
Abstract
Background:
Core stabilization training is used to improve postural balance in musculoskeletal problems.
Objectives:
The purpose of this study was to investigate the effectiveness of stabilization training in adolescent idiopathic scoliosis.
Study design:
A randomized controlled trial, pretest–posttest design.
Methods:
In total, 25 subjects with adolescent idiopathic scoliosis were randomly divided into two groups: stabilization group (n = 12) and control group (n = 13). The stabilization group received core stabilization in addition to traditional rehabilitation, and the control group received traditional rehabilitation for 10 weeks. Assessment included Cobb’s angle on radiograph, apical vertebral rotation in Adam’s test, trunk asymmetry (Posterior Trunk Symmetry Index), cosmetic trunk deformity (Trunk Appearance Perception Scale), and quality of life (Scoliosis Research Society-22 questionnaire).
Results:
Inter-group comparisons showed significantly greater improvements in the mean change in lumbar apical vertebral rotation degree and the pain domain of Scoliosis Research Society-22 in the stabilization group than those in the control group (p < 0.05). No significant differences were observed for other measurements between the groups; however, trends toward greater improvement were observed in the stabilization group.
Conclusion:
Core stabilization training in addition to traditional exercises was more effective than traditional exercises alone in the correction of vertebral rotation and reduction of pain in adolescent idiopathic scoliosis.
Clinical relevance
Stabilization exercises are more effective in reducing rotation deformity and pain than traditional exercises in the conservative rehabilitation of adolescent idiopathic scoliosis. These improvements suggest that stabilization training should be added to rehabilitation programs in adolescent idiopathic scoliosis.
Keywords
Background
Adolescent idiopathic scoliosis (AIS) is present in 2%–4% of children and occurs in 10-year-old children to maturity. In AIS, improper mechanical forces acting on the spine lead to biomechanical and physiological alterations along the trunk segment. 1 The trunk is the core segment of the body that controls the center of gravity and maintains postural stability. 2 Impaired neuromuscular control of the trunk segment and the postural asymmetry observed in patients with AIS may alter the motor control of the trunk segment leading to decreased postural stability during movement. 3
Poor balance, decreased postural control, and increased body sway have been recorded in AIS. 3 The deep trunk muscles (transversus abdominis and multifidus) play an essential role in maintaining postural stability. 4 Activation of these muscles in a feed-forward mechanism minimizes changes in the center of gravity. Therefore, pathological muscle alterations may lead to impaired postural control changes in AIS. Many studies have confirmed the altered muscle properties in AIS. Muscle imbalance in the lumbar multifidus and deep paraspinal muscles has been recorded. 5 Muscle atrophy and alterations in muscle fiber composition have been demonstrated to be leading to these muscle imbalances. Paravertebral muscle atrophy has been characterized with increased fatty infiltration. 6 Alterations in fiber composition of the spinal muscles have been shown to include reduced type I fibers and increased type IIB and IIC fiber compositions in both the convex and concave sides of the curve. 7 Weiss 8 hypothesized that a decrease in the type I fibers in the postural muscles causes inability to maintain tonic contraction for long periods of time, leading to postural deficits in AIS. In addition, Zoabli et al. 9 reported imbalance in the electromyography (EMG) activity with muscle volume differences between the left and right sides of the spine in scoliosis.
Rehabilitation exercises involving deep trunk muscles may increase postural stability and decrease postural asymmetries. Core stabilization (CS) is a recently developed exercise approach aimed at improving postural balance and preventing compensatory movements by controlling the position of the trunk in static postures and functional activities.2,4,10 CS has been reported to improve muscle imbalance, particularly between the multifidus and paraspinal muscles, thus enhancing local and global spinal stability. 11 CS has been found to be more effective than general fitness exercises for improving spinal stabilization. 12 Shin et al. 13 found that CS exercises increased sitting balance in AIS. Alves de Araujo et al. 14 reported improvements in Cobb’s angle and pain scores.
