
Abstract
Background:
The fitting rate of the C-Leg electronic knee (Otto-Bock, D) has increased steadily over the last 15 years. Current cost-utility studies, however, have not considered the patients’ characteristics.
Objectives:
To complete a cost-utility analysis involving C-Leg and mechanical knee users; “age at the time of enrollment,” “age at the time of first prosthesis,” and “experience with the current type of prosthesis” are assumed as non-nested stratification parameters.
Study design:
Cohort retrospective.
Methods:
In all, 70 C-Leg and 57 mechanical knee users were selected. For each stratification criteria, we evaluated the cost-utility of C-Leg versus mechanical knees by computing the incremental cost-utility ratio, that is, the ratio of the “difference in cost” and the “difference in utility” of the two technologies. Cost consisted of acquisition, maintenance, transportation, and lodging expenses. Utility was measured in terms of quality-adjusted life years, computed on the basis of participants’ answers to the EQ-5D questionnaire.
Results:
Patients over 40 years at the time of first prosthesis were the only group featuring an incremental cost-utility ratio (88,779 €/quality-adjusted life year) above the National Institute for Health and Care Excellence practical cost-utility threshold (54,120 €/quality-adjusted live year): C-Leg users experience a significant improvement of “mobility,” but limited outcomes on “usual activities,” “self-care,” “depression/anxiety,” and reduction of “pain/discomfort.”
Conclusion:
The stratified cost-utility results have relevant clinical implications and provide useful information for practitioners in tailoring interventions.
Clinical relevance
A cost-utility analysis that considered patients characteristics provided insights on the “affordability” of C-Leg compared to mechanical knees. In particular, results suggest that C-Leg has a significant impact on “mobility” for first-time prosthetic users over 40 years, but implementation of specific low-cost physical/psychosocial interventions is required to retun within cost-utility thresholds.
Background
Quality of life (QoL) is a relevant outcome to consider when assessing the impact of lower-limb prosthetic technologies. 1 However, studies report that while new technologies mostly advance mobility,2,3 their impact on QoL is limited. Indeed, Sinha and Van Den Heuvel’s 4 review of 26 studies reported that QoL of lower-limb amputees remains moderately above 50%. 5 This evidence is troublesome in light of the increasing costs of new biomechatronic solutions6,7 and urges healthcare providers to (1) select prosthetic solutions with the highest demonstrated effects on patients’ QoL, with an efficient use of economic resources8,9 and (2) to design interventions that optimize how the prosthesis is supplied to a patient.
In this context, decision-making must be evidence based. While several studies reported data on technical specifications, functional outcomes, and costs associated with new prostheses (mostly prosthetic knees 8 ), few works combined this information and compared prosthetic solutions according to their cost-effectiveness or cost-utility.8,10–13 In particular, cost-utility analysis (CUA) has become a standard component of Health Technology Assessment since its end-result indicator—the incremental cost-utility ratio (ICUR)—provides healthcare decision-makers and providers with a straightforward information, that is, how much a “unit of utility improvement” would cost them and/or the society.14,15 Assuming a timeframe of analysis (e.g. 5 years) and two alternative technologies A and B, ICUR is the ratio between the difference in costs and the difference in utility of A and B
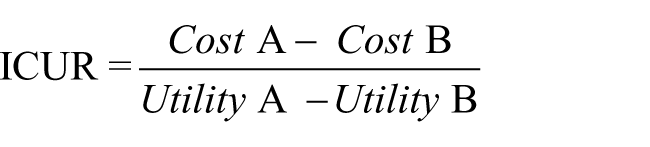
Cost incorporates the expenses sustained for the technology within the timeframe, commonly expressed in monetary units (e.g. euros, dollars); utility is typically measured in quality-adjusted life years (QALY), 16 that is, the number of years lived in full health over the timeframe by patients exposed to the technology. If technology A is less expensive and more useful, the decision to opt for A over B is straightforward (Figure 1). The opposite is equally true. Otherwise, the origin of the mixed results has to be carefully analyzed and comparison with generally acceptable cost-utility thresholds must be undertaken. CUA has been largely employed for technology assessment in a wide range of fields17,18 and endorsed by international Agencies such as International Network of Agencies for Health Technology Assessment (INAHTA) and National Institute for Health and Care Excellence (NICE). The threshold for accepting a new technology is a political matter that varies country by country. In a recent study, Dakin et al. 19 established that NICE practical acceptability threshold is between 39,000 and 44,000 £ per QALY, while Eichler et al. 20 reported a range from 30,000 to 100,000 US$/QALY.
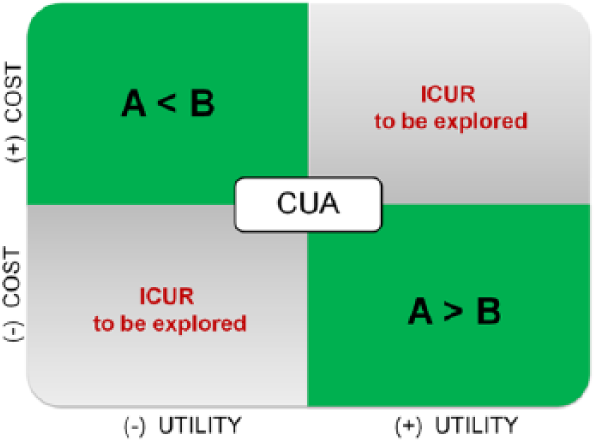
Cost-utility decision-making process.
Current CUA studies on lower-limb prosthetics suffer from two main limitations: (1) the majority of evidence comes from samples of limited size (N < 100 participants) and (2) past studies did not explore how cost and utility are affected by patients’ characteristics, that is, they have not stratified the analysis based on personal features. Based on this additional knowledge, healthcare providers could make more informed decisions regarding whether adoptions and interventions should be differentiated among different groups of patients.
