
Abstract
Background:
Granuloma annulare is a benign, inflammatory skin disorder with no distinct aetiology or widely accepted pathogenic process.
Case description and Methods:
We report a case of a 71-year old female with a 4-year history of an erythematous annulopapular lesion to the lateral aspect of her right forearm from a pressure pleat ridge in a high-density polyethylene plastic elbow orthosis to immobilise a prior radial head fracture. Morphological and histopathological assessment was consistent for granuloma annulare.
Findings and Outcomes:
The granuloma annulare was ameliorated after 3 months of high-potency topical steroids under occlusive dressing.
Conclusion:
This case highlights an atypical presentation of a pressure-induced patch of localised granuloma annulare persisting long-term after temporary use of a high-density polyethylene orthosis with a pleated point ridge. Special care should be taken when choosing the appropriate orthosis in patients with sensitive skin conditions. Moulded orthoses can have defects after manufacturing that can lead to localised skin irritation, inflammation and subsequent rash formation.
Clinical relevance
Appropriate casting and splint moulding should be taken into special consideration in patients with sensitive skin conditions. This prevents or diminishes the chance inducing or exacerbating skin conditions.
Background
Granuloma annulare (GA) is widely described in its different clinical forms including annular, linear, localised, disseminated, subcutaneous, papular and perforating. Localised GA accounts for 75% of cases of GA mostly occurring in females, a 2:1 ratio, and typically in the population under the age of 30 years.1,2 Localised GA often presents from a solitary patch to clusters of annular skin coloured to erythematous papules commonly seen on the dorsal hands or feet of patients affected. The current literature informs that localised GA is self-limiting with resolution commonly reported up to a few years after onset. 3
Case description and Methods
A 71-year old Caucasian female was referred for assessment after a 4-year history of an intermittently pruritic, erythematous annulopapular lesion to the right lateral forearm. Relevant medical history included an open reduction internal fixation for a radial head fracture followed by the use of high-density polyethylene plastic orthosis for immobilisation. Several months after application of the elbow orthosis the patient reported a small tan scar-like lesion on the lateral forearm. The initial diagnosis of the skin lesion was a possible stitch granuloma or early keloid scar. After 4 years of progressive increase in size, the patient pursued dermatological care for assessment of the lesion. Of note, the patient reported a pleated ridge on the inner aspect of the elbow orthosis that corresponded to the skin lesions’ line.
The patient’s other medical history included type II diabetes mellitus, hypertension, dyslipidaemia and a previous ischaemic stroke. The patient’s medications included metformin, gliclazide, atorvastatin, amlodipine and clopidogrel. Physical examination revealed an erythematous, annulopapular patch to the right lateral forearm (Figure 1). Examination of the plastic splint revealed a pleated edge defect pressing on the skin corresponding to the arcal shape of the annulopapular lesion (Figures 2 and 3). A pressure-induced patch GA was the working diagnosis with a differential diagnosis of discoid eczema, cutaneous parasitic infection and dermatophyte infection.
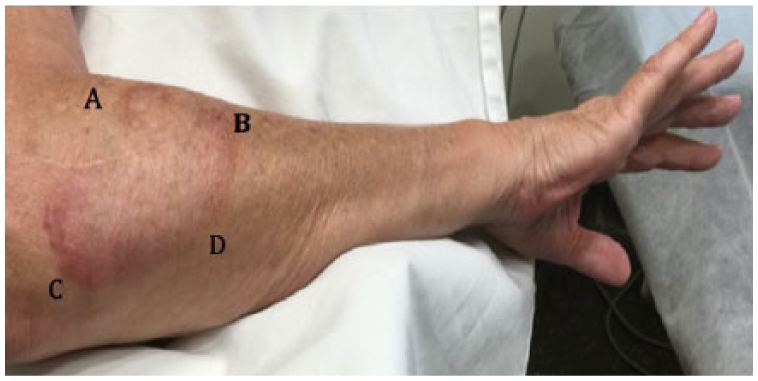
Large patch of localised GA to the lateral forearm. Points A, B, C and D outline the geographic distribution of the GA corresponding to the pleated defect of the plastic orthosis.