There are several scoliosis-specific exercise methods including Schroth, scientific exercise approach to scoliosis (SEAS), and general exercise programs such as yoga and pilates. A recent Cochrane review reported that a very low-quality evidence supports that scoliosis-specific exercises could reduce curve progression and brace prescription compared to traditional physiotherapy. 15
CS increases the recruitment efficiency of the stabilizing muscles around the spine, thereby improving the ability of the core muscles to correct and maintain the alignment of the spine. 16 However, there are limited studies demonstrating the effectiveness of CS in patients with AIS. The objective of this study was to investigate the effect of CS on curve magnitude, posture, trunk deformity, and quality of life in patients with AIS.
Methods
Participants
The study participants comprised patients who were diagnosed with AIS and referred by their physician to receive a spinal brace and exercise treatment at the School of Physiotherapy and Rehabilitation of Hacettepe University. Inclusion criteria were adolescents with idiopathic scoliosis between the ages of 10 and 16 years who were referred for a spinal brace. Patients with a history of rheumatological, neuromuscular, cardiovascular, pulmonary, or renal diseases were excluded. In addition, those with congenital scoliosis or spinal deformity, those who had undergone surgical correction of the spine, who had a tumor, who were unable to participate in the supervised sessions, or those who refused to follow treatment were excluded.
This study proposal was approved by the Research Ethics Board of Hacettepe University. On their first visit, patients with AIS were informed about the study. All patients and their families signed informed consent prior to the study. Patients were blinded to the type of exercise intervention that they were going to receive.
Study design
Patients were randomly divided (using simple randomization) into either a stabilization group or a control group. Patients in both groups received 20 sessions of a 1 h supervised treatment program two times per week for 10 weeks. For supervised exercises, the stabilization group received CS exercises, and the control group received traditional exercises. Both groups also performed daily home exercises. In addition to these interventions, custom-made spinal braces were designed for all the patients, and they were instructed to wear them 22 h daily.
Intervention
Traditional and stabilization exercises were performed by a trained physical therapist (first author (G.G.)). The control group received a traditional treatment program that included exercise training and bracing. Traditional exercise programs for scoliosis include breathing exercises, posture training, spinal flexibility exercises, stretching exercises for the involved muscles (especially for the concave side of the curve), and general strengthening exercises for the main muscle groups of trunk, pelvis, and shoulder girdle muscles (especially for the convex side of the curve). 17 The program progressed in accordance with the functional improvement of each patient. Spinal bracing is one of the most important components of traditional treatment in patients with AIS who have a curve of above 20°. 18 In this study, custom-made spinal braces were designed for the patients in order to correct the lateral deviation and rotational components of the scoliotic deformity. 19 A thoraco-lumbo-sacral brace was designed based on the symmetric, patient-oriented, rigid, three-dimensional, active (SPoRT) concept. 20 The brace-wearing protocol involved 22 h of brace wearing and 2 h of removal for hygienic activities and exercise.
The stabilization group received CS exercises in addition to the traditional treatment program. The CS training principles comprise respiratory control, neutral spinal position, rib cage placement, scapular position, and neck–head position. The CS training program included local muscle stability training (transversus abdominis, multifidus, and diaphragm), global muscle stability training (oblique abdominal muscles, psoas major, quadratus lumborum, and pelvic floor muscles), global muscle mobility training (rectus abdominis, back extensors, and hamstring muscles), and strength training of the core muscles through the thoracolumbar fascia by maintaining the neutral spine position. Diaphragmatic breathing technique was used during exercises. Exercises gradually progressed from the training of the core muscles in static body positions to the training of activation of the core muscles during functional tasks in dynamic body positions. The patients proceeded to the next level when they successfully completed the weekly program. Patients who could not manage to complete the program continued with the same exercises and performed a few simple exercises from the next level with fewer repetitions.
