
Abstract
Background:
A diverse range of elastomeric liner products are available to people with transtibial amputation. However, little information is available about how prosthetists select the product best suited to each patient.
Objectives:
To determine how prosthetists obtain information about liners, which features are most relevant to the selection process, and which products are used most for patients with transtibial amputation.
Study design:
Cross-sectional survey.
Methods:
A custom online survey was developed to solicit information about prosthetists’ liner selection practices. Prosthetists with experience managing transtibial patients were recruited via advertisements posted in magazines, at conferences, and on a listserv. Responses were analyzed to characterize prosthetists’ liner selection practices.
Results:
Data from 106 experienced prosthetists (mean age: 44.4 years, mean experience: 15.7 years) were included. Most prosthetists (94%) obtained liner information from manufacturer representatives, websites, or literature. On average, respondents factored nine different liner characteristics into their selection processes. Prosthetists reported experience with 16 unique liner products with their transtibial patients, but routinely used fewer than 3.
Conclusion:
Although many different prosthetic liners are available, prosthetists regularly use only a few select liner products. Tools or strategies to objectively compare prosthetic liners across manufacturers are likely needed to facilitate more diverse prescription practices.
Clinical relevance
Knowledge of prosthetists’ prosthetic liner selection practices may guide development of evidence-based resources or tools to facilitate matching patients with appropriate liners. Results of this study may also inform researchers and manufacturers about desirable liner characteristics and direct development of novel liner products to address prosthetists’ clinical needs.
Keywords
Background
The quality of socket fit is commonly acknowledged by both patients and prosthetists as the most important aspect of a prosthesis.1 –3 The prosthetic liner, which acts as an interface between the rigid socket and the delicate tissues of the residual limb, is a primary contributor to socket fit. The prosthetic liner generally serves two key functions—to protect the residual limb and to couple the limb to the prosthesis.2,4,5 The liner therefore plays a key role in achieving a well-fitting, comfortable, and functional prosthetic limb. 2
Selecting a liner for an individual patient requires careful consideration of the patient’s physical presentation, their functional status, and their personal goals. A prosthetist must also consider the liner’s design, features, and performance in order to appropriately match it to the patient’s needs. Contemporary prosthetic liners are often made of elastomeric materials (i.e. copolymer, polyurethane, silicone, thermoplastic elastomer), but vary in their chemical and physical composition. As such, liners exhibit a range of mechanical properties (e.g. coefficient of friction, compressive stiffness, shear stiffness, and tensile stiffness).5,6 These properties directly affect the liner’s ability to suspend the prosthesis on the limb, resist shear stresses that can lead to skin breakdown, accommodate limb volume fluctuations, limit pistoning, and protect bony prominences.5–7 The challenge for the prosthetist is in choosing a liner product from the many available options.
At present, there are dozens of commercial elastomeric liner products available for patients with transtibial amputation. While the availability of so many liners allows practitioners to choose the liner most appropriate for each individual patient, the great diversity of products may also challenge practitioners to stay up-to-date on available options. Regrettably, there is limited scientific evidence available to direct selection of liners for prosthetic patients. In absence of empirical evidence, it has been suggested that prosthetists’ liner selection practices are instead guided by product literature, peer recommendations, experience, or intuition. 8 However, research is needed to confirm this assumption or determine which other factors contribute to prosthetists’ selection processes. Knowledge of prosthetists’ selection practices may also help to inform development of liners with desirable characteristics or creation of resources (i.e. tools or educational materials) to assist practitioners with matching liners with specific patients.
The purpose of this study was to determine how prosthetists gained information about elastomeric liners, what liner characteristics factored into their selection decisions, and which liners were most often selected for their patients with transtibial amputation. We hypothesized that prosthetists receive information about elastomeric liners primarily from prosthetic manufacturers. 8 We also expected that prosthetists select liners based on their ability to fulfill the fundamental goals of a liner (i.e. protect the limb and suspend the prosthesis). 2 Finally, we expected that prosthetists would routinely use a small number of liners with which they have experience. 8 To address these hypotheses, we developed and administered an online survey to prosthetists in North America. Results were used to characterize prosthetists’ liner prescription practices and to identify opportunities for improving how prosthetic liners are selected for individual patients.
Methods
Participants
Prosthetists with experience providing care to lower limb prosthetic patients were recruited to participate in the study. Inclusion criteria were 21 years of age or older; eligible to provide prosthetic services in the United States or Canada; at least 1 year experience providing prosthetic services of persons with lower limb loss; and ability to read, write, and understand English. No exclusion criteria were applied. Candidate participants were identified through print advertisements in clinical magazines (e.g. O&P Edge), flyers posted at professional meetings (e.g. American Academy of Orthotists and Prosthetists Annual Meeting), and postings to the orthotic and prosthetic listserv (i.e. OANDP-L).
