
Abstract
Background:
Hundreds of investigations examining biomechanical outcomes of various prostheses have been completed, but one question remains unanswered: how much time should an amputee be given to accommodate to a new prosthesis prior to biomechanical testing?
Objective:
To examine the literature for accommodation time given during biomechanical investigations to determine whether consensus exists.
Study design:
Systematic review.
Methods:
A systematic search was completed on 7 January 2016 using PubMed and Scopus.
Results:
The search resulted in 156 investigations. Twenty-eight studies did not provide an accommodation or were unclear (e.g. provided a “break in period”), 5 studies tested their participants more than once, 25 tested only once and on the same day participants received a new prosthesis (median (range): above-knee: 60 (10–300) min; below-knee: 18 (5–300) min), and 98 tested once and gave a minimum of 1 day for accommodation (hip: 77 (60–180) days; above-knee: 42 (1–540) days; below-knee: 21 (1–475) days).
Conclusion:
The lack of research specifically examining accommodation and the high variability in this review’s results indicates that it remains undecided how much accommodation is necessary. There is a need for longitudinal biomechanical investigations to determine how outcomes change as amputees accommodate to a new prosthesis.
Clinical relevance
The results of this review indicate that little research has been done regarding lower-limb amputees accommodating to a new prosthesis. Improper accommodation could lead to increased variability in results, results that are not reflective of long-term use, and could cause clinicians to make inappropriate decisions regarding a prosthesis.
Keywords
Introduction
Lower-limb amputees are routinely prescribed a prosthetic limb a few months post amputation. Depending on the type and cause of amputation and the activity level of the amputee, the type of prosthesis prescribed can vary greatly between amputees. While hundreds of investigations have been performed that examine biomechanical outcomes of various types of prostheses, one thing remains unclear: when should biomechanical investigations be performed?
To our knowledge, there have been almost no studies conducted that examine accommodation in amputees. English et al. 1 published a case study examining accommodation time of a single male knee disarticulation amputee. The participant was evaluated over 3 weeks in two different knee prostheses and the authors concluded that 1 week of accommodation was needed prior to making a clinical decision regarding a new prosthesis, and at least 3 weeks of accommodation were needed for research purposes. They did test the participant out to 21 weeks in one of the limbs and noted that changes still continued to occur over that time; but they concluded that this amount of accommodation was not necessary for conclusions regarding gait stability. 1 The lack of published literature regarding amputee accommodation has led us to question whether there is agreement in how much accommodation time is appropriate for biomechanical investigations examining a new prosthesis.
While there has been minimal published research regarding accommodation other than English et al., 1 the lack of accommodation information has been discussed in the literature. Highsmith 2 discussed the current general knowledge regarding accommodation and training with microprocessor-controlled prosthetic knees and noted that there is indecision in the research community of how to determine accommodation. In addition, Hafner and colleagues3,4 discussed the issues of accommodation after having completed a systematic review regarding outcomes with microprocessor-controlled prosthetic knees. They noted that the investigations included in their review had a wide range of accommodation times, ranging from minutes to 39 weeks, and many did not report whether accommodation had been provided.3,4 While these investigations provided information regarding the current thoughts regarding accommodation, they only focused on above-knee amputees using microprocessor-controlled prosthetic knees. The review presented here attempts to further expand on this topic.
It is important to understand accommodation as an amputee should be given time to accommodate to a new limb prior to performing a biomechanical investigation to ensure proper function of the prosthesis. A common aim in biomechanical examinations of amputees is to provide clinicians useful information on outcomes to improve their patient’s function. Improper accommodation could lead to increased variability in results, results that are not reflective of long-term use, and could cause clinicians to make inappropriate decisions regarding a prosthesis. As it is unclear from the literature how much accommodation is appropriate, the goal of this systematic review was to identify evidence-based consensus of when biomechanical analysis on the amputee population should occur after a patient receives a new prosthetic limb.
Methods
A systematic literature search was conducted 7 January 2016 using PubMed (1964–January 2016) and Scopus (1948–January 2016) to find all peer-reviewed original research articles examining biomechanical parameters in unilateral lower-limb amputees. The following lines were used as input: (lower limb OR lower-limb OR thigh OR leg OR shank) AND (amput* OR transtibial OR transfemoral) AND (prosth*). The databases searched titles, keywords, abstracts, and MeSH terms.
As the goal of this systematic review was to determine how much time, if any, investigations gave for accommodation, any articles related to an investigation of a lower-limb prosthesis had to be gathered and then read to determine whether accommodation was provided. As such, the initial inclusion and exclusion criteria for the automated database searches were kept broad to obtain a large collection of possible articles. The search was limited to peer-reviewed journal articles, human participants, and the English language. Titles, abstracts, and full texts were then manually screened as necessary to further exclude non-peer-reviewed conference proceedings, theses, dissertations, reviews, case reports, and white articles. Studies examining only bilateral amputee populations or participants under the age of 18 years were excluded to eliminate possible confounding factors.
