic scoliosis is important.
Objectives:
To analyze the validity and reliability of the Turkish version of the Brace Questionnaire.
Study design:
Cohort study, evaluation of reliability and validity of the Turkish version of the Brace Questionnaire.
Methods:
Twenty-eight patients undergoing brace treatment for adolescent idiopathic scoliosis (median age: 14.6 years) were included in the study. The Brace Questionnaire was translated into Turkish and administered to the patients twice at an interval of 5 days. Reliability was assessed using the test–retest method (Pearson’s correlation coefficient); internal consistency was analyzed using Cronbach’s alpha. Validity was assessed by correlating the Brace Questionnaire with the Bad Sobernheim Stress Questionnaire-Brace and Scoliosis Research Society-22 questionnaire.
Results:
The mean Cobb angles were 31.1° ± 8.3° and 29.7° ± 9° for thoracic and lumbar regions, respectively. Cronbach’s alpha was 0.94. Intraclass correlation coefficient was 0.95 in test–retest reliability analysis. The correlations between Brace Questionnaire and Bad Sobernheim Stress Questionnaire-Brace and Scoliosis Research Society-22 were r = 0.67 and r = 0.64, respectively.
Conclusion:
The Turkish version of the Brace Questionnaire to measure the effects of brace treatment on quality of life in adolescent idiopathic scoliosis was found to have good validity, excellent reliability, and high internal consistency.
Clinical relevance
We recommend routine use of the Brace Questionnaire in scoliosis patients to evaluate brace-related quality of life and relevant factors and to support the individual when necessary during such treatment.
Keywords
Background
The most efficient conservative treatment for idiopathic scoliosis (IS) is reported to be a spinal orthosis when the curvature progression is moderate (Cobb angle: 20°–40°) 1 to severe (⩾45°), 2 and skeletal development has not been completed. 3
The primary purpose of orthosis application is to prevent further progression of the curve during the period of growth. 1 Additionally, the literature reports orthosis application to be effective in decreasing curvature progression in patients with good compliance (duration of orthosis use > 20 h/day). 4
It is also known that rib cage mobility can be limited with an orthosis, leading to paravertebral muscle weakness and decreased aerobic work capacity. 5 Furthermore, an orthosis may create psychological stress as it can cause the child to become conscious of his or her appearance and avoid school physical activity or leisure time activities 5 and negatively affect the quality of life.
Evaluation of brace treatment is suggested to include the patient’s perspective, which can be obtained with the use of patient-reported outcome measures. 6 Therefore, a brace-related questionnaire is needed to provide objective information regarding the selection of the correct treatment method to the clinician and to meet the expectations of the patient by considering the potential problems.
The Brace Questionnaire (BrQ) was developed in Greece to meet this need. The scale investigates the effect of orthosis application in scoliosis from many aspects (such as functional, social, emotional, and spiritual) that form the components of quality of life.7,8 Vasiliadis et al. emphasized the importance of BrQ in the evaluation of the effectiveness of brace treatment in terms of informing the clinician of factors related to the quality of life and the effect of the brace. They reported BrQ to be sensitive in determining the specific problems related to the brace and to be reliable and valid in those with mild and moderate scoliosis. 8 The BrQ has been validated and culturally adapted for use in various countries and continents, including English, 8 Polish, 9 Italian, 10 French, 11 and Chinese 12 versions.
Although there are some relevant questionnaires such as the Bad Sobernheim Stress Questionnaire-Brace (BSSQ-Brace) and the Scoliosis Research Society-22 (SRS-22) questionnaire, others focus mainly on the surgical effects, and only a few questionnaires investigate the effect of the brace on the quality of life. The BrQ is the only questionnaire designed to assess the quality of life for children undergoing non-operative (conservative) treatment with braces and is a comprehensive one. Therefore, it is the proper instrument for the assessment of quality of life in a braced child suffering scoliosis. 8 The SRS-22 was designed to assess the quality of life for children who had surgical treatment. 13 The BSSQ-Brace is not a comprehensive one; it is shorter and oriented toward the stress and feelings of the child treated with brace. It does not cover the full range of a child’s activities of daily life. 14 The BrQ has self-evident strengths as compared with these generic instruments by virtue of its increased sensitivity to the unique problems related to the brace itself. All the items of BrQ chosen were reported to be consistent with the need-based theory of quality of life. 8 The aim of this study was to investigate the Turkish adaptation of the BrQ as a new method in evaluating the quality of life of scoliotic individuals who are treated with a spinal orthosis.