In this framework, this study focuses on prosthetic knees, which are the most expensive component in lower-limb prostheses. In particular, the aim was to perform a stratified cost-utility analysis (sCUA) on a large sample of lower-limb amputees, to compare the most used microprocessor controlled knee on the market, the C-Leg (Otto-Bock, DE), with a selection of advanced mechanical knee (MK) competitors. In particular, “age at the time of enrollment in the study,” “age at the time of first prosthesis,” and “experience with the current type of prosthesis” (in years) were assumed as non-nested stratification parameters. By performing a sCUA, we expected to (1) identify groups of patients with an unfavorable ICUR, (2) highlight the domains in which the C-Leg/MK competitors bring advantages to the patients, and (3) help designing targeted interventions to improve cost-utility.
Methods
Context and study design
The study was commissioned by the Prosthetic Centre of the Italian Workers’ Compensation Authority, which is a Public Body in Italy (hereinafter INAIL-PC). As per INAIL Regulation,21–23 patients affected by work-related injuries are supplied free-of-charge of any knee joint deemed medically appropriate. INAIL internalizes the costs for knees (including microprocessor controlled knees) and prosthesis components, as well as the costs for patients’ rehabilitation and gait training.
This retrospective study comprised of seven steps: (1) selection of MKs to be compared to the C-Leg; (2) definition of patients’ inclusion/exclusion criteria; (3) definition of the stratification parameters; (4) cost data collection through the INAIL-PC database; (5) utility data collection through a self-report survey, sent to eligible participants via mail; (6) execution of the non-sCUA; and (7) execution of the sCUA. The study was approved by the Institutional Review Board and was coherent to all the ethical requirements.
Selection of comparative MK joints
Commercial MKs were reviewed based on recommended target population (i.e. medical activity levels) and prevalence of use at INAIL-PC, resulting in over 20 different models. The mechanical solutions chose to compare to the C-Leg were those (1) recommended by the producer for K3 patients, as the C-Leg; (2) most commonly supplied in the back-up prosthesis of C-Leg users; (3) internationally available; and (4) with at least 8 years of application records at INAIL-PC. Only three MKs satisfied these criteria, that is, 3R60 (Otto-Bock; N = 1175), Total Knee 2100 (Össur, IS; N = 255), and Total Knee 2000 (Össur, IS; N = 209).
Participants’ inclusion/exclusion criteria
The target population for this study included unilateral transfemoral amputees who (1) were amputated for work-related injuries; (2) were at least 35-year old at the time of enrollment; and (3) were fit with C-Leg or 3R60/Total Knee 2000/Total Knee 2100. All participants were fit with an Össur Variflex foot since this represents the only foot supplied with C-Leg knees at INAIL-PC. Patients with a current diagnosis of cancer, who were under treatment or suspended the treatment less than 6 months before enrollment, were excluded. A total of 242 eligible patients were extracted from the INAIL-PC database, which collects all prosthetic treatments completed by the Prosthetic Center since year 1998.
Stratification parameters
Based on Sawers and Hafner, 3 participants were stratified based on three non-nested parameters:
Age at the time of enrollment, with three subsets, that is, 35–53, 54–65, and >65 years;
Age at the time of first prosthesis (age at which the patient received a prosthesis for the first time in life), with three subsets, that is, <26, 26–40, and >40 years;
Experience with the current type of prosthesis (in years), with two subsets, that is, 0–7 years and >7 years with C-Leg or MKs.
Data collection
Costs were measured retrospectively over a 5-year period, 13 adopting the provider (i.e. INAIL) perspective. For each patient, data were extracted from INAIL-PC database. Specifically, we considered the cost of prosthesis acquisition, maintenance, transportation, and overnight stays, which constitute the principal sources of expense in which C-Leg and MK competitors may differ. Other costs related to prosthesis fitting, hospitalizations, and rehabilitation were not considered as common to both C-Leg and MKs.
Additional information and utility data were collected by mailing to each patient a self-report survey. This included both multiple-choice and open-ended questions, concerning (1) demographics (age, sex, height/weight, marital status, and living situation), (2) amputation (side/level), (3) employment (level of education, professional status, and role before/after amputation), and (4) prosthesis (age at the time of first prosthesis, experience with the current type of prosthesis, hobbies/sports). To measure utility, the survey included a standardized measure of QoL, the EQ-5D (EuroQoL Group 24 ). The questionnaire comprises five dimensions (“physical mobility,” “self-care,” “usual activities,” “pain/discomfort,” and “anxiety/depression”) for which three levels of answer are possible (1: no problem, 2: some problems, and 3: severe problems). By answering the five dimension items, each patient defines a health profile, for example, 11121, that can be converted into an index score using an Excel sheet provided by the EuroQoL Group. 25 Scores were computed by adopting the “UK EQ-5D index calculator” sheet, which returns values ranging from −0.594 (i.e. 33333) to 1.0 (i.e. 11111). Of note, negative scores are a matter of concern when they affect the calculation of the mean values. In this study, only two patients showed negative scores (respectively, −0.184 and −0.349) that were anchored to zero. EQ-5D constituted our measure of QALY/year, where a value of 0.0 = death and 1.0 = optimal health. The QALY/year value was then multiplied by 5 to calculate a 5-year QALY, in accordance with previous work. 13 It is relevant here to remind that the presence of at least one “3” answer generates a penalty in the QALY value, that is, a substantial decrease in time spent in full health.