To be classified as a biomechanical investigation, the study had to objectively evaluate amputees. A biomechanical investigation could involve the use of force platforms, quantitative two-dimensional (2D) video or three-dimensional (3D) motion analysis, measurement of muscle activity, or analysis of energy consumption. Objective functional outcomes, such as the 6-minute walk test, were also acceptable. Studies that only reported subjective assessments, such as self-reported surveys and subjective gait analysis, were excluded. Articles that only examined a change in alignment, mass, inertia, socket or pylon features of a prosthesis were excluded. Only articles that examined a new prosthesis with a new foot, ankle, knee, or hip joint unit were included in this review. While alignment, mass, inertia, socket, pylon, or similar changes could, if large enough, effectively result in a new prosthesis that would warrant accommodation time, these studies were excluded because such changes are made on an individual basis. Limiting to new prosthesis joint created a more homogenous, comparable amount of accommodation that would be expected across studies.
Two independent reviewers completed the search. One reviewer read and extracted data from the final set of articles. A third independent reviewer completed a quality assessment check on a random 10% of the final articles to ensure data were extracted accurately. The data extracted included whether accommodation was given, how much time was given, and whether justification of accommodation was provided. Basic population characteristics (sex, age) and population size were also extracted.
Results
A total of 8058 unique hits were found between PubMed and Scopus. After reviewing titles and abstracts, a total of 349 articles remained. Of these, 123 matched our criteria of a peer-reviewed article that presented the results of a biomechanical investigation where the amputee participants were given a new prosthetic limb. The references of these articles were also evaluated using the same criteria, resulting in an additional 31 articles for a final total of 154 articles (Figure 1).
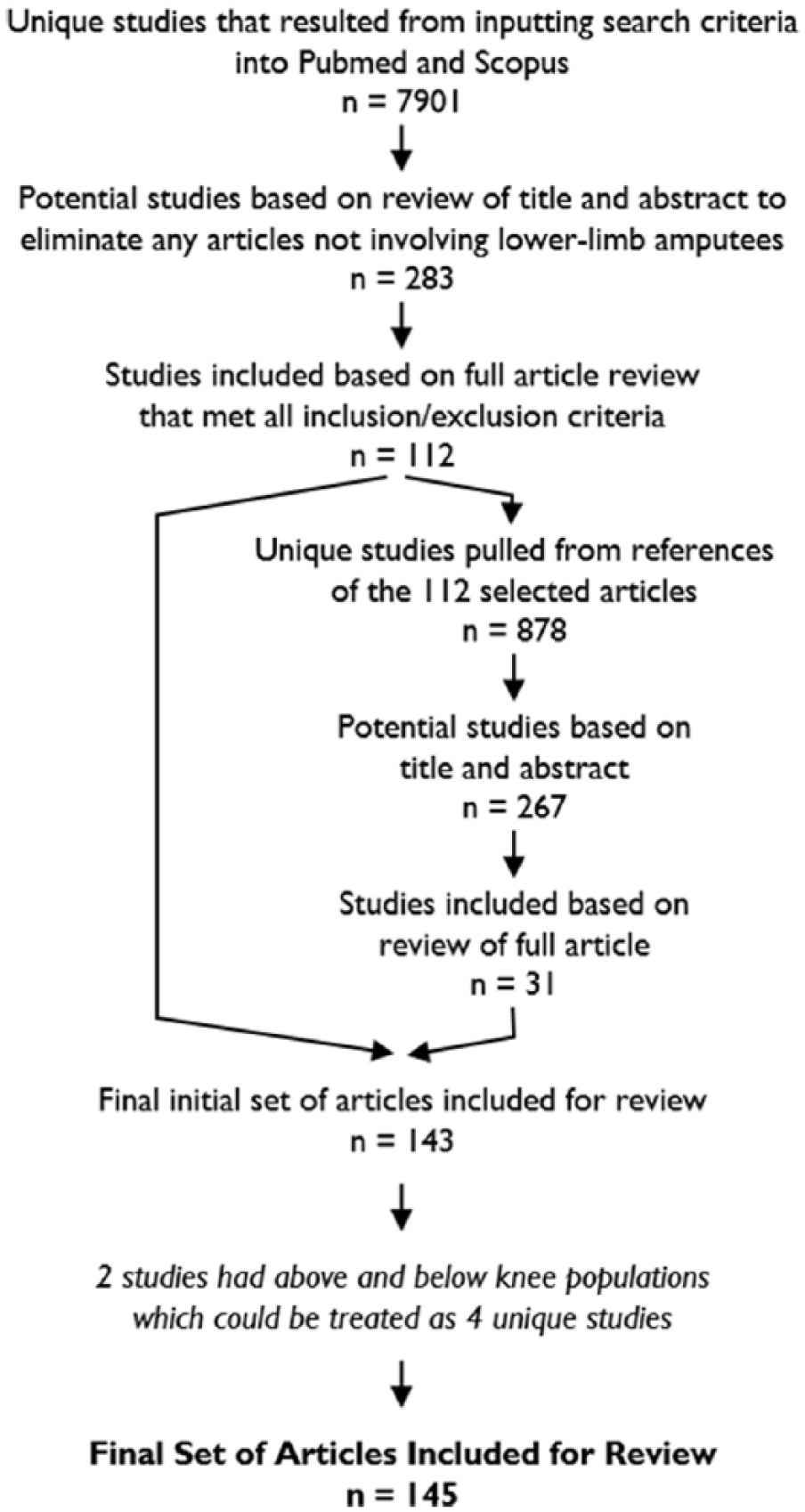
Selection process of the final 156 studies included in this review.
