
Abstract
Background:
Recent literature indicates equivalent costs of walking can be achieved after a transtibial amputation when the individual is young, active, and/or has extensive access to rehabilitative care. It is unknown if a similar cohort with transfemoral amputation can also achieve lower metabolic costs of walking than previously reported.
Objective:
Compare metabolic cost in individuals with a transfemoral amputation to controls and to the literature across a range of walking speeds.
Study design:
Cross-sectional.
Methods:
A total of 14 individuals with a unilateral transfemoral amputation (27 ± 5 years, N = 4 mechanical knee, N = 10 microprocessor knee) and 14 able-bodied controls (26 ± 6 years) walked at self-selected and four standardized speeds. Heart rate, metabolic rate (mL O2/kg/min), metabolic cost (mL O2/kg/m), and rating of perceived exertion were calculated.
Results:
Self-selected speed was 8.6% slower in the transfemoral amputation group (p = 0.031). Across standardized speeds, both metabolic rate and metabolic cost ranged from 44%–47% greater in the transfemoral amputation group (p < 0.001), heart rate was 24%–33% greater (p < 0.001), and perceived exertion was 24%–35% greater (p < 0.009).
Conclusion:
Although the transfemoral amputation group was relatively young, physically fit, and had extensive access to rehabilitative care, the metabolic cost of walking fell within the ranges of the literature on older or presumably less fit individuals with transfemoral amputation.
Clinical relevance
Developments in prosthetic technology and/or rehabilitative care may be warranted and may reduce the metabolic cost of walking in individuals with a transfemoral amputation.
Background
Walking independently with a lower limb prosthesis is a common, and often attainable, rehabilitation goal for individuals with a lower limb amputation. However, a full return to pre-injury ambulation can be hindered by the elevated metabolic cost of walking. “Metabolic cost” in this document refers to the metabolic energy expended, scaled to mass, per unit distance. Individuals with lower limb amputations are known to spend more energy than able-bodied individuals during walking1,2 with more proximal amputations associated with greater energy consumption than distal amputations. 3 At similar walking speeds, individuals with a unilateral transfemoral amputation (TFA) have a 20%–60% greater metabolic cost of walking than their able-bodied counterparts.3–12
This elevated metabolic cost of walking may be related, in part, to the number, type, and magnitude of compensations to control balance and propulsion. Individuals with TFA lack biological ankle push-off power and compensate by increasing mechanical work at the hip to continue forward progression.13–15 Similarly, increased demand is often placed on hip and pelvic musculature to control prosthetic knee and intact hip stability, 16 but these muscles (e.g. glutei) are larger and less efficient for propulsion. While these deviations may depend on the type of prosthetic device utilized (i.e. mechanical vs microprocessor controlled knee),17–19 energy expenditure during walking is reported to be independent of device classification. 20
Study methodologies and participant characteristics are important to consider when interpreting metabolic differences reported in the literature between individuals with amputations and able-bodied controls. Often, comparisons are at self-selected walking speeds (SSWS); however, individuals with TFA typically choose a slower walking speed than their most economical speed. 6 Furthermore, participant characteristics can play a key role in the metabolic and functional differences between individuals with vascular versus traumatic amputations. Vascular amputations are often associated with a greater metabolic cost than traumatic amputations, even when the level of amputation is the same.21–23 Age may contribute to worsened walking economy, resulting from various factors such as reduced muscular efficiency.24,25 Other characteristics, such as fitness, may also influence heart rate (HR) 26 and metabolic cost. 27 Therefore, a variety of factors should be considered when determining the metabolic cost of walking after an amputation and some reports indicate the gap between individuals with amputations and able-bodied individuals has the potential to narrow even further.
