
Abstract
Background:
This study reviewed prevalence of patients with lower limb amputations with above normal weight profile, with body mass index over 25, in seven disablement services centres managing their amputee rehabilitation in the United Kingdom.
Objectives:
To review two clinical standards of practice in amputee rehabilitation. Ambulant lower limb amputees should have their body weight recorded on an electronic information system, with identification of cohort with body weight >100 kg. Lower limb amputees to be provided with suitable weight-rated prosthesis.
Study design:
Observational study of clinical practice.
Methods:
Data were collected from the Clinical Information Management Systems. Inclusion criteria – subjects were ambulant prosthetic users with some prosthetic intervention in the last 5 years and had at least one lower limb amputation.
Results:
In 96% of patients, the weight record profile was maintained. In addition, 86% were under 100 kg, which is the most common weight limit of prosthetic componentry. Of 15,204 amputation levels, there were 1830 transfemoral and transtibial sites in users with body weight over 100 kg. In 60 cases, the prosthetic limb build was rated to be below the user body weight.
Conclusions:
In 96% of our patients, body weight was documented, and in 97%, the prosthetic limb builds were within stated body weight limits, but this may not be the case in all the other disablement services centres in the United Kingdom. Also, the incidence of obesity in the United Kingdom is a growing problem, and the health issues associated with obesity are further compounded in the amputee population.
Clinical relevance
Prosthetic componentry has distinct weight limits which must be considered during prescription. As people with amputation approach the limits of specific components, clinicians are faced with the challenge of continued provision in a safe and suitable manner. This article reviews the amputee population and the current national profile to consider trends in provision and the incidence of these challenges.
Background
The rate of obesity in the United Kingdom is rising significantly with almost a quarter of all adults in the United Kingdom being classed as obese on body mass index (BMI; normal: 19–25; obese: >30) in 2008. Studies have also shown that waist circumference, which is another strong health indicator, was increasing alongside this with 39% of adults presenting with increased waist circumference in 2008 as compared to 23% in 1993.1,2 The problem appears to be affecting all age ranges with 16.8% of boys and 15.2% of girls aged 2–15 years, classed as obese, an increase from 11.1% and 12.2%, respectively, in 1995–2010. 3
The health impact of increased body weight is well known with cardiovascular morbidity issues such as increased cardiac strain, increased energy expenditure, risk of myocardial infarction, diabetes and stroke. From a mechanical perspective, there is also a demonstrable increase in the presentation of osteoarthritis and biomechanical cost of ambulation. Additionally, from a psychosocial point of view, there is a significant increase in risk of depression, infertility and shortened life expectancy.
In the amputee population, most of the increased risk factors are already present in this vulnerable dysvascular cohort, with or without diabetes.
Along with the associated health factors and co-morbidities of amputees with increased body mass, there are mechanical implications to consider with the provision of a suitable prosthesis with component weight limitations. Modern-day prostheses are modular in construction, and each component must be tested to a specific weight limit to ensure that they can withstand the forces applied by prosthetic users. These tests form part of the International Standards Organisation (ISO) standard 10328. These standards are enforced by the UK Medical Devices Directive (MDD). Increased body weight beyond the specified weight limits of available prosthetic componentry presents a clinical risk that has to be considered carefully to balance the risk to the patient, along with the benefits of increasing function and activity of the individual. The range of components that are available at higher weight limits is restricted, presenting reduced functional options to the user and prescribing team. There is also a notable risk of litigation in inappropriate prosthetic component prescriptions. Prosthetic fitting also becomes more challenging with increased load to transmit through the prosthetic socket in limited pressure–tolerant anatomical areas.
We reviewed the prevalence of ambulant patients with lower limb amputations with above normal weight profile with BMI over 25 in seven disablement services centres (DSC) managing their amputee/prosthetic rehabilitation in the United Kingdom.
