
Abstract
Background:
Many individuals with lower limb loss report concern with walking ability after completing structured traditional rehabilitation.
Objectives:
The purpose of this study was to explore the impact of a supervised community–based exercise program on balance, balance confidence, and gait in individuals with lower limb amputation.
Study design:
Repeated measures.
Methods:
The supervised exercise program was offered biweekly for 6 weeks. The GAITRite System by CIR Systems, Inc., the Figure-of-8 Walk Test, and Activity-specific Balance Confidence Scale were used to measure clinical outcomes pre- and post-intervention.
Results:
In total, 16 participants with lower limb amputation (mean age: 50.8 years) completed the study. A multivariate, repeated measures analysis of variance indicated a statistically significant effect of training across six clinical outcome measures (F(6, 10) = 4.514, p = .018). Moderate effect sizes were found for the Figure-of-8 Walk Test (η2 = .586), Activity-specific Balance Confidence Scale (η2 = .504), and gait velocity at comfortable walking speed (η2 = .574). The average increase in gait speed was clinically meaningful at .14 m/s.
Conclusion:
The supervised community–based exercise program implemented in this study was designed to address specific functional needs for individuals with lower limb loss. Each participant experienced clinically meaningful improvements in balance, balance confidence, and walking ability.
Clinical relevance
The provision of a supervised community–based exercise program, after traditional rehabilitation, provides opportunity to offer a continuum of care that may enhance prosthetic functional ability and active participation in the community for individuals with lower limb amputation.
Keywords
Background
There are 1.9 million Americans living with the loss of a limb, and this number is expected to double by 2050. 1 The number of people who incur lower limb amputation (LLA) rises annually owing to, among other factors, an increasing number of older adults and a higher incidence of diabetes and dysvascular conditions. 2 The impact of LLA on walking ability and community engagement is significant, irrespective of the result of disease or traumatic accident. Even after completing a rehabilitation program with prosthetic training, many individuals with limb loss continue to express concerns of decreased strength and coordination of residual limb muscles, altered balance, fear of falling, reduced cardiovascular endurance, and diminished walking ability in the community.3–5
Regaining balance is fundamental for functional training, as individuals with LLA must learn new motor coordination and balance strategies to successfully walk with a prosthesis.6–8 Specifically, amputation of the lower limb results in diminished proprioceptive input from the ankle and/or knee and a modified center of mass, which requires trust in use of a prosthetic limb for balance and gait control. In addition, fear of falling may lead some individuals with amputation to assume a sedentary lifestyle and decrease active participation in the community. Self-reported number of falls per year for those with unilateral LLA is greater than the annual incidence rates of falls among community-dwelling elderly: 52% as compared with 30%, respectively. 4 Low balance confidence, in persons with amputation, has been shown to be directly associated with the need for an assistive device with walking, 8 while better balance was found to be predictive of increased participation in the community. 9
Individuals with LLA also present with unique issues secondary to prosthesis use that challenge rehabilitation efforts in promoting optimal long-term functional outcomes. Successful prosthetic ambulation in the community, for example, is dependent upon having sufficient physical capacity, including aerobic capacity, muscular force, balance, and flexibility.9,10 Van Velzen et al. 10 found that the percentage of individuals with LLA who were able to regain community walking ability varied (56%–97%) and more than 80% needed an additional walking aid for safety. Research further suggests that the optimal goal of training for preventing falls in individuals with LLA is to promote a “functional gait” using a prosthesis as close to normal a gait pattern as possible.8,9
A major objective of Healthy People 2020, a 10-year agenda of the US government to improve the health of Americans (https://www.healthypeople.gov/2020/About-Healthy-People), is to promote regular participation in exercise and physical activity for health maintenance. Research, however, illustrates that people with disabilities are less likely to participate in physical activity due to physical, emotional, and psychological barriers, inaccessibility of facilities, and lack of staff trained in working with people with disabilities.11–13 In persons with LLA, restrictions in participation are commonly reported in activities such as sports/physical recreation, leisure/cultural activity, and employment/job seeking and are most often attributed to environmental barriers and a lack of accessible exercise programs.14–15 The increasing number of individuals living with LLA warrants exploration of optimal health care programs that can enhance physical fitness and health promotion across the lifespan.
While there are numerous studies on the positive effects of exercise training on balance and gait in able-bodied individuals,16,17 to our knowledge, there is little to no current literature exploring the impact of community-based exercise programs designed specifically for individuals with LLA. The purpose of this exploratory study was to discover the impact of a supervised community–based group exercise program on balance, balance confidence, and gait ability for individuals with LLA.