Recent research contradicts the commonly held belief that amputation necessarily increases the metabolic cost of walking. Relatively young (29.9 ± 5.3 years), active, Service Members with a traumatic transtibial amputations (TTA) showed equivalent metabolic rates (VO2), metabolic costs, and ratings of perceived exertion (RPE) to individuals with and without an amputation across a range of five walking speeds, standardized by leg length (0.74 ± 0.02–1.68 ± 0.05 m/s). 28 Thus, amputation may not unavoidably increase the cost of walking and pre-amputation metabolic costs of walking may be achieved with passive prostheses. Similar findings of equivalent metabolic costs between individuals with and without TTA when walking at the same speed occur infrequently in the literature but have been reported in children with traumatic amputations or congenital limb absences29,30 and other cohorts of Service Members. 12
Although the equivalent metabolic costs between individuals with TTA and controls were promising, it was not expected that individuals with more proximal amputations (e.g. TFA) could attain the same results as able-bodied individuals. Individuals with TFA face additional challenges compared to their TTA counterparts and, as a result, individuals with TFA walk with greater gait deviations from able-bodied gait than individuals with TTA. These deviations include vaulting, hip hiking and circumduction, and trunk lean,13,16 all of which must be controlled or initiated with greater and more prolonged activity of the trunk and lower extremity musculature. 31 However, it was theorized that certain subsets of the TFA population may be able to attain lower values than previously reported.
Young, active, and physically fit individuals with amputations, with broad access to physical therapy and prosthetics care, represent an ideal population to investigate the independent effect of amputation without the confounding factors of age, dysvascular disease, rehabilitation care limitations, and other factors and comorbidities that can influence metabolic cost. Therefore, the purpose of this study was to compare the metabolic cost of walking in cohort of young Service Members with a TFA to previous reports from the literature on individuals with both traumatic and dysvascular amputations. We hypothesized that Service Members with a TFA would have a greater metabolic cost of walking than controls, but a lower cost than previously reported in the literature in individuals who were older, presumably less fit, and/or when vascular disease was the etiology for TFA. A secondary purpose was to compare the metabolic cost of walking across a range of speeds between young, active, and otherwise healthy Service Members with a TFA and able-bodied controls.
Methods
A total of 14 Service Members with traumatic unilateral TFA and 14 able-bodied controls participated in this study. Inclusion criteria consisted of 18–44 years of age (based on prior population level age classifications 32 ), independent ambulation with a prosthetic limb for at least 2 months, and the ability to walk on a treadmill unassisted without the use of handrails. Exclusion criteria consisted of conditions or medications affecting metabolism and/or comorbidities limiting independent ambulation. All participants had extensive, daily access to rehabilitative care at the Center for the Intrepid, 33 and, due to occupational fitness requirements, were presumed to be physically fit prior to injury. While “extensive rehabilitation” has yet to be defined, or quantified, by either the Military or civilian sector, post-amputation rehabilitation of Service Members has been previously described,33–35 and it is important to note some of the differences between the care of Military and civilian amputees. These articles detail how individuals with amputations at the military’s Advanced Rehabilitation Centers receive nearly daily therapy sessions and have access to services for over nine different disciplines including physical therapy, occupational therapy, recreational therapy, nutrition, and behavioral health. In addition, Service Members do not have the same insurance limitations as civilians and receive prosthetic devices specific for the activities that are necessary for them to achieve their rehabilitation goals. (In contrast, the cost of prosthetic care is such that a civilian with an amputation may receive only one new prosthetic limb every 5 years. 36 ) Non-amputee, able-bodied control participants were recruited from the local population of active duty military personnel. All participants provided written informed consent for the research procedures approved by the Brooke Army Medical Center Institutional Review Board.
A portable metabolic unit (K4b2, Cosmed, Inc, Rome, Italy) was calibrated using known volume and gas concentrations as per manufacturer’s instructions and it collected expired gases with 30-s averaging. Participants wore a plastic mask secured over their nose and mouth and a HR monitor (Polar Electro Inc., Lake Success, New York) around the chest during six walking conditions. Then, participants walked on a treadmill at five standardized speeds and one SSWS. The SSWS was based on the mean speed of five passes across a 10-m-long walkway. Standardized speeds were based on leg lengths (measured from the greater trochanter to floor on the intact limb during relaxed standing with both feet on the floor) and Froude numbers of 0.06 (FR1), 0.10 (FR2), 0.16 (FR3), 0.23 (FR4), and 0.31 (FR5) 37 using the equation

The use of Froude speeds facilitates equivalent task demands across individuals with different anthropometric characteristics. The FR3 number approximates an average SSWS in able-bodied individuals and two speeds greater than and less than this speed were included to provide a range of walking speeds.