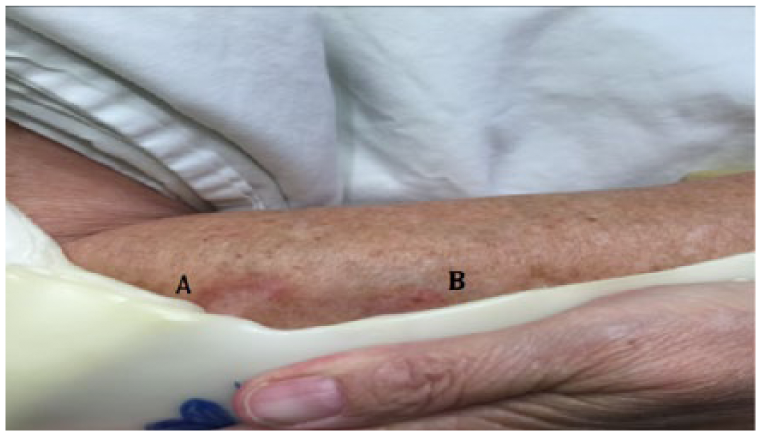
Plastic elbow orthosis with pleated ridge defect corresponding to arcal line of the GA along points A and B.
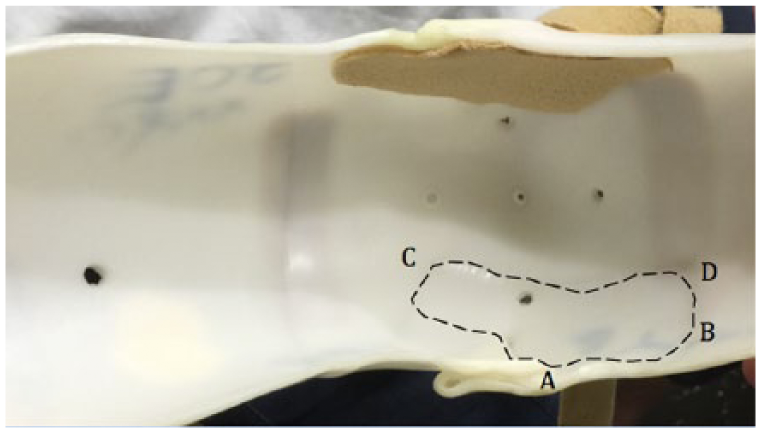
Pleated ridge defect demonstrated from the inside of the plastic elbow orthosis.
A 4-0-mm-punch biopsy of the lesion was obtained for histological examination, which demonstrated granulomatous and perivascular inflammation of the superficial and mid-dermis composed of palisading histiocytes around regions of necrobiosis with increased mucin deposition (Figures 4 to 6) in keeping with a diagnosis of a GA. The patient’s laboratory findings (full blood count, urea, electrolytes, creatinine, liver function test, lipids, thyroid function, blood glucose and HbA1c) showed a blood glucose of 8.3 mmol/L and a corresponding HbA1c of 8.7. All other laboratory findings were within normal limits including the fasting lipid panel and thyroid function test.
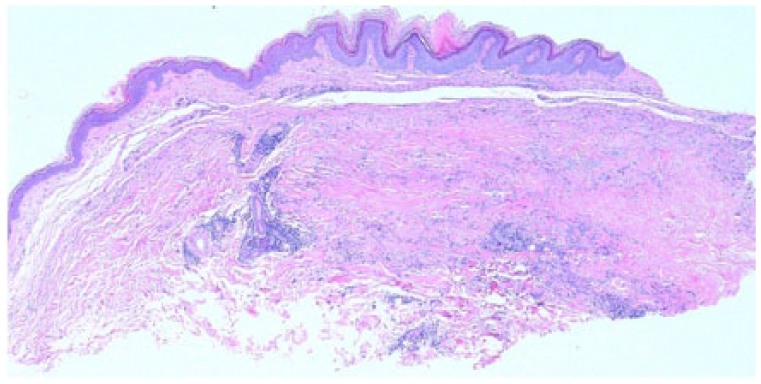
Low power (4×) demonstrating granulomatous inflammation along with hypertrophy of the epidermis.
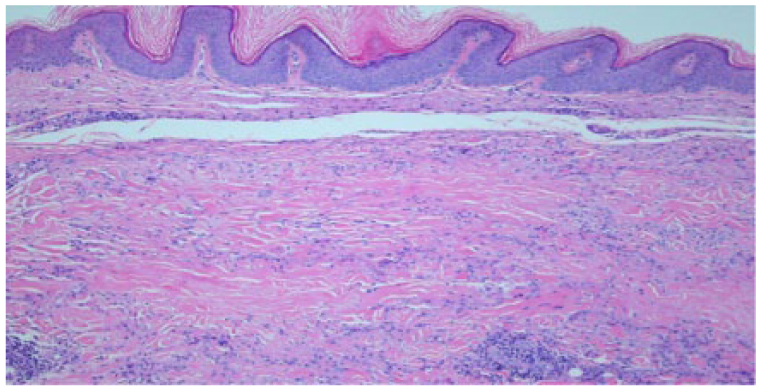
Low power (10×) demonstrating granulomatous and perivascular inflammation with necrobiosis of annular lesion.