Data analysis
Considering the two groups of C-Leg and MK users without stratification, qualitative and quantitative variables were compared with χ2 and Student t-tests, respectively (SPSS 20, IBM, USA). The ICUR was calculated by dividing (1) the difference in costs and (2) the difference is utility between C-Leg and MK competitors
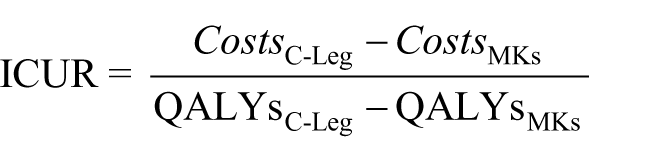
The incremental cost of the new technology was estimated by opposing the total costs of the two alternative technologies incurred during the complete life cycle of 5 years. Costs were not discounted since the dominant portion of the total costs takes place in a single year, that is, the first year, when the knee prosthesis is purchased. The incremental utility (difference in QALYs) was evaluated by comparing the results of the EQ-5D questionnaire in the two groups.
The same approach was applied to examine the incremental costs, incremental QALYs, and ICUR between C-Leg and MK users, within each of the three stratification parameters.
For ICUR interpretation, we assumed an ICUR acceptability threshold of 54,120 €/QALY. This was based on converging the 44,000 £ upper-threshold provided by Dakin et al., 19 from Pound to Euro, using the average exchange rate (1.23) over the period (2007–2011) of observation for this study. This is prudential compared to the maximum acceptability threshold reported by Eichler et al. 20 which is as high as 100,000 US$/QALY, that is, approximately 72,200 €/QALY (considering the average exchange rate for years 2007–2011).
Results
The results are divided into three main sections that examine (1) patients’ enrollment and sample characteristics, (2) non-stratified, and (3) sCUA.
Patients enrolled
The survey was delivered to 242 patients, and 135 usable questionnaires were returned. Eight questionnaires were discarded from the analysis since respondents did not fill in all items measuring QoL. The remaining questionnaires (N = 127) passed the quality check. All patients confirmed the data extracted from the INAIL-PC archives and provided informed consent and were thus enrolled in the study.
The final sample included 70 C-Leg patients and 57 MK patients. Statistical analysis confirmed that the two groups were comparable, as no significant differences emerged in terms of demographics (i.e. age, gender, height, and weight), amputation, and socio-economic variables (e.g. civil and professional status, academic degree, hobby, and sport) (Table 1). No significant differences emerged from respondents and non-respondents.
Sample characteristics.
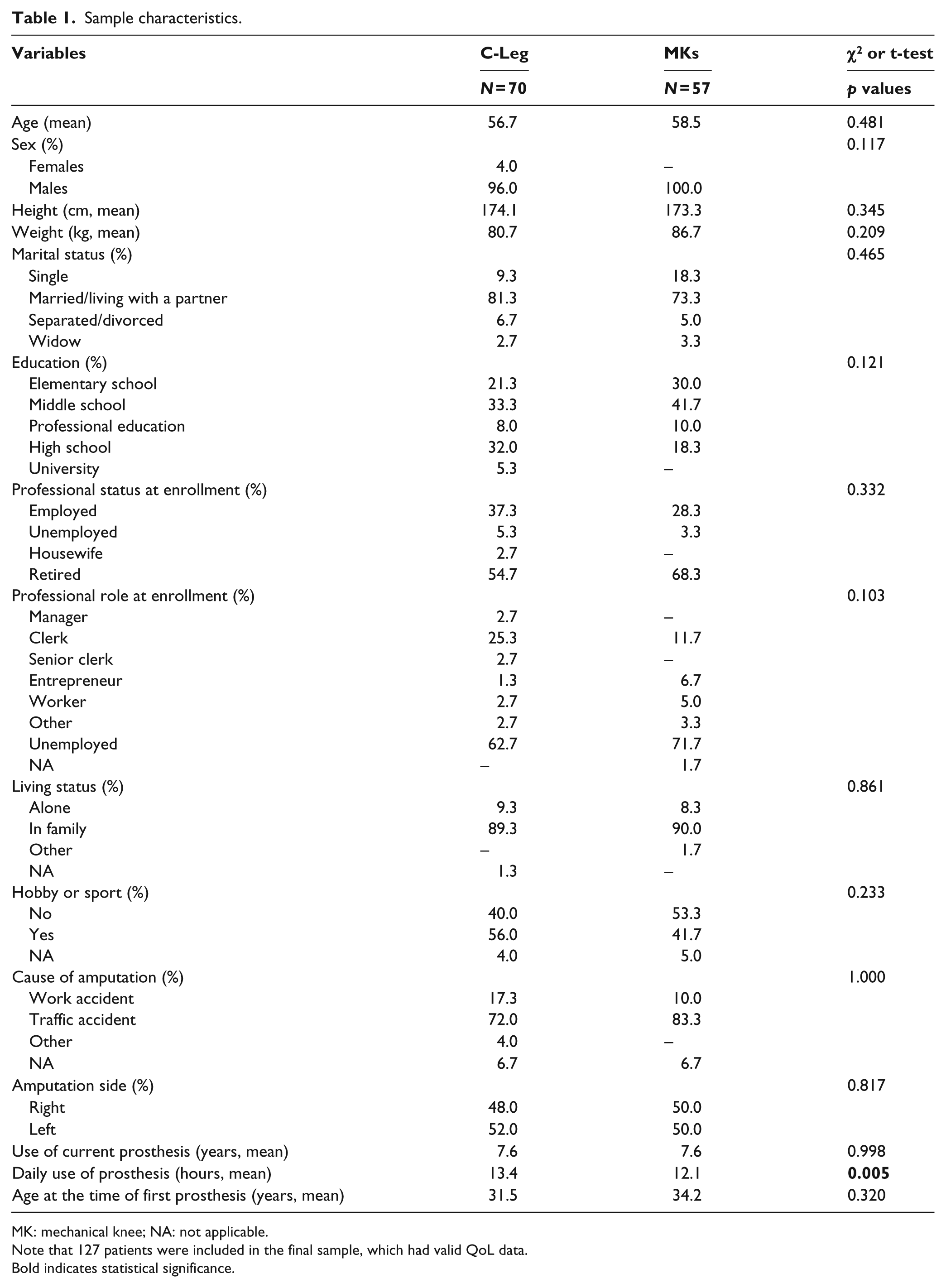
MK: mechanical knee; NA: not applicable.