Assessments
Demographic data and patient characteristics, including age, gender, height, body mass, Risser sign, and curve pattern, were collected. Skeletal immaturity based on the Risser stages was recorded for each patient at the first visit. Curvatures were classified according to the King classification system. The following outcome measures were performed before and after 10 weeks of intervention in both groups: curve magnitude with the measurement of the Cobb angle on antero-posterior radiograph, apical vertebral rotation (AVR) with a scoliometer in Adam’s test, trunk asymmetry with the Posterior Trunk Symmetry Index (POTSI), cosmetic trunk deformity with the Trunk Appearance Perception Scale (TAPS), and quality of life with the Scoliosis Research Society-22 questionnaire (SRS-22).
The Risser sign provides information about the skeletal maturity and spinal growth. It is based on the ossification of the iliac apophysis, which is evaluated with a four-grade scale from 0 (no ossification) to 5 (fused ossified apophysis). 21
King classification system includes five types of curve definitions based on the location of the curve apex and flexibility on X-ray as follows: Type 1: double curve, lumbar curve larger and stiffer than the thoracic curve; Type 2: double curve, thoracic curve larger and stiffer than the lumbar curve; Type 3: single thoracic curve; Type 4: long thoracic curve with L4 tilted into the curve; and Type 5: double thoracic curve. 22
Lateral curvature of the spine was measured with the Cobb method on the antero-posterior radiograph in degrees. The rotation of the apical vertebrae of the curve was measured in degrees using a scoliometer in the Adam’s forward-bending test. 23 The change in AVR was reported to be ⩾5° in order to have clinical significance. 24
TAPS was used to assess the perceived body image and to evaluate the outcome of the interventions on cosmetic deformity. TAPS comprises three sets of figures. Each figure is scored from 1 (greatest deformity) to 5 (smallest deformity). The mean score expresses the average of three drawings. 25 POTSI was used to quantify trunk asymmetry with photographic assessment of posture. It is a two-dimensional surface topography system, which is based on the measurements taken from the patient’s back with a tapeline. The total POTSI score is calculated as the sum of six indices, that is, three frontal asymmetry indices and three height difference indices. 26
The SRS-22 questionnaire has been used to evaluate quality of life. It consists of 22 questions covering five domains: pain, self-image, function/activity, mental health, and management satisfaction. Each item is scored from 1 (worst) to 5 (best). Each domain has its own scoring system. A total score is calculated from the average of the five domains. This tool has good to excellent internal consistency and test–retest reliability. 27
Compliance with the treatment was assessed using patients’ self-reports. For exercises, the question was “Did you perform your exercise for 1 h daily?” For the braces, the question was “Did you wear your spinal brace 22 h daily?” Patients were requested to rate themselves out of a score of 100%, and the results were recorded as a percentage.
Statistical analysis
Statistical power analyses based on the information from previous studies (for our primary outcome measurement method of Cobb’s angle)13,28 were used to determine the optimum sample size. The number of subjects required for the final analysis was calculated to be 10 for each treatment group with a 20% missing rate. The α-level used in determining the sample size was 0.05, and the ideal power was considered to be 80%. Descriptive statistics were expressed as means and standard deviations (SDs). Fisher’s exact test was used to determine whether patients were equally distributed across the two groups in terms of gender and King classification categories. Differences observed with interventions were analyzed with the Wilcoxon signed-rank test. Between the groups, differences were compared using the Mann–Whitney U test. A level of significance of p < 0.05 was accepted for the study. All analyses were performed using SPSS for Windows version 11.0 (SPSS Inc.).
Results
Among the 44 patients admitted to the department, 25 fulfilled the inclusion criteria. In all, 19 patients could not participate in the study because of the following reasons: five patients refused to participate, six had a history of previous conservative treatment, and eight were unable to attend the supervised sessions. The study was completed with 25 patients (12 in the stabilization group and 13 in the control group) with 100% attendance compliance (Figure 1).