Two of the articles included in this review examined both above- and below-knee populations.5,6 Since each article reported the characteristics and results for each amputee population separately, these two articles were treated as if they were actually four articles. As such, even though only 154 articles were included in this review, the results from 156 investigations are presented here.
In all, 67 studies involved above-knee amputees (transfemoral amputation or knee disarticulation),5–71 85 involved below-knee amputees (transtibial amputation or Syme’s amputation),5,6,72–154 and 4 involved hip amputees (hip disarticulation or transpelvic amputation).155–158
Population characteristics
A total of 1489 amputee participants were examined from the 156 studies. Time since amputation and prosthesis experience varied greatly between and within studies. By examining authorship and participants’ sex, age, height, and weight, 16 duplicate populations from 35 investigations were identified (Table 1). After adjusting for duplicate populations, an estimated total of 1266 unique amputees were examined (Table 2). Twenty-four studies did not report (NR) the sex of the participants.6,12,36,42,52,55,56,60,65,69,80,82,88,89,102,112,113,120,124,130,138,147,152
Sixteen population groups were used multiple times in a total of 35 investigations.
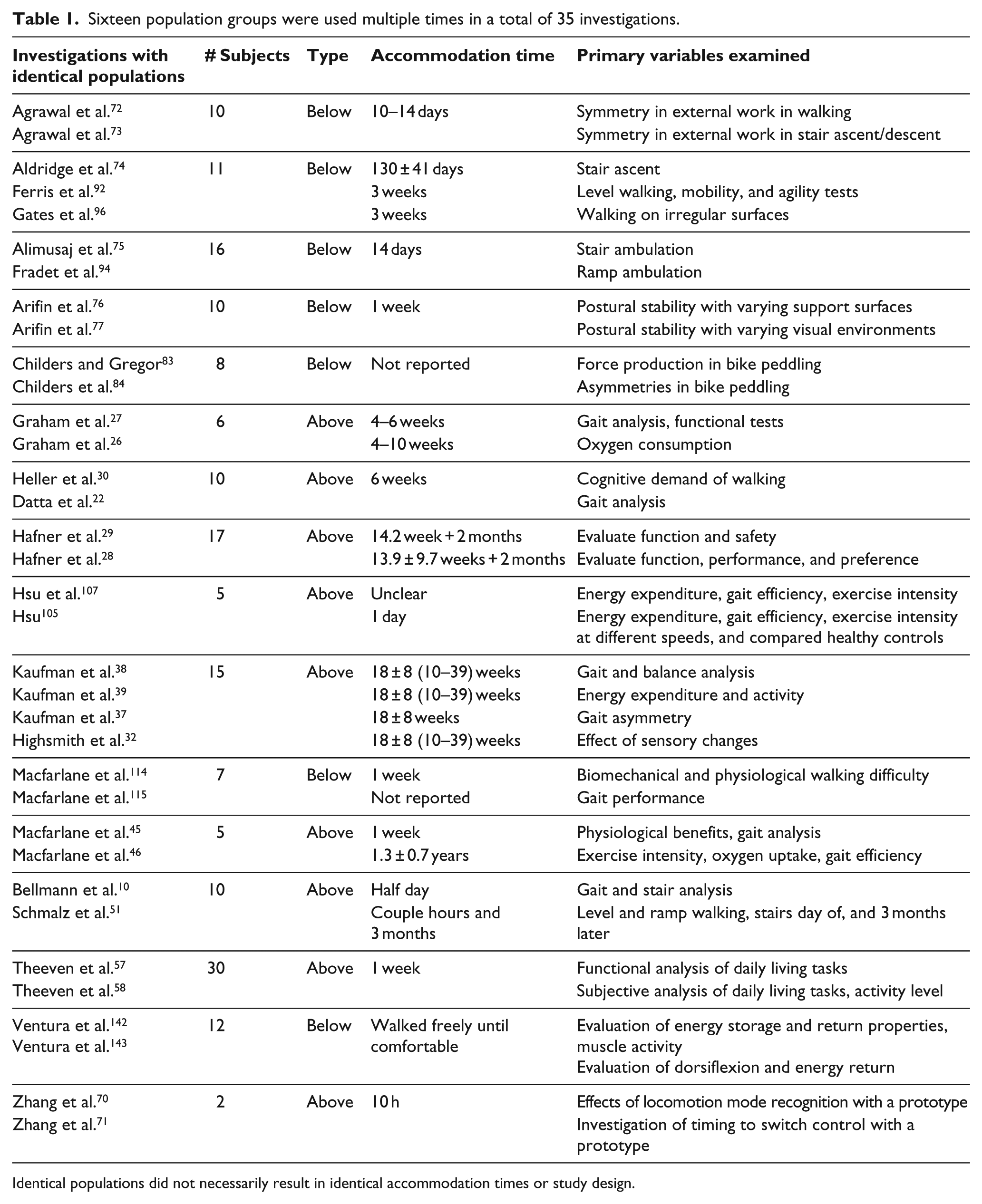
Identical populations did not necessarily result in identical accommodation times or study design.
Population characteristics of all unique populations.