Methods
A convenience sample of males and females older than 18 years of age, who were no longer engaged in structured rehabilitation, were recruited from a private-practice prosthetic clinic. Inclusion criteria for the study were community-dwelling adults with LLA, proper fit of a prosthesis as determined by the referring prosthetists, independent bipedal ambulation with or without an additional assistive device, and ability to read/write in English. Each participant completed the Physical Activity Readiness Questionnaire (PAR-Q), which screened for potential medical complications associated with exercise. When PAR-Q results indicated the participant may be at risk, he or she was asked to seek medical clearance for exercise from a physician prior to participation. Individuals with health conditions deemed unsafe for exercise, such as uncontrolled cardiovascular diseases, diabetes, stroke, and unstable bipedal ambulation, were excluded. This study was approved by the University of North Georgia Institutional Review Board.
Clinical outcome measures
The Figure-of-8 Walk Test (F8W), used to measure gait skill and dynamic balance, is based upon three measures: time for completion, amplitude (number of steps taken), and smoothness (hesitancy, stopping, or changing pace). The F8W involves alternating walking in straight and curved paths in a confined space, which requires continual adjustment in weight shifting and movement control. 18 Smoothness is recorded as 0 or 1 for each component; 1 point is given for no hesitancy (extraneous movement to adjust position to complete curve about marker, no stopping during test, and consistent pace for entire walk pattern). The F8W test is considered a valid measure of daily walking skills and provides indirect information about gait speed, a standard measure of safe community ambulation. 18
The Activity-specific Balance Confidence (ABC) Scale 19 was used to rate balance confidence, on a scale from 0% to 100% while performing various ambulatory activities. An averaged sum score of 50% or less describes a low level of physical function, 50%–80% describes a moderate level of physical function, and scores 80% or higher describe a high level of physical function. 20 The ABC Scale yields strong test–retest reliability in older adults (r = .92) and in persons with LLA (r = .91). 20
Spatial–temporal parameters of ambulation were assessed using GAITRite (GAITRite® Gold; CIR Systems, Havertown, PA, USA), an electronic portable walkway. 21 In healthy participants, GAITRite measurements yield intraclass correlation coefficient (ICC) values between .80 and .92 at preferred walking speeds and between .79 and .89 at fast walking speeds (FWS). 22 The GAITRite Functional Ambulation Performance (FAP) scoring system 23 comprises the linear relationship of step length/leg length ratio to step time when the velocity is “normalized” to leg length. In healthy adults, FAP scores range from 95 to100 points and have an inter-rater reliability of ⩾.99. 24 Normative data for individuals with LLA are not reported in the literature.
Procedures
Participants provided informed consent and demographic data, and they completed the ABC survey at the initial session. Baseline vital sign measurements, blood pressure (BP), heart rate (HR), and rate of perceived exertion (RPE) were measured at rest. Maximum exercise HR was calculated as 220 minus participant’s age. Target HR for moderate intensity level exercise was established as 60%–80% of the participant’s predicted maximum HR.
During balance and gait testing, participants were guarded by the researchers as needed for safety. For the F8W test, time to complete, amplitude (number of steps), and smoothness were recorded. Participants were instructed to complete the test as quickly as possible; use of assistive device was recorded. Two trials were conducted; the first trial began with the prosthetic side on the inside pass of the figure-8 pattern and a second trial started with the non-prosthetic side on the inside. Two walking speeds were collected using the GAITRite—comfortable walking speed (CWS) and FWS. The participants’ height, weight, and leg length were measured and entered into the software to allow for FAP calculation. The use of assistive device was also recorded. For CWS, participants were instructed to walk at a comfortable pace similar to that used when walking at home or in a hallway. Following a 2-min rest period, participants were instructed to walk at his or her fastest pace possible (FWS), without increasing his or her perceived risk or fear of falling. Two sequential trials were collected at each speed.
At study completion, the participants were tested with the same procedures as in the pre-test. A post-study assessment survey was included to allow the participants opportunity to evaluate the quality of the program.
The 6-week intervention program
Participants were placed into one of two exercise groups: transfemoral (TF) or transtibial (TT); the individual with TF plus TT LLA was placed in the TF group. The supervised exercise program met 1 h twice a week for 6 weeks. The exercise program (Table 1) focused on stretching, core (trunk) and lower extremity strength and flexibility exercise, and static and dynamic balance and gait activities (Figures 1–3). Exercise modifications and increased supervision were provided for participants in the TF group to prevent prosthetic knee instability. The initial resistance level for lower extremity strengthening with elastic resistance bands was determined using a 10-repetition max test at pre-test. The participant was required to stretch the band two times the resting length and complete 10 repetitions with moderate difficulty (Figure 4). Re-assessment of level of resistance, speed of movement, and number of repetitions for all exercises was done weekly, and the resistance and/or intensity was increased accordingly. During each session, the participants were also monitored for RPE, BP, and HR to ensure that he or she was exercising within a physiologically advantageous zone for moderate intensity training. Researchers assisted participants in the performance of exercises and provided guarding for safety during all activities as needed.