Methods
The BrQ
The BrQ is a quality-of-life scale that was developed in 2006 by Vasiliadis et al. based on a patient series with scoliosis and contains items relating to brace use. It consists of 34 questions under eight specific domains: (1) general health perception: two questions; (2) physical functioning: seven questions; (3) emotional functioning: five questions; (4) self-esteem and esthetics: two questions; (5) vitality: two questions; (6) school activity: three questions; (7) body pain: six questions; and (8) social functioning: seven questions. The answers given to the questions (Likert-based) are categorized in the form of always, most of the time, sometimes, almost never, and never. All the topics were prepared based on the need to determine the health-related quality of life. The entire questionnaire is reported to take 10–12 min to complete. The minimum score is 20 and the maximum score is 100. Score calculation is as follows: always = 5, most of the time = 4, sometimes = 3, almost never = 2, and never = 1 for questions 4, 5, 6, 12, 14, 15, 16, and 17 and always = 1, most of the time = 2, sometimes = 3, almost never = 4, and never = 5 for questions 1, 2, 3, 7, 8, 9, 10, 11, 13, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, and 34. Each question has a value with the score being multiplied by 20 during score calculation. The final score is the total of all scores divided by 34. Additionally, scores for all eight domains can be calculated by taking the average of that particular section. High scores indicate a better quality of life.
The BrQ is important as it multidirectionally queries the effect of brace use on many parameters, is practical and easy to use, and measures brace-related quality of life. Vasiliadis et al. 8 found the BrQ to be valid, reliable, and effective in measuring the changes with brace treatment in the study they conducted on 28 individuals with adolescent IS (AIS).
Subjects
The study was conducted on 28 subjects (25 females and 3 males) with AIS with a mean age of 14.6 years (minimum 10 years, maximum 17 years) who were conservatively treated with a spinal orthosis. There was a right thoracic left lumbar curve in 13, right thoracolumbar curve in 10, right thoracic curve in 3, and left lumbar curve in 2 subjects. The inclusion criteria were diagnosis of IS; having used a spinal orthosis for 20–23 h/day for a minimum of 3 months; lack of congenital scoliosis or spinal deformity, or any neuromuscular, rheumatic, renal, cardiovascular, and pulmonary system disorder; lack of tumors anywhere in the body; lack of a history of spinal surgery; and voluntary participation in the study. The study was found to be appropriate in terms of medical ethics by the University Clinical Studies Ethics Committee. Informed signed consent was obtained from the individuals and their families.
The intercultural adaptation principles of Beaton et al. 15 were used for the translation process of the questionnaire. After the necessary written permissions were received from the authors of the BrQ, translation from English into Turkish was conducted by two different translators whose native language was Turkish. One of the translators was informed of the purpose of the study to prevent uncertain meanings emerging from the original questionnaire. The other translator did not receive this information. The two translations were compared to eliminate any inconsistency. Finally, the Turkish translations were back-translated into English by a translator whose mother language was English and who had no information on the study. The result was compared with the original questionnaire and reviewed for inconsistencies. No substantial differences in meaning were found between the translations.
The Turkish version of BrQ was administered to 15 healthy individuals in the pilot study before the questionnaire was finalized. The translation of each question was evaluated in terms of applicability and comprehensibility, and some minor changes were made for consistency.
The new version (the Turkish version of the BrQ is given as supplement) was administered to 28 individuals with AIS included in the main study following the pilot study. The study was conducted in two steps: first, the BrQ was translated to Turkish and the cultural adaptation performed; second, the statistical validity and reliability of the Turkish version of BrQ (internal consistency and test–retest reliability) had to be demonstrated. Validity is the degree to which a method correctly measures the relevant parameters. 16 We evaluated the relationship between the BrQ and the BSSQ-Brace and SRS-22 questionnaires to determine the validity of the BrQ in our study. Reliability is the degree to which a measurement method gives the same result without an error when repeated at two different times with no expectation of a change at constant conditions and in the same patient population. 17 The patients who had been using a spinal orthosis for minimum of 3 months completed the BrQ twice, with an interval of 5 days, to evaluate the test–retest reliability in our study. No treatment other than the orthosis was used for the patients for these 5 days.