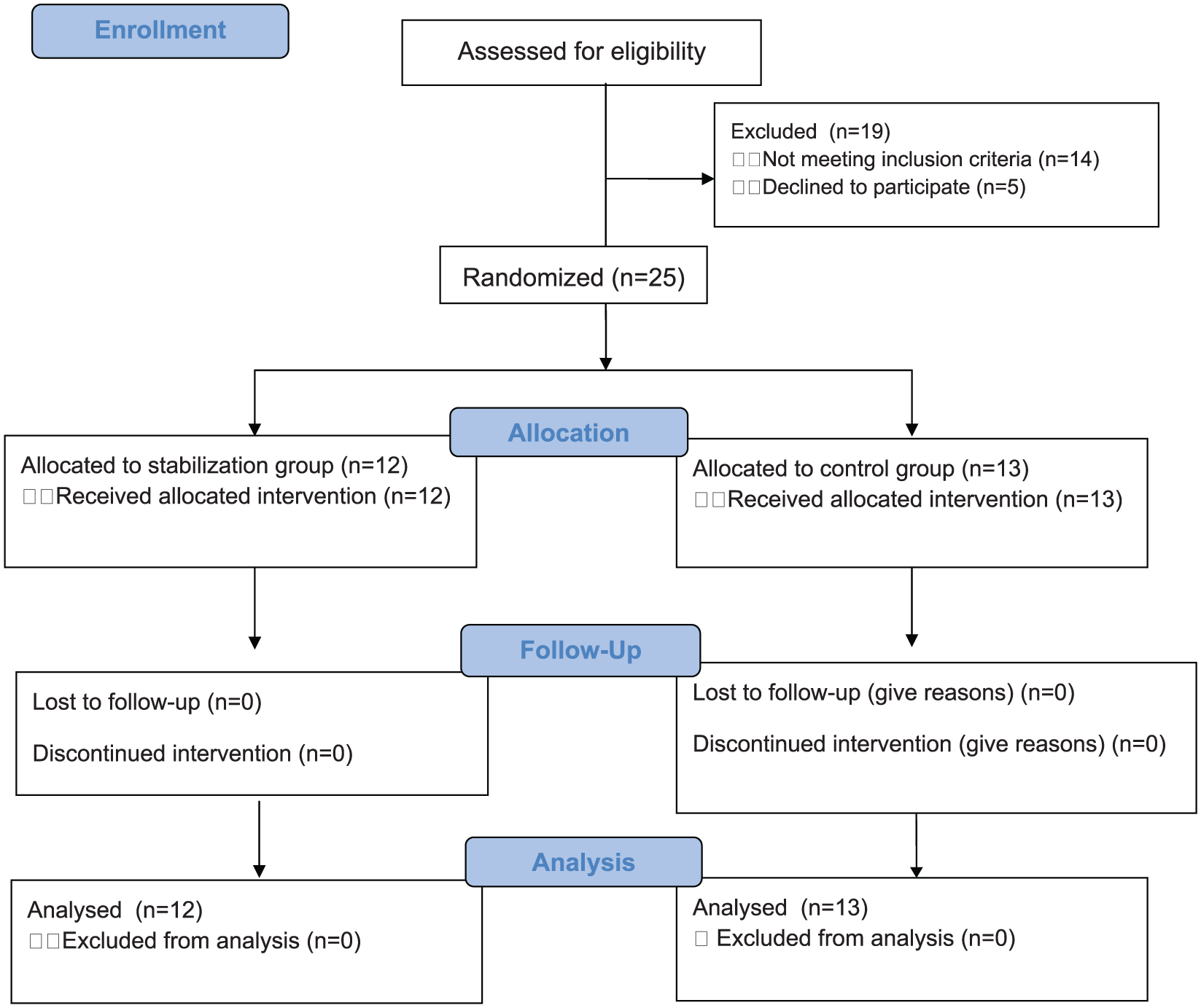
Flow diagram for participant enrollment, allocation, follow-up, and analysis.