Note that 127 patients were included in the final sample, which had valid QoL data.
Bold indicates statistical significance.
In addition, no statistically significant differences emerged in the distribution of subjects among subset, within each stratification parameter (Table 2).
Distribution of patients across stratification subgroups.
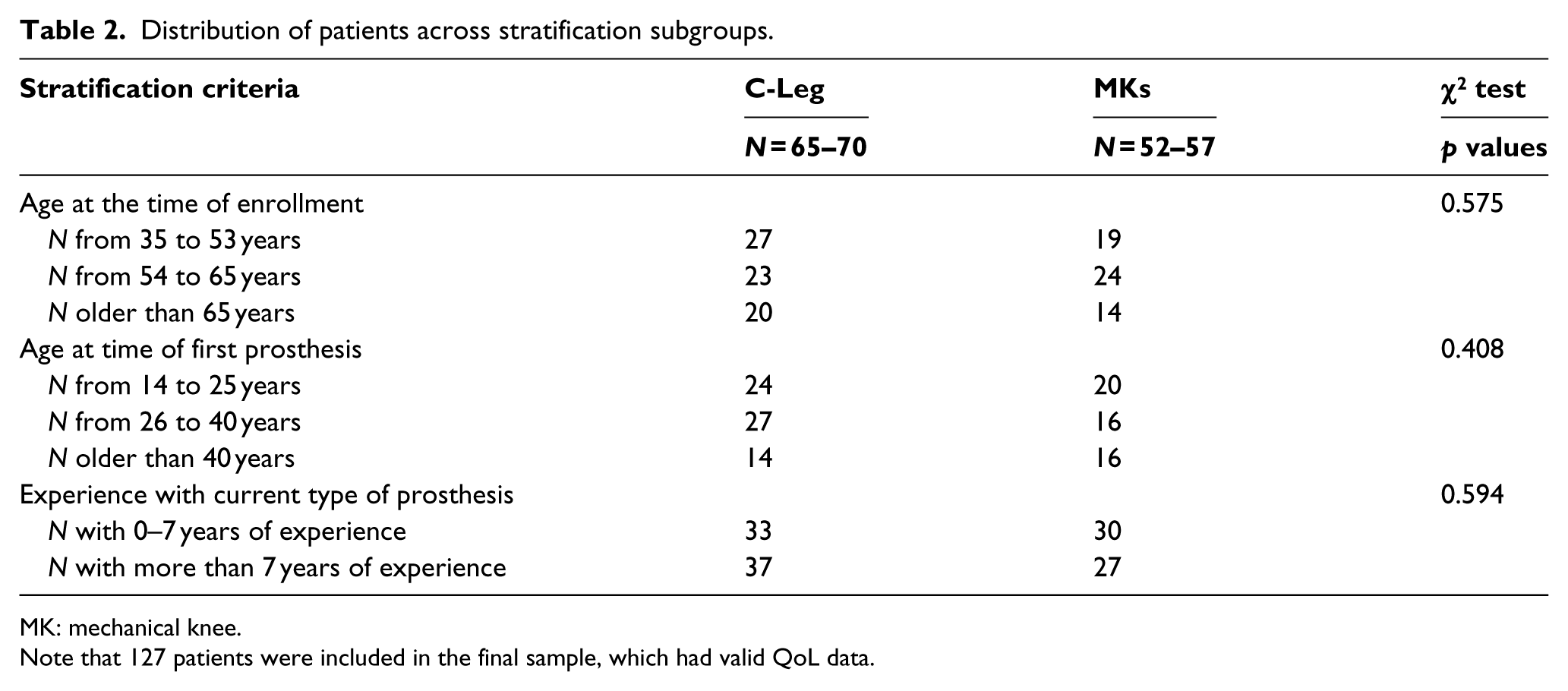
MK: mechanical knee.
Note that 127 patients were included in the final sample, which had valid QoL data.
Non-stratified CUA
In this section, results are reported for the comparison between all C-Leg and all MK users, without stratification.
Costs differences
Table 3 shows the average incremental costs per patient over 5 years. There is, indeed, a relevant difference in terms of costs (18,421.25 €) between the C-Leg and MK competitors, and the cost for the technology acquisition represents the main source of difference. No costs for maintenance and repair were observed outside the warranty period; cost for transportation and overnight stays had a marginal impact on incremental costs.
Incremental costs over 5 years.