Brace treatment method
The patients in this study used a spinal orthosis of symmetrical structure that was rigid and active and had been designed and produced specifically for each patient using a three-dimensional approach. The mechanism of action of the orthosis is to improve the sagittal plane deformity by pushing the pelvis upward, while actively correcting the lateral deviation and rotation of the spine, thus ensuring a symmetrical vertebral column posture. The characteristic of a thoracolumbar-sacral orthosis (TLSO) is its ability to provide symmetrical posture with the help of the three-dimensional active correction principle while the orthosis is preserving the original body shape. It is worn under the clothes and is not visible, to increase its use by the subjects. It allows the individual to move comfortably by not limiting the mobility of the body (flexion, lateral flexion, and rotation) or of the four extremities. 18
Other evaluation tools
The BSSQ-Brace and SRS-22 questionnaires, which are related to scoliosis-related quality of life and for which a Turkish validity study has been conducted previously, were used for the validity measurements of the BrQ scale and subscales.
SRS-22 is a simple and practical quality-of-life questionnaire created specifically for individuals with scoliosis. It consists of 22 questions including parameters of pain, self-image/appearance, function/activity, mental health, and satisfaction with treatment. Each question is scored between 1 (worst answer) and 5 (best answer). The total score expresses the average of these five domains. 13
BSSQ-Brace is a health-related quality-of-life scale querying psychological stress due to the brace. It is a reliable scale in the evaluation of the mental state of scoliotic individuals. The answer of each of the eight questions is scored between 0 (highest stress) and 3 (lowest stress). The highest total score of 24 indicates the lowest stress while 0–8 points is accepted as high stress, 9–16 points as moderate stress, and 17–24 points as low stress. 19
Statistical analysis
All analyses were conducted using the SPSS (version 15.00) statistical software program (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used for age, Cobb angle, and apical vertebral rotation variables of the individuals, and these were expressed as mean ± standard deviation. The critical significance level was determined as p < 0.05. Frequency was used for values regarding curve type. Mean ± standard deviation was calculated for the BrQ, BSSQ-Brace, and SRS-22 scale and subscale scores. The intraclass correlation coefficient (ICC) was used to evaluate the test–retest reliability of the BrQ. Although the ICC can vary between 0.00 and 1.00, an ICC of 0.60–0.80 indicates a good reliability, and scores more than 0.80 indicate excellent reliability. 17 The internal consistency of the questions was evaluated using Cronbach’s alpha coefficient. The internal consistency was accepted as very good if the coefficient was larger than 0.80. 20 Pearson’s correlation coefficient was calculated for validity using the BSSQ-Brace and SRS-22 tests. Moreover, the relationship between the BSSQ-Brace and SRS-22 questionnaires for two different items was evaluated with Pearson’s correlation coefficient. The validity coefficient was considered excellent for 0.81–1.0, very good for 0.61–0.80, good for 0.41–0.60, adequate for 0.21–0.40, and weak for 0–0.21. 16
Results
Information on the age, Cobb angle, apical vertebral rotation degree, daily brace use duration, brace treatment duration, and BSSQ-Brace and SRS-22 scores is presented in Table 1. The mean BSSQ-Brace score showed that the individuals had a moderate level of stress related to the spinal orthosis. The SRS-22 total score indicated that the individuals had a good quality of life. Table 2 presents the total BrQ score, domain scores, and individual scores for the questions.
Descriptive statistics for age, Cobb angle, AVR, brace wearing time, BSSQ-Brace, and domain descriptions for SRS-22 questionnaire.