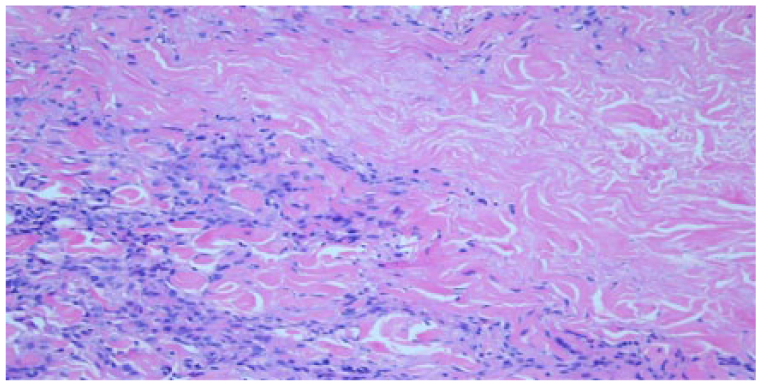
Higher power (20×) demonstrating palisading histiocytes around regions of necrobiosis and increased mucin deposits.
The patient was subsequently commenced on betamethasone dipropionate ointment 0.05% topical steroid applied to the patch GA once per day under an occlusive dressing using DuoDERM. Three months after initiation of treatment, the patient’s GA was improving with less erythema and palpable induration. The patient also reported resolution of episodes of pruritis after commencing the 0.5% betamethasone dipropionate ointment.
Discussion
GA is a relatively common skin disease with no clear aetiological or pathogenic cause. The published literature describes numerous contributing factors increasing the risk of developing GA including diabetes, thyroid disease, dyslipidaemia, malignancy, hepatitis and HIV.4,5 While our patient demonstrated poorly controlled diabetes as evident by their elevated blood sugar and high HbA1c, this would have predisposed her to generalised form of GA. Conversely, our patient’s presentation was consistent with episodes of intermittent, localised pressure from a pleated ridge defect in her elbow splint leading to the development of a significant patch of localised GA on the forearm. Moreover, our patient also returned a normal fasting lipid panel and normal thyroid function test, thus excluding these as a possible cause of her GA.
As seen in Figure 3, our patient’s elbow cast has a significant defect outlined along points A, B, C and D with Figure 2 demonstrating an arcal line of the GA corresponding to the pleat defect in the elbow orthosis along points A to B. While the literature describes an association of localised GA to occur in regions of trauma, 3 no studies or case reports were found documenting pressure-induced GA from an orthosis or cast. Despite the elbow orthosis being moulded from high-density polyethylene, we do not believe it leeched chemical onto the skin that could have induced our patient’s patch GA, especially with no cases reported in the current literature. As such, we believe it was solely the mechanical pressure from the orthosis pleated ridge that was responsible for the development of our patient’s patch of GA.
While no specific treatment exists to treat GA, application of high-potency topical steroids is usually first choice often improving the clinical course of the disease. 3 Other reported treatments of GA include injection of intralesional steroids with triamcinolone and systemic agents using oral steroids while some cases reported use of biologic agents, namely, adalimumab and etanercept in the more persistent cases.3,6–8 Of the GAs that do not respond to topical steroids or systemic agents, clinical reports of cryotherapy, phototherapy, laser therapy and even narrow band UVB (NB-UVB) have been efficacious.7–9 In the more resistant forms of GA, surgical excision has been documented with good cosmetic outcome. 10 Fortunately, after 3 months of 0.5% topical betamethasone dipropionate ointment under an occlusive duoderm dressing, our patient’s GA improved both symptomatically and clinically preventing the need for more invasive treatment.
Conclusion
This case of localised GA highlights the clinical importance of identifying pressure-induced GA. In particular, extra attention should be afforded to cast/orthosis selection and the manufacturing process in patients with a known history of inflammatory skin disorders in minimising or preventing additional episodes of GA.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manu-script.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.