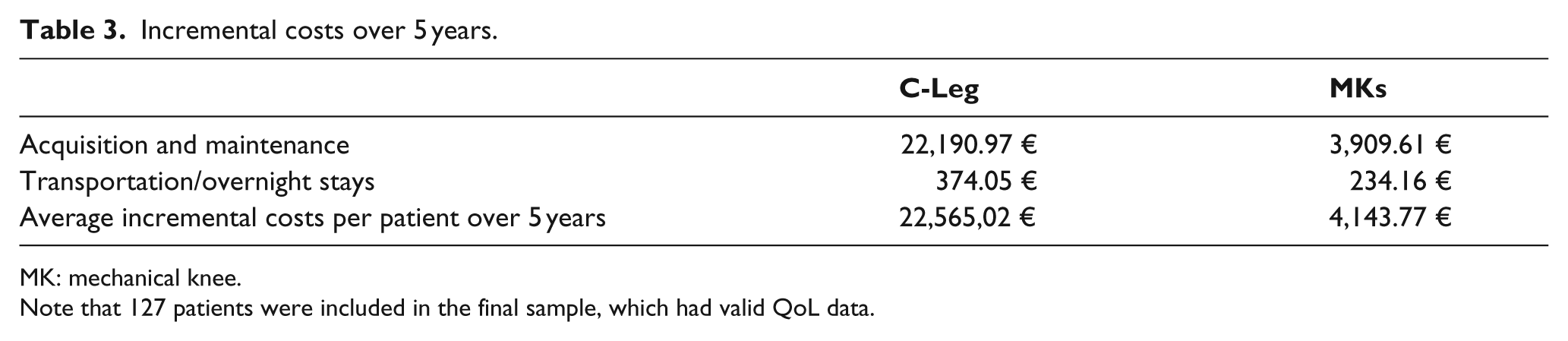
MK: mechanical knee.
Note that 127 patients were included in the final sample, which had valid QoL data.
Utility differences
Table 4 shows the difference in QALYs between C-Leg and MK patients. C-Leg users experienced significantly higher levels of QoL than MK users (EQ-5D mean = 0.768 vs 0.677; p = 0.006), and this difference (0.091 points) represents the incremental utility of using the C-Leg. As such, over a 1-year period, amputees with C-Leg benefit from a 9% absolute increase (i.e. 33 days) in their utility. In a 5-year period, the QALY for C-Leg patients is then 3.842 versus 3.383 for MK patients. The incremental utility of C-Leg in a 5-year timespan is thus +0.459 QALYs, that is, about 6 months in full health.
Quality of life in lower-limb amputees.
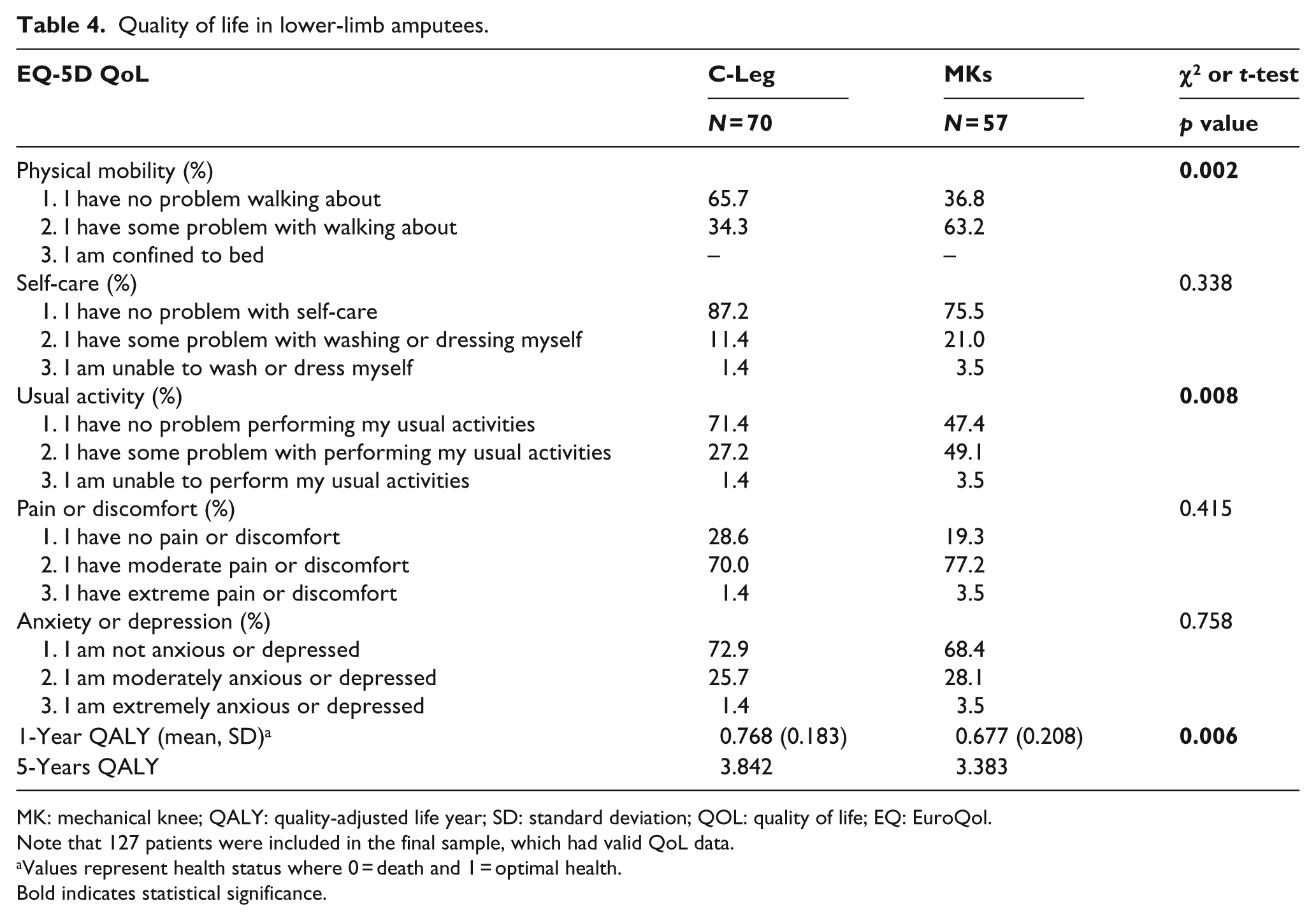
MK: mechanical knee; QALY: quality-adjusted life year; SD: standard deviation; QOL: quality of life; EQ: EuroQol.