Supervised community–based exercise program.
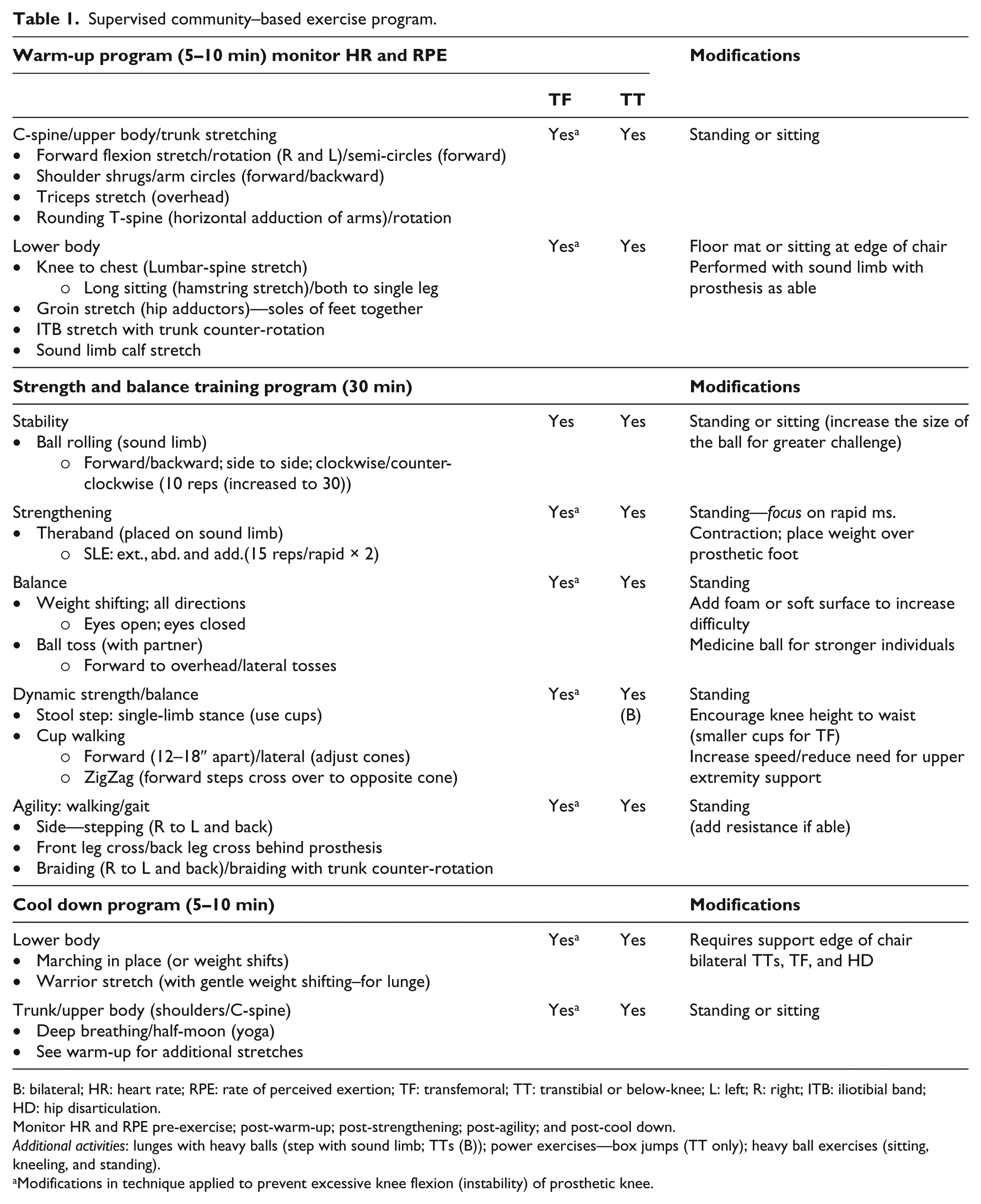
B: bilateral; HR: heart rate; RPE: rate of perceived exertion; TF: transfemoral; TT: transtibial or below-knee; L: left; R: right; ITB: iliotibial band; HD: hip disarticulation.
Monitor HR and RPE pre-exercise; post-warm-up; post-strengthening; post-agility; and post-cool down.
Additional activities: lunges with heavy balls (step with sound limb; TTs (B)); power exercises—box jumps (TT only); heavy ball exercises (sitting, kneeling, and standing).