There were no between-group differences regarding the baseline characteristics (p > 0.05) (Table 1). Compliance with home exercises (82.25 ± 15.33 for the stabilization group, 88.05 ± 15.08 for the control group, p = 0.216) and brace wearing (86.92 ± 9.88 for the stabilization group, 88.8 ± 13.03 for the control group, p = 0.586) did not differ between the groups.
General characteristics of the patients.
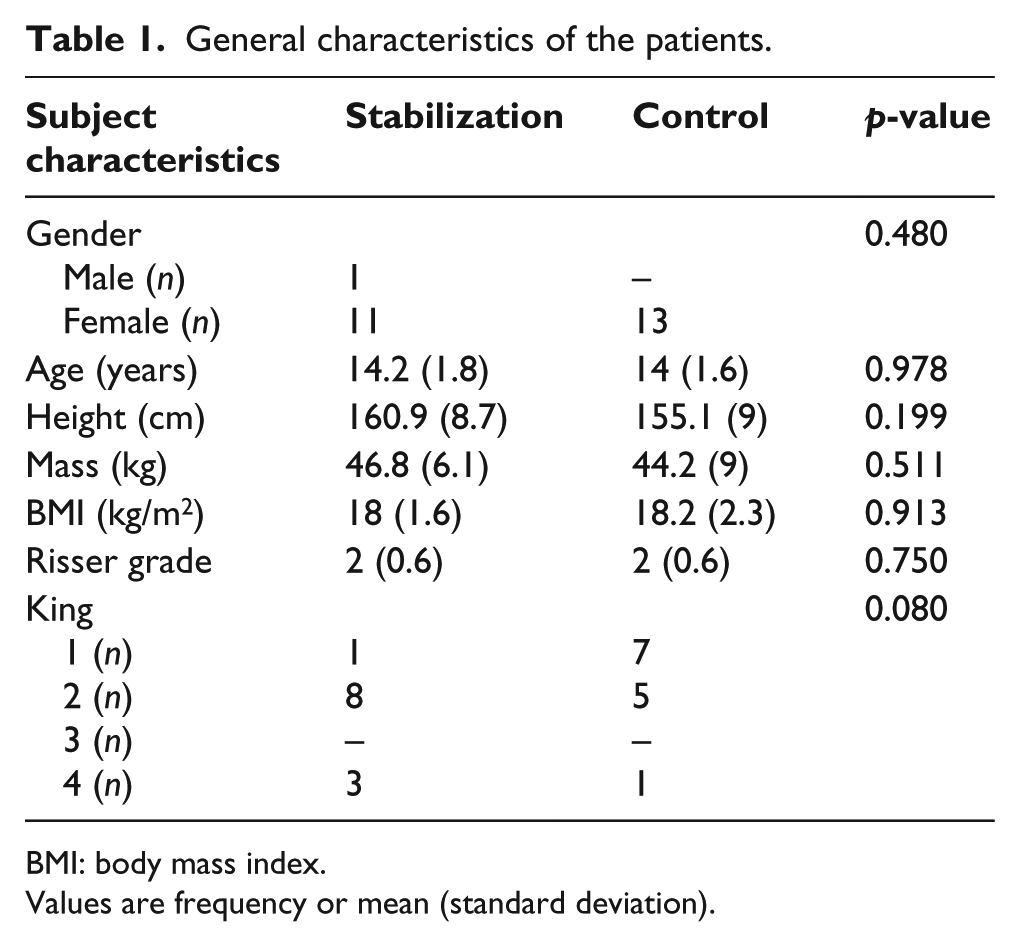
BMI: body mass index.
Values are frequency or mean (standard deviation).