Survey design
An online, self-report survey (Supplementary Appendix 1) was developed to solicit information about prosthetists’ liner selection practices. Examples of specific elastomeric liner products were drawn from prosthetic distributors (e.g. SPS, Alpharetta, GA; Cascade, Chico, CA) and manufacturer (e.g. Otto Bock, Austin, TX; Össur, Reykjavik, Iceland) websites and catalogs, in consultation with clinical prosthetists. Questions were grouped according to the following categories: sources of liner product information (two questions), characteristics of importance in liner selection (one question), and use of existing liner products (nine questions). The survey also included demographic questions (e.g. sex, age, ethnicity, race) and questions related to professional experience (e.g. clinical education, certification, experience). Response options (e.g. multiple-choice, short answer) varied by question. Questions were pilot-tested with three prosthetists and feedback was used to revise questions, as needed. The survey was administered using open-source survey software (Catalyst WebQ) hosted at the University of Washington (Seattle, WA).
Survey administration
Study postings directed interested prosthetists to a website to determine their eligibility. Respondents self-screened by answering a series of questions about the study inclusion criteria (e.g. “Are you eligible to provide prosthetic services in the United States or Canada?”). Respondents who met the inclusion criteria were directed to the survey. Upon conclusion of the survey, respondents were allowed to enter a drawing for one of 10 US$50 gift cards. No identifiable information was collected, unless respondents elected to enter the drawing. The survey remained available for 2 months. All study procedures were reviewed and determined to qualify for exempt status by a University of Washington institutional review board.
Analysis
Survey records were exported from WebQ to Microsoft Excel (Microsoft, Redmond, WA) for data visualization and analysis. Survey results were screened for missing data and/or potentially invalid responses (e.g. respondents selected the same answer to all questions). Frequencies and percentages were calculated for survey questions with nominal and ordinal responses (e.g. sex and level of education); mean values and standard deviations (SDs) were calculated for questions with ratio responses (e.g. age and time in clinical practice). Responses regarding use of specific liner products were used to bin the product as “routinely used” (i.e. respondent reported using the product “always” or “often”) or “not routinely used” (i.e. respondent reported using the product “sometimes,” “rarely,” or “never”) to facilitate presentation of data. Responses to optional, open-ended questions were reviewed and summarized.
Results
Respondent characteristics
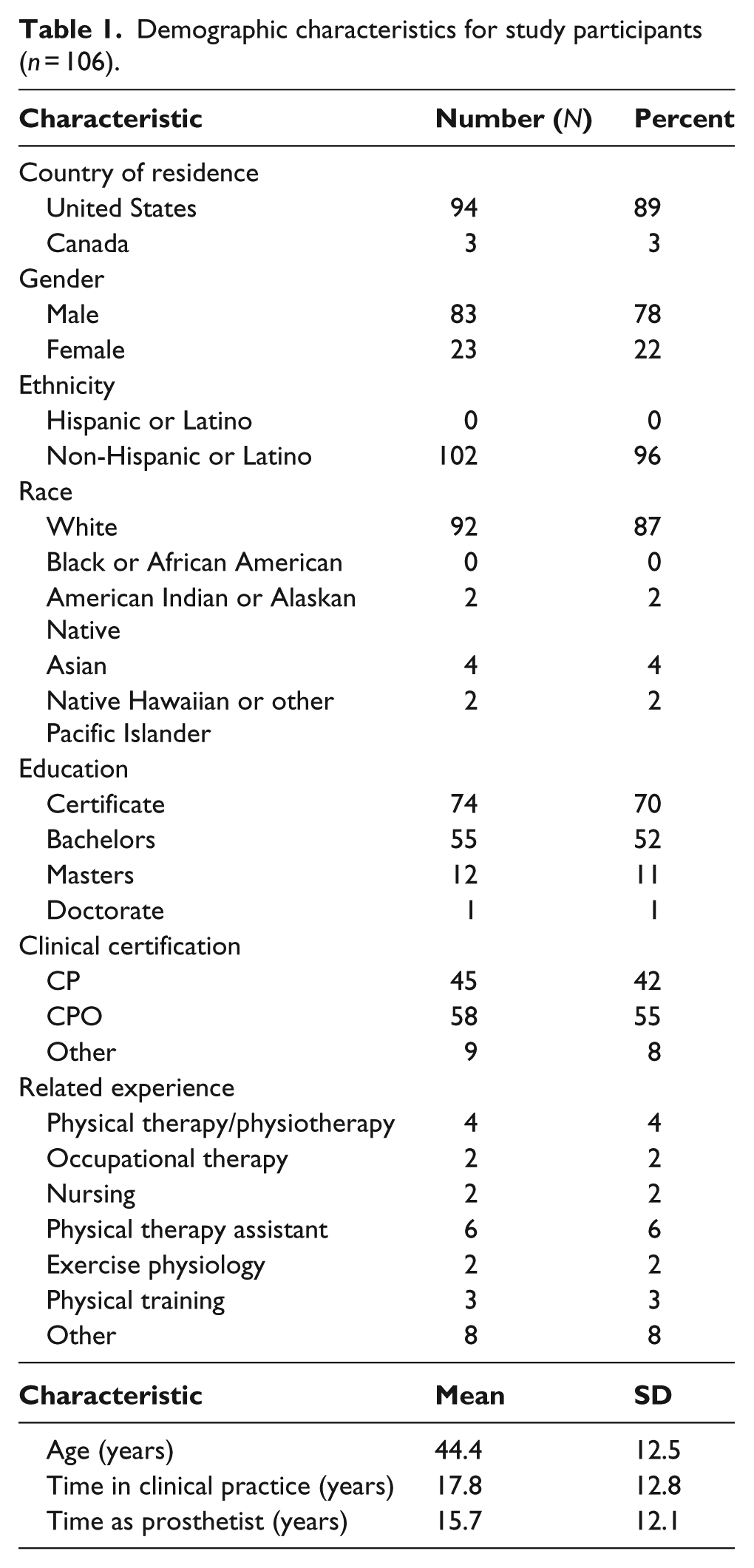
In all, 113 people responded to the survey. Seven respondents were removed from the dataset due to invalid responses. Respondents in the final dataset (n = 106, Table 1) were mostly male (78%), non-Hispanic White (87%), and US residents (89%). On average, respondents were mid-career and experienced in providing prosthetic care to people with limb loss (i.e. mean age = 44.4 years, 15.8 years in prosthetics practice).