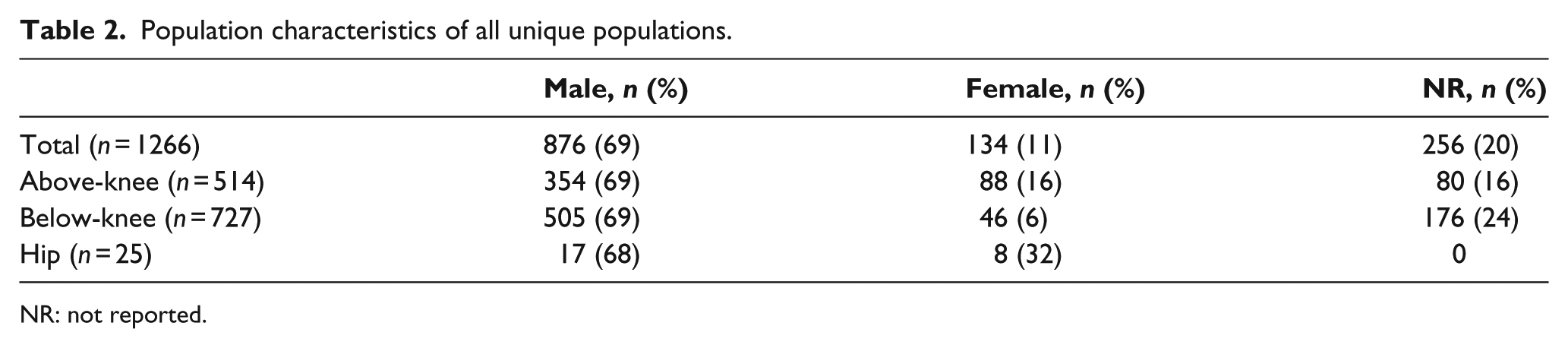
NR: not reported.
The median size of unique populations was 8 (range: 2–30). The most common population size was 10, used in 20 studies.10,17,30,54,60,64,68,72,77,85,90,95,112,121,123,127–129,134,138
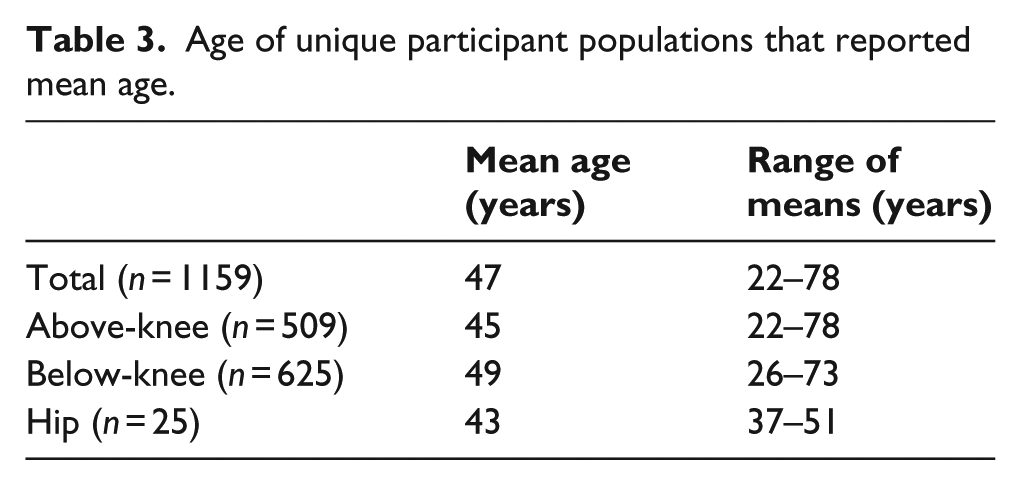
Of the 143 unique study populations, 129 reported a mean age (58 above-knee studies, n = 509 participants; 67 below-knee, n = 625; four hip, n = 25). A total of 10 reported only a range of ages (all below-knee, n = 70), and 4 did not provide any information regarding ages (1 above-knee, n = 5; 3 below-knee, n = 32); thus, 107 participants were excluded when calculating the average age of all participants. The average age, weighted by number of participants per study, of the 1159 participants across the 129 studies that reported mean ages was 47 years (Table 3).
Age of unique participant populations that reported mean age.
The reported causes of amputation were trauma, dysvascular complications, cancer, congenital, or other (Table 4). The “other” category includes amputations categorized as non-peripheral vascular disease, nonvascular, or nondysvascular, and amputation due to infection, secondary illness, polio, sepsis, disease, Beurger’s disease, and lupus. Trauma accounted for the most amputations for above- and below-knee amputees. In the hip populations, cancer was the leading cause. In total, 31 studies (12 above-knee, 19 below-knee) did not report the cause of amputation.5,7,17,24,25,34,40,41,44,59,70,71,78,80,86,89,91,110,112,113,120,121,125,134,143,144,146,151,152,154
Cause of amputation of all unique populations.