Note that 127 patients were included in the final sample, which had valid QoL data.
Values represent health status where 0 = death and 1 = optimal health.
Bold indicates statistical significance.
When considering each EQ-5D dimensions separately, the two groups significantly differed in terms of “physical mobility” (p = 0.002) and “usual activity” (p = 0.008), in favor of the C-Leg. Although C-Leg had better scores for the other three dimensions (i.e. higher rate of “no problem” answers), differences were not statistically significant.
ICUR
As noted above, over a 5-year period, (1) the mean difference in costs between C-Leg and MKs was 18,431.25 € and (2) the mean difference in QoL was 0.459 QALYs. As such, ICUR values for the present sample was 40,155.45 €/QALY, and fell below ICUR acceptability thresholds (54,120 €/QALY).
sCUA
Table 5 summarizes results of costs, utility, and ICUR, stratified according to each parameter. In the following section, results are commented by stratification parameter.
Stratified CUA.
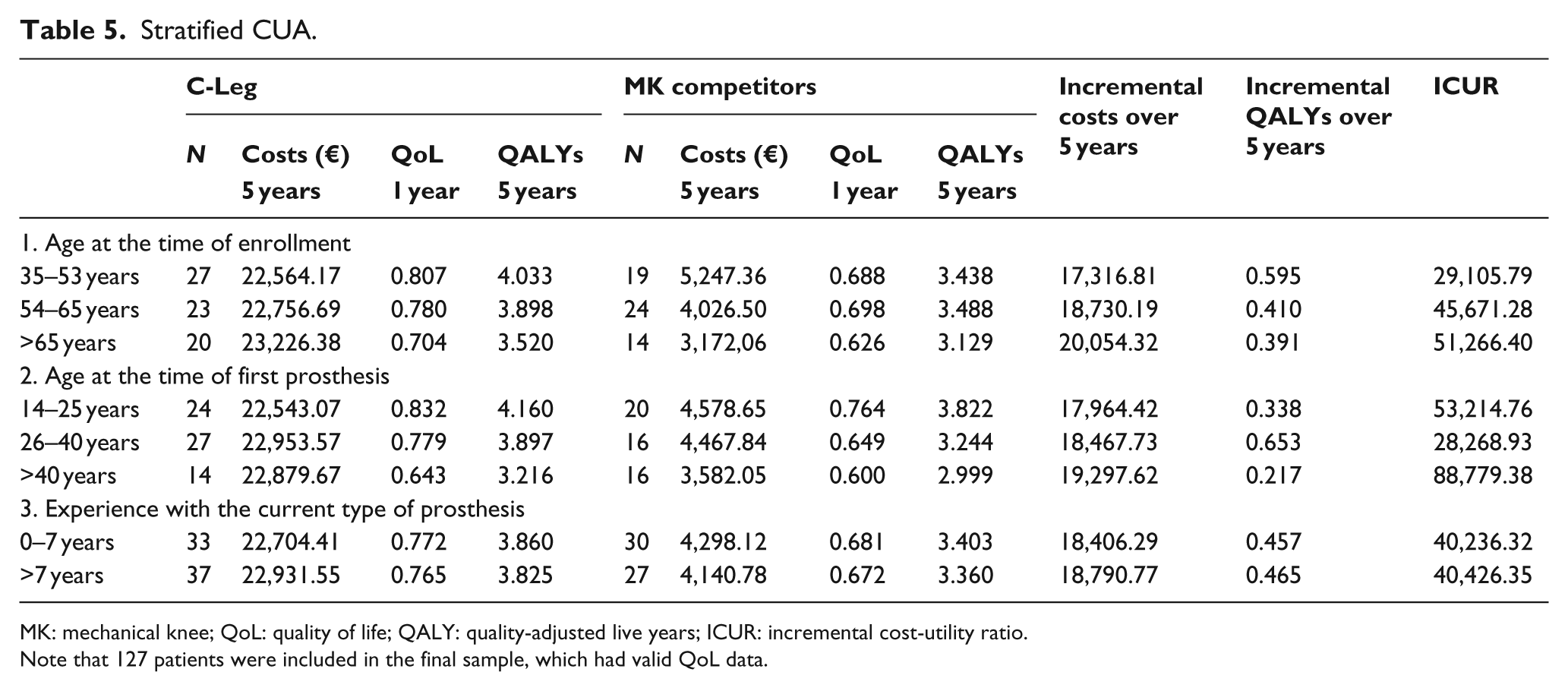
MK: mechanical knee; QoL: quality of life; QALY: quality-adjusted live years; ICUR: incremental cost-utility ratio.
Note that 127 patients were included in the final sample, which had valid QoL data.
First sCUA: age at the time of enrollment
As specified above, for this stratification parameter, three subsets were defined: 32–53, 54–65, and >65 years. In terms of costs, no substantial differences exist among the three subsets of C-Leg users. Instead, relevant differences were observed among MK users, with costs decreasing with increasing age (e.g. patients of 35–53 years spent on average 5247.36 € vs 3,172.06 € spent by patients of >65 years). As such, the incremental costs of C-Leg versus MK competitors increased with age, with a maximum of 20,054.32 € for the subgroup of >65 years.