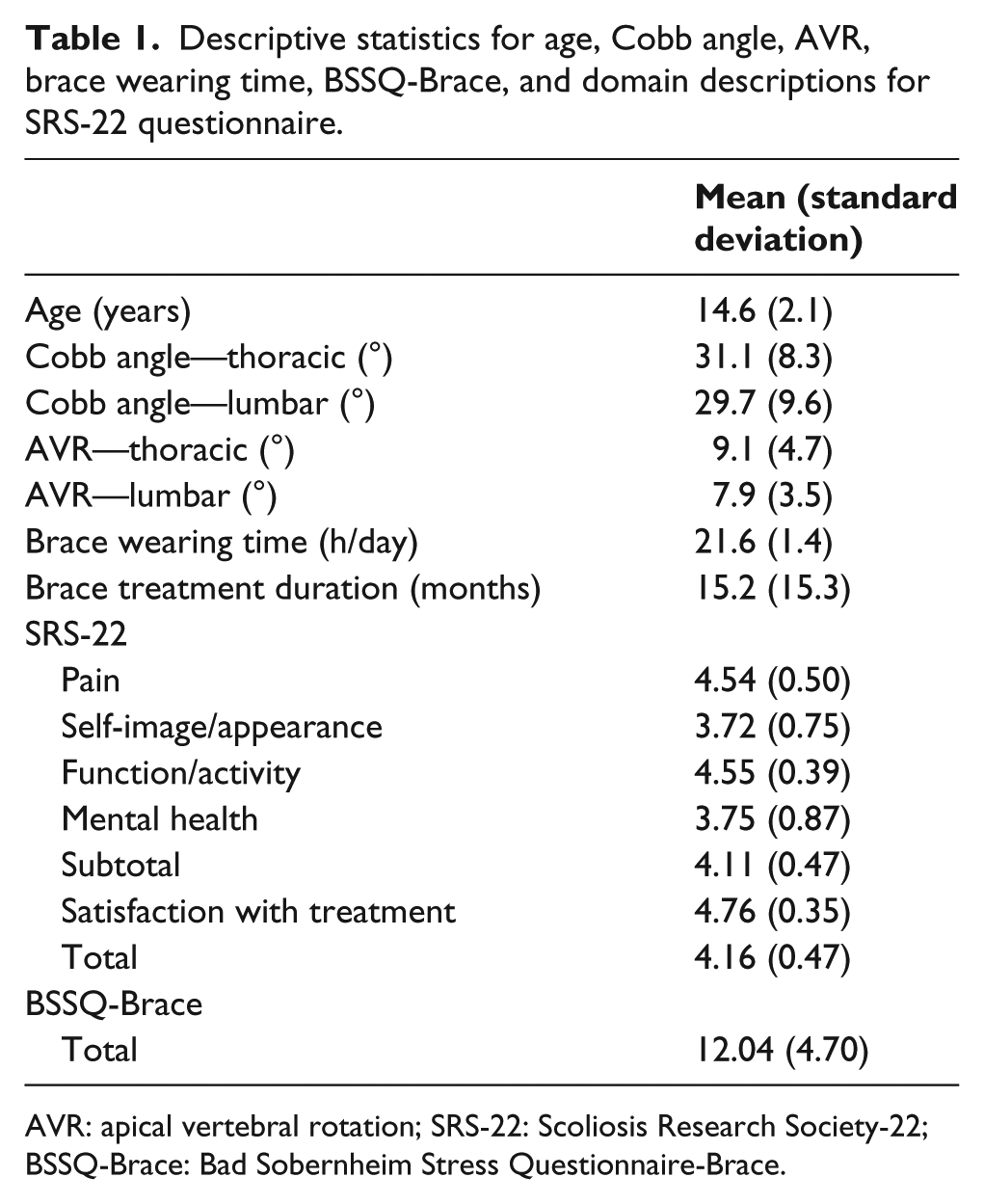
AVR: apical vertebral rotation; SRS-22: Scoliosis Research Society-22; BSSQ-Brace: Bad Sobernheim Stress Questionnaire-Brace.
Overall test and retest scores of patients for each domain, each item, and total BrQ.