Demographic characteristics for study participants (n = 106).
Sources of liner product information
Respondents indicated that they received information about liners from a variety of sources (Figure 1). The large majority of respondents (94%) reported that they obtained information from manufacturers (i.e. representatives, websites, or literature). Fewer reported receiving information at conferences or meetings (75%) from clinical magazines (65%) or from scientific journals (33%). A number of respondents noted (via their open-ended comments) that they also obtained information from other prosthetists (18% of respondents) and patients (5% of respondents).
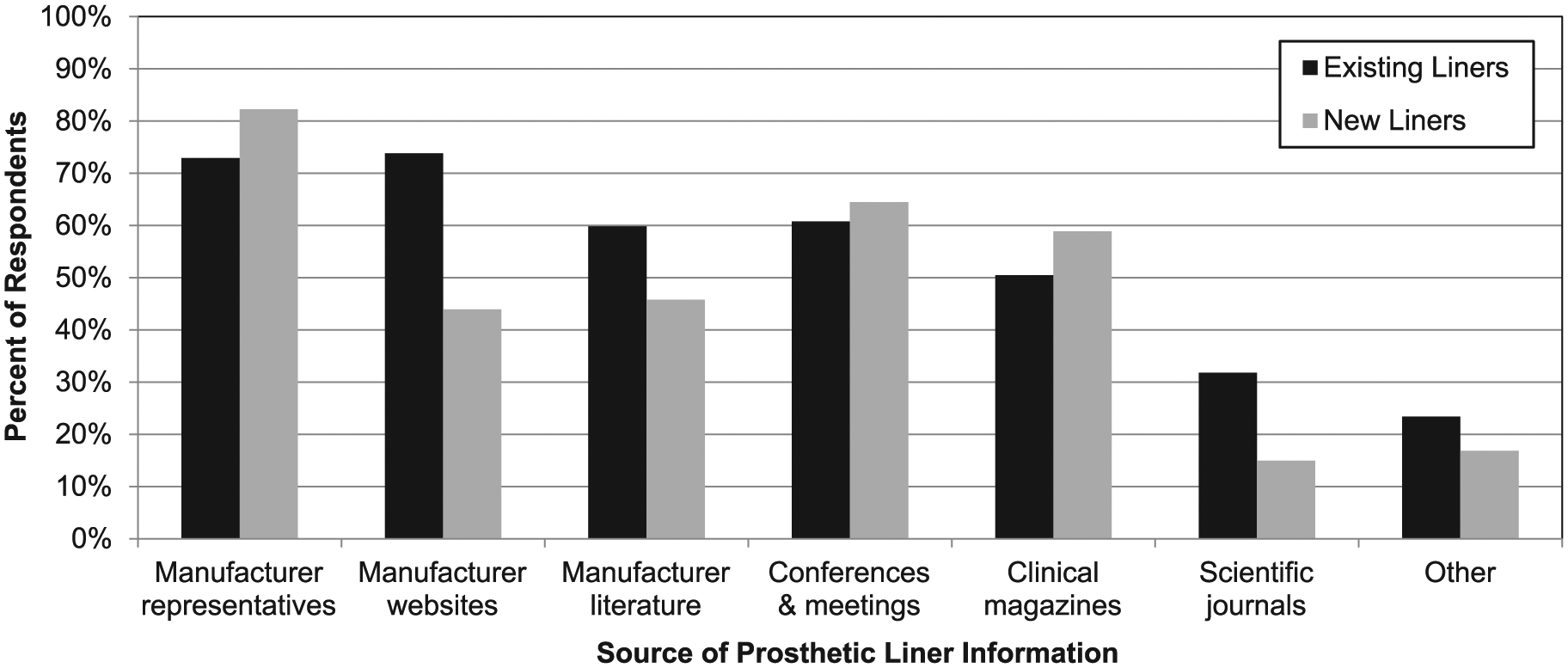
Sources of prosthetic liner information. Prosthetists identified where they obtained information about existing (black) and new (gray) prosthetic liners.
Characteristics of importance in liner selection
Prosthetists reported that a number of liner characteristics contributed to their selection process (Figure 2). On average, respondents indicated that 9 of the 22 liner characteristics included in the survey were considered when selecting a liner for their prosthetic patients. The most commonly endorsed properties included durability (91%), comfort (87%), and suspension features (78%); the least common were appearance (8%), temperature control (7%), and visual features (2%). Prosthetists noted (via open-ended comments) other characteristics that were not listed in the survey, including ease of donning/doffing (n = 6), range of knee motion (n = 2), and available sizes (n = 1). Multiple prosthetists (n = 8) noted that their priority characteristics would be dependent on the patient (e.g. limb shape, skin quality, activity level, medical history).
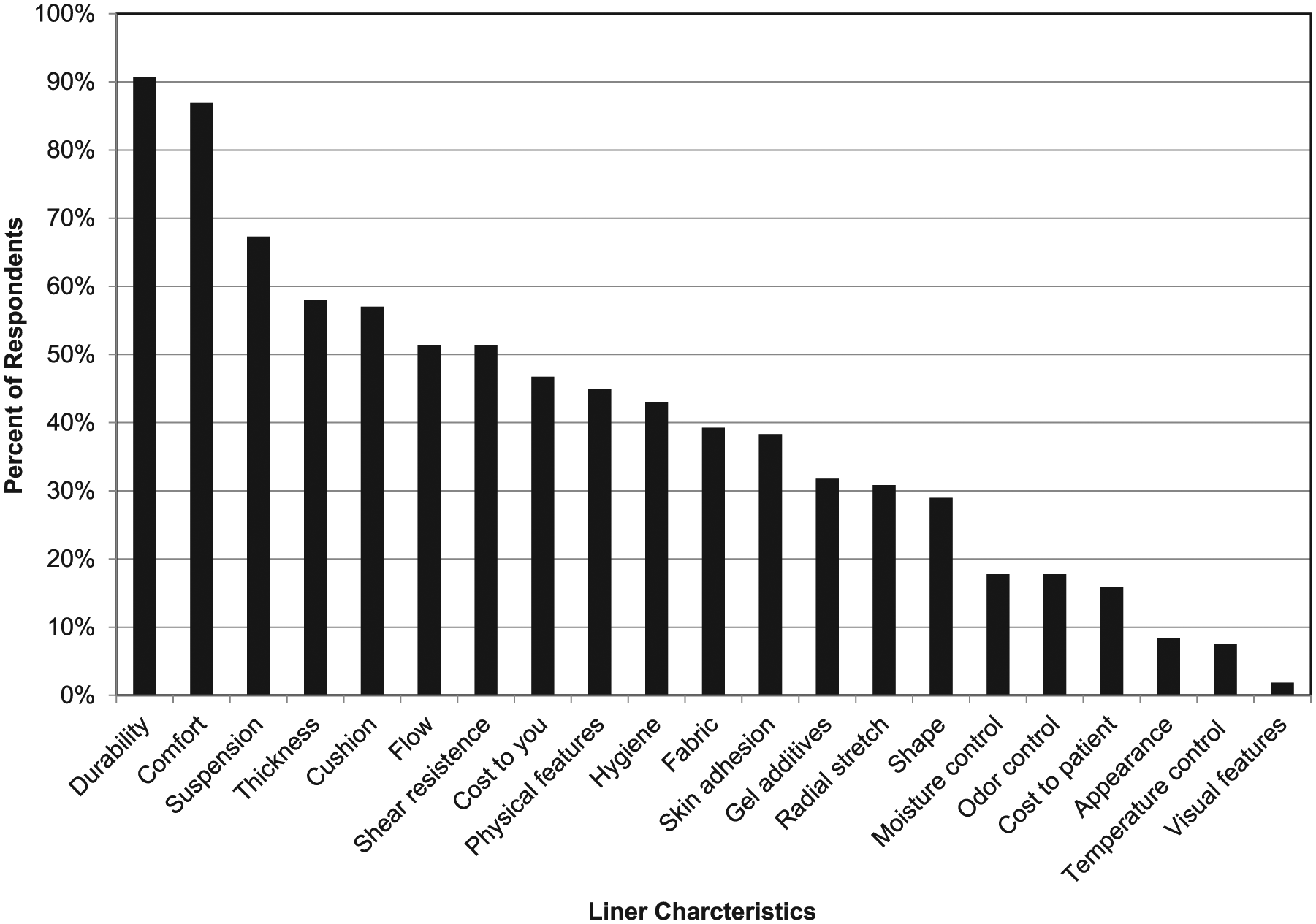
Characteristics that affect prosthetists’ selection of liner products. Characteristics are presented in order of those most commonly endorsed by surveyed prosthetists.
Use of existing liner products
On average, prosthetists reported having used 16 of the 71 liners listed on the survey with their patients, but routinely (i.e. “always” or “often”) used only 2–3 (mean = 2.6, SD = 2.0) unique liner products (Table 2). A small portion of respondents (12%) indicated they “always” used a single liner product with all their patients. Each of the 71 liner products included in the survey was used by at least two prosthetists, but no single product was used by all prosthetists. Liner products by Össur, WillowWood, ALPS, Otto Bock, and medi were among those most routinely used by prosthetists in the study (Table 3). Routinely used products were manufactured from a variety of materials, including silicone (n = 13), thermoplastic elastomer (n = 8), and urethane (n = 3).
Mean number of liner products used by prosthetists by frequency of use.
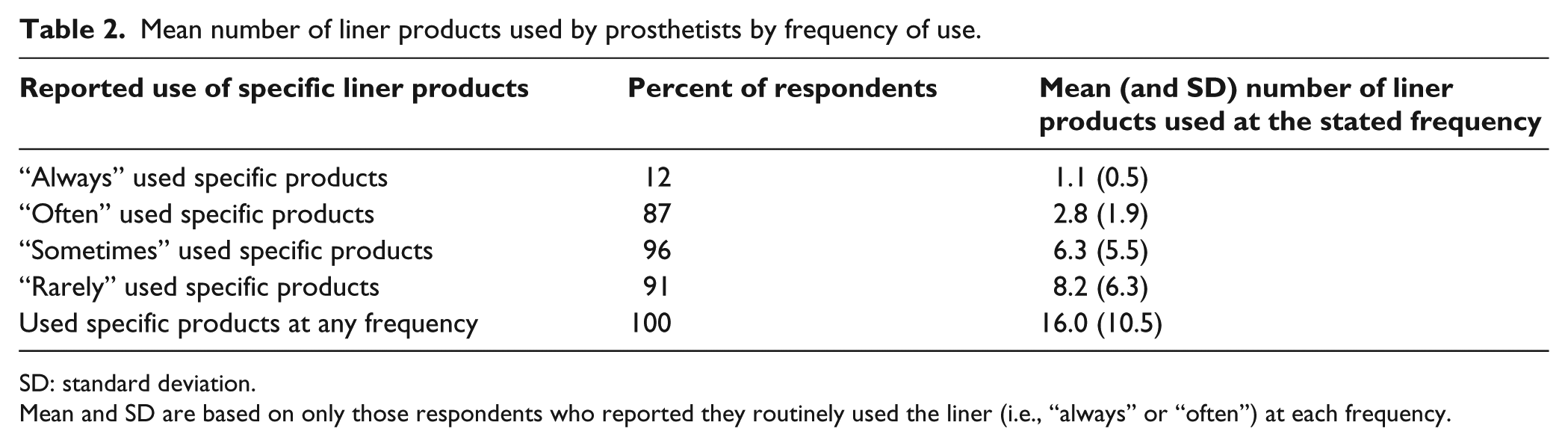
SD: standard deviation.