All testing was conducted in a single session. The treadmill walking conditions started with the slowest speed and progressed to the fastest speed. Approximately 5 min of walking were performed at each speed condition or until a steady-state rate of oxygen consumption was achieved for at least 2 min. Steady state was determined as a change of less than 10% in VO2 values during the final 2 min of data collection. 38 If steady state had not been achieved, subjects continued to walk until a 2-min plateau in oxygen consumption was reached. In the final 30 s of walking at each condition, participants rated their perceived exertion on a Borg scale from 6 to 20. 39 Rest was permitted between conditions as needed.
The FR5 speed presented a challenge for most (N = 10) prosthesis users to perform without the use of treadmill handrails and, therefore, this speed was excluded from any further metabolic analysis; it was only used to identify the fastest speed tested. Steady-state VO2 and HR were averaged during the final 2 min of data collection and scaled to biological body mass (i.e. exclusive of prosthesis mass). A two-way (group × speed) mixed model, repeated-measures analysis of variance (ANOVA) was performed in SPSS software (IBM Corporation, Armonk, NY). Mauchly’s tests for sphericity assessed variance between groups and Huynh–Feldt corrections were applied as necessary. Significant main effects of group were separated within each speed with post hoc, unpaired t-tests. Sequentially rejective Bonferroni–Holm corrections 40 were applied for five comparisons for gross metabolic cost, VO2, HR, and RPE. Post hoc comparisons between speeds were not performed. The unadjusted criterion for statistical significance was set at α = 0.05.
Results
All 14 individuals with a TFA were able to complete walking speeds FR1-FR3, but only 11 were able to complete FR4. All control participants were able to complete FR1-FR4 speed conditions. Respiratory exchange ratio values were <1.0 for all subjects and across all completed conditions, suggesting that walking at these standardized speeds may not have elicited an anaerobic response (mean (standard deviation, SD) TFA: FR1: 0.80 (0.07), FR2: 0.84 (0.07), FR3: 0.86 (0.07), FR4: 0.91 (0.06); Control: FR1: 0.75 (0.06), FR2: 0.78 (0.04), FR3: 0.80 (0.04), FR4: 0.81 (0.05)). Individual participant characteristics are presented in Table 1. There were no significant differences between groups for age (p = 0.760), height (p = 0.991), mass (p = 0.181), or leg length (p = 0.987). The similarities in leg lengths resulted in standardized speeds (FR1-FR4) that were not significantly different between groups (all p > 0.639). SSWSs, however, were significantly faster in the control group (TFA: 1.23 (0.10) m/s, Control: 1.34 (0.16) m/s, p = 0.031).
Individual participant characteristics.
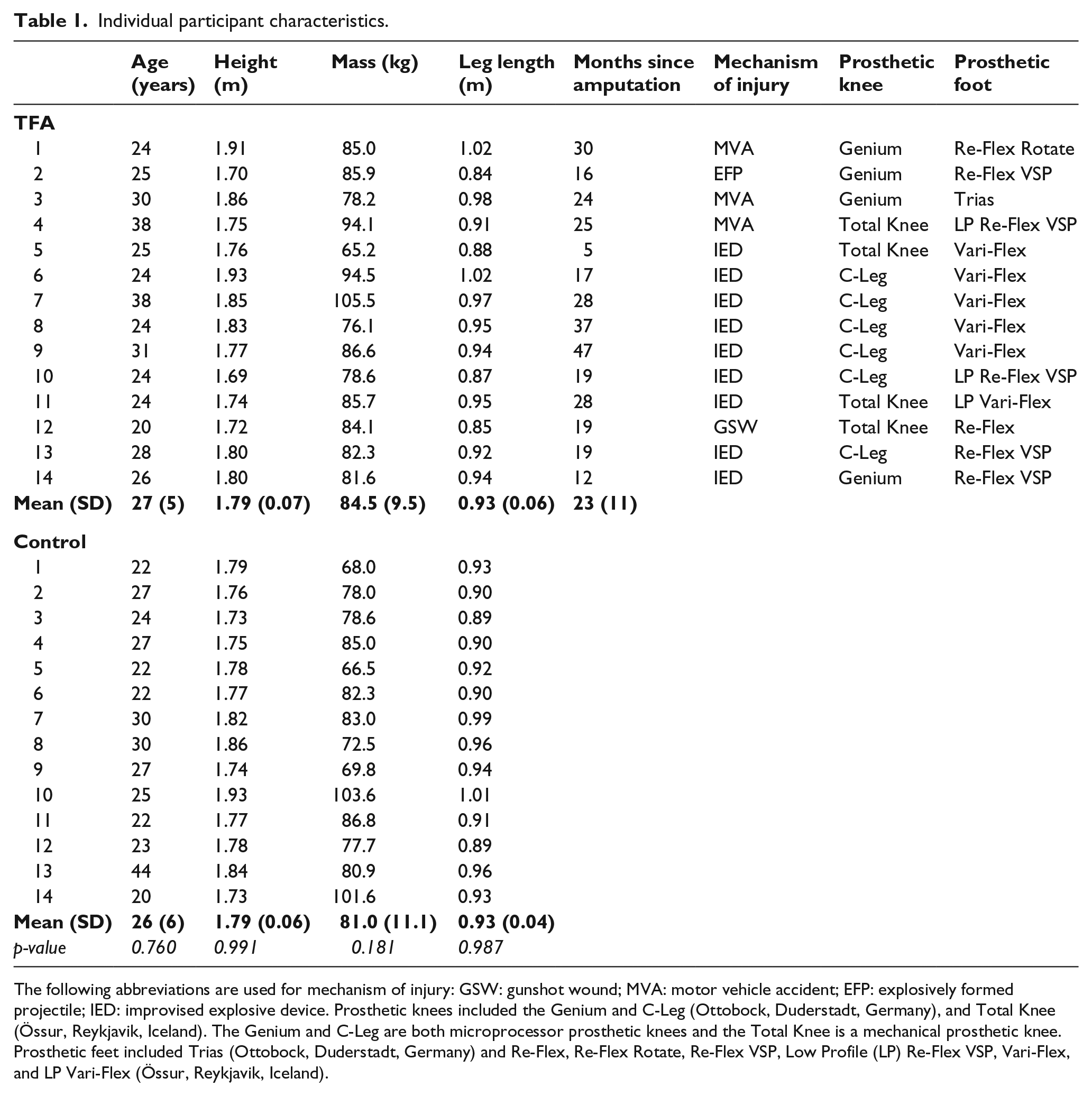
The following abbreviations are used for mechanism of injury: GSW: gunshot wound; MVA: motor vehicle accident; EFP: explosively formed projectile; IED: improvised explosive device. Prosthetic knees included the Genium and C-Leg (Ottobock, Duderstadt, Germany), and Total Knee (Össur, Reykjavik, Iceland). The Genium and C-Leg are both microprocessor prosthetic knees and the Total Knee is a mechanical prosthetic knee. Prosthetic feet included Trias (Ottobock, Duderstadt, Germany) and Re-Flex, Re-Flex Rotate, Re-Flex VSP, Low Profile (LP) Re-Flex VSP, Vari-Flex, and LP Vari-Flex (Össur, Reykjavik, Iceland).
The conditions of sphericity were not met for speed, VO2 metabolic cost, RPE, and HR, and Huynh–Feldt corrections were applied. There was a significant main effect of group (p < 0.001) such that the TFA group demonstrated significantly greater VO2 values than their able-bodied counterparts across all walking speeds (Table 2, Figure 1). Specifically, rates were 44%, 45%, 47%, and 47% greater than able-bodied controls at FR1, FR2, FR3, and FR4 speeds, respectively (p < 0.001 for all post hoc comparisons). Since the two groups walked at equivalent standardized speeds, percent increases in metabolic cost were almost identical to increases in VO2 (p < 0.001 for all post hoc comparisons), and all values increased with speed. At the SSWS, VO2 was 34% greater than controls (p < 0.001), but both groups chose SSWS at or near the most economical walking speed (lowest metabolic cost) of the four speeds tested (Figure 2). VO2 values at rest were not significantly different between groups (p = 0.885).
Mean (standard deviation bars) dependent measures.