Average body weight loss in a unilateral transtibial (below knee) amputee is 7% of body weight, while in transfemoral cases, it is 16% of body weight. 4
Aims
The aim of the study was to review two clinical standards of practice in amputee rehabilitation/prosthetic provision:
Ambulant lower limb amputees should have their body weight recorded on an electronic information system, with identification of cohort with body weight >100 kg.
Lower limb amputees should be provided with suitable weight-rated prosthesis.
Methods
Data were obtained from the Clinical Information Management System (CIMS) databases from seven prosthetic clinics in the United Kingdom. The data were anonymised and secure. A total of 23,850 amputation were identified with 18,596 of them relating to the lower limb amputations (Figure 1). Inclusion criteria were that the subject was an ambulant prosthetic user, namely, had some kind of prosthetic intervention in the last 5 years and had at least one lower limb amputation. Major bilateral lower limb amputees made up 10% of all lower limb amputees cohort, of which 2% were noted to have limited ambulation. Upper limb amputees were excluded as the focus of the investigation related to weight-bearing prostheses.
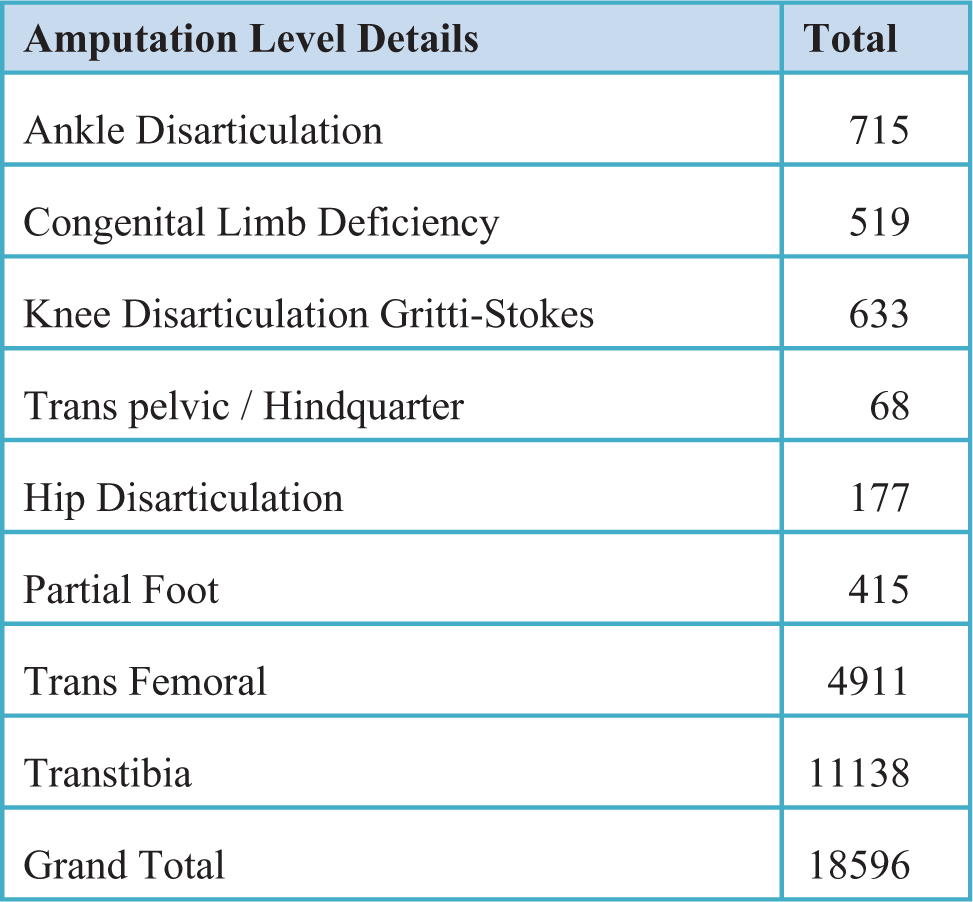
Data from the Clinical Information Management System.