Mean and SD are based on only those respondents who reported they routinely used the liner (i.e., “always” or “often”) at each frequency.
Elastomeric liners most often used by prosthetists for people with transtibial amputation.
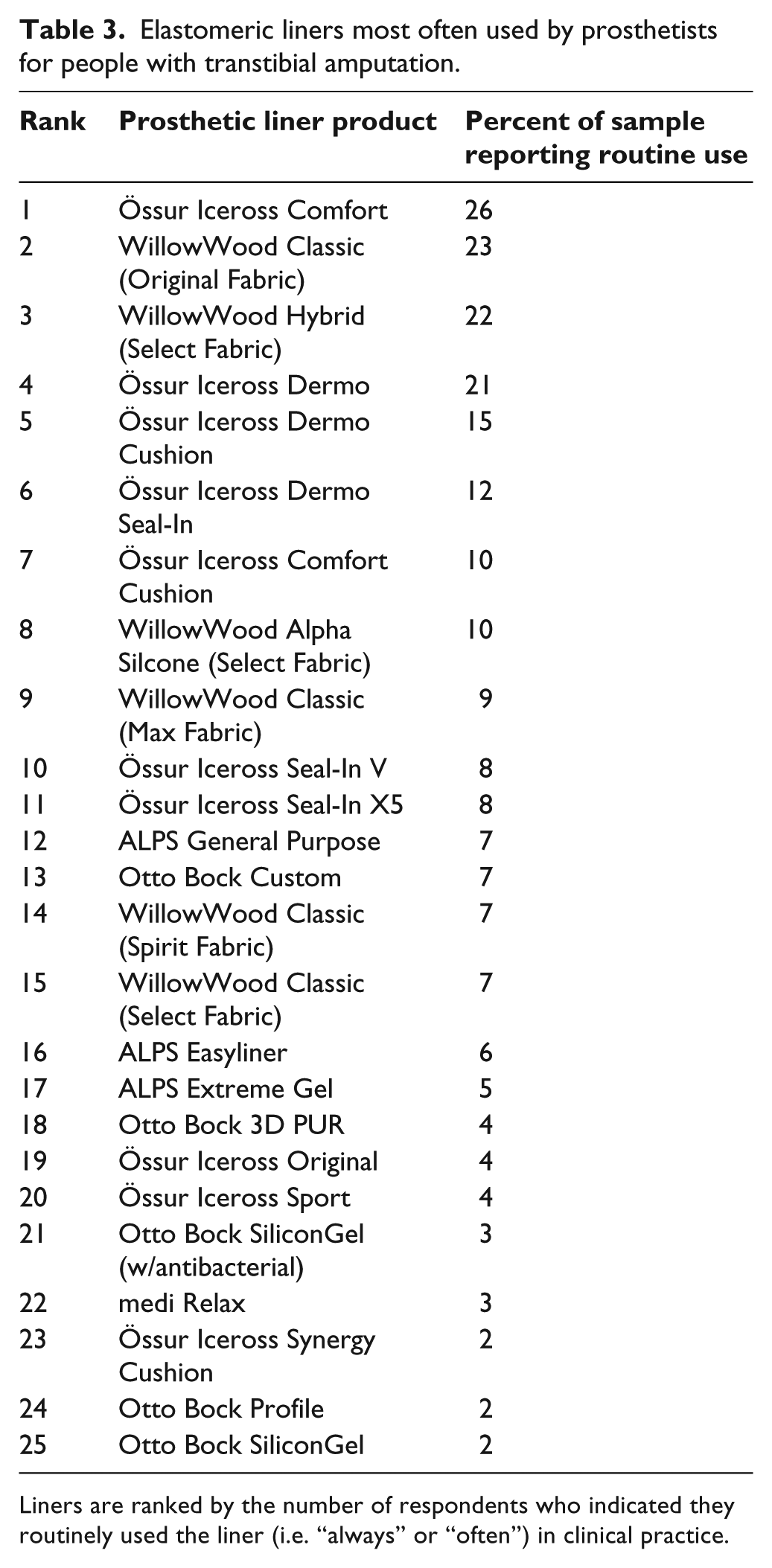
Liners are ranked by the number of respondents who indicated they routinely used the liner (i.e. “always” or “often”) in clinical practice.