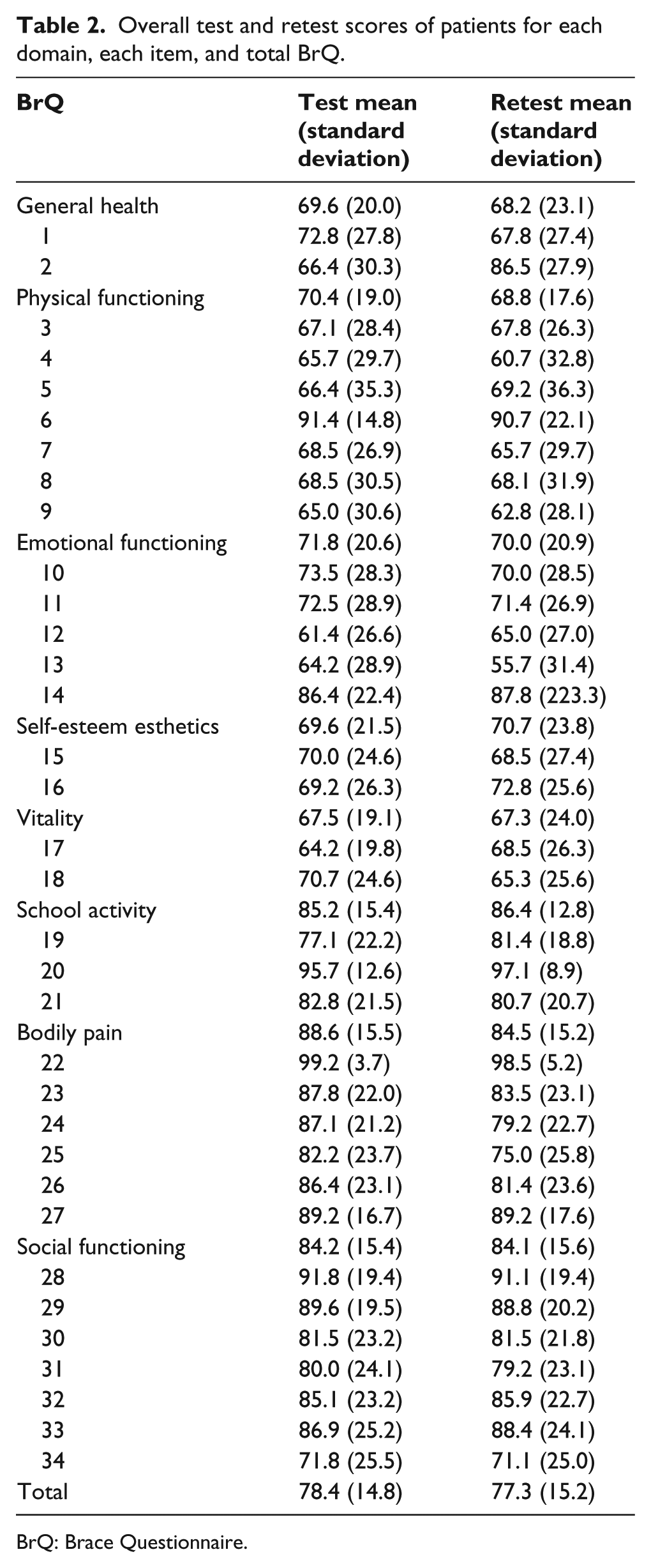
BrQ: Brace Questionnaire.
Test–retest reliability for the BrQ total score was identified as excellent (ICC = 0.95, 95% confidence interval: 0.900–0.984). Calculations of Cronbach’s alpha coefficient for the first and second administrations of the BrQ were both 0.94, indicating very good internal consistency. Test–retest reliability results of the BrQ domains are presented in Table 3 and varied between good and excellent.
Test–retest reliability results of BrQ and its domains.
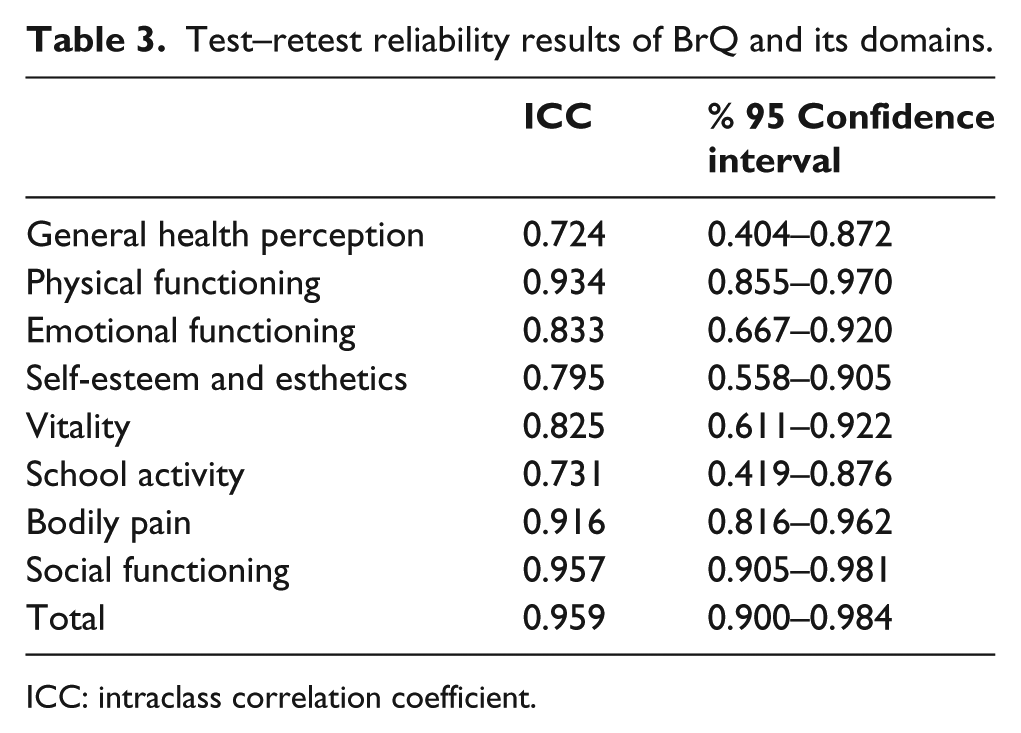
ICC: intraclass correlation coefficient.