Modifications in technique applied to prevent excessive knee flexion (instability) of prosthetic knee.

Ball rolling exercise: the sound limb is placed (non-prosthetic) on top of the ball and will rapidly roll the ball in multiple directions while increasing body weight shift over the prosthetic limb.
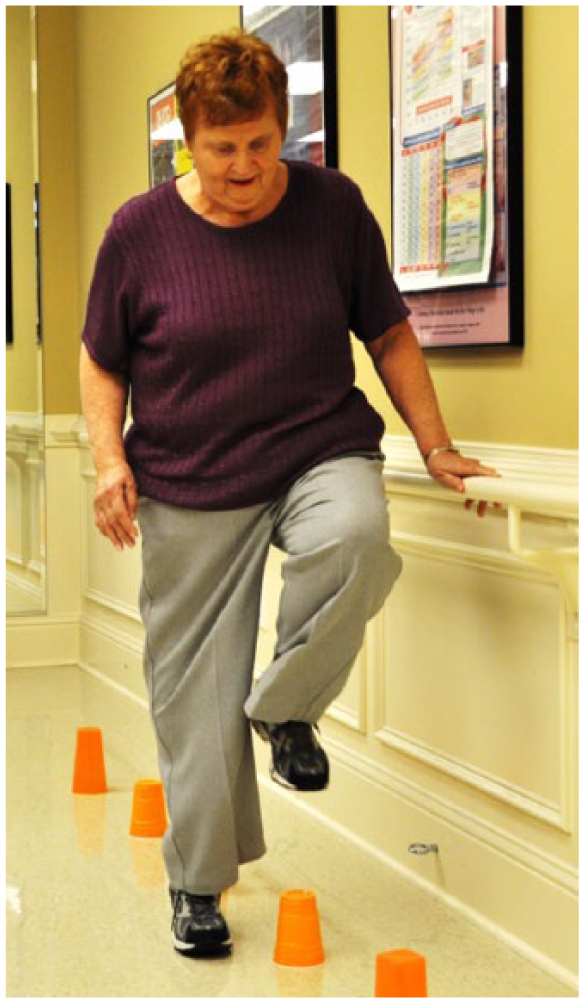
Cup walking exercise: for TT participant, activity may be completed foot-over-foot; TF will step over with sound limb only and progress prosthetic limb up to cup to prevent knee instability.

Dynamic balance and gait activity: participant performs cross-over steps between cones (TT prosthetic limb is behind).

Strengthening exercise with Theraband on prosthetic side (also performed on sound limb).
Statistical analysis
All data were analyzed using SPSS version 23.0 for Windows (SPSS, Chicago, IL, USA). Scores from outcome measures were included in data analysis only for those participants who completed testing and did not miss more than two exercise sessions during the 6-week intervention program. Data from the GAITRite for the two trial walks at each speed were combined during data reduction using the program software version 4.0; averaged scores were then entered into the SPSS database. For the purpose of statistical analysis, only the TF data were entered as the prosthetic side for the one individual with TF and TT amputation. Additionally, the left side was randomly chosen as the prosthetic side for data analysis for the participant with bilateral TT amputation.
Clinical data were also collected on multiple variables as there is no previous literature to suggest the potential effect size or sample size required for this type of intervention program; therefore, descriptive statistics were examined for all variables. A repeated measures analysis of variance (RM-ANOVA) was calculated to test the hypotheses that a supervised community–based program would improve gait, balance, and balance confidence. The variables included gait velocity at CWS, FAP score, time to complete and number of steps taken during the F8W test, and ABC total score.
Results
A total of 16 participants completed this study. Demographic, amputation-related factors, and type of assistive devices used are presented in Table 2. The mean age of participants was 50.8 (range: 22–87) years; 68.8% were female and 31.2% were male; and 87.5% had unilateral amputation and 12.5% had bilateral amputation. The mean number of years since LLA was 8 years and the mean number of hours the prosthesis was worn per day was 10.4 h.
Demographic and physical characteristics of the sample (N = 16).