Discussion
To our knowledge, this is the first study to evaluate prosthetists’ prosthetic liner prescription practices. We used an online survey to solicit information from experienced prosthetists about the elastomeric liners they provided to their patients with transtibial amputation. Similar surveys have been used to assess other aspects of prosthetists’ professional practices, including utilization of evidence from state-of-the-science conferences, 9 perceived barriers and facilitators to evidence-based practice, 10 and use of outcome measures in clinical practice. 11 Here, the survey was used to identify resources prosthetists used to obtain information about elastomeric liners, characteristics of importance in the clinical selection process, and specific liner products used by prosthetists.
Sources of liner product information
As expected, 8 prosthetists predominantly obtained information about liner products from manufacturers. Factors that contribute to the reported preference for manufacturer-provided information likely include both the accessibility and timeliness of information obtained in this manner. Despite widely acknowledged barriers to research literature access in O&P,12 –14 Andrysek et al. 10 reported that most prosthetists have access to journal articles, conferences, and clinical magazines. However, fewer than 50% reported using resources to obtain clinical information. They were instead more likely to consult with peers or search the Internet for answers to clinical questions. Manufacturer-provided liner information is generally free and readily accessible on the Internet and is likely preferred for its ease of access. Similarly, manufacturer-provided information may be more up-to-date than that from other sources. More than 50% of prosthetists acknowledged that a key reason empirical (i.e. research) evidence is not consulted is that it is generally out-of-date. 10 Given that new liners are released regularly, obtaining timely information about these products from sources other than manufacturers may be challenging. Finally, it is possible that prosthetists rely on manufacturer information in absence of empirical evidence. A relative dearth of evidence pertaining to prosthetic liners has been noted 8 and may be a reason for prosthetists’ limited use of information from peer-reviewed resources in this study. However, if prosthetists are to engage in evidence-based practices in the future, efforts to develop and disseminate research evidence related to prosthetic liners will be needed. 12
Characteristics of importance in liner selection
Prosthetists in this study acknowledged that they considered an array of characteristics when selecting a liner for their patients with transtibial amputation. That so many different criteria are considered reinforces the critical importance of a good limb-socket interface,1 –3 and the clinical challenge in matching each patient with an optimal prosthetic liner. As hypothesized, characteristics most commonly considered pertained to a liner’s primary functions, protection of the limb, and suspension of the prosthesis.2,4,5 Features such as comfort, thickness, and cushion were among the top five most endorsed considerations. Suspension was the third-most endorsed consideration, indicating that it too was a priority. The importance of these characteristics in the selection process is not surprising, as both comfort and suspension are believed to be advantages to elastomeric liners, when compared with other types of interfaces. 15 Cost is increasingly a concern in the provision of healthcare interventions, like prosthetic liners. 8 Interestingly, cost of the liner was only considered by about half the sample in the selection process. The patient’s cost was considered by far fewer of the prosthetists (16%), likely due to the fixed rate of reimbursement for elastomeric liners under US Center for Medicare and Medicaid Services guidelines. 16
Use of existing liner products
Despite the availability of a large number and variety of elastomeric liners for patients with transtibial amputation, prosthetists generally used relatively few products with their patients. This confirms previous assumptions that prosthetists often elect to use a few liners with which they have experience and success with patients. 8 Products routinely used were also sourced from just 4 of the 12 liner manufacturers with products included in the survey (i.e. Ossur, WillowWood, ALPS, and Ottobock). The limited diversity of liner selection observed in this study may be due to a variety of factors, including familiarity with products that work well, reluctance to try new products, perceived similarity among available liner products, or an absence of empirical evidence to promote a change in customary liners. As prosthetic liners are not generally interchangeable and changing liners would require fabrication of a new socket, prosthetists may deem the risk to try a new product too high. Services provided by the manufacturer (e.g. discounts, education, samples, rapid shipping, or overall customer service) may also influence selection and encourage prosthetists to more often use specific products.
Directions for future work
Results of this study can be used to direct future research and educational efforts. For example, the limited diversity of liners used by respondents in the study may indicate that prosthetists do not have sufficient information about liners, other than those few with which they have experience. To consider new liners, practitioners may need tools that allow them to easily compare and contrast liner properties. For example, the Prosthetic Liner Assistant (PLA), an interactive database of elastomeric liner products, was developed to allow practitioners to compare and contrast commercial liners by material (i.e. copolymer, polyurethane, silicone, thermoplastic elastomer), thickness (i.e. fixed-thickness, tapered, or anatomic), or mechanical properties (i.e. compressive resistance, shear resistance, stretch resistance, adherence, volume accommodation, thermal conductivity, and cost). 17 Results of this study may inform development of new tests to include in the PLA so that it includes additional characteristics of importance to prosthetists (e.g. liner durability).