In terms of utility, for C-Leg patients QoL constantly decreased with age. For MK competitors, differences between the subset 35–53 years and 54–65 years were marginal, while a drop is visible for patients of >65 years. As such, the incremental 5-year QALYs decreased with patients’ age, that is, 0.595 QALYs of younger-middle age adults versus 0.391 QALYs for older participants. From the incremental costs and QALYs, it followed that the ICUR increased with age, although values stand below the acceptability threshold of 54,120 €/QALY.
Second sCUA: age at the time of first prosthesis
For this stratification parameter, three subsets were defined: <26, 26–40, and >40 years. In terms of costs, while C-Leg remained relatively stable across subsets (~22,000 €), MKs costs were higher for those who had the first prosthesis in young age (14–25 years). Indeed, the incremental 5-year costs increased with age, with a maximum of 19,297.62 € for patients of >40 years.
In terms of utility, for both C-Leg and MK users, patients fitted with a prosthesis in young age had substantially higher QoL than patients who had the first prosthesis later in life. The highest incremental QALYs was observed in the subgroup of 26–40 years (i.e. 0.653 QALYs), followed by the subsets of <26 years (0.338 QALYs) and the >40 years (0.217 QwALYs). For this latter group, the drop in incremental QALYs is remarkable compared to the younger ages.
ICUR was therefore lower for patients in subgroup of 26–40 years (28,268.93 €/QALY) compared to patients in subsets of <26 years (53,214.76 €/QALY) and >40 years (88,779.38 €/QALY). Of note, the ICUR value for subset of > 40 years stands above the acceptability threshold.
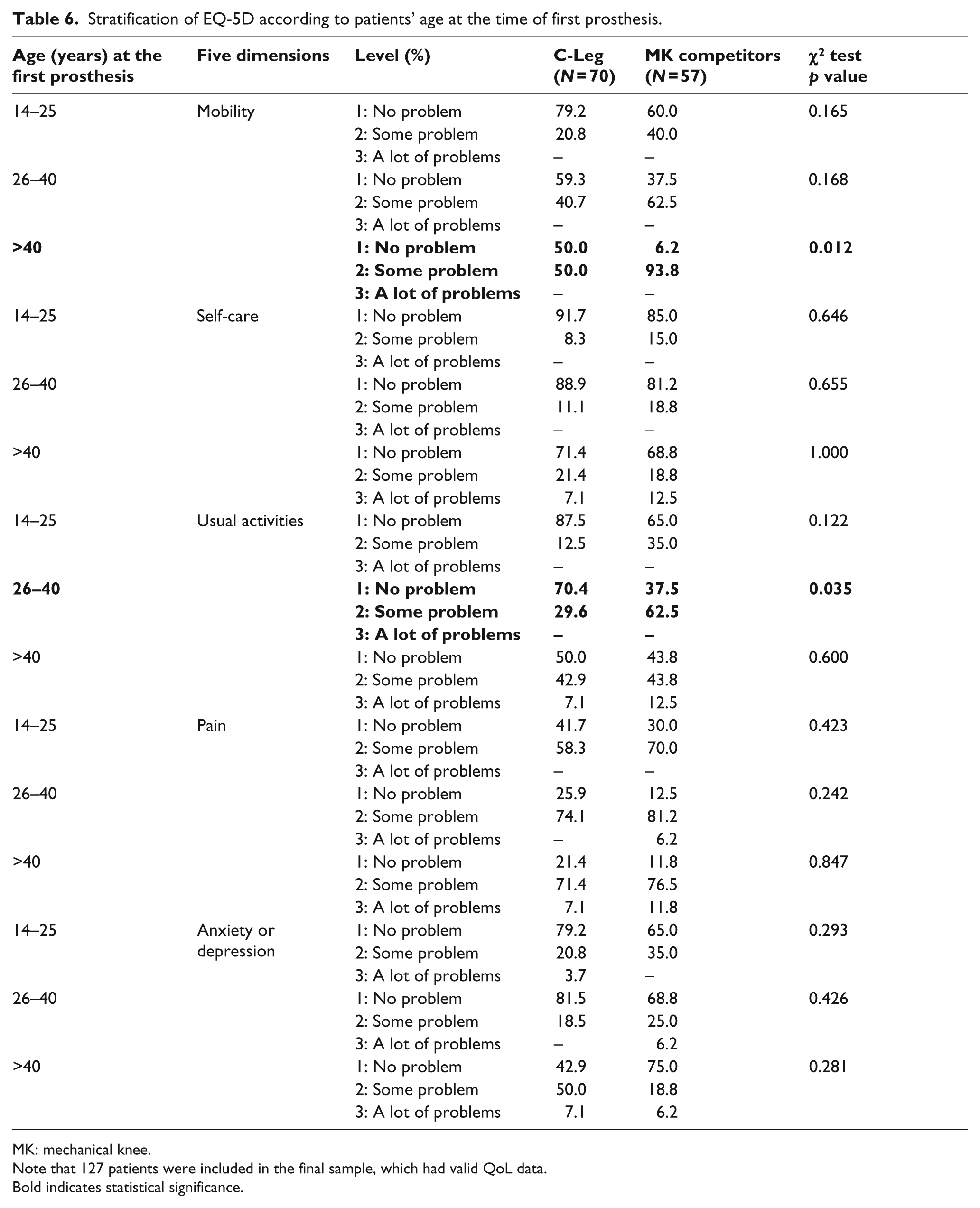
To gain a better understanding, Table 6 provides a comparison between C-Leg and MK users for each of the EQ-5D dimensions, within each of the three “age at the time of first prosthesis” subsets. A significant improvement was observed in “physical mobility” (i.e. greater number of “no problem” answers) for C-Leg patients fitted with a prosthesis after 40 years of age; C-Leg users fitted after 40 years experienced problems in “self-care,” “usual activities,” “pain/discomfort,” and “anxiety/depression” similarly to MK users fitted at the same age. By contrast, a significant improvement was observed in “usual activities” (but not for the other dimensions) for C-Leg patients compared to MK patients within the subset of 26–40 years.