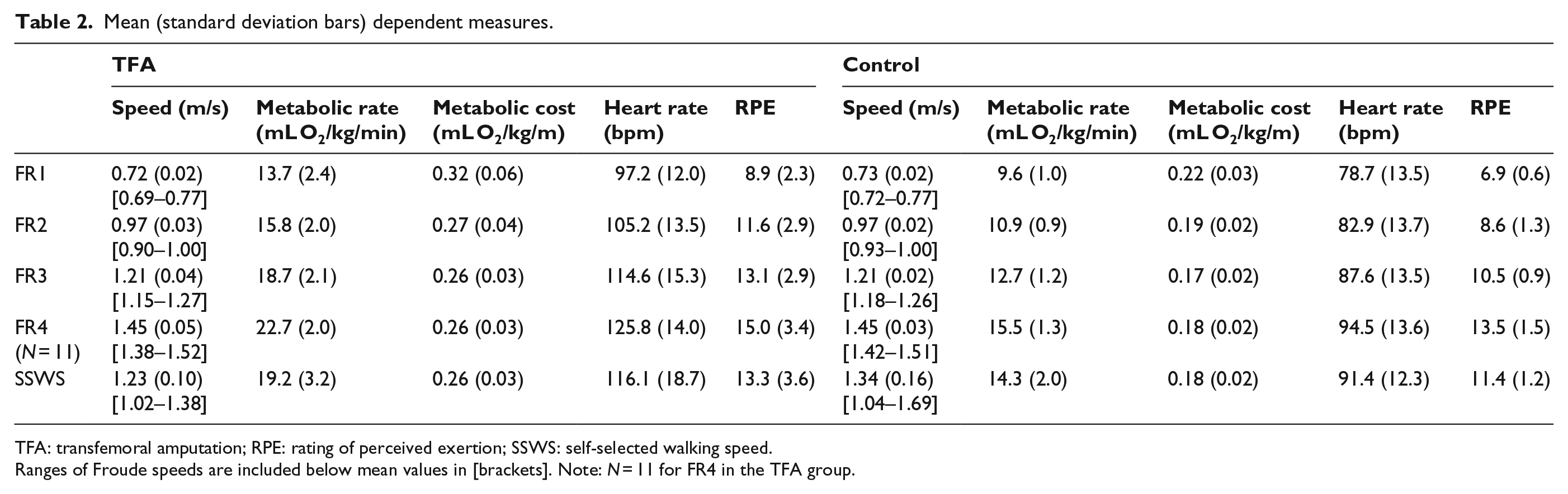
TFA: transfemoral amputation; RPE: rating of perceived exertion; SSWS: self-selected walking speed.
Ranges of Froude speeds are included below mean values in [brackets]. Note: N = 11 for FR4 in the TFA group.

Mean (standard deviation bars) metabolic rate (VO2) across the standardized (FR1-4) and self-selected walking speed (SSWS). symbols indicate mean SSWS values for each group. *Post hoc statistical significance between groups at each speed. Low horizontal lines indicate speed ranges for each of the Froude speeds. Note: 11 TFA participants completed the FR4 speed.
Mean (standard deviation bars) metabolic cost as a function of walking speed. symbols indicate mean SSWS values for each group. *Post hoc statistical significance between groups at each speed. Low horizontal lines indicate speed ranges for each of the Froude speeds. Note: 11 TFA participants completed the FR4 speed.
HR results were similar to VO2 and there was a significant main effect of group for HR (p < 0.001) and rates were 23%, 27%, 31%, and 33% greater in the TFA group compared to controls at FR1, FR2, FR3, and FR4 speeds, respectively (p ⩽ 0.001 for all comparisons) (Table 2, Figure 3). At the SSWS, HR was 27% greater than controls (p < 0.001). HR at rest was not significantly different between groups (p = 0.364).
Mean (standard deviation bars) heart rate (HR) across the standardized (FR1-4) and self-selected walking speeds (SSWS). symbols indicate mean SSWS values for each group. *Post hoc statistical significance between groups at each speed. Low horizontal lines indicate speed ranges for each of the Froude speeds. Note: 11 TFA participants completed the FR4 speed.