The weight of each individual user, age, activity level, amputation site(s), cause of amputation and limb build type were recorded for each amputation. The mean age was 55 with a range of 0–98 years, and the mean recorded weight as 75.4 kg with a range of 6–179 kg.
Prosthetic components tend to be limited to a weight limit of 100 kg. There are some minor exceptions to this with paediatric limb systems, but these are used infrequently. Hence, users of less than 100 kg were excluded.
To enable review, the subjects were split into six distinct weight range groups:
Group 1 <100 kg
Group 2 100–125 kg
Group 3 125–136 kg
Group 4 136–150 kg
Group 5 150–166 kg
Group 6 166 kg+
These groups reflect prosthetic industry componentry weight limit thresholds across the major suppliers globally. At the time of the study, 166 kg was the highest weight-rated componentry that was Conformity European (CE) marked and available in the United Kingdom, indicating that any subjects with lower limb amputations above this weight limit had no standard prosthetic modular solutions available. The data were analysed in relation to the two clinical standards identified in this review.
Results
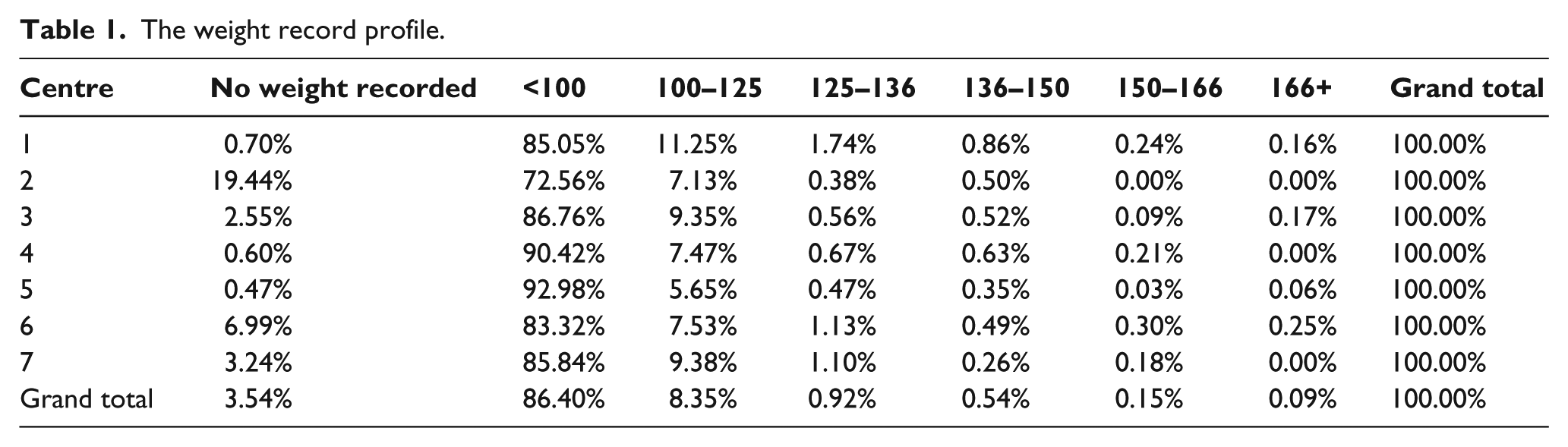
Of all the records reviewed, 3.54% of subjects had a body weight of 0.00 kg recorded on CIMS. This was considered as a non-record. Across the various centres, the range was 0.47%–19.44%.
In 96% of patients, the weight record profile was maintained. Of note, 86.4% of subjects were less than 100 kg, which is the most common weight limit of prosthetic componentry from global suppliers (Table 1).
The weight record profile.
When reviewed against activity levels, it was found that various activity level descriptors were used, and due to limitations of users with both upper and lower limb amputations, 1248 amputation sites could not be linked to an activity level.