On comparing all the parameters, the baseline values did not differ between the groups (p > 0.05) (Tables 1 and 2). An inter-group comparison revealed significantly greater improvements in lumbar rotation and the pain domain of SRS-22 (p < 0.05) (Table 2). The mean change (SD) in the degree of lumbar rotation between pre- and post-treatment was a reduction of −3.89 (2.09) in the stabilization group and −2.09 (2.02) in the control group. In addition, the mean change in the pain domain of SRS-22 between pre- and post-treatment was an improvement of 0.27 (0.40) in the stabilization group and a worsening of −0.05 (0.59) in the control group (p < 0.05) (Table 2). No significant differences were observed for Cobb’s angle, rotation, trunk asymmetry, cosmetic trunk deformity, and quality of life between the two groups; however, trends toward improvement were observed in all measures for the patients in the stabilization group (Table 2).
Main outcome measures by group at the pre- and post-treatment assessments.
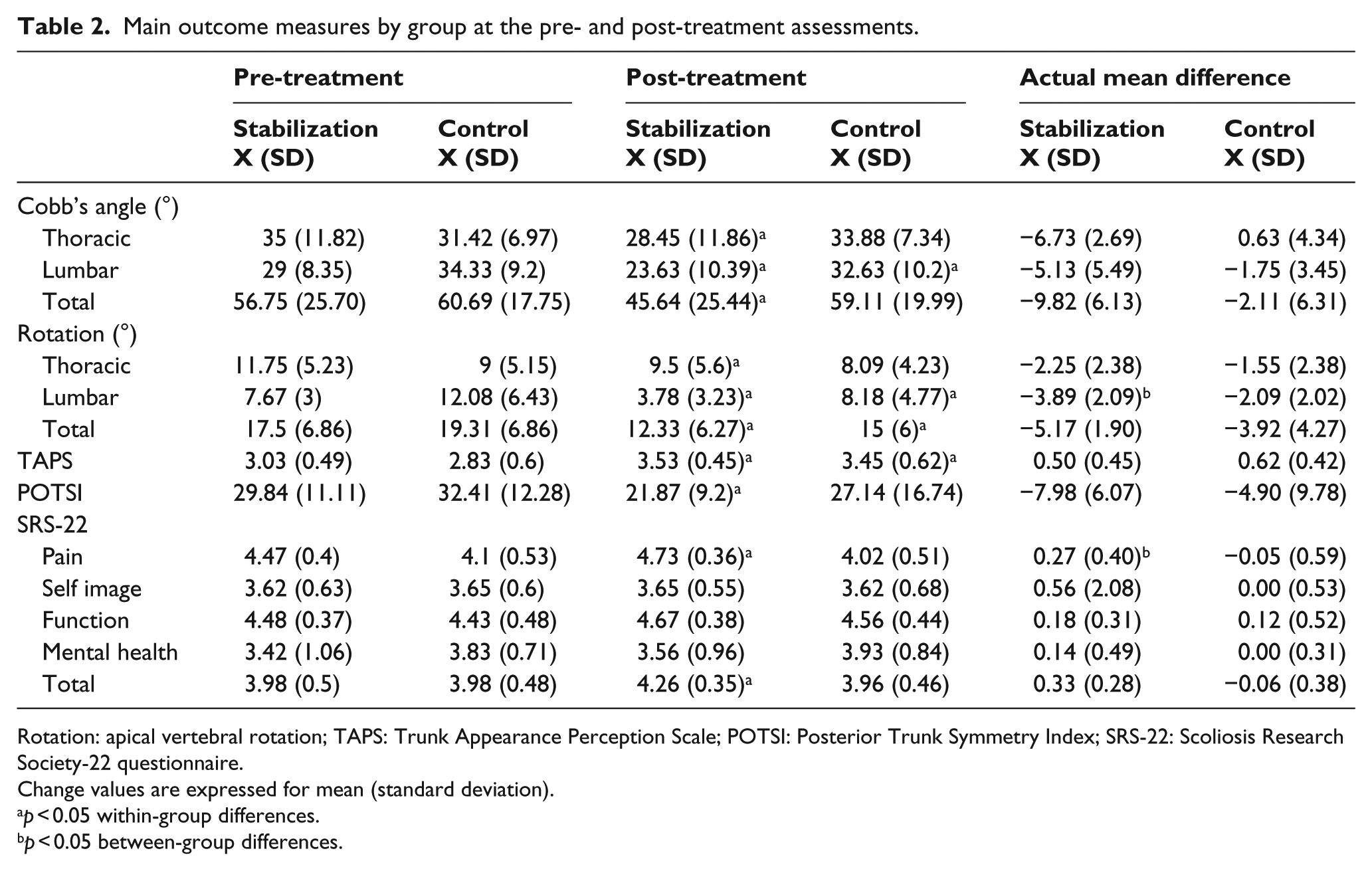
Rotation: apical vertebral rotation; TAPS: Trunk Appearance Perception Scale; POTSI: Posterior Trunk Symmetry Index; SRS-22: Scoliosis Research Society-22 questionnaire.