There was a significant main effect of group for RPE (p = 0.027) such that the TFA group perceived walking to be more strenuous than their able-bodied counterparts (Table 2, Figure 4). Specifically, RPE values were 28%, 35%, 24%, and 24% greater in individuals with TFA compared to controls at FR1, FR2, FR3, and FR4, respectively (p ⩽ 0.009 for all post hoc comparisons). RPE values were not significantly different at the SSWS (p = 0.076) even though values were, on average, 16.3% greater than controls.
Mean (standard deviation bars) rating of perceived exertion (RPE) across the standardized (FR1-4) and self-selected walking speeds (SSWS). symbols indicate mean SSWS values for each group. *Post hoc statistical significance between groups at each speed. Low horizontal lines indicate speed ranges for each of the Froude speeds. Note: 11 TFA participants completed the FR4 speed.
There were significant main effects of speed for VO2 (p < 0.001), HR (p = 0.034), and RPE (p < 0.001) such that the dependent measures increased with increasing speed. There were no significant interactions.
Discussion
The purpose of this study was to investigate the metabolic demand of walking in a cohort of Service Members with a unilateral TFA, across a range of speeds, and to compare these results to previous literature. As anticipated, the metabolic cost of walking was greater for individuals with a TFA than controls but, contrary to our hypothesis, this cohort of young Service Members with extensive access to rehabilitative care fell within the ranges reported in the literature and was not more economical than previous reports on older and potentially less fit individuals. On average, both VO2 and metabolic cost were 46% greater in the TFA group than controls. Although a few previous reports had indicated that normative metabolic rates and metabolic costs of walking could be achieved in individuals with TTA,12,28–30 the same results were not expected when the amputation was above the knee. However, our hypothesis that the metabolic demand of walking for young, active, and otherwise healthy individuals with a TFA would be less than previously reported in the literature was not supported. Values from this study fell well within the ranges of those reported in the literature for individuals with a unilateral TFA. For example, Starholm et al. 41 reported that individuals with a TFA consume 47% more oxygen per meter than controls at their most economic speed and Chin et al. 11 found similar VO2 values across a wide range of pre-determined, set speeds in their cohort of relatively young individuals who had sustained a traumatic TFA.
Lower extremity gait biomechanics may explain part of the increase in metabolic demand following a TFA. For example, the co-contraction of the lower extremity musculature common in individuals with amputations is thought to stabilize the lower extremity but could also contribute to an elevated energy cost. 42 Kinematic compensations that modify the path of the center of mass may also play a role. For individuals with either a TFA or a TTA, the mechanical work needed for the step-to-step transition from the amputation to sound limb is a major determinant in the increase in metabolic demand.14,15 The amputated limb is limited in its abilities to produce net positive mechanical work and the sound limb must then compensate to restore lost energy,43,44 all of which require energy generation and increase the metabolic demand of locomotion. The total mechanical work needed during these transitions increases with walking speed, 15 and metabolic demand is expected to increase accordingly. 45
Walking speed plays an important role in the metabolic cost of walking for individuals with amputations. Since many previous studies did not standardize walking speeds, we examined percent increases in metabolic cost between groups. Percent increases in the metabolic cost of walking between individuals with TFA and able-bodied controls range from 20% to 56% greater in the literature.3–11 In a similar patient population of young, active Service Members with a TFA, Bell et al. 46 found that VO2 values were 16% greater than this study as participants walked around a 65-m track at speeds equivalent to our FR3 speed. Waters et al. 3 reported metabolic cost values in agreement with Bell et al. 46 when young individuals with unilateral TFA walked around a similarly sized 60.5-m track, albeit at a slower speed. Comparisons of metabolic demand between treadmill and overground walking in individuals with amputations have previously found greater values on the treadmill,47,48 but this was not found when comparing this study to the literature. Figure 5 shows that a range of overlapping metabolic cost values for treadmill and overground walking, across many speeds, even with prosthesis type was the same.