The correlation between the overall score of each domain and the average score of each question considered to the part of the domain in BRQ is presented in Table 4. The relationship between the BrQ domains and the relevant questions varied between adequate and excellent (r = 0.28–0.95).
The relation between each domain of the BrQ and each items of the domain.
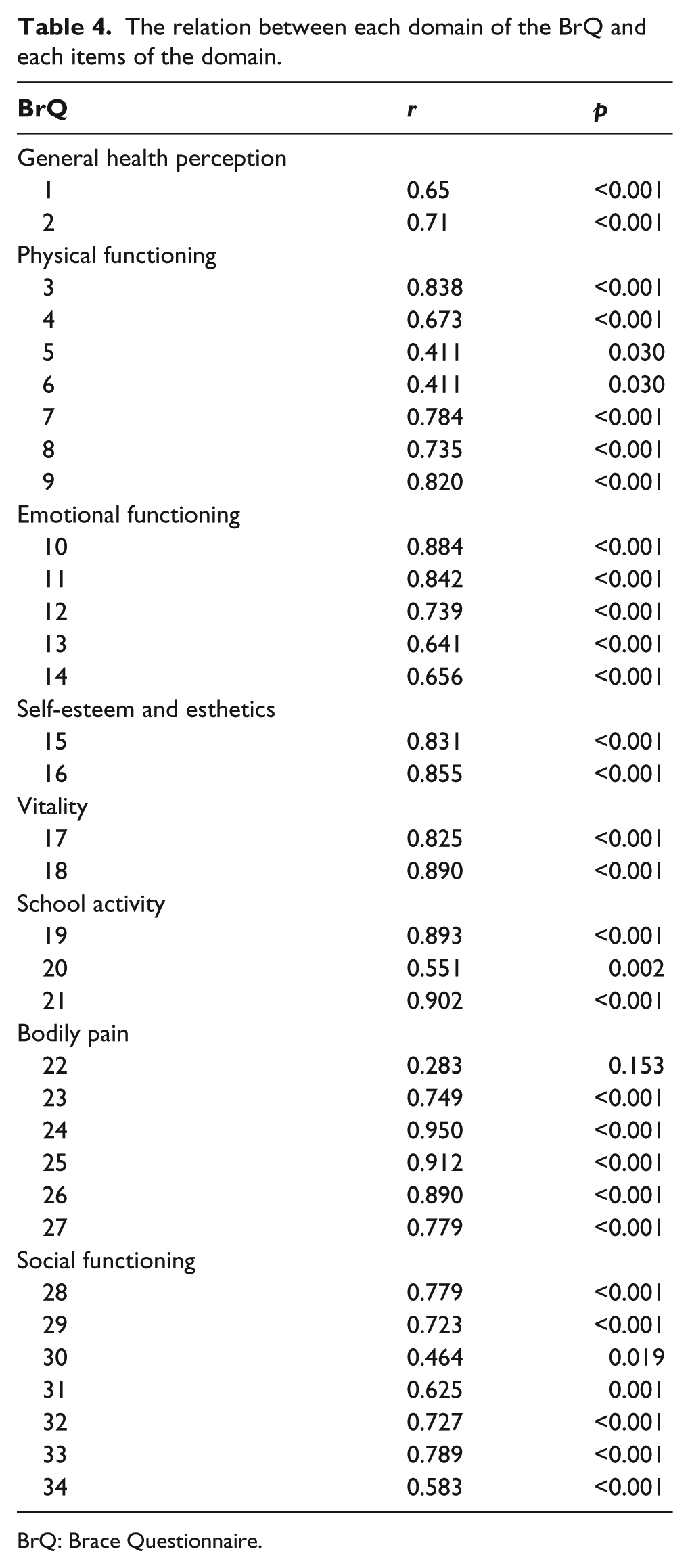
BrQ: Brace Questionnaire.