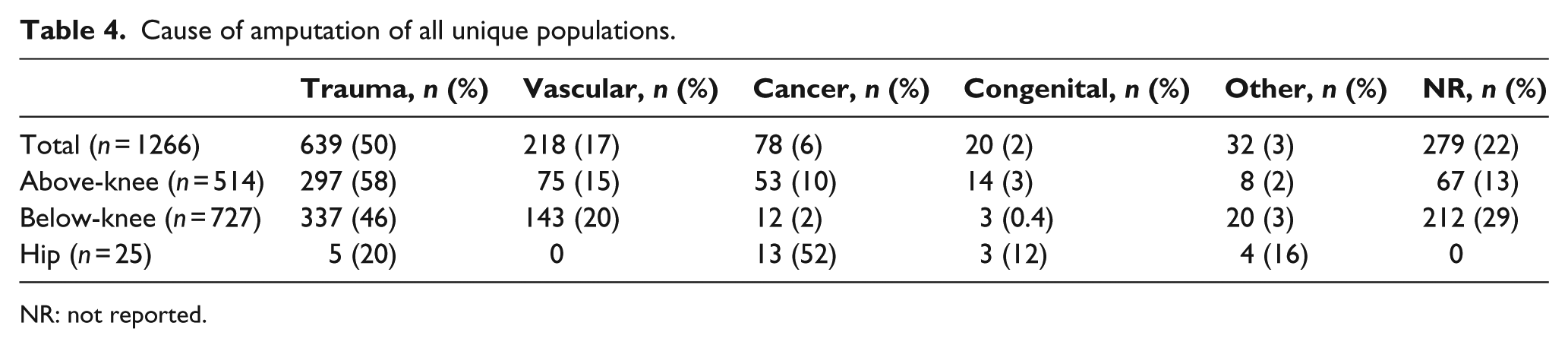
NR: not reported.
Accommodation time
The accommodation times from all 156 studies are included in this analysis. Even though multiple investigations used the same subject populations, we did not remove any investigation from this portion of the analysis as the reported results and accommodation times were not necessarily the same (Table 1). From all 156 investigations included in this review, 28 studies (1 hip, 6 above-knee, and 21 below-knee) either did not specify any accommodation or were unclear in how much time was given.5,12,20,40,52,60,78,83,84,98,102,112–114,116,121,123,131,135,142–144,149,153,154,157 Phrases such as “break in period,” 113 “walked freely until comfortable,”142,143 and “intensive practice phase” 52 were used to describe accommodation times. Twenty (1 hip, 2 above-knee, and 17 below-knee) of these 28 studies made no mention of the time between receiving and testing the new prosthesis.5,40,78,83,84,98,102,107,112–114,116,121,123,131,144,153,154,157
Five studies (one above-knee and four below-knee) examined their participants at multiple time points after receiving a new prosthesis.51,90,100,109,148 Delussu et al. 90 tested below-knee amputees the day of, 30, 60, and 90 days after receiving a new prosthesis. Grabowski et al. 100 tested below-knee amputees 3 and 21 days after. Isakov et al. 109 tested below-knee amputees the day they received the new prosthesis and 3 weeks later. Wurdeman et al. 148 tested below-knee amputees the day of receiving the new prosthesis, 1.5, and 3 weeks after. Schmalz et al. 51 tested above-knee amputees the day of receiving the new prosthesis and 3 months after.
In all, 25 studies (7 above-knee and 18 below-knee) tested their amputees only once and tested on the day of receiving a new prosthesis with times ranging from within minutes of receiving the new limb to approximately a half-day after (Table 5).6,9,11,25,55,56,59,79,80,87,89,93,99,103,104,110,111,117,122,130,132,134,139,145 Eighteen (4 above-knee and 14 below-knee) of the 25 tested within the first hour.6,55,56,59,80,89,93,103,110,111,117,122,130,132,134,139,145
Accommodation results for the 25 studies that tested their participants only once and on the same day participants received a new prosthesis.

For studies that provided a range of data, the midpoint was used during calculations. Units in minutes.
The remaining 98 studies (3 hip, 53 above-knee, and 42 below-knee) reported accommodation times, tested their participants only once, and did not test on the same day of the participants receiving a new limb (Figure 2, Tables 6 and 7).7,8,10,13–19,21–24,26–39,41–50,53,54,57,58,61–77,81,82,85,86,88,91,92,94–97,101,105,106,108,115,118–120,124–129,133,136–138,140,141,146,147,150–152,155,156,158 Seventy-four of the 98 reported a single accommodation time (e.g. 2 weeks). Nine of the 98 reported the accommodation as a mean time with standard deviation (SD) (e.g. 43.1 ± 18.1 days). The last 15 of the 89 reported a range of time (e.g. 4–10 weeks) or a mean ± SD with a range (e.g. 18 ± 8 weeks with range: 10–39 weeks). The below-knee populations were given the shortest accommodation times (median (interquartile range): 21 (12–30) days) compared to the above-knee populations (42 (14–90) days) and the hip populations (77 (69–129) days).