Change values are expressed for mean (standard deviation).
p < 0.05 within-group differences.
p < 0.05 between-group differences.
Discussion
The results of this study showed that CS training is effective in reducing AVR and pain in patients with AIS. In addition, stabilization exercises are more effective than traditional exercises in reducing lumbar rotation deformity as measured by scoliometer. This is the first study investigating the effects of conservative treatment, including CS training and spinal bracing using outcomes of scoliosis as parameters, such as body posture, trunk deformity, pain, and quality of life in AIS.
Treatment strategies, which trigger the prevention of scoliosis progression and reduce the rate of surgery, are crucial in patients with AIS. 29 Measurement of the curve magnitude with the Cobb method and AVR is decisive in determining scoliosis progression. 30 In this study, CS training was more effective in the reduction of AVR of the lumbar region. For the chaos theory of scoliosis, the scoliotic curve represents a discontinuous system. For a rotation below 25°, the lever arms of the muscles on the concave and convex sides are around the instant rotation center of the vertebral body and enable the stability of the spine; for this movement, all the spinal muscles attempt to correct the scoliosis. If the rotation exceeds 25°, the lever arms of the concave and convex muscles are on the same side with relation to the instant rotation center of the vertebral body. Therefore, contraction of the stabilization muscles creates a rotator effect which causes worsening of scoliosis. 31 We think that reduction in vertebral rotation is associated with neuromuscular retraining around the spine and re-education of the spinal muscles’ ability to stabilize the curve against rotation with core training. 4 Previous studies mainly investigated the effect of intervention on Cobb’s angle. Authors obtained a reduction in Cobb’s angle with pilates-based exercises 14 and reported a greater correction of Cobb’s angle in scoliosis with the core muscle release technique than with general exercise and electrotherapy. 32 Negrini et al. found that SEAS exercise was more effective than traditional physiotherapy for reducing curve progression. The average Cobb angle was reduced 3° in SEAS group, whereas it stayed unchanged in traditional physiotherapy group. 33
Weiss et al. 34 reported better results with 35 months of treatment in scoliosis-intensive rehabilitation (Schroth method) group (53%–70% improvement) versus control group (29%–44% improvement). In this study, we did not find any significant improvement in Cobb’s angle in the stabilization group. However, the trend toward better results in the thoracic and total Cobb angle in the stabilization group suggests that further research should be conducted. The total Cobb angle reduced on average 9° and 2° in the CS and control groups, respectively.