The BrQ total score showed very good correlations with the BSSQ-Brace (r = 0.67, p = 0.000) and SRS-22 (r = 0.64, p = 0.001) questionnaires. This result indicates that the BrQ has a very high degree of validity.
The relationship between the similar domains of the BrQ and SRS-22 questionnaire was also investigated in the study. An adequate level of correlation was found between physical function scores and the appearance-esthetic perception scores. A better correlation than the other two parameters was observed with the presence of a very good relationship between the mental health (emotional function) scores. A very good relationship was also present between the total scores of the two questionnaires (Table 5).
The relation between similar domains of SRS-22 and BrQ.
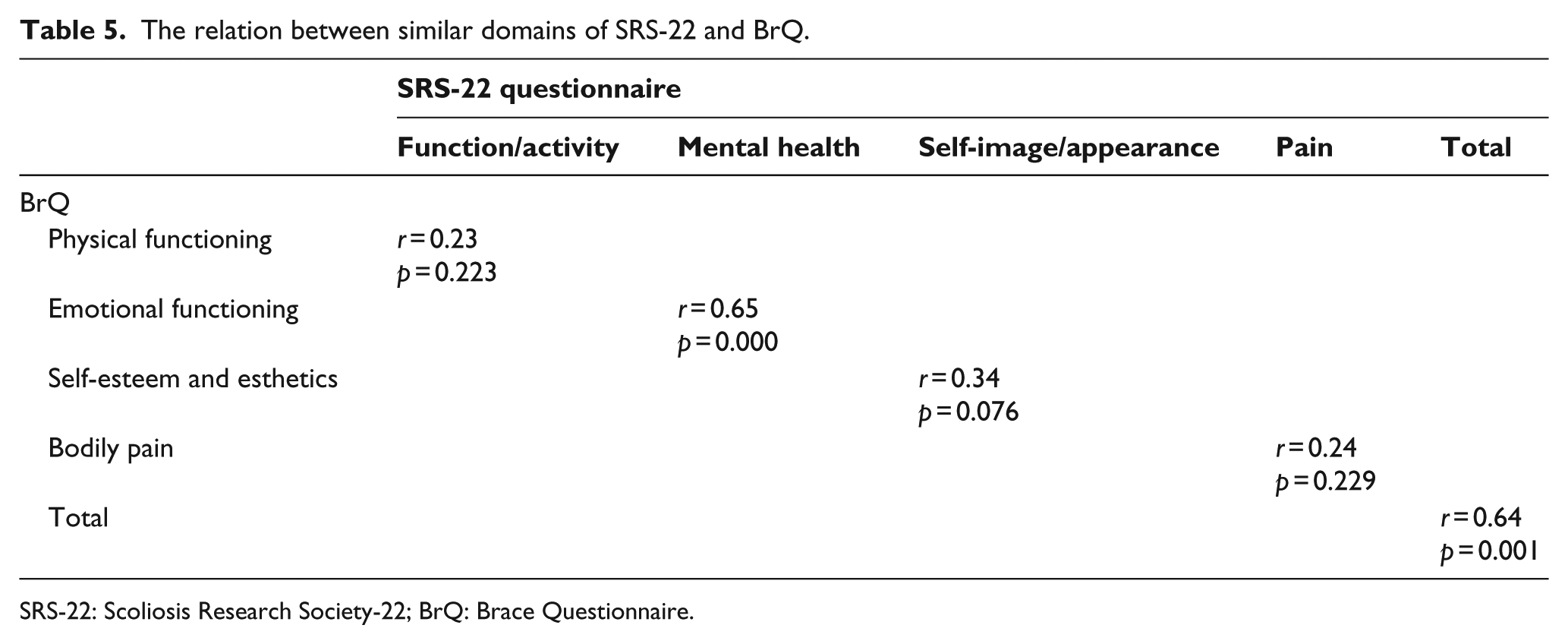
SRS-22: Scoliosis Research Society-22; BrQ: Brace Questionnaire.