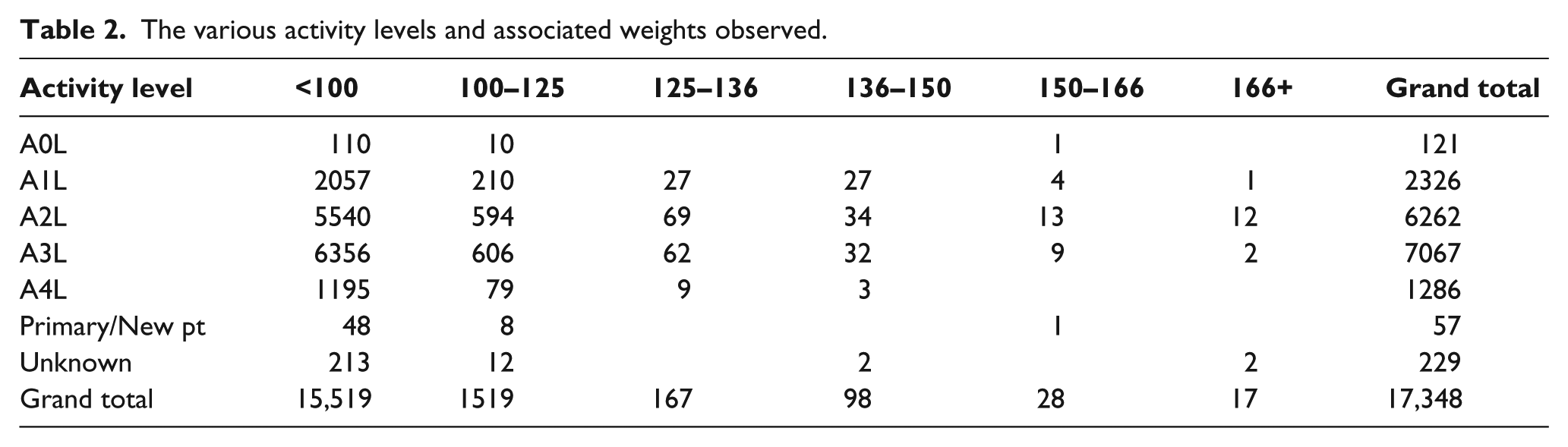
The most common activity codes used are detailed in Figure 2, and Table 2 outlines the various activity levels and associated weights observed. It is of note that only 17 amputation sites are associated with a user of 166 kg+, and of these, only two were linked to an activity level equal to that of a community ambulatory.
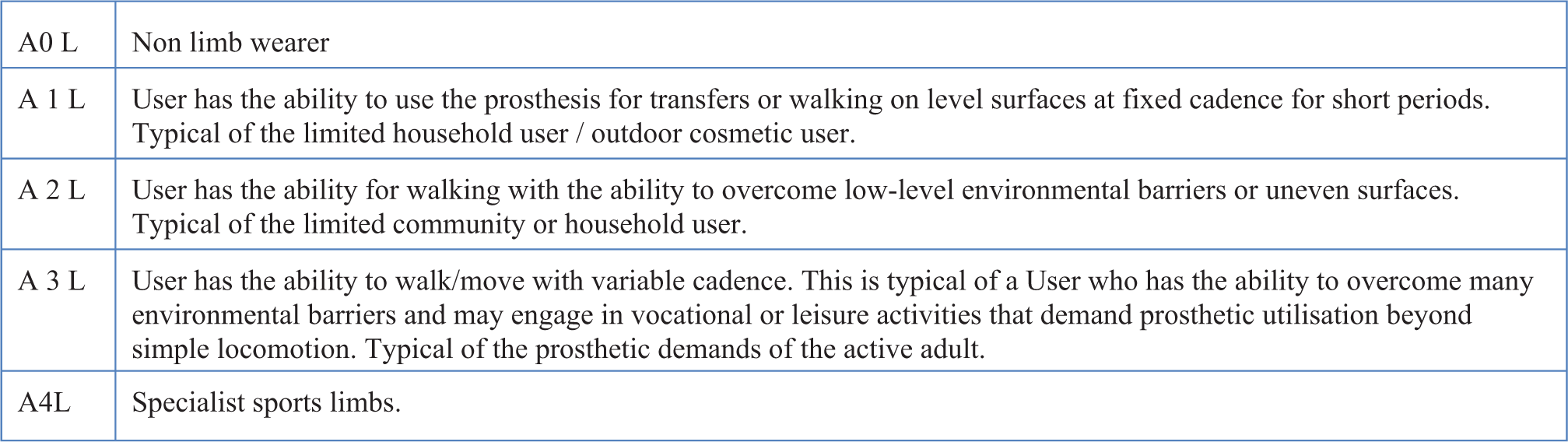
The most common activity codes.