The treatment of AIS has been reported to be aimed at improving cosmetic appearance and trunk balance. 35 TAPS is used to assess trunk deformity and self-image. TAPS has excellent internal consistency, test–retest reliability, and a good capacity for differentiating the severity of the disease in AIS. 25 We used TAPS to assess the treatment effects on visible aspects of the patients’ spinal deformity. Furthermore, while traditional methods like the Cobb angle focus on evaluating internal deformity of the spine, POTSI assesses the external shape of the trunk in terms of asymmetry. 26 In this study, stabilization training did not result in significant improvement in cosmetic deformity and trunk symmetry. However, in the POTSI measurements, the trend toward improved body symmetry within the stabilization group could be related to a previous review, which indicated that pilates-based spinal stabilization exercises produced postural facilitation and straightening of the spine by assisting the reactivation of spinal muscles. 36 Shin et al. 13 demonstrated that CS exercises could improve sitting balance in AIS and suggested that this was caused by improvement in trunk muscle strength and trunk symmetry. Emery et al. 16 reported that pilates therapy improved core strength, scapulae kinematics, and spine posture by facilitating postural symmetry. Our initial results showed that traditional exercise training is not sufficient to reduce body asymmetry.
It has been suggested that quality of life should be taken into account during treatment because scoliosis affects quality of life. 37 SRS-22 is a commonly used self-report scale for assessing the quality of life in scoliosis. A preliminary study reported a higher complaint rate of back pain in patients with scoliosis than in healthy individuals. 38 In the natural course of scoliosis, due to asymmetrical loading on the spine, intervertebral disc and facet joint degeneration and differences in spinal muscle length occur, leading to chronic pain. Therefore, for the conservative treatment of AIS, pain relief is considered to be important. 38 In this study, CS training was found to improve the pain domain of SRS-22. This suggests that stabilization training improved the global musculature and its ability to balance the loads on the body. In addition, it improved the local musculature and its ability to maintain force control within the spine. This increase in the spinal stability may provide painless movements in the routine functional tasks. A review has reported the effectiveness of stabilization exercises in reducing pain in a heterogeneous group of patients with lower back pain. 39 Using the pilates method, Alves de Araujo et al. 14 observed reduction in back pain in scoliosis. In addition, a trend toward improvement in the quality of life with stabilization training was observed. We propose that with pain-free movements, CS training provides confidence to individuals to use their spine for physical activities, and this improves their quality of life. Traditional exercises were insufficient in improving quality of life and pain. These results are not comparable with previous studies because in the literature, these studies mostly compared quality of life and pain between patients who were surgically treated and/or treated with braces. 35 Few studies have investigated the effects of exercise on quality of life in AIS, and they all differ in terms of patient characteristics, procedures, and study settings. Monticone et al. 17 reported that active self-correction and task-oriented exercises were superior to traditional exercises in improving quality of life in mild scoliosis. Unlike our study, Vasiliadis and Grivas 37 reported that quality of life in patients with AIS was negatively affected by conservative treatment, including braces and exercises. It has been previously reported that stabilization training improves quality of life in patients with lower back pain; 40 however, there has been no comparable study in scoliosis. In addition, there is no study which reported on the efficacy of scoliosis-specific exercises to improve cosmetic problems, quality of life, disability, pain, and physiological issues in recent Cochrane review. 15
This study included an AIS population which was close to skeletal maturity (Average 14 years and Risser 2). The CS training intervention might be more significant in younger patients (lower Risser sign) with AIS who have high risk of curve progression. However, there were some limitations in this study. We did not objectively measure the patients’ ability to contract the core muscles properly. In addition, compliance to home exercises and wearing of braces was subjective. Although change in lumbar AVR was statistically significant, the clinical significance was questionable (small magnitude of rotational change < 5°). However, positive change in lumbar AVR with stabilization training showed that CS training is a promising approach especially to treat lumbar AVR in patients with idiopathic scoliosis.
Conclusion
Our study indicated that CS exercises are more effective in reducing AVR and pain than traditional exercises for the conservative treatment of AIS. In addition, CS training was helpful in improving curve magnitude, trunk deformity, postural symmetry, and quality of life with trends toward better outcomes in AIS. The improvements obtained are valid for the 10 weeks of treatment (for short treatment time), and further studies are warranted with long time follow-up.
Footnotes
Acknowledgements
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Coordination Unit of Hacettepe University (project no. 014 T11 102 002).