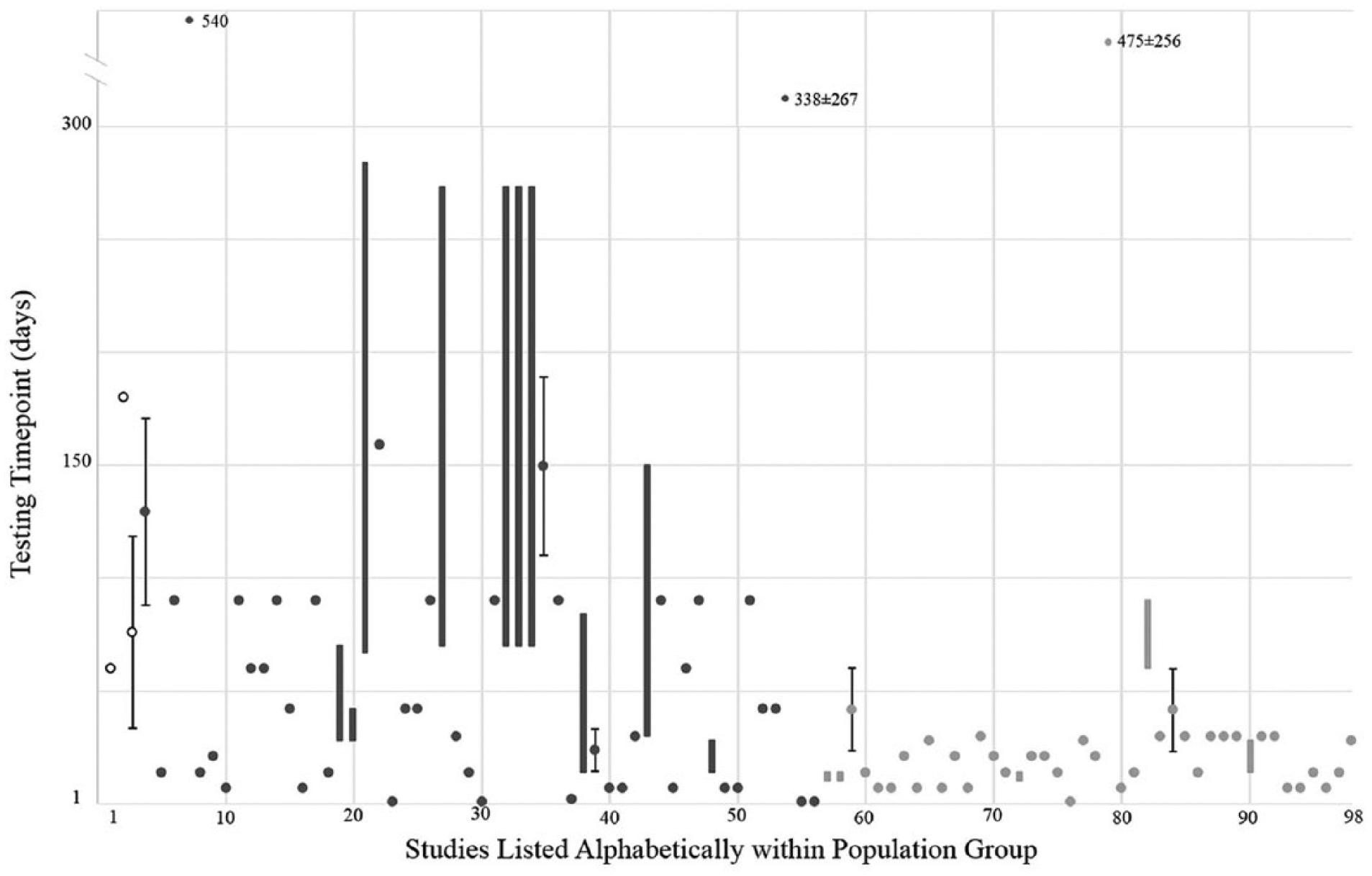
Reported testing time points of 98 studies that tested participants once and allowed a least 1 full day of accommodation. A single given time is represented by dot, a range of accommodation times is represented by a box, and mean time ± SD is represented by a dot with error bars. Non-solid black indicates hip populations, dark gray above-knee populations, and light gray below-knee populations. Information on references and accommodation times can be found in Table 6.
List of author and accommodation times of the 98 studies shown in Figure 2.

Accommodation results of the 98 studies that tested their participants only once and gave at least 1 full day of accommodation.
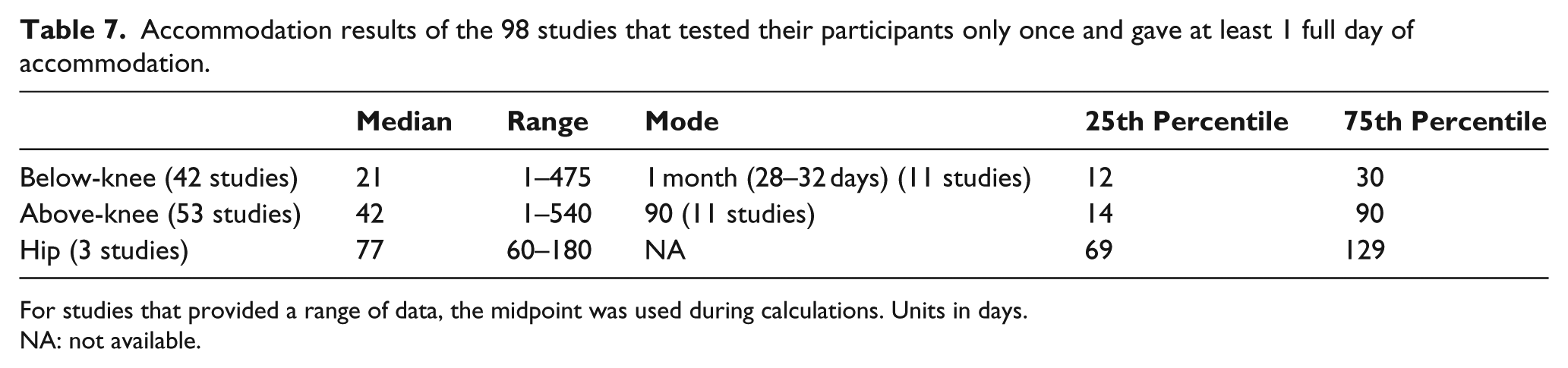
For studies that provided a range of data, the midpoint was used during calculations. Units in days.