The various activity levels and associated weights observed.
The cause of amputation/limb loss in Figure 3 reflects to greater extent the health-risk factors outlined in the ‘Background’ section with an increasing presentation of dysvacularity-related amputations and a trend of increasing cohort of post-trauma amputations. The causation profile differs from National Amputee Database (NASDAB), 5 in which three-quarters of causation were noted to be due to dysvascular cause.
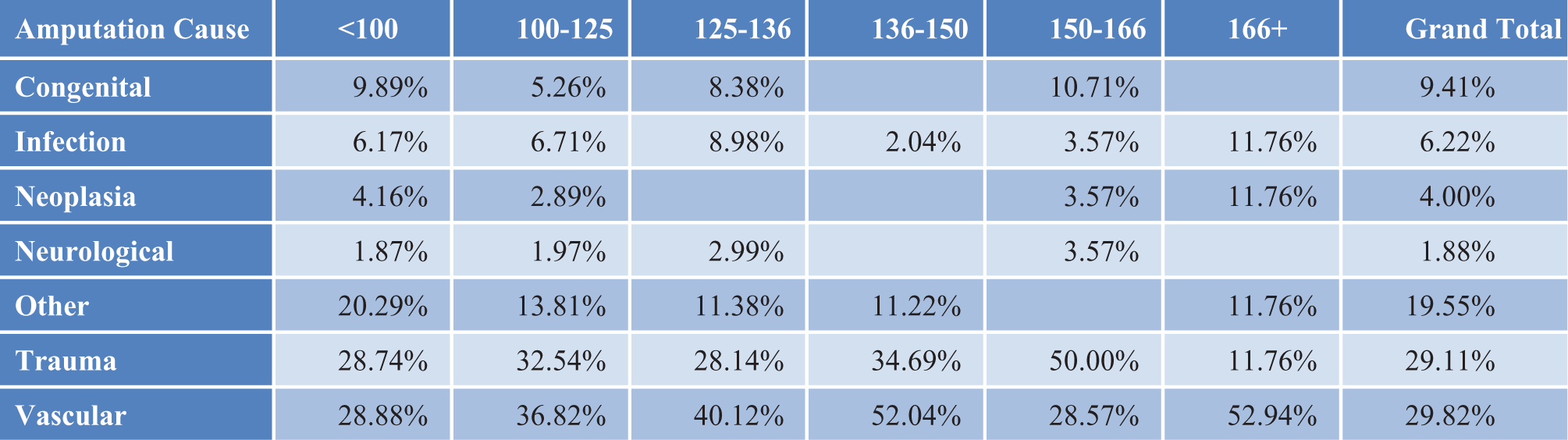
The cause of amputation/limb loss.