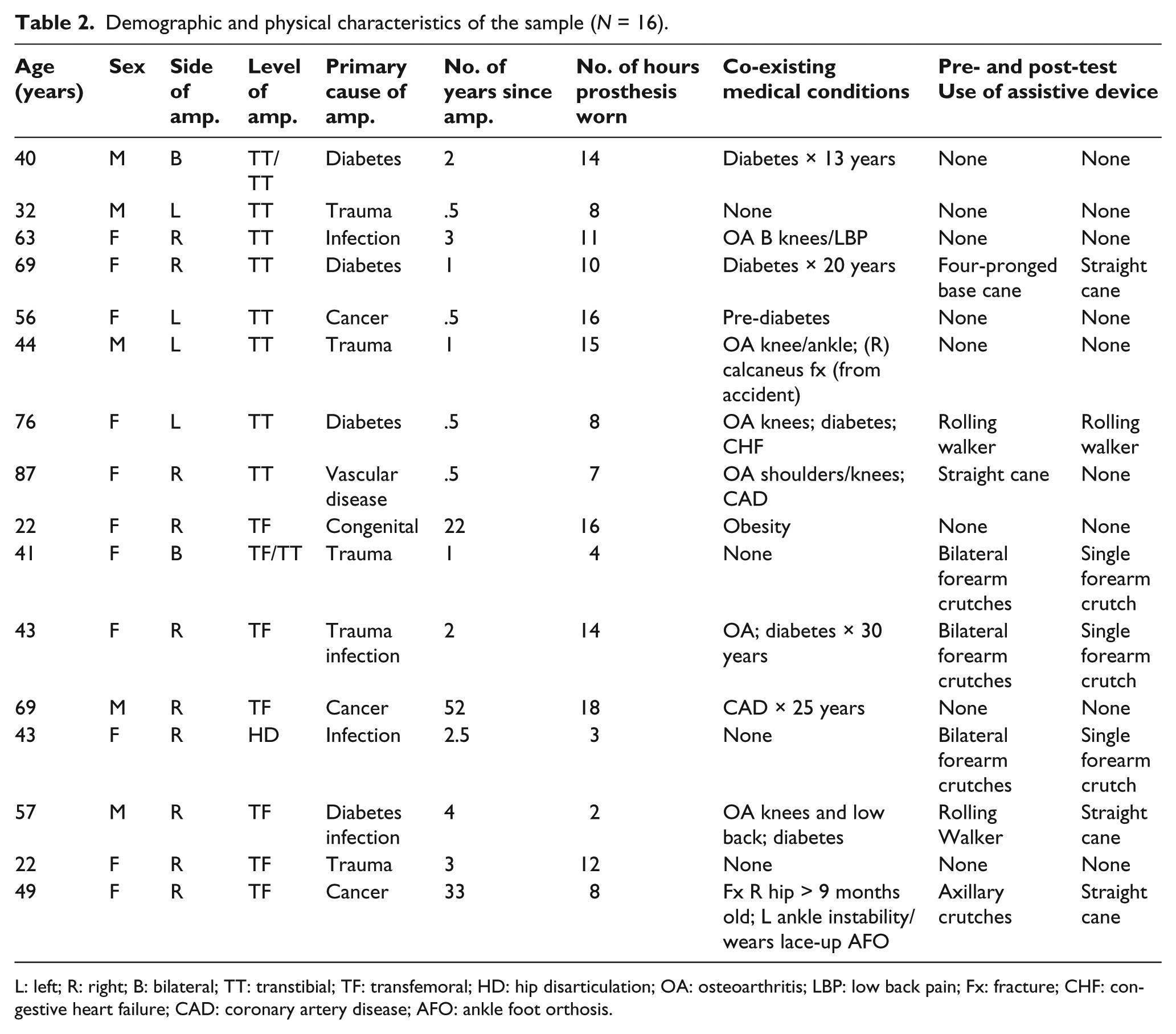
L: left; R: right; B: bilateral; TT: transtibial; TF: transfemoral; HD: hip disarticulation; OA: osteoarthritis; LBP: low back pain; Fx: fracture; CHF: congestive heart failure; CAD: coronary artery disease; AFO: ankle foot orthosis.
Results of the total model summary of the RM-ANOVA for the six variables entered was statistically significant (F(6, 10) = 4.514, p = .018). Table 3 presents effect size and calculated power for the six test variables. The F8W test results illustrated decreases in time to complete and amplitude, reflecting an increase in dynamic balance. Mean scores for time to complete and amplitude did not yield a significant difference in time when starting from the prosthetic versus non-prosthetic side; therefore, scores were averaged for these variables. The assessment of smoothness was included in data analysis; however, comparisons were difficult to interpret due to a change in type of assistive device (decreased use of) from pre- to post-test.
Clinical outcome results—RM-ANOVA (effect size and power).