NA: not available.
Discussion
The goal of this systematic review was to determine when biomechanical investigations were performed after an amputee receives a new prosthesis. The results of this review indicate that there is little consensus in accommodation time for above- and below-knee populations and there is a need for research to determine the effect of accommodation on biomechanical outcomes.
Five of the 156 investigations tested their amputee populations more than once. Three of these investigations tested at two different time points.51,100,109 Grabowski et al. 100 performed testing at 3 days and 21 days. They reported a significant reduction in metabolic cost at day 21 compared to day 3 while participants wore the K3 Promoter foot. The results seem to indicate that accommodation had not occurred by day 3. Isakov et al. 109 performed testing the day their participants received a new limb and 3 weeks later. The participants were below-knee amputees still in the hospital recovering from the amputation while receiving intensive physical therapy. While the authors did not specifically address accommodation, they did note that significant improvement was seen at week 3 compared to the first day in various parameters and “… that in people who have recently experienced [below-knee amputation] there is a continuous process of compensation and adaptation to the new situation of a partial limb loss.” Schmalz et al. 51 performed testing within a couple of hours and 3 months after receiving a new limb, with the goal being to determine whether a well-established transfemoral amputee currently using a C-Leg could transition quickly to a new Genium knee unit after only a few hours. The results of the article did show minimal differences in outcome measures between the two time points, indicating that the amputees appeared to have accommodated to the Genium over 3 months. While this study does address the question of accommodation, it only examined well-established amputees at two time points who were already active users with a C-Leg as they transitioned to a slightly more advanced Genium knee. The authors did note that accommodation appears to occur quickly if the amputee is already familiar with the motion patterns capable with the new knee (e.g. climbing stairs), but that if an amputee is not familiar with the motion then a longer accommodation period would be required. 51
The last two of these five studies examined their participants more than two times.90,148 Delussu et al. 90 performed testing at 1 h, 30 days, 60 days, and 90 days. The authors reported that improvements in level walking outcomes occurred across all time points, with the most improvement seen at 90 days, which they interpreted as indicating the user was fully accommodated to the new limb. 90 Wurdeman et al. 148 performed testing the day of their participants receiving a new limb and 1.5 and 3 weeks later. While the goal of the article was to use Lyapunov exponents to determine if changes occurred in stride-to-stride fluctuations at each joint, they only examined their population out to 3 weeks. The authors’ main finding was that there was significantly reduced fluctuation at 1.5 weeks in the prosthetic ankle joint compared to the sound ankle, but there were little differences between the initial testing and the testing at 3 weeks. They argued that this was indicative of a learning technique used to accommodate to the prosthesis. 148
Some conclusions regarding accommodation can be made from these five studies’ results. The results from Wurdeman et al. 148 are perhaps the most interesting as they showed that changes do occur after receiving a new limb but they found minimal differences between the first and last testing points. As Grabowski et al., 100 Isakov et al., 109 and Schmalz et al. 51 only examined their participants at two distinct time points, it is difficult to say whether their participants had accommodated to a new limb at the end time point. It is clear, however, that outcome variables were different between the first and end time points, indicating that participants were not accommodated at initial testing. Delussu et al. 90 also support this conclusion as they noted changes occurred over four distinct time points. Thus, it can be argued that testing within 3 days of receiving a new limb may not produce results relevant to long-term use. It is important to note that this conclusion has implications for the clinical fitting and alignment process performed upon receipt of a new prosthesis. In general, a prosthetist or clinician makes alignment changes based on observational gait analysis immediately after fitting the new limb. The resultant optimal alignment may not still be appropriate after time passes and the amputee accommodates to their new prosthesis. Additional gait observations and adjustments may need to be made to ensure a proper fit and alignment throughout the first few weeks of use.
In all, 28 studies either gave no accommodation or were unclear in how much time was provided. While some of these studies indicated that they gave their participants time to accommodate, phrases such as “break in period,” 113 “walked freely until comfortable,”142,143 and “intensive practice phase” 52 do little to indicate exactly how much time was provided. Twenty of these 28 gave no indication that any accommodation was provided. Based on other investigations that observed changes weeks after being given a new limb, the long-term relevance of these results that provided minimal or no accommodation is questionable.