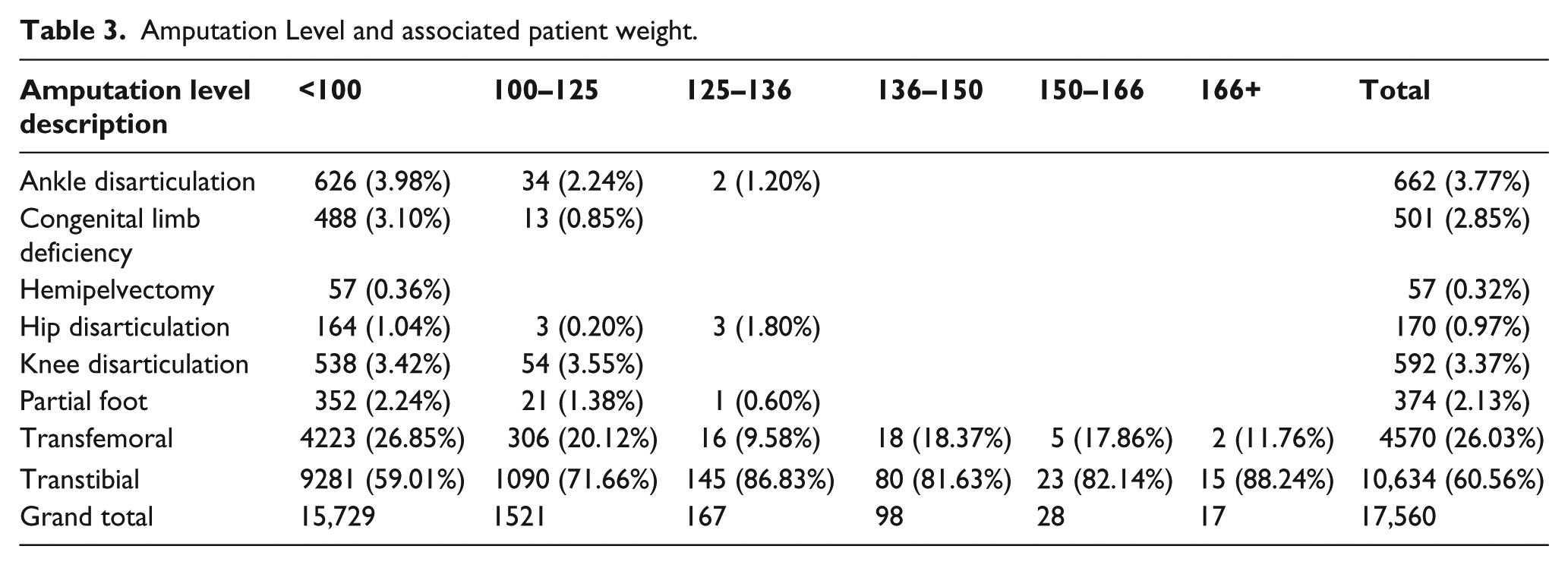
When focusing on users with a recorded weight on CIMS, there were 17,560 lower limb amputation sites in total with transtibial and transfemoral amputations accounting for 86.59% of all amputations as seen in Table 3. These 15,204 amputations levels being the most common with the most standardised prosthetic limb builds were the focus of the further analysis.
Amputation Level and associated patient weight.
As seen in Figure 4, there are 1830 transtibial and transfemoral sites that present with users of body weight over 100 kg. These amputation sites were reviewed against the prosthetic limb build provided, as they give an indication, although not explicitly, of the weight limit of the prosthesis. Nationally, there is a classification system for the components available by prosthetic components supplier. The prostheses were split into categories of modular (types 1–6), water activity, unknown and conventional. Conventional artificial limb prostheses are not modular in build and are completely custom made from raw materials such as metal, wood and leather. They are not subject to the static load testing, as detailed in ISO 10328.