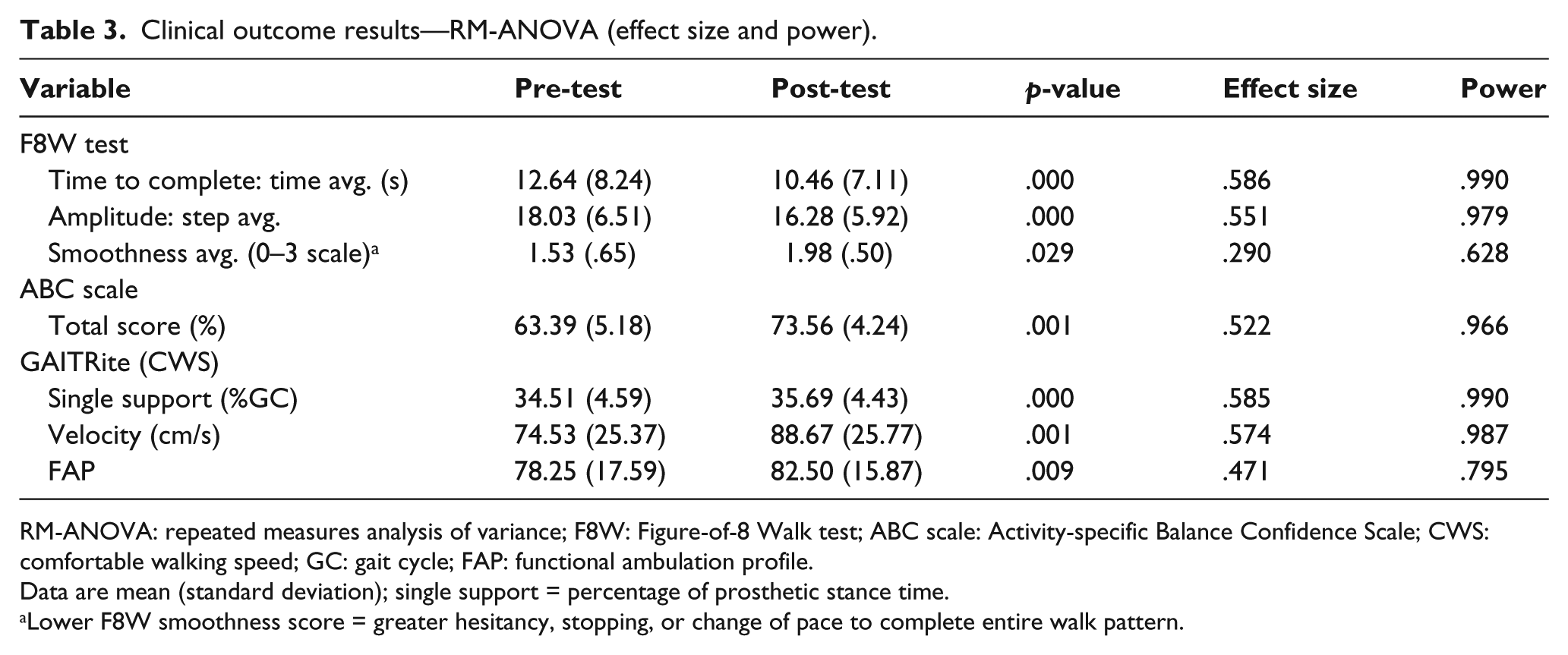
RM-ANOVA: repeated measures analysis of variance; F8W: Figure-of-8 Walk test; ABC scale: Activity-specific Balance Confidence Scale; CWS: comfortable walking speed; GC: gait cycle; FAP: functional ambulation profile.
Data are mean (standard deviation); single support = percentage of prosthetic stance time.
Lower F8W smoothness score = greater hesitancy, stopping, or change of pace to complete entire walk pattern.
Results of the ABC scale revealed an increase in the total group mean score from 63.4% to 73.7%. At completion of the study, balance confidence was noted to be higher in the TT group than in the TF group, 76.1% and 71.3%, respectively. In 37.5% of total participants, the ABC mean score increased by greater than 10%; two participants had a 5% decrease in mean score for balance confidence; one TF participant noted on the survey that she had experienced a fall one week prior to post-testing and was “more concerned about falling.” Only 25% of the total group at pre-test and 31% at post-test achieved an average score of 80% or higher, indicative of high-level physical function.
Additional GAITRite spatial–temporal parameters assessed included velocity, cadence, prosthetic and non-prosthetic step length, stride length, single-limb support, and FAP (Table 4). During CWS at post-test, the average velocity for all 16 participants increased by .14 m/s; average velocity increased by .17 m/s for the TT group and .13 m/s for the TF group. FWS also revealed mean score increases in velocity, cadence, prosthetic and non-prosthetic stride length, and in prosthetic and non-prosthetic single-limb support. Only CWS is described for functional ambulation, as this self-selected speed is more closely correlated with typical walking ability and correlates with the FAP. 25
Clinical outcome results—additional GAITRite parameters.