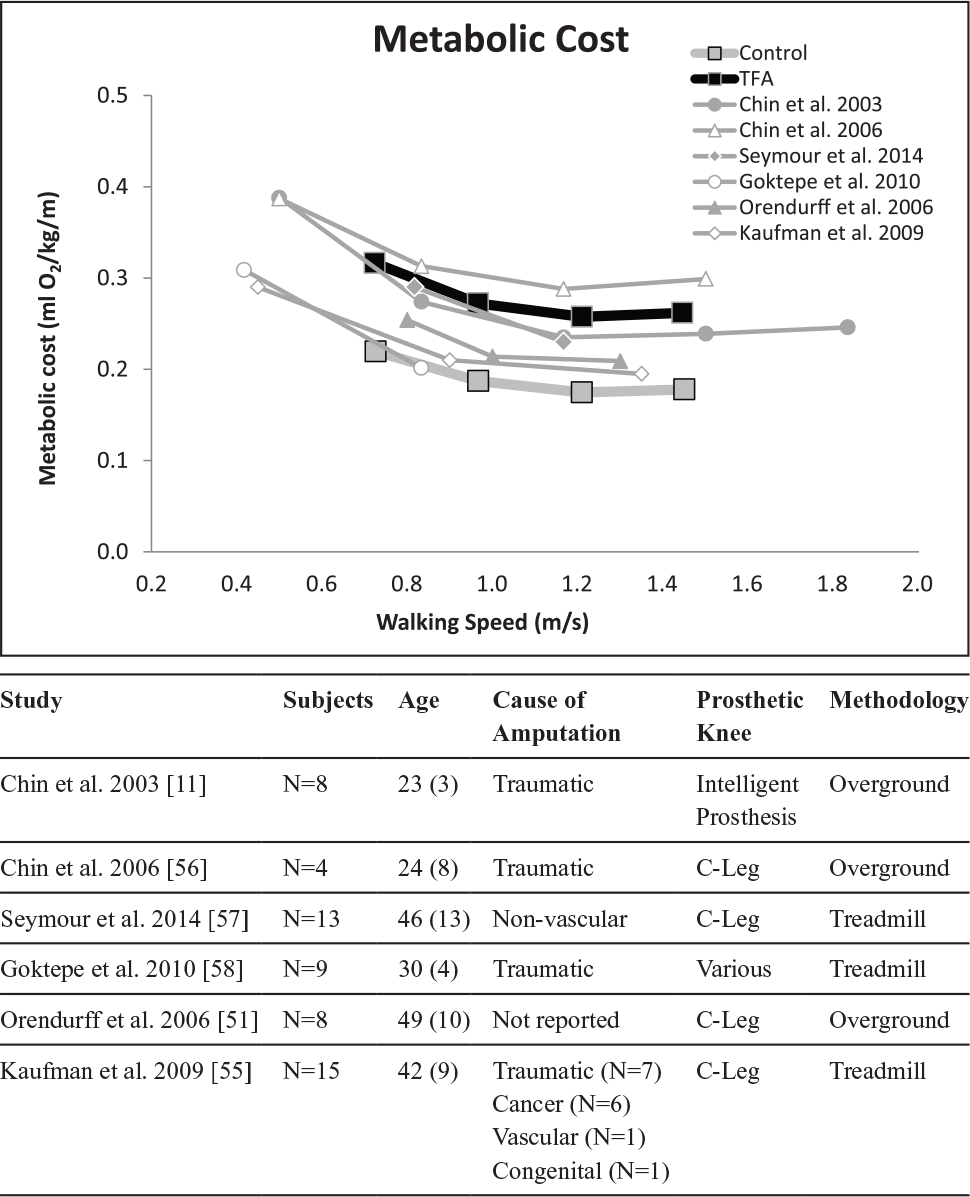
Mean metabolic cost from data in this study and prior literature on individuals with transfemoral limb loss. Data from this study for individuals with a transfemoral amputation (TFA) and the able-bodied control subjects are in bold lines. Subject characteristics from prior literature can be found below the figure.
Incorporating standardized speeds is important for comparative purposes, but SSWS may have greater relevance to daily life. Some previous literature indicates that individuals with a TFA do not necessarily prefer to walk at the most economical speed, but choose a slower speed, 6 while other literature 49 reports faster SSWS than the most economical. This lack of consistency among the literature indicates that ambulating at the least metabolic cost may not always be the primary optimization criteria for some individuals with amputation (stability, maneuverability, cosmesis, etc. may also play roles). However, the participants in this study did choose SSWSs that approximated their most economical speed (i.e. lowest metabolic cost). These SSWSs (1.23 (0.10) m/s) were significantly slower than their able-bodied counterparts (1.34 (0.16) m/s) and were within the ranges previously reported in this patient population. 46 For example, SSWS in a similar population of Service Members with a TFA averaged 1.11 and 1.28 m/s for individuals with short and long residual limbs, respectively. 46 These results differ substantially from other research on older patients with a dysvascular TFA, who walk substantially slower (e.g. 0.41 m/s9) than relatively younger individuals with a traumatic TFA.