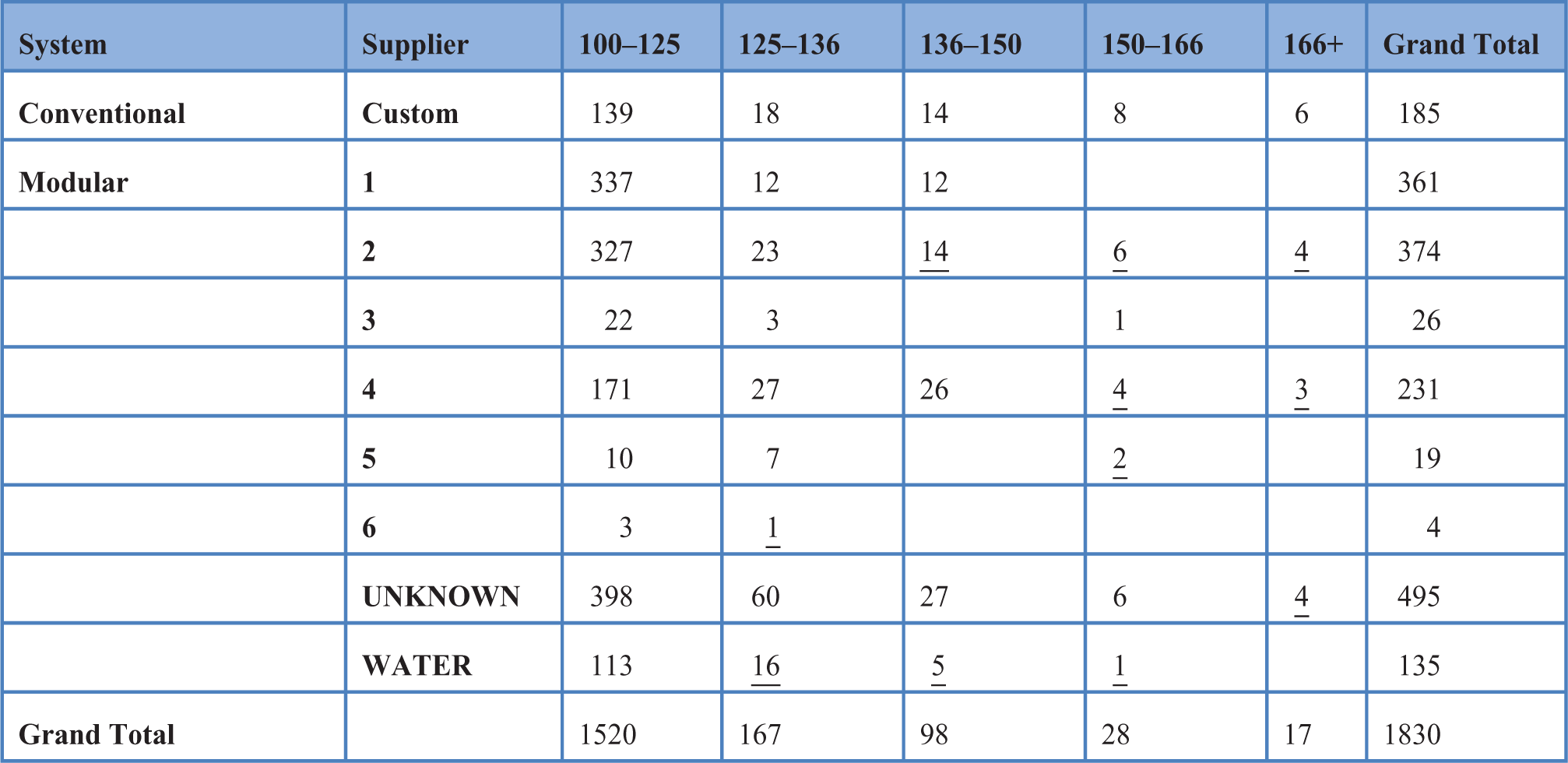
Transtibial and transfemoral sites that present with users of body weight over 100 kg.
From the various suppliers, at the time of the review, the indicative weight limits available were as follows: Modulars 1 and 2 and water activity up to 125 kg, Modular 5 up to 136 kg, Modulars 4 and 6 up to 150 kg and Modular 3 up to 166 kg. Unknown limb builds could fall into any of the above categories.
A total of 17 cases in 125–136 kg category, 19 cases in 136–150 kg category and 11 cases in 150–166 kg category.
Seven cases in 166+ kg category.
In 60 cases (3%), the prosthetic limb build appears to be rated below the user body weight, which represents a clinical risk.