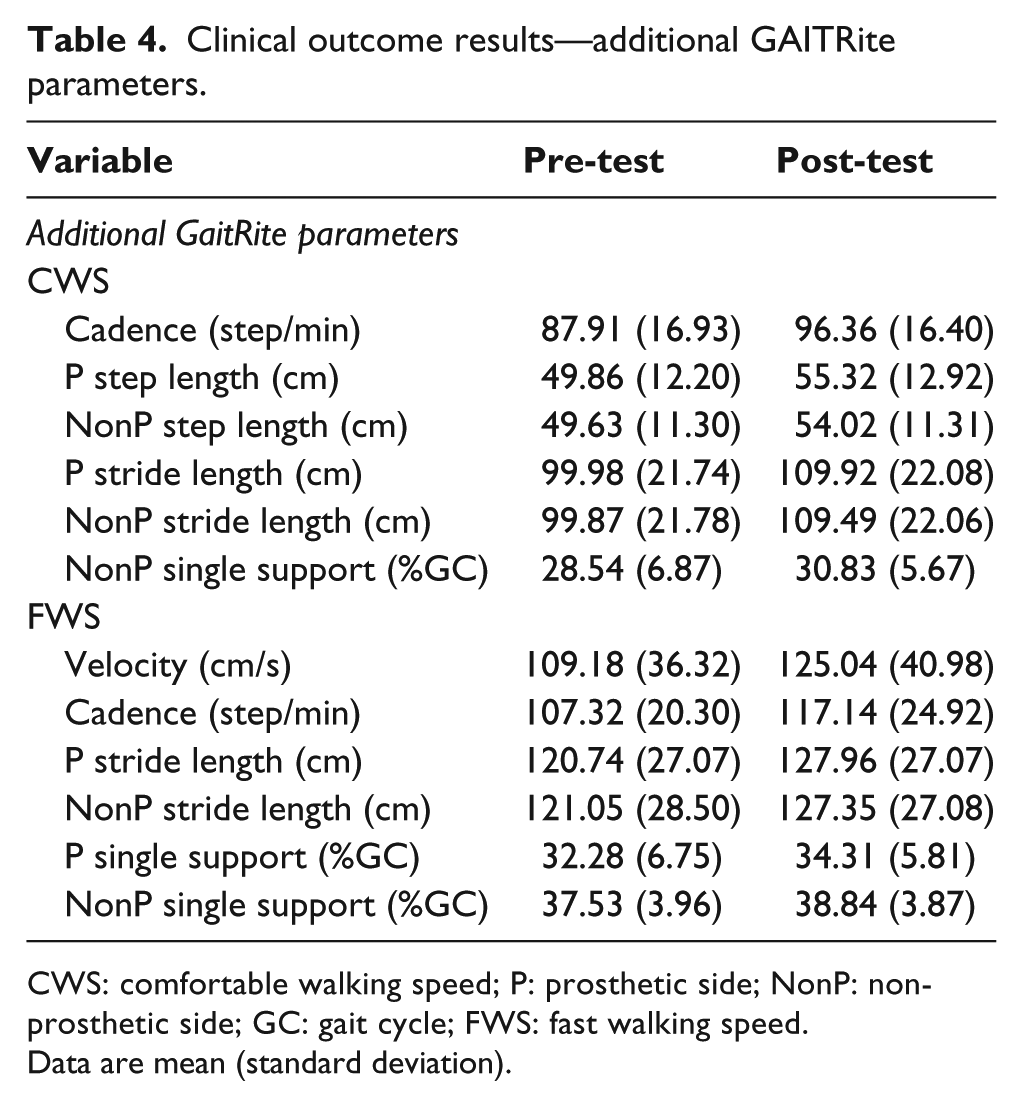
CWS: comfortable walking speed; P: prosthetic side; NonP: non-prosthetic side; GC: gait cycle; FWS: fast walking speed.
Data are mean (standard deviation).
Discussion
Following in-patient rehabilitation, individuals with LLA typically receive limited physical therapy sessions with most therapy models in the United States suggesting a prosthetic gait training period of 2–6 weeks. 26 Afterward, some individuals with limb loss have expressed concerns about continuing exercising without monitoring and/or supervision, mostly because some do not have access to, or knowledge of, safe exercise to perform in the community or local gym.5,7,25 With these concerns in mind, the 6-week intervention program created for this study focused on addressing amputee-specific needs in static and dynamic balance, strength training, and gait activities—all of the exercises were designed to enhance prosthetic trust (stance time) and walking ability.
For individuals with LLA, placing full weight on the prosthesis can be a very fearful event. If prosthetic trust (knowing one’s prosthesis will support him or her) is not achieved, an individual may walk at a slower speed thereby decreasing overall functional ambulation.27,28 The lower extremity strengthening program (ball rolling and Theraband) sought to increase prosthetic trust by enhancing muscular strength, proprioception, and dynamic control. The GaitRite results for single-limb prosthetic stance time increased for all individuals, which were indicative of improvement in the ability to maintain standing static posture on the prosthetic limb.