Discussion
Considering Turkish socio-cultural conditions, this study demonstrated that the BrQ was highly reliable and valid in individuals with AIS using spinal orthoses. Our results are comparable with previous studies using the original Greek version and English, 8 Polish, 9 Italian, 10 French, 11 and Chinese cultural adaptations of the BrQ.
The BrQ has been developed for individuals with AIS who are conservatively treated with a brace and aims to evaluate the quality of life due to brace use. The developers have reported that it shows lower scores in moderate and severe scoliosis than in mild scoliosis. It has also been reported to be sensitive in showing changes over time because it measures the increase or decrease in the quality of life according to an improvement or deterioration of the spinal curve. 8
AIS itself is a factor that negatively affects body image, lifestyle, and behavior. 21 The spinal orthosis also creates a stressful experience by affecting the body appearance perception of the individual, relationships with other individuals, and quality of life.12,22 Additionally, orthosis use can cause pain and the applied corrective forces can create pressure discomfort. 23 Quality of life has been reported to change according the severity of the scoliosis, the skeletal maturation level, orthosis treatment duration and the amount of correction. 24 Rivett et al. compared brace use compliance and quality of life assessed by the BrQ and found weak compliance with brace use to be associated with lower quality of life. They reported that quality of life with AIS was related to psychosocial coping mechanisms rather than the physical deformity itself. They also emphasized the importance of family participation in the treatment together with the scoliotic individual in increasing compliance and improving quality of life. 25 It is important for the clinician to be informed of the brace-related factors that influence the patient’s quality of life in this regard.
The BrQ has been adapted into five languages: English, 8 Polish, 9 Italian, 10 French, 11 and Chinese. 12 Kinel et al. 9 reported the Polish adaptation of the BrQ to be reliable and valid and its internal consistency to be high in their evaluation of the brace-related quality oflife in 35 individuals with AIS with a mean Cobb angle of 35.1° ± 10.6° (Cronbach’s alpha = 0.94). Considering Turkish socio-cultural conditions, the reliability (ICC = 0.95) and internal consistency (Cronbach’s alpha = 0.97) of the BrQ were found to be excellent in our study where we prepared and used the Turkish adaptation of the questionnaire. Aulisa et al. 10 conducted the translation of the BrQ from the Greek original version to Italian and found the Italian version to be valid and reliable (r = 0.88; p < 0.001, Cronbach’s alpha = 0.86). They reported the BrQ to show a high degree of correlation with the SRS-22 questionnaire (r = 0.826; p < 0.001). They also reported the individual comparisons of the subsections of the BrQ with the parameters of SRS-22 to show a high degree of correlation. 10 Such high correlation of the BrQ with the BSSQ-Brace and SRS-22 indicates that it has a high degree of validity.
Our study supported the use of BrQ for clinical and research purposes with its easy applicability, time, and cost effectiveness in AIS patients who have brace treatment. However, there was a limitation in this study. The sensitivity of the BrQ to change could have been evaluated. Future research shall assess the responsiveness of the Turkish version of the BrQ to examine its ability to detect important changes in brace-related quality of life over time.
Conclusion
The BrQ is a valid and reliable questionnaire that queries brace-related quality of life in individuals with AIS who use a spinal brace and investigates functions such as general health perception, physical function, emotional function, self-esteem and esthetics, vitality, school activity, body pain, and social function. We recommend routine use of the BrQ in all scoliosis patients to evaluate brace-related quality of life and relevant factors and to support the individual when necessary during such treatment. We believe this approach will increase brace compliance to ensure successful treatment.
Supplemental Material
Turkish_BrQ – Supplemental material for The Turkish version of the Brace Questionnaire in brace-treated adolescents with idiopathic scoliosis
Supplemental material, Turkish_BrQ for The Turkish version of the Brace Questionnaire in brace-treated adolescents with idiopathic scoliosis by Gözde Gür, Yavuz Yakut and Theo Grivas in Prosthetics and Orthotics International
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.