Stratification of EQ-5D according to patients’ age at the time of first prosthesis.
MK: mechanical knee.
Note that 127 patients were included in the final sample, which had valid QoL data.
Bold indicates statistical significance.
Third sCUA: experiences with the current type of prosthesis
For this stratification parameter, two subsets were assumed, namely 0–7 years and > 7 years of experience. In this case, C-Leg and MK patients of both subsets showed similar values for costs and utility. The incremental 5-year costs were ~18,000 €; the incremental 5-year QALYs were ~0.450. ICUR values were almost identical for the two subsets, that is, ~40,000 €/QALY, which fall below the ICUR acceptability threshold.
Discussion
CUA is a powerful tool to support decision-making. However, CUAs applied to prosthetics suffered from two shortcomings so far: (1) the limited sample of patients included in the analysis, and (2) the lack of stratification of results based on patients’ features. With this study, we aimed to complete a CUA between C-Leg and MKs on the largest samples of transfemoral amputees (N = 127) considered so far. In addition, we wanted to extend the CUA considering three stratification parameters (sCUA), to support patient-specific decision-making on technology adoption and modality of provision. We will first discuss CUA results and then focus on sCUA findings.
CUA results were in line with existing work.8,13 C-Leg has better impact on patients’ QoL, but also higher costs, with an ICUR of 40,155.45 €/QALY. Remarkably, this value stands below the ICUR acceptability thresholds (54,120 €/QALY), suggesting a satisfactory degree of cost-utility for C-Leg. The higher costs of C-Leg were balanced by significant improvements for its users, particularly in the “physical mobility” and “usual activities” dimensions of EQ-5D, compared to MK users. In other words, over a 5-year period, the observed incremental QALYs are “value-for-money.”
Findings from the sCUA represent a step forward for an informed decision-making on prosthesis provision. ICUR exceeded the acceptability threshold of 54,120 €/QALY (and even the higher 72,200 €/QALY threshold), for a specific subset of patients, that is, those who were fit with the first prosthesis >40 years of age. Based on this result, it might be superficially concluded that C-Leg should not be provided to these patients. However, a deeper investigation of the sCUA suggests otherwise. Indeed, the analysis of ED-5D showed that first-time prosthetic users of >40 years significantly benefit from C-Leg in terms of “physical mobility.” By contrast, the benefits of C-Leg are less remarkable when considering other QoL dimensions: a non-negligible percentage of patients fitted with either C-Leg or MKs in later life experienced “a lot of problems” in terms of “self-care,” “usual activities,” “anxiety/depression,” and “pain.” In other words, older amputees are similarly affected by psychosocial and psychophysical barriers independently of the type of prosthesis used. As such, the implementation of cost-affordable interventions to break these barriers might boost QoL, supported by the advantages in physical mobility offered by C-Leg. This might bring ICUR within the cost-useful range. For instance, interventions might be targeted to: (1) activities-of-daily-living (ADLs) accomplishment, through gait/rehabilitation training; (2) pain control, through increased physical therapy and medications (e.g. stump and back pain 26 ); (3) create specific job-reintegration pathway; 27 (4) promote sport practice and the use of “apps” that engage in physical activity and challenges between “friends”; 28 (5) promote peer-counseling and support, 29 even through social networks; and (6) improve self-esteem with professional psychological support. 29
The results reported in this study are based on patients treated by a single Prosthetic Center, which is the largest prosthetic provider in Italy and part of a Public Body. Therefore, the same group of prosthetists and physical therapists treated all patients consistently. Limitations, however, do apply. First, all patients suffered from a traumatic, work-related amputation (that include home-to-work car accidents), that is, caution is needed in generalizing results to other etiologies. Second, the retrospective nature of the study could have introduced biases, for example, we cannot exclude that C-Leg had been provided to patients with more opportunities to improve QoL. Nonetheless, the two groups were similar for most patient characteristics. Third, CUA should be extended by considering additional stratification criteria. Self-reported QoL varies greatly among individuals with lower-limb amputation, and several factors beyond those considered here (e.g. level of psychological distress, social support) might be responsible for this variability. 30 Fourth, the response rate to the survey was relatively moderate: 50% of the sample returned valid questionnaires. Fifth, the study used the EQ-5D three-level answer version as a measure of QoL, which is very common in the literature but might be subject to ceiling effect and be less informative than the five-level answer version. 31 Finally, our research has context-specific elements, for example, the costs of prostheses that might limit the direct application of the analysis in any context. We thus encourage replicating results across different national and local settings, as well as developing and exploiting multi-center databases.
Conclusion
Our study described an application of sCUA to support decision-making on both the adoption and the modality of provision of C-Leg, across different subgroups of patients. In particular, we showed that providers should supply C-Leg to patients receiving the first prosthesis: (1) before 40 years of age, because the higher costs are balanced by substantial improvements in QOL; (2) patients of >40 years, because of relevant and crucial improvements in mobility, but adopting interventions that address the psychosocial and psychophysical barriers affecting usual activities, self-care, pain, and anxiety/depression.
Footnotes
Author contribution
A.G. Cutti, E. Lettieri, G. Verni, and C. Masella designed the research. M. Del Maestro, M. Luchetti, and A.G. Cutti collected data. A.G. Cutti, E. Lettieri, M. Del Maestro, and G. Radaelli performed the analyses. All authors contributed to and have approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was founded by the Italian Workers’ Compensation Authority, project C.5.