In total, 25 studies tested the day of their participants receiving a new limb, with 18 testing within the first hour. Only 7 of the 25 involved above-knee populations.6,9,10,25,55,56,59 It should be noted that at least six studies appeared to test prototype devices which would have most likely prohibited the amputee participants from wearing the device home and having a proper accommodation time.79,80,87,99,104,117 Providing a short accommodation time may also be by design to examine the immediate effects of a new limb; however, of the 25 studies that tested the day of provision, only one study explicitly indicated that they were studying the immediate effects of a new limb. 11
It is clear from the 98 studies that gave their participants at least one full day for accommodation that there is little consistency or agreement on accommodation. However, there does appear to be a consensus that below-knee amputees do not need as much time to accommodate to a new limb as above-knee amputees. The median for below-knee amputees was 21 (range: 1–475; interquartile range: 12–30) days. This is less time than the 42 (range: 1–540; interquartile range: 14–90) days given to above-knee amputees and the 77 (range: 60–180; interquartile range: 69–129) days given to hip populations. This consensus makes logical sense as a below-knee amputee loses articulation at one main joint whereas above-knee amputees lose two. Learning how to use a prosthesis with two joints should prove more difficult.
A few studies did provide detailed plans for accommodation. For example, Hafner and colleagues28,29 provided two additional months of accommodation time after their participants decided they had sufficiently accommodated to the new prosthesis. Segal et al. 53 gave their participants three additional months of accommodation after spending 1 month accommodating with a new prosthesis. In the case of testing an amputee in a prosthesis previously worn, some investigators varied the accommodation time. For example, Doane and Holt 91 gave 2 days of accommodation if the participant was using a prosthetic foot he or she had already worn or gave 1 week if a new prosthesis was being tested.
Justification for providing or not providing accommodation was not given in all investigations. Eighty-three of the 156 studies made no comments regarding accommodation or did not provide a justification of a given accommodation time.5,6,13–17,21,24–27,33,35–37,40–42,48,52,54,56,60–63,66,75,78,79,83–86,91,92,94–96,101,103,104,107,109,112–115,118,120–125,127–131,133–138,140,143,144,146,147,149,150,152–154,157 Fourteen of the 156 studies specifically cited or discussed the case study by English. Six of these 14 studies8,50,76,77,148,151 directly used the time recommended by English (1–3 weeks) while the other 8 studies used longer accommodation times.28–30,47,51,53,68,156 The remaining 59 studies did provide some form of justification of their accommodation time, but most of these investigations followed the advice of a clinician or prosthetist, allowed the amputee to decide whether they had accommodated sufficiently, cited other investigations’ times, or followed their own design. Many authors mentioned in their limitations that there was a lack of research available on accommodation, and that the times provided may have been too short to fully ensure their participants had accommodated properly to a new device.
Only 3 of the 59 studies that provided justification used objective performance-based measurements to provide proof that their participants had accommodated to a new limb. Silver-Thorn and Glaister 55 provided accommodation until the participants’ self-selected level walking speed with a new prosthesis was within 10% of their speed with their original limb. Portnoy et al. 126 noted that as there was no change in cadence between the original and new limbs that their participants were accommodated. Finally, Devlin et al. 23 provided accommodation until the participants’ 2-minute walk tests with the new limb and original limb did not differ by more than 6%. While these three investigations used objective measurements to assess accommodation, their determination of accommodation relied on comparisons to the original limb which is not ideal as the amputees had switched to a new prosthesis and thus changes should be expected in functional outcomes. These three studies also highlight that providing a fixed accommodation time may not be appropriate. Every amputee adjusts and adapts to a new limb differently, and thus, it follows that accommodation times would differ across participants. Using a fixed accommodation time, this individuality is ignored. The use of performance-based outcomes would allow for consistency across varying amputee populations, so that age, sex, type and cause of amputation, type of prosthesis, prosthetic experience, and other physical or mental conditions are not ignored when setting an accommodation time. Using performance-based outcomes, researchers could be more confident that each of their participants is accommodated to a new limb.
The use of performance-based outcomes to determine accommodation has not yet been examined, and this review has further demonstrated the need for serial testing to be completed to fully determine how amputees accommodate to a new prosthesis. In addition, more complicated tasks, such as stair climbing, may require longer accommodation than simple tasks, such as level walking. It is also important to consider that different outcomes (e.g. kinematics, kinetics, functional tests, energy consumption) may require different accommodation times. These topics need to be further explored and examined in future investigations. Finally, knowing the repeatability of the outcome of interest is critical to investigation accommodation time and identifying when an outcome has plateaued. The five investigations that examined their participants more than once could conclude that their outcomes of interest had not stabilized by the early testing time points, but no conclusions could properly be made regarding the final testing time point. Biomechanical outcomes have natural variability that should be fully characterized in amputee populations before determining that a plateau effect has occurred and the amputee has accommodated to their device.
Conclusion
It is evident from this systematic review that there is little consistency in when biomechanical investigations are performed on amputee participants. Because it is not always feasible or cost efficient to test amputees multiple times for each individual investigation or clinical case, there is a clear need for published research examining the effect of accommodation on biomechanical outcomes to provide guidance for both the researcher and clinician on the most optimal time to evaluate amputees. Future investigations should attempt to examine amputee participants multiple times over the first year after receiving a new prosthesis to determine how and when biomechanical outcomes stabilize. Multiple investigations should be conducted to evaluate accommodation differences between type of amputation (transfemoral versus transtibial) and type of prosthesis (e.g. mechanical devices, variable damping, powered, energy storage and return). The results of these investigations would help determine testing parameters for researchers, as well as inform clinicians and their patients on what to expect after receiving a new prosthesis.
Footnotes
Acknowledgements
The authors would like to thank Katherine Heath and Aashika Katapadi for their assistance in performing the systematic review search and data extraction.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.