Discussion
In 7 out of 42 DSCs in the United Kingdom, recording of user’s body weight was clearly done on a regular basis with less than 4% having the body weight missing from the CIMS record. However, due to the potential risk of increased body weight, it should be mandatory to keep an ongoing record. Also, this study did not review the accuracy of the data and that the presence of the recorded weight does not necessarily confirm that is the current measured body weight of the individual. It is recommended that body weight be measured and recorded routinely at attendances within the prosthetic clinic.
There is concern about the indicator of safety levels in regard to componentry. Lower limb prosthetic devices are provided to enable some sort of ambulation for the user. The simple biomechanics of motion will result in forces up to six times the static load due to the acceleration and increased momentum in situations such as stair descent, jogging and walking. The testing systems currently used for prosthetic devices do not take into account these dynamic forces. Some prosthetic componentry suppliers confirm that the weight limits published are below the static test load, but the magnitude is not confirmed. This consideration becomes less crucial when we consider that bariatric users identified in this study are assessed as low activity.
In our study, 3% of prosthetic limb builds were rated below the user body weight, signifying clinical risk. Reviewing the provision of prosthetic devices by limb category per amputation is limited in its accuracy as the limb build, while being a good indicator of the weight limit of a device is not definitive. If a limb build system rated to 125 kg has a prosthetic device such as a standard modular foot integrated into the build, the weight limit of the prosthesis as a whole is 100 kg due to the limit of the weakest element, namely, the standard foot. The classification of limb build systems could be expanded to incorporate limb build weight limits. Furthermore, additional recording of the weakest component within the CIMS system would complement the mandatory body weight recording outlined above.
This situation presents a dilemma for the prosthetic team as there is a conflict of priorities. Research has shown that ambulation and increased activity have several health benefits including weight loss, decrease in dependency, and emotional well-being, and provision of a lower limb prosthesis has also been shown to increase activity and improve related issues. Therefore, it is in the patient’s interest to use the prosthesis and increase activity. However, if the commercially available componentry required to manufacture the prosthesis does not meet the required weight limit, there is a risk to the user.
It is important that the amputee rehabilitation teams educate the high BMI patient regards dietetic and weight loss regime and also refer appropriate patients in the early stages to the regional obesity clinics. In some of the cases above, there would be an option to change limb build systems to increase the weight limit, although this could limit the options of functional items. It is not that prosthetic knee units do not currently offer as high weight limits as other components, for example, feet; however, when a set of components have been tested to meet the biomechanical demand of the user, it would be sensible to protect the user in this way. In the presence of a situation where it is considered that a functional item that is weight rated under the body weight of the user would be beneficial, clinical practice reveals that team decisions are taken to make a risk assessment with observed practice of documenting this decision with the user’s involvement and ongoing monitoring.
Although custom-built devices or conventional build options are available, as highlighted the physical load that any such device will stand is untested with ISO 13028 standards.
Conclusion
Although our study confirms that in 96% of our patients body weight was documented and in 97% of our patients the prosthetic limb builds were with stated body weight limits, this may not be the case in all the DSCs in the United Kingdom. Also, the incidence of obesity in the United Kingdom is a growing problem, and the health issues associated with obesity are further compounded in the amputee population. When dealing with bariatric amputees using functional lower limb prosthesis, careful consideration is needed to minimise risk to users by maximising their potential for physical activity while curtailing the risk of failure of the prescribed device. This issue affects both unilateral and bilateral lower limb amputees. Multidisciplinary decisions are considered paramount, and documentation of care/monitoring schedule is recommended. Considering the increasing prevalence of obesity in the United Kingdom, it is but logical that the prevalence of bariatric amputees will also increase in tandem; hence, we suggest larger prospective studies to confirm our findings.
Footnotes
Acknowledgements
We would like to thank Nicola Gorton and Julie Kay Sportelli for their assistance and the patients who we reviewed for the study.
Conflict of interest
None.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.