Maximum tested walking speeds in this study were faster than those reported in the literature. Genin et al. 1 reported maximal attainable walking speeds ranging from 1.1 to 1.3 m/s for Cambodian landmine survivors who had undergone unilateral TFA (mean age, 34.7 years). In this study, although the groups were not instructed to walk as fast as possible, the peak speeds tested (without handrail support) in the TFA group were greater than those reported by Genin et al. 1 at an average of 1.49 (0.15) m/s and range from 1.24 to 1.77 m/s (fastest speed of a completed steady-state metabolic trial). However, likely differences in access to care, the type of rehabilitation received, and prosthetic devices may account for these differences. 50 For comparison, control participants walked at an average maximum tested of 1.67 m/s at FR5 and this speed ranged from 1.40 to 1.75 m/s, depending on leg length. It is possible that many of the participants in the TFA group may have been near their maximum sustainable speed at FR4 because only four participants were able to walk long enough to establish steady-state VO2 at the FR5 speed. However, at the maximum tested speeds, mean HR was 125 bpm, mean RPE was 15, and respiratory exchange ratios were less than 1.0, all of which suggests that acute cardiovascular fatigue was unlikely.
HR results were similar to VO2 and RPE in that they were greater in the TFA group across all walking speeds (24%–33% greater than controls). In a group of individuals with TFA, Gitter et al. 4 reported 36% and 49% increases from controls at matched speeds of 0.83 m/s (equivalent to FR1-2) and 1.11 m/s (equivalent to FR2-3). Greater HR was expected, as no prior literature has reported that HR values can return to pre-amputation levels during walking. Post-amputation, a number of physiological and cardiac changes may occur as a result of recovery from trauma, including a decrease in the contractile capacity of the myocardial tissue, regardless of the level or location of amputation. 51 The increase in HR may then serve to counter this decrease in stroke volume to maintain the necessary cardiac output.
Several limitations should be considered. First, ambulation times were variable and participants differed in their experience using a prosthetic knee. However, previous studies have found no differences in VO2 in individuals with amputations with shorter and longer prosthetic usage times. 46 In addition, both microprocessor and mechanical knees were included in this study based on previous reports indicating no significant differences in VO2 between devices.52,53 Also, data were only collected on a treadmill and energy cost is generally lower when walking at the same speed over ground. 48 An additional limitation is that subjects were not required to fast prior to data collection and the thermic effect of food on metabolic rate may have had a small effect on the results. Finally, although we believe scaling metabolic data to biological body mass is most appropriate, it may have affected the comparisons made to the control participants and to the literature as not all prior studies reported scaling procedures. If mass included the prosthesis, scaled metabolic values would have been artificially lower and the percent differences between individuals with TFA and controls would have been smaller.
Conclusion
The metabolic cost of walking was, on average, 46% greater in Service Members with a TFA compared to able-bodied controls, despite their youth, high level of pre-amputation fitness, and extensive access to rehabilitative care. VO2, HR, and RPE values were greater than controls across a range of walking speeds and magnitudes fell within the ranges of previous literature on the general population of individuals with unilateral TFA. The high metabolic demands may have also contributed to a slower SSWS than controls. The results indicate that developments in prosthetics and advances in rehabilitative care may be warranted for individuals with a TFA, regardless of their access to care, youth, or prior physical fitness level.
Footnotes
Author contribution
E.R.E. contributed to study concept and design, analysis and interpretation of data, and statistical analysis. E.R.E. and C.A.R. contributed to drafting of manuscript. All authors contributed to critical revision of manuscript for important intellectual content. J.W. obtained funding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Military Amputee Research Program, Telemedicine and Advanced Technology Research Center (Grant/Award Number: W81XWH-06-2-0073).