Study results could also be used to guide development of educational resources for students and practicing clinicians. For example, continuing educational courses that explain how specific liner material properties6,18 –20 affect users’ limb health outcomes21,22 may encourage practitioners to consider liners that exhibit desirable characteristics. Resources (e.g. clinical algorithms) could be developed from these efforts to help practitioners determine whether elastomeric liners are appropriate for the patient, and which products would best serve specific patients. Development and application of evidence-based clinical algorithms or guidelines would also encourage professional practices and support justification of selected liners.
Results of this study may also guide new research and development efforts. Development of new liner materials has been noted as a priority by prosthetic researchers. 23 The priority of liner characteristics identified by respondents in this study may aid in development of liners that target features of clinical need. For example, durability was noted as an important liner feature among more than 90% of all prosthetists in this study. Concerns of elastomeric liner durability are also acknowledged in the scientific literature. Efforts to make liners more durable are challenging, as liners with increased durability generally transmit higher shear forces and increase risk of skin breakdown. 24 Thus, novel approaches to developing liners that are both soft and durable should be considered a priority. Development of liners with improved durability could improve patient satisfaction and reduce healthcare costs.
Study limitations
The number of participants in this study (n = 106) was relatively small compared to the overall population of prosthetists in the United States and Canada (estimated at 5800 and 200, respectively).25,26 However, prosthetists included in the study sample (Table 1) reflected the current diversity of prosthetists in the field by sex, age, ethnic and racial status, education level, and years of clinical experience. 27 Study participants were recruited through advertisements posted in clinical magazines, at conferences, or on the O&P listserv. Thus, the sample may be biased toward clinicians with a tendency to seek knowledge about clinical interventions through publications, meetings, or peer communications. Prosthetists that do not utilize these resources and instead rely primarily on experience and/or intuition when selecting interventions for their patients may not be well reflected in the study sample.
We also restricted participation in the study to prosthetists in North America, and most of the respondents (89%) were from the United States. Thus, the practice patterns described by our results may not reflect those of prosthetists in other areas of the world. Differences in healthcare and reimbursement systems present in the United States (e.g. fixed-cost reimbursement for prosthetic liners) may affect selection practices. Prosthetists who practice in places with different financial, legal, or medical policies may select liners based on other criteria. Evaluation of practices in these areas is needed to confirm similarities or differences with the results reported here.
Another limitation to this study is the method used to collect data about prosthetists’ liner practices. The survey used in this study was developed by the investigators to address the proposed hypotheses. We pilot-tested the survey and revised questions based on feedback from several clinical prosthetists prior to large-scale administration. However, as the goal of the survey was to solicit general information about practice patterns (and not to derive a score like in a traditional health outcomes survey), we elected not to subject the survey questions to more formal psychometric testing methods. This approach is common in surveys of professional practice patterns.27,28
Conclusion
The goal of this study was to further our understanding of prosthetists’ liner selection practices, specifically how prosthetists learn about and choose liners for individual patients. Results indicate that manufacturers are the primary source of information about both new and existing prosthetic liner products. When choosing liners, prosthetists consider a range of characteristics related to both the liner and the patient. Fundamental liner properties such as durability, comfort, and suspension are often a priority. Results also show that prosthetists use only a few different prosthetic liner products for their patients with transtibial amputation, despite the commercially availability of more than 70 unique products. Reasons for prosthetists’ liner restricted practices are unclear, but may be due to a scarcity of objective and comparable information about available liner products. Objective tools or resources that allow practitioners to compare and contrast desirable liner characteristics may help to facilitate greater variety in product selection and ability to match individual patients with the liner product best suited to their needs.
Footnotes
Author contribution
Brian Hafner, John Cagle, Katheryn Allyn, and Joan Sanders helped with the study concept and design; Brian Hafner, John Cagle, and Katheryn Allyn helped with the acquisition of data; Brian Hafner helped with analysis and interpretation of data; Brian Hafner helped with the drafting of manuscript; John Cagle, Katheryn Allyn, and Joan Sanders helped with critical revision of manuscript for important intellectual content; Joan Sanders obtained funding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Child and Human Development of the National Institutes of Health under award number R01HD065766. The content is solely the responsibility of the authors and does not necessarily represent the official views of National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.