Dynamic balance, or the ability to maintain one’s center of mass over the base of support when changing directions, is another pivotal factor in maintaining overall functional ambulation. 27 Meaningful clinical changes were noted in the F8W test with increased smoothness, fewer steps, and faster time to complete. The inclusion of prosthetic specific dynamic standing and stepping exercises in this intervention program contributed to these findings. Lower extremity Theraband resistance exercises, which were progressed to high-repetition rapid motion and ball tossing standing on foam platforms, may have contributed to enhanced dynamic balance. Dynamic movement (rapid alternating motions) of the sound limb also encouraged increased prosthetic limb stance demands during cup-walking, as cups were placed for participants to step over in varied directions. At program completion, many participants were able to perform dynamic exercises without arm support or with only finger-tip support on a railing.
Balance confidence, as per the ABC, improved in the TT group (14.3%) and TF group (18.7%). Older participants reported lower confidence than younger, and the lowest ABC score was reported by one individual with bilateral amputation. Initially, only three participants had an ABC score <50%, indicative of confidence with lower level functional tasks, such as walking around the house. At completion of the program, all the participants’ scores were >50%, reflecting increased confidence with moderate activity level, such as walking outdoors or up/down a ramp, while 37.5% in the TT group and 25% in the TF group were more confident with higher level activity, including walking in crowded areas in the community. Increased balance confidence alone may have contributed to improvements noted in specific balance and gait outcome measures.
Gait speed has been shown to be the sixth vital sign and is a known indicator of functional ability and balance. 29 A change in velocity of .1 m/s is a clinically meaningful difference for normal walking speed in older adults and is a useful predictor of higher levels of functional performance and well-being. 30 In this study, the quality of gait (step length and stance time) and gait speed improved as participants became more effective in the ability to perform the exercises in a smooth and controlled manner. Overall, 94% of our participants increased in CWS and FWS; only two participants (both TT level) reached normative, able-bodied, values of 1.2–1.4 m/s. 29 While all participants improved in their FAP gait scores, only three individuals with TT amputation reached normative ranges for healthy adults.
The positive changes made in balance and gait ability may have contributed to finding 43% of participants were able to reduce their use of an assistive device/s by completion. Several of the TT participants became increasingly successful in performing dynamic activities without upper extremity support and others jogged for the first time since amputation. One participant, who had amputation secondary to congenital limb deformity and previously had no fear of falling, experienced her first fall in several years while “doing more,” which impacted her ABC score and post-test gait velocity. Those who had always used an assistive device reported being able to “move better” after the program.
Another unanticipated finding was the amount of body weight loss and change in residual limb size and shape experienced during the study. Of the 16 participants, 63% in the TT group and 50% in the TF group needed new sockets within the 6-week intervention. Those who reported weight loss also experienced a decline in socket fit/comfort with a resultant decrease in prosthetic control. Several participants wore as many as 12 ply socks in order to achieve a comfortable socket fit while continuing to participate in exercise. The prosthetic clinic partners were able to provide three of the nine with a temporary check-socket to complete the study. Future programs should consider clinically measuring weight loss and residual limb change to ensure optimal prosthetic comfort/fit for individuals interested in participating in increased physical activity and exercise.
Limitations of this study included sample size and lack of control group, length of exercise program, and monitoring of residual limb shape and size. An exercise program of 6 weeks allows for opportunity for neural change; however, it may not be long enough for true physiological change. According to Chin et al., 30 older individuals with limb loss who can sustain an exercise intensity of ⩾50% of VO2max are more often successful prosthetic users. Extending a program such as this from 1 to 12 weeks may promote greater changes in strength and physical fitness, potentially promoting a stronger effect on balance and walking ability. Future researchers might also consider measuring balance using more sensitive measures, such as a Biodex Balance System, Timed-up and Go, or Berg Balance Test.
Conclusion
Supervised community–based exercise programs may provide opportunity for clinicians to offer a continuum of care that enhances prosthetic functional ability and active participation in the community for individuals with LLA. While this study had a limited number of participants with LLA, improvement was found in balance, balance confidence, and various gait parameters for those who completed this study.
Footnotes
Acknowledgements
The authors would like to thank Rusty Walker, CP, FAAOP, at ProCare Prosthetics & Orthotics, Inc. in Buford, GA, USA, for supporting this research study and for the use of their facility and willingness to make prosthetic adjustments when needed by participants. The authors would also like to thank G Wells Petras, MA, LPC for his assistance in recruiting participants, data collection, and assistance with supervision during